Introduction
Primary bone marrow diffuse large B-cell lymphoma
(DLBCL) is an uncommon type of non-Hodgkin's lymphoma (NHL). DLBCL
may involve nodal or extranodal sites (1); however, initial presentation in the bone
marrow occurs infrequently (2–6).
Extranodal involvement of the bone marrow as an isolated and unique
localization of aggressive NHLs has been reported (7), including cases of anaplastic large cell
lymphoma or DLBCL.
The rapid diagnosis of primary bone marrow DLBCL is
challenging, as the clinical symptoms and signs are nonspecific. In
addition, the clinical features, optimal management, diagnostic
procedures and prognostic factors associated with this disease
remain to be elucidated (8).
Recently, the diagnostic criteria for primary bone marrow lymphoma
(PBML) have been proposed, and the clinicopathological features of
this extremely rare tumor have also been documented (7). The current study presents the case of a
patient with primary bone marrow DLBCL who was admitted to the
hospital with symptoms of fever and arthralgia. A correct initial
diagnosis of primary bone marrow DLBCL was determined by multiple
bone marrow biopsies at different locations.
Case report
A 41-year-old male patient was admitted to the
Affiliated Hospital of Jining Medical University (Jining, China) on
August 4th, 2014, with initial complaints of a high fever and
arthralgia. The patient also presented with recent onset of
pharyngalgia, coughing, weight loss and malaise. Following
admission, a physical examination revealed that the patient's body
temperature was 39.4°C; however, lymphadenopathy and
hepatosplenomegaly were not observed. Blood tests indicated
leukopenia and anemia [white blood cell (WBC) count,
2.75×109/l (normal, 3.5–9.5×109/l); red blood
cell (RBC) count, 2.62×1012/l (normal,
4.3–5.3×1012/l); hemoglobin (HGB) level, 100 g/l
(normal, 130–175 g/l)], elevated lactate dehydrogenase (LDH) levels
(1,191 U/l; normal, 90–240 U/l) and elevated C-reactive protein
(CRP) levels (39.83 mg/l; normal, 0–10 mg/l). All other results,
including comprehensive serology and screening for autoimmune
antibodies, were unremarkable. A bone marrow puncture of the right
posterior iliac crest was a dry tap. No abnormalities were detected
(data not shown). Contrast-enhanced computed tomography (CT;
SOMATOM Definition Flash CT; Siemens Healthcare, Erlangen, Germany)
confirmed no hepatosplenomegaly, and malignancy could not be
confirmed.
In the following week, pancytopenia, LDH elevation,
direct bilirubin elevation, CRP elevation and B symptoms were not
resolved. These results indicated no lymph node and extranodal
involvement, but suggested bone marrow involvement. Bone marrow
aspiration was repeated in the left posterior iliac crest and
sternum, and a bone marrow biopsy of the left posterior iliac crest
was performed. Resected tissues were formalin-fixed,
paraffin-embedded and cut into sections (2–4 µm) using a RM2235
rotary microtome (Leica, Wetzlar, Germany). Peripheral blood
samples and bone marrow aspirate smears were stained with
Wright-Giemsa (Beijing Leagene Biotech Co., Ltd., Beijing, China)
for morphological evaluation (Olympus L100 S600; Olympus, Tokyo,
Japan). Formalin-fixed specimens were stained with hematoxylin and
eosin (Beyotime Institute of Biotechnology, Shanghai, China) for
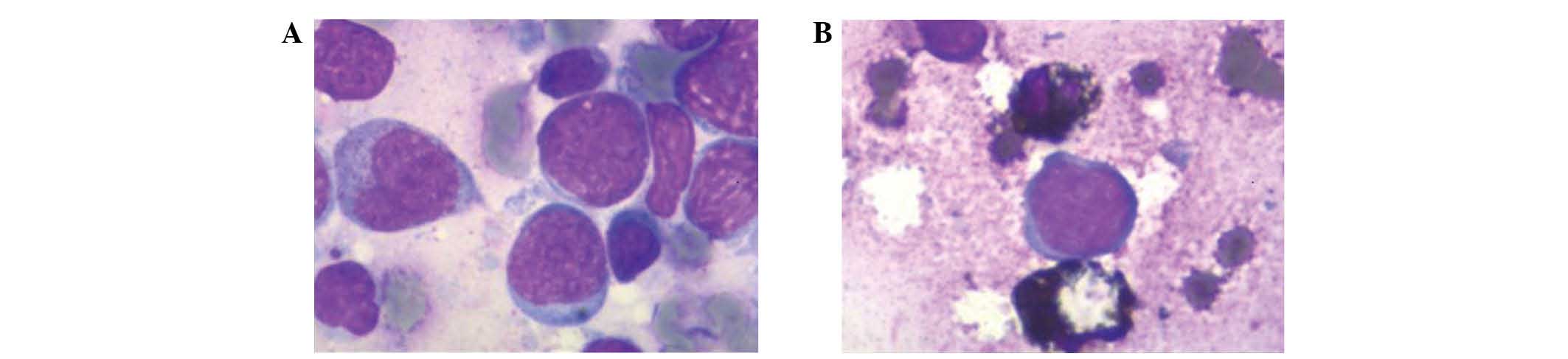
histological evaluation. Large lymphoma cells were present in the
marrow aspirates on Wright-Giemsa-stained (Fig. 1A) and leukocyte peroxidase
(myeloperoxidase)-stained (Fig. 1B)
slides.
