Introduction
Breast cancer is one of the most common malignant
cancers among women, and in some cases, is life threatening
(1). The American Cancer Society has
reported that new cases of invasive breast cancer in the USA will
reach 246,660 by 2016, accounting for 29% of de novo
malignancies among women, and breast cancer-related mortality is
estimated to reach 40,450 in 2016 (2). In China, breast cancer is the most
prevalent cancer in women, and the number of new cases diagnosed is
increasing every year (3). Developing
novel biomarkers of breast cancer may improve knowledge of how
breast cancer develops, and potentially allow more efficient
therapeutic strategies to be implemented.
Tyrosine-protein kinase receptor UFO (Axl), belongs
to the TAM family of receptor tyrosine kinases, which consists of
Axl, tyrosine-protein kinase receptor Tyro3, and tyrosin protein
kinase Mer. Axl is a transforming gene that was originally isolated
from patients with chronic myelogenous leukemia (4). The growth arrest specific gene 6 (Gas6)
is a ligand of Axl, and the binding of Gas6 to Axl results in the
dimerization of Gas6/Axl complexes, activating intracellular
tyrosine kinase, and triggering a series of signal transduction and
biological effects (5). It has
previously been reported that Axl participates in signaling
pathways related to carcinogenesis and cancer development, such as
the phosphatidylinositol 3-kinase/protein kinase B pathway, the
Janus kinase/signal transducers and activators of transcription
pathway, and nuclear factor-κB signaling pathway (6–8). It has
also been demonstrated that Axl is an underlying oncogenic factor
involved in the epithelial-mesenchymal transition, which allows
epithelial cells to undergo cell migration and invasion, and thus
contribute to tumor metastasis (9).
Axl has been implicated in different types of human cancer and is
related to their development and clinical prognosis. These include:
Gastric (10), lung (11), bladder (12), thyroid (13), pancreatic (14) and colon (15) cancer.
Methods of blocking Axl expression by RNA silencing
or Axl inhibition have been studied in vivo and in
vitro. The results of these studies suggest that Axl is a
promising target in cancer therapy. For example, LY2801653, a multi
kinase inhibitor of the hepatocyte growth factor receptor (MET) and
Axl, is capable of inhibiting cell migration, proliferation and
anti-tumor activities (16). The
effects of inhibiting Axl expression by Amuvatinib (MP470) have
been studied in gastrointestinal stromal tumors and breast cancer
(17). Furthermore, Foretinib, an
experimental multi kinase inhibitor targeting MET, vascular
endothelial growth factor receptor 2, and Axl, may inhibit the
proliferation and survival of colorectal cancer cells (18).
The association between Axl and breast cancer has
been widely researched. However, the clinicopathological
significance and the prognostic role of Axl in breast cancer
remains controversial, and there have been few studies
investigating the exact role of Axl in breast cancer. The present
study aimed to measure Axl expression in breast cancer tissue and
noncancerous lesions by immunohistochemical staining, and to
explore the prognostic value of Axl in patients with breast
cancer.
Materials and methods
Patients and surgical specimens
Specimens were obtained from 60 female patients
(average age, 50.60±1.36) undergoing surgery at the Department of
Breast Surgery, the First Affiliated Hospital, Henan University of
Science and Technology, between January and August 2010. Informed
consent was obtained from all the patients to use the surgical
specimens for scientific research. The specimens included 60 cases
of breast infiltrative ductal cancer tissues and 40 cases of benign
breast lesions (25 mammary dysplasia and 15 breast fibroadenoma).
The median age of patients at breast cancer diagnosis was 48 years
old (range, 28–80 years). None of the patients received
chemoradiotherapy or endocrine therapy before surgery, and there
were no obvious abnormalities in the preoperative function of the
heart, lungs, liver, or kidney of any patients. There was also no
distant metastasis detected in any patients before operations were
performed. The clinicopathological characteristics of the patients
with breast cancer are presented in Table
I.
 | Table I.Patient clinicopathological
characteristics. |
Table I.