For flow cytometry, 50 µl aliquots of cell
suspensions were incubated at room temperature (22–25°C) with the
following fluorescent monoclonal mouse anti-human antibodies (BD
Biosciences, San Jose, CA, USA) for 30 min: Cluster of
differentiation (CD)45-peridinin-chlorophyll protein complex (cat.
no. 564106), CD10-phycoerythrin (PE; cat. no. 561002),
CD20-fluorescein isothiocyanate (FITC; cat. no. 556632),
CD34-allophycocyanin (APC; cat. no. 560940), CD11c-APC (cat. no.
559877), CD5-FITC (cat. no. 561896), CD19-PE (cat. no. 561741) and
immunoglobulin κ (cat. no. 555861) and λ (cat. no. 562893) light
chains. Next, 2.5 ml ammonium chloride (BD Biosciences) was added
for 10 min to lyse the RBCs. The cells were centrifuged at 190 × g
for 5 min using the Cence H1650R centrifuge (Cence, Changsha,
China) and washed with phosphate-buffered saline. The second cell
pellet was resuspended in 0.5 ml PBS containing 1% formaldehyde
(Polysciences Inc., Warrington, PA, USA). Cells were analyzed using
a FACSCalibur flow cytometer (BD Biosciences). Data were quantified
using CellQuest software (BD Biosciences). Flow cytometry confirmed
the presence of lymphoma in the aspirates, which revealed
positivity for cluster of differentiation (CD)20, CD19, CD10 and λ
light chain, and negativity for CD5, CD11c and κ light chain
(Fig. 2).
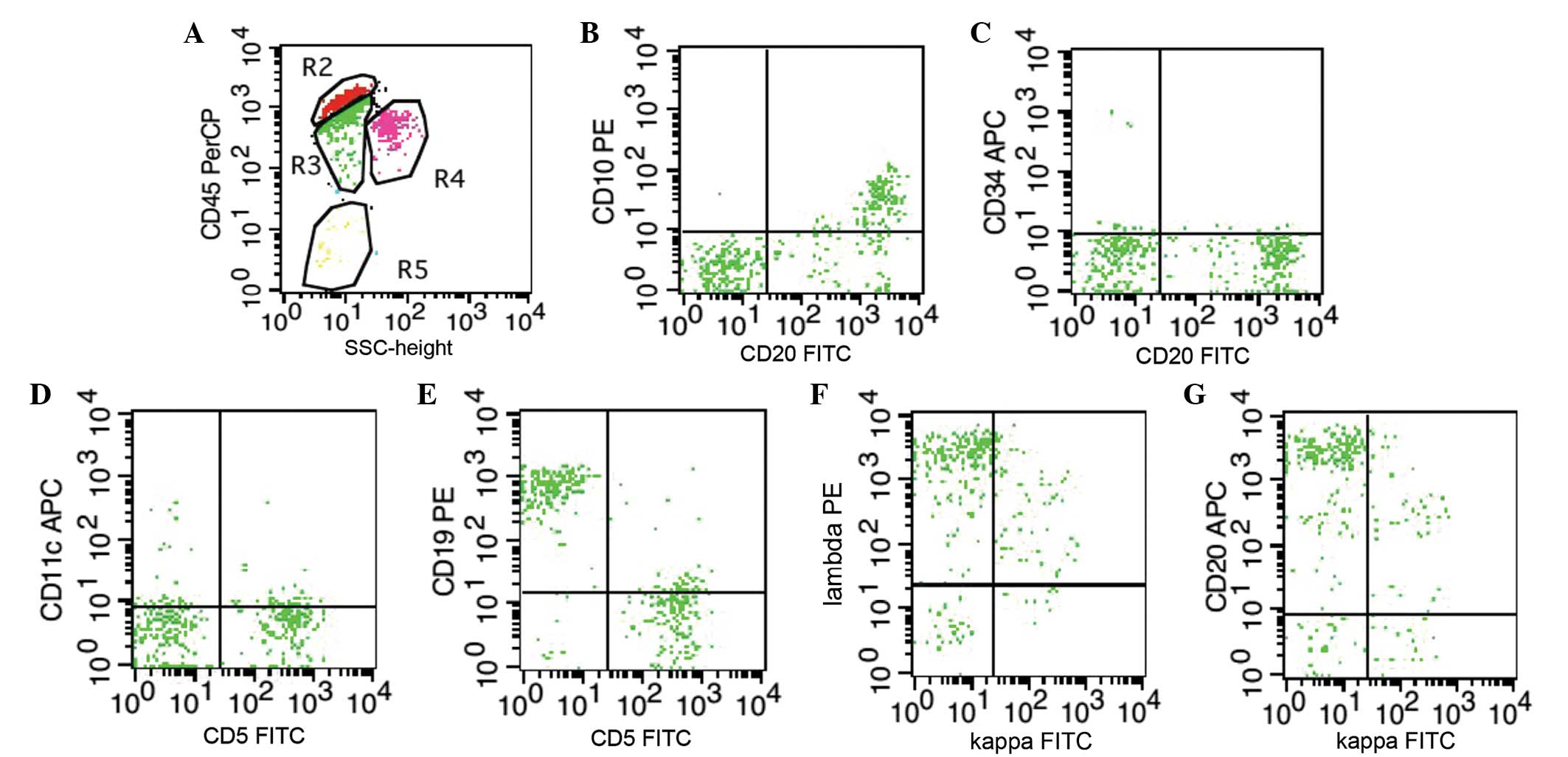 | Figure 2.Immunophenotype of the bone marrow
cells as detected by flow cytometric analysis. (A) CD45 was used to
gate B lymphocytes. (B-G) Cells were positive for (B, C and G) CD20
(positive rate >20%), (B) CD10, (E) CD19 and (F) λ light chain,
and negative for (D) CD11c, (D and E) CD5 and (G) κ light chain.
CD, cluster of differentiation; FITC, fluorescein isothiocyanate;
PE, phycoerythrin; APC, allophycocyanin; SSC, side scatter. |
Biopsy specimens revealed focal hyperplasia of large
abnormal lymphoid cells and bone marrow necrosis (Fig. 3A–B). Bone marrow biopsy specimens were
formalin-fixed, paraffin-embedded and cut into 2–4-µm sections
using the RM2235 rotary microtome. Each section was stained with
hematoxylin and eosin and used for immunostaining.
Immunohistochemical analyses were performed using an autostainer
(Benchmark XT system; Ventana Medical Systems, Inc., Tucson, AZ,
USA) according to the manufacturer's protocol. The following
ready-to-use mouse monoclonal primary antibodies were used: CD43
(cat. no. 14690602), CD10 (cat. no. 14368806), CD20 (cat. no.
140316020), CD38 (cat. no. 141124341), terminal deoxynucleotidyl
transferase (cat. no. 140508197), Ki67 (cat. no. 14690209) and
CD79a (cat. no. 14620803) (ZSGB-BIO, Beijing, China); and CD34
(cat. no. END-R-7-CE; Leica). Following incubation with the primary
antibodies at 4°C overnight, sections were incubated with a
monoclonal biotin-conjugated goat anti-mouse IgG secondary antibody
(cat. no. Kit-9710; ready-to-use; Fuzhou Maixin Biotech. Co., Ltd.,
Fuzhou, China) at 37°C for 30 min, followed by peroxidase-labeled
streptavidin and diaminobenzidine chromogen (Ventana UltraView
Universal DAB Detection Kit; Ventana Medical Systems, Inc.).