Patient clinicopathological
characteristics.
| Patient
characteristics, n=60 |
|---|
|
|---|
| Variable | Number (%) |
|---|
| Age, years |
|
| ≤50 | 33 (55.0) |
|
>50 | 27 (45.0) |
| Histological
grade |
|
| G1 | 13 (21.7) |
|
G2/G3 | 47 (78.3) |
| Tumor size, cm |
|
|
<2 | 24 (40.0) |
| ≥2 | 36 (60.0) |
| Lymph node
status |
|
| N0 | 35 (58.3) |
| N+ | 25 (41.7) |
| TNM stage |
|
| I | 19 (31.7) |
| II | 28 (46.7) |
| III | 13 (21.7) |
| ER |
|
|
Negative | 25 (41.7) |
|
Positive | 35 (58.3) |
| PR |
|
|
Negative | 32 (53.3) |
|
Positive | 28 (46.7) |
| HER-2 |
|
|
Negative | 41 (68.3) |
|
Positive | 19 (31.7) |
| Ki-67, % |
|
|
≤14 | 19 (31.7) |
|
>14 | 41 (68.3) |
| Molecular
subtype |
|
| Luminal
type | 36 (60.0) |
|
Non-luminal type | 24 (40.0) |
Postoperative treatment was performed according to
the National Comprehensive Cancer Network (NCCN) guidelines. The
tissue specimens were fixed in 10% formaldehyde solution and
embedded in paraffin blocks. Paraffin blocks were cut into sections
3 µm thick. All cases of breast cancer were confirmed by
professional pathologists by hematoxylin-eosin (HE) staining, and
were categorized according to the 7th edition of the American Joint
Committee on Cancer Tumor-Node-Metastasis (TNM) stage
classification (19). The molecular
subtyping of breast cancer followed the guidelines issued at the
St. Gallen International Breast Cancer Conference 2013 (20); the luminal type included luminal A and
luminal B type breast cancer, the non-luminal type included Erb-B2
overexpression and basal-like type breast cancer.
Immunohistochemistry IHC
The paraffin sections of cancerous and benign
lesions were baked for 2 h at 60°C, deparaffinized with
dimethylbenzene and hydrated in gradient ethanol. Tissue antigen
retrieval was performed using citrate sodium buffer (pH 6.0) at
95°C for 15 min and cooled at room temperature for 30 min.
Endogenous peroxidase was blocked with methanol containing 3%
H2O2 for 10 min, then the slides were treated
with 5% normal goat serum (SL2; Beijing Solarbio Science &
Technology Co., Ltd., Beijing, China) for 30 min to limit
non-specific binding. The anti-Axl rabbit polyclonal antibody
(1:100; ab37861; Abcam, Cambridge, MA, USA) was overlaid on the
sections and incubated overnight at 4°C. Following re-warming at
room temperature for 1 h and three washes in PBS (AR0030; Wuhan
Boster Biological Technology, Ltd., Wuhan, China), sections were
incubated with horseradish peroxidase-labeled secondary antibody
(1:500; SA00001-2; Wuhan Sanying Biotechnology, Wuhan, China) for
30 min at room temperature. Diaminobenzidine (DAB-0031; Fuzhou
Maixin Biotech Co., Fuzhou, China) was used for antigen detection.
Subsequently, the slides were counterstained with hematoxylin for
10 sec, dehydrated in gradient ethanol and mounted, and then viewed
under an optical microscope. Negative controls used for comparison
were incubated with phosphate buffer saline instead of the primary
antibody.
Evaluation of immunohistochemical
staining
Sections were evaluated independently by two
different investigators with no prior knowledge of patient clinical
information, and disagreements were resolved through discussion.
Human epidermal growth factor receptor 2 (HER-2) staining was
carried out and evaluated according to the standards provided by
NCCN: −, ±, + were all defined as negative; +++ as positive, and
FISH quantitative determination was conducted when the staining
score ≥++ (21).
Axl expression score was based on an intensity score
(IS) and a proportion score (PS). IS was graded on the following
scale: No staining, 0; mild staining, 1; moderate staining, 2;
intense staining, 3; extremely intense staining, 4. The PS was
graded as follows: ≤10%, 0; 11–25%, 1; 26–50%, 2; 51–75%, 3;
>75%, 4. Therefore, the range of the combined staining score
(IS+PS) was 0–8. A total score ≤1 was considered to be negative
(−); a score of 2–3 was considered to be weakly positive (+); a
score of 4–6 was considered to be positive (++); a score of 7–8 was
considered to be strong positive (+++). Scores of (−) and (+) were
regarded as low levels of expression, whereas scores of (++) and
(+++) were regarded as high levels of expression.
Follow-up information
The 60 breast cancer patients were followed up by
telephone conversation, although home visits were also undertaken
if required. Telephone numbers and addresses were acquired from
patient records. The follow-up deadline was September 2015. Patient
survival time was calculated from the date of operation until the
date of cancer-related mortality. Disease-free survival time (DFS)
and overall survival time (OS) were adopted as prognostic indexes.