Evaluation was then performed using an Olympus BX51 microscope
(Olympus Corporation, Tokyo, Japan). All immunostaining was
performed using a BenchMark XT automated immunostaining device
(Ventana Medical Systems, Inc.). Immunohistochemical staining
indicated that the abnormal cells were positive for CD20, melanoma
associated antigen (mutated) 1, CD79a, Ki-67 and silver staining;
and negative for CD10, CD34, CD38, CD43 and terminal
deoxynucleotidyl transferase (Fig.
3C–L). This immunophenotype matches that previously ascribed to
DLBCL (9). A diagnosis of primary
bone marrow DLBCL was made based on these results.
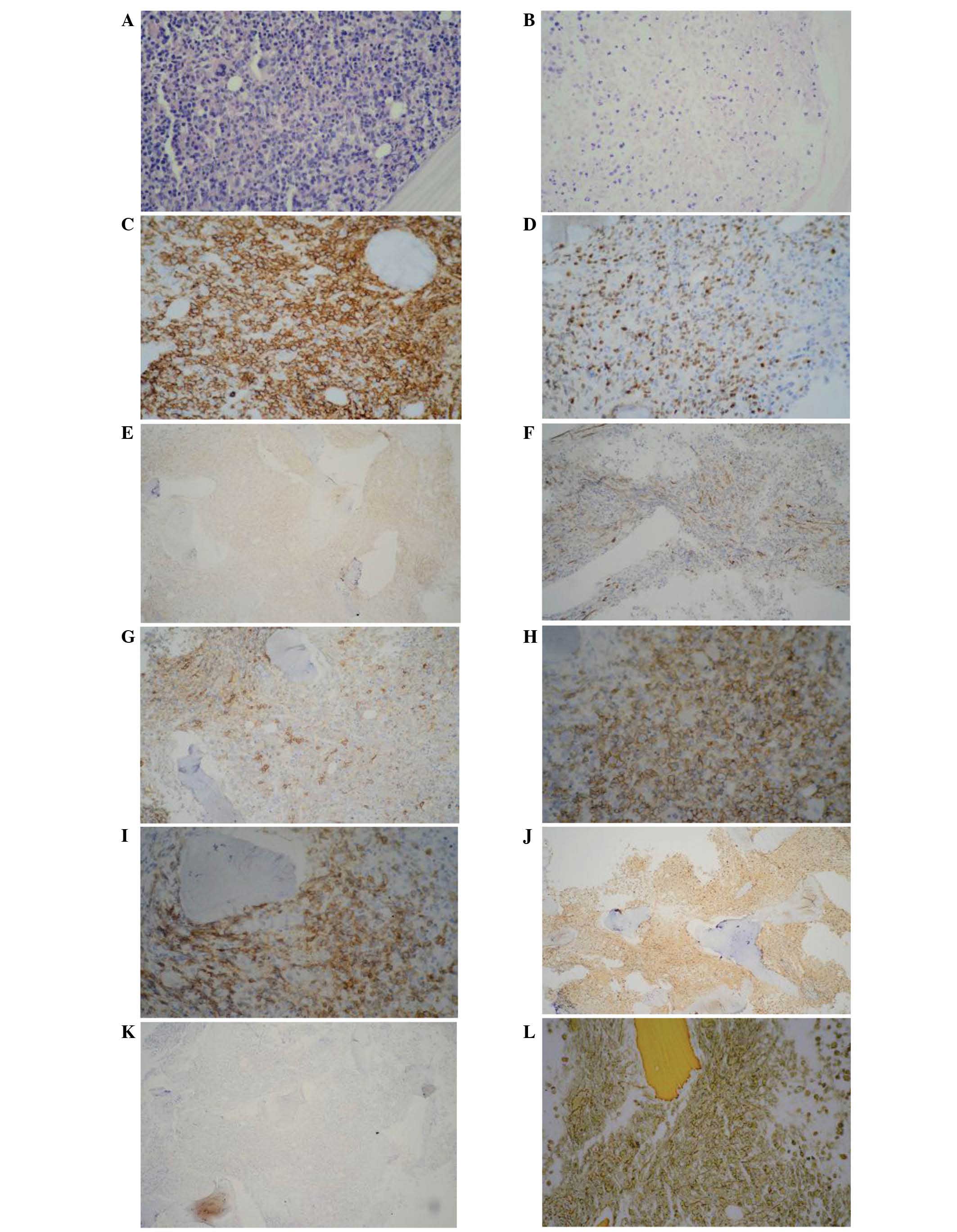 | Figure 3.Histopathological and
immunohistochemical features of the bone marrow biopsy. Images of
the bone marrow biopsy showed involvement of large abnormal
lymphoid cells with focal clusters. (A) Hyperactivity of the bone
marrow (hyperplasia) and (B) necrotic zone (hematoxylin and eosin
staining; magnification, ×400). The tumor cells were (C) positive
for CD20 (magnification, ×400), (D) positive for melanoma
associated antigen (mutated) 1 (magnification, ×400), (E) negative
for CD10 (magnification, ×100), (F) negative for CD34
(magnification, ×200), (G) negative for CD38 (magnification, ×200),
(H) negative for CD43 (magnification, ×400), (I) positive for CD79a
(magnification, ×400), (J) positive for Ki-67 (magnification,
×100), (K) negative for terminal deoxynucleotidyl transferase
(magnification, ×100), and (L) positive for silver staining
(magnification, ×400). CD, cluster of differentiation. |
In August 2014, the patient was administered with
four cycles of chemotherapy with cyclophosphamide, vincristine,
epirubicin and prednisone (CHOP regimen) plus etoposide as part of
a 3-week standard cycle, as follows: Etoposide [50
mg/(m2x day)], vincristine [0.4 mg/(m2 ×
day)] and epirubicin [15 mg/(m2 × day)] administered via
continuous intravenous (i.v.) drip for 96 h; cyclophosphamide (750
mg/m2, i.v., day 5); and prednisone [60
mg/(m2 × day), orally, days 1–5]. Cerebrospinal fluid
examination showed no obvious lymphomatous infiltration (data not
shown). Following one course of chemotherapy, remission of symptoms
was observed. The patient's temperature returned normal, and the
arthralgia reduced. Blood tests indicated a WBC count of
6.10×109/l, RBC count of 2.37×1012/l and HGB
level of 67 g/l, and the bone marrow tests indicated partial
remission. If the patient achieved complete remission, another two
cycles of CHOP chemotherapy would be administered as consolidation
therapy. If not, other chemotherapy regimens would be explored. The
last follow-up was conducted on May 7, 2015, however, the patient
has since been lost to follow-up.
Discussion
Extranodal DLBCLs have specific clinicopathological
features that are dependent on the organ of origin (3). Previous reports have shown that invasion
of lymphoma cells may be detected in the brain, adrenal glands,
kidney and skin in autopsy cases (10–17).
However, DLBCL primarily arising from the bone marrow is an
extremely rare entity, with only a few retrospective studies and
sporadic cases reported in the literature (4,18–22). Previously, Wong et al (23) reported 14 cases of large cell lymphoma
with initial manifestation in the bone marrow, of which 4 exhibited
a B-cell phenotype, 3 a T-cell phenotype, and 1 a non-T non-B
phenotype. The majority of patients had ‘swinging’ fever and
peripheral blood cytopenia. However, in the present case, the
patient complained only of fever and arthralgia as the initial
symptoms. This presentation is extremely rarely reported.
The diagnosis of primary bone marrow DLBCL is
difficult due to the absence of guidelines regarding clinical
features, optimal management, diagnostic procedures and prognostic
factors (8). As no lesions were
observed in the present case, and only fever and joint pain were
reported, multiple bone marrow biopsies in different locations were
performed. DLBCL is most commonly diagnosed using positron emission
tomography (PET)-CT (24,25). By contrast, the current study relied
on multiple bone marrow biopsies combined with the clinical
findings, physical examination, morphology and flow cytometry
results. The findings of the present case corresponded to the
diagnostic criteria of PBML previously proposed (7). Notably, the patient in the present case
complained primarily of joint pain. This may have resulted from
bone marrow necrosis. However, this should be studied further.
The optimal therapy for PBML has still not been
proposed. Autologous hematopoietic stem cell transplantation or
multi-agent chemotherapy with rituximab plus CHOP regimen followed
by involved field radiotherapy are typically the chosen treatment
options (17,26–29).
However, the exact roles and effects of these treatments are
unclear due to the extremely low incidence of the disease. In the
present study, the patient received CHOP regimen plus etoposide,
and achieved a reduction in the fever and arthralgia, in addition
to partial remission as indicated by bone marrow tests.