The DFS events included locoregional recurrence, distant metastasis
and contralateral breast cancer. OS events included all
cancer-related mortality. Recurrence, distant metastasis and
contralateral metastasis of patients were confirmed by X-ray plain
film, ultrasonography, computed tomography and pathological
examination.
Statistical analysis
The association between Axl expression and
clinicopathological features were analyzed by χ2 or
Fisher's exact tests. Correlational analyses were conducted using
the analysis of Spearman rank correlation. Patient survival was
estimated using the Kaplan-Meier method and compared with the log
rank test. Prognostic factors were analysed by the Cox proportional
hazard model, and the assignment of risk factors is presented in
Table II. All statistical analyses
were performed using the SPSS 21.0 program (IBM SPSS, Inc., Armonk,
NY, USA). P<0.05 was considered to indicate a statistically
significant difference.
| Table II.Classification and assignment of
prognostic influence factors in patients. |
Table II.
Classification and assignment of
prognostic influence factors in patients.
| Variable
classification and assignment | Variables |
|---|
| Age, years | ≤50=0,
>50=1 |
| Histological
grade | G1=0, G2/G3=1 |
| Tumor size | <2 cm=1, ≥2
cm=0 |
| Lymph node
status | N0=0, N+=1 |
| TNM stage | I=0, II/III=0 |
| ER | Negative=0,
positive =1 |
| PR | Negative=0,
positive =1 |
| HER-2 | Negative=0,
positive =1 |
| Ki-67 | ≤14%=0,
>4%=1 |
| Molecular
subtype | Non-luminal type=0,
luminal type=1 |
| Axl | Negative=0,
positive=1 |
| DFS | Month(s) |
| DFS status | Metastasis or
recurrence=0, truncated=1 |
| OS | Month(s) |
| OS status | Death=0,
truncated=1 |
Results
Axl is highly expressed in malignant
breast cancer tissue compared with benign breast lesions
Positive immunoreactivity for Axl was mainly
observed in the cell cytoplasm and membrane; the positive cells
were stained brown and diffusely distributed (Fig. 1). In total, 34 (56.67%) patients with
breast cancer were classified as ++ or +++, indicating high levels
of Axl expression. Regarding Axl immunoreactive intensity, 16
patients were classified as negative, 10 as weak, 18 as moderate
and 16 as intense. Furthermore, there were 13 patients with benign
breast lesions exhibiting high expression of Axl, which accounted
for 32.50% of all benign breast lesion cases (13/40). There was a
significant difference in Axl expression between malignant breast
cancer and benign breast lesions (P=0.018; Table III).
 | Figure 1.Immunohistochemical staining of Axl in
breast cancer tissues and benign breast cancer tissues. (A) High
expression of Axl in breast infiltrating ductal carcinoma: Axl
expression was mainly detected in the cytoplasm and cell membrane;
the positive cells were stained brown and diffusely distributed.
(a-1, magnification, ×200; a-2, magnification, ×400). (B and C) Low
expression of Axl in benign breast lesions: (B) Axl expression in
mammary dysplasia (b-1, magnification, ×200; b-2, magnification,
×400); (C) Axl expression in breast fibroadenoma (c-1,
magnification, ×200; c-2, magnification, ×400). Axl,
tyrosine-protein kinase receptor UFO. |
| Table III.Difference of Axl expression between
malignant breast cancer and benign breast lesions. |
Table III.
Difference of Axl expression between
malignant breast cancer and benign breast lesions.
| Axl expression | Breast cancer
(n=60) | Benign breast
lesion (n=40) | χ2 | P-value |
|---|
| High
expression | 34 | 13 | 5.627 | 0.018a |
| Low expression | 26 | 27 |
|
|
Correlation between Axl expression and
clinicopathological characteristics
There was no significant correlation between Axl
expression and age, tumor size, lymph node metastasis, TNM staging,
HER-2, and the expression of Ki67 protein, which is associated with
cell proliferation. However, a significant correlation was observed
between Axl expression and tumor histologic grade, estrogen
receptor (ER) expression and progesterone receptor (PR) expression
(P=0.033, P=0.028, P=0.007; Table
IV). Increased expression of Axl in luminal breast cancer was
observed in 69.44% (25/36) of cases, and was significantly higher
than positive Axl expression in non-luminal breast cancer which was
37.50% (9/24), (P=0.014; Table IV)
Moreover, Spearman rank correlation demonstrated that Axl
expression was positively correlated with histologic grade
(r=0.275, P=0.034), ER (r=0.284, P=0.028) and PR (r=0.364, P=0.007;
all Table V).
| Table IV.Association between Axl expression
and clinicopathological characteristics in breast cancer
tissues. |
Table IV.