In conclusion, DLBCL primarily arising from the bone
marrow is an extremely rare entity. The present case demonstrates
that awareness should be raised of bone marrow DLBCL, particularly
in patients presenting with fever and arthralgia. In addition, when
lymphoma is suspected, it is imperative to perform multiple bone
marrow biopsies in various locations. The long-term outcome and the
prognosis of DLBCL require further investigation with more
cases.
Acknowledgements
This study was supported by the Science and
Technology Program of Shandong Province, China (grant no.
2012YD18066) and the Health and Family Planning Commission of
Shandong Province (grant no. 9,2012).
References
|
1
|
Yamashita T, Ishida M, Moro H, Yumoto H,
Uchibayashi S, Yoshii M, Nakanishi R, Okuno H, Yoshida T, Okuno T,
et al: Primary bone marrow diffuse large B-cell lymphoma
accompanying cold agglutinin disease: A case report with review of
the literature. Oncol Lett. 7:79–81. 2014.PubMed/NCBI
|
|
2
|
Morice WG, Rodriguez FJ, Hoyer JD and
Kurtin PJ: Diffuse large B-cell lymphoma with distinctive patterns
of splenic and bone marrow involvement: Clinicopathologic features
of two cases. Mod Pathol. 18:495–502. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mann RB: Are there site-specific
differences among extranodal aggressive B-cell neoplasms? Am J Clin
Pathol. 111(1 Suppl 1): S144–S150. 1999.PubMed/NCBI
|
|
4
|
Lapa C, Knott M, Rasche L, Herrmann K,
Buck AK and Rosenwald A: Primary bone marrow diffuse large B-cell
lymphoma affecting distal parts of the legs as a cause of
persisting B symptoms. Eur J Haematol. 93:545–546. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ogura K, Miyake N, Yasuda H, Udaka N and
Hirano T: Diffuse large B-cell lymphoma initially manifesting in
bone marrow: A case report. Rinsho Byori. 58:1176–1180. 2010.(In
Japanese). PubMed/NCBI
|
|
6
|
Antic D, Petrovic N, Pelemis M, Stevanovic
G, Perunicic M and Mihaljevic B: ‘Invisible’ primary cutaneous
diffuse large B-Cell lymphoma, leg type, as a cause of fever of
unknown origin. J Clin Oncol. 31:e276–e279. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Martinez A, Ponzoni M, Agostinelli C,
Hebeda KM, Matutes E, Peccatori J, Campidelli C, Espinet B, Perea
G, Acevedo A, et al: Primary bone marrow lymphoma: An uncommon
extranodal presentation of aggressive non-Hodgkin lymphomas. Am J
Surg Pathol. 36:296–304. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jiang AG, Gao XY and Lu HY: Diagnosis and
management of a patient with primary pulmonary diffuse large B-cell
lymphoma: A case report and review of the literature. Exp Ther Med.
8:797–800. 2014.PubMed/NCBI
|
|
9
|
Menon MP, Pittaluga S and Jaffe ES: The
histological and biological spectrum of diffuse large B-cell
lymphoma in the World Health Organization classification. Cancer J.
18:411–420. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Oehler E, Valour F, Hachulla E and Ghawche
F: Myopericarditis as the presenting manifestation of adult Still's
disease. Rev Med Interne. 35:827–830. 2014.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Imamura K, Awaki E, Aoyama Y, Kondo S,
Horie Y, Ohama E and Nakashima K: Intravascular large B-cell
lymphoma following a relapsing stroke with temporary fever: A brain
biopsy case. Intern Med. 45:693–695. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lokesh KN, Sathyanarayanan V,
Kuntegowdanahalli CL, Suresh TM, Dasappa L and Kanakasetty GB:
Primary diffuse large B-cell lymphoma of testis: A single centre
experience and review of literature. Urol Ann. 6:231–234. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kashimura M, Noro M, Akikusa B, Okuhara A,
Momose S, Miura I, Kojima M and Tamaru J: Primary splenic diffuse
large B-cell lymphoma manifesting in red pulp. Virchows Arch.
453:501–509. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim HS: Primary testicular diffuse large
B-cell lymphoma: A case report focusing on touch imprint cytology
and a non-germinal center B-cell-like phenotype. Exp Ther Med.
6:33–36. 2013.PubMed/NCBI
|
|
15
|
Zhang X, Sun M, Zhang L and Shao H:
Primary hepatosplenic CD5-positive diffuse large B-cell lymphoma: A
case report with literature review. Int J Clin Exp Pathol.
6:985–989. 2013.PubMed/NCBI
|
|
16
|
Kodama K, Massone C, Chott A, Metze D,
Kerl H and Cerroni L: Primary cutaneous large B-cell lymphomas:
Clinicopathologic features, classification, and prognostic factors
in a large series of patients. Blood. 106:2491–2497. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Al Shemmari S, Sankaranarayanan SP and
Krishnan Y: Primary mediastinal large B-cell lymphoma: Clinical
features, prognostic factors and survival with RCHOP in Arab
patients in the PET scan era. Lung India. 31:228–231. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Níáinle F, Hamnvik OP, Gulmann C,
Bermingham C, Kelly J, McEvoy P and Murphy P: Diffuse large B-cell
lymphoma with isolated bone marrow involvement presenting with
secondary cold agglutinin disease. Int J Lab Hematol. 30:444–445.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kajiura D, Yamashita Y and Mori N: Diffuse
large B-cell lymphoma initially manifesting in the bone marrow. Am
J Clin Pathol. 127:762–769. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chang H, Hung YS, Lin TL, Wang PN, Kuo MC,
Tang TC, Wu JH, Dunn P and Shih LY: Primary bone marrow diffuse
large B cell lymphoma: A case series and review. Ann Hematol.
90:791–796. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sumi M, Ichikawa N, Shimizu I, Yotsumoto
M, Ueno M and Kobayashi H: Primary diffuse large B-cell lymphoma of
the bone marrow complicated with autoimmune hemolytic anemia and
erythroid hypoplasia. Rinsho Ketsueki. 48:571–575. 2007.(In
Japanese). PubMed/NCBI
|
|
22
|
Hishizawa M, Okamoto K, Chonabayashi K,
Kaneko H, Watanabe M and Tsudo M: Primary large B-cell lymphoma of
the bone marrow. Br J Haematol. 136:3512007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wong KF, Chan JK, Ng CS, Chu YC, Li LP and
Chan CH: Large cell lymphoma with initial presentation in the bone
marrow. Hematol Oncol. 10:261–271. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Jerusalem G, Beguin Y, Fassotte MF, Najjar
F, Paulus P, Rigo P and Fillet G: Whole-body positron emission
tomography using 18F-fluorodeoxyglucose for posttreatment
evaluation in Hodgkin's disease and non-Hodgkin's lymphoma has
higher diagnostic and prognostic value than classical computed
tomography scan imaging. Blood. 94:429–433. 1999.PubMed/NCBI
|
|
25
|
Zinzani PL, Fanti S, Battista G, Tani M,
Castellucci P, Stefoni V, Alinari L, Farsad M, Musuraca G, Gabriele
A, et al: Predictive role of positron emission tomography (PET) in
the outcome of lymphoma patients. Br J Cancer. 91:850–854.
2004.PubMed/NCBI
|
|
26
|
Tai WM, Quah D, Yap SP, Tan SH, Tang T,
Tay KW, Koo YX, Tao M, Quek R and Lim ST: Primary mediastinal large
B-cell lymphoma: Optimal therapy and prognostic factors in 41
consecutive Asian patients. Leuk Lymphoma. 52:604–612. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Avilés A, Neri N, Fernández R,
Huerta-Guzmán J and Nambo MJ: Randomized clinical trial to assess
the efficacy of radiotherapy in primary mediastinal large
B-lymphoma. Int J Radiat Oncol Biol Phys. 83:1227–1231. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhu YJ, Huang JJ, Xia Y, Zhao W, Jiang WQ,
Lin TY, Huang HQ and Li ZM: Primary mediastinal large B-cell
lymphoma (PMLBCL) in Chinese patients: Clinical characteristics and
prognostic factors. Int J Hematol. 94:178–184. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Niscola P, Palombi M, Fratoni S, Perrotti
A and de Fabritiis P: Primary diffuse large B-cell lymphoma of the
bone marrow in a frail and elderly patient successfully treated
with rituximab, cyclophosphamide, doxorubicin, vincristine, and
prednisone. Blood Res. 48:296–297. 2013. View Article : Google Scholar : PubMed/NCBI
|