Association between Axl expression
and clinicopathological characteristics in breast cancer
tissues.
|
| Axl expression |
|
|
|---|
|
|
|
|
|
|---|
| Variables | Low expression | High
expression | χ2 | P-value |
|---|
| Age, years |
|
| 0.134 | 0.714 |
|
≤50 | 15 | 18 |
|
|
|
>50 | 11 | 16 |
|
|
| Histological
grade |
|
| 4.533 | 0.033a |
| G1 | 9 | 4 |
|
|
|
G2/G3 | 17 | 30 |
|
|
| Tumor size, cm |
|
| 1.629 | 0.202 |
|
<2 | 8 | 16 |
|
|
| ≥2 | 18 | 18 |
|
|
| Lymph node
status |
|
| 0.008 | 0.930 |
| N0 | 15 | 20 |
|
|
| N+ | 11 | 14 |
|
|
| TNM stage |
|
| 2.267 | 0.322 |
| I | 7 | 12 |
|
|
| II | 11 | 17 |
|
|
|
III | 8 | 5 |
|
|
| ER |
|
| 4.848 | 0.028a |
|
Negative | 15 | 10 |
|
|
|
Positive | 11 | 24 |
|
|
| PR |
|
| 7.186 | 0.007a |
|
Negative | 19 | 13 |
|
|
|
Positive | 7 | 21 |
|
|
| HER-2 |
|
| 0.979 | 0.322 |
|
Negative | 16 | 25 |
|
|
|
Positive | 10 | 9 |
|
|
| Ki-67, % |
|
| 3.279 | 0.070 |
|
≤14 | 5 | 14 |
|
|
|
>14 | 21 | 20 |
|
|
| Molecular
subtype |
|
| 5.984 | 0.014a |
| Luminal
type | 11 | 25 |
|
|
|
Non-luminal type | 15 | 9 |
|
|
| Table V.Spearman rank correlation of Axl
expression with clinicopathological characteristics. |
Table V.
Spearman rank correlation of Axl
expression with clinicopathological characteristics.
|
| Axl |
|
|
|---|
|
|
|
|
|
|---|
| Factors | Low expression | High
expression | r | P-value |
|---|
| Histological
grade |
|
|
|
|
| G1 | 9 | 4 | 0.275 | 0.034a |
| G2/G3 | 17 | 30 |
|
|
| ER status |
|
|
|
|
|
Negative | 15 | 10 | 0.284 | 0.028a |
|
Positive | 11 | 24 |
|
|
| PR status |
|
|
|
|
|
Negative | 19 | 13 | 0.346 | 0.007a |
|
Positive | 7 | 21 |
|
|
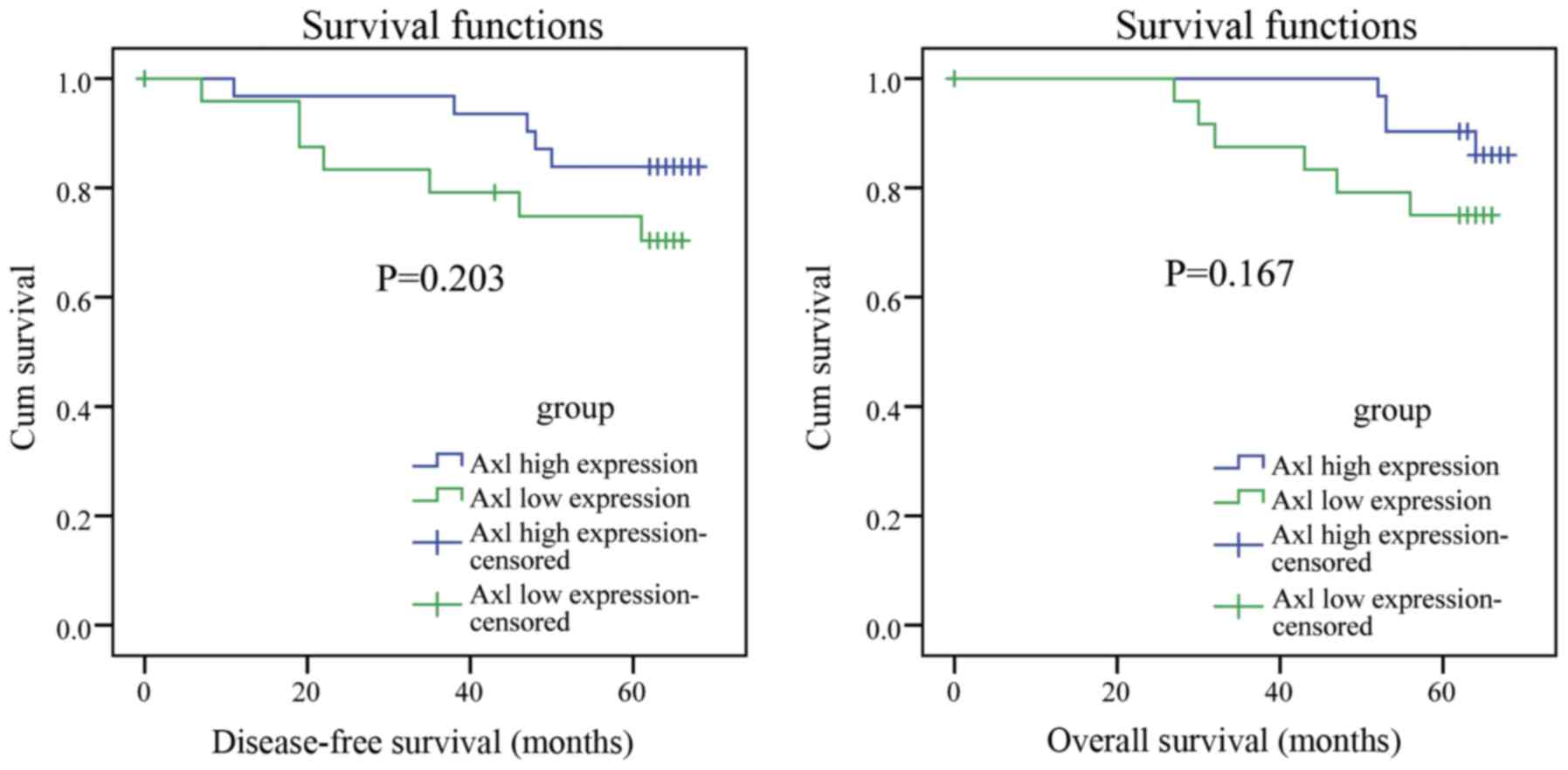
Correlation between Axl expression and
prognosis of patients with breast cancer
In the present study, 5 patients were lost to
follow-up after surgery. In total, 12 cases of
recurrence/metastasis and 10 cases (one patient died in an
accident) of mortality were observed in the follow-up. Kaplan-Meier
survival analysis (Fig. 2)
demonstrated that there were no significant differences between Axl
expression level and DFS/OS (Plog-rank>0.05). Therefore,
it remains unclear whether there is an association between Axl
expression and the OS/DFS of the breast cancer patients.
Cox regression analysis results for
the prognostic factors of the 60 patients with breast cancer
Potential prognostic factors of 60 cases breast
cancer patients were analyzed by the Cox proportional hazard model
to explore the relationship between patient survival and several
explanatory factors. The results demonstrated that HER-2 was the
main factor associated with the DFS of patients with breast cancer
(P=0.013; Table VI). Age and HER-2
were the factors associated with the OS of breast cancer patients
(P=0.037, P=0.017; Table VI).
However there was no significant association between increased Axl
expression and DFS/OS.
| Table VI.Cox regression multi-factor analysis
results for DFS and OS. |
Table VI.
Cox regression multi-factor analysis
results for DFS and OS.
| Factors | B | SE | Wald | df | P-value | OR | 95% CI |
|---|
| DFS |
|
|
|
|
|
|
|
|
HER-2 | 1.525 | 0.613 | 6.184 | 1 | 0.013a | 4.597 | 1.381–15.296 |
| OS |
|
|
|
|
|
|
|
|
Age | 1.504 | 0.721 | 4.352 | 1 | 0.037a | 4.502 | 1.095–18.503 |
|
HER-2 | 1.591 | 0.668 | 5.670 | 1 | 0.017a | 4.907 | 1.325–18.175 |
Discussion
The enhanced expression of Axl has been reported in
different types of cancer, indicating that Axl may be important in
the onset and progression of malignant tumors. Axl is a member of
the TAM receptor tyrosine kinase subfamily, which regulates a
series of pathophysiological processes including cell
proliferation, migration, invasion, cytokine release and apoptosis
(22–24). Furthermore, Holland et al
(25) have demonstrated that Axl is
essential for endothelial cell proliferation, migration, lumen
formation, and angiogenesis regulation in tumor formation, which
supports tumor progression.
In the present study, Axl expression was assessed by
analysing samples taken from patients with breast cancer. The
results indicated that Axl expression was significantly upregulated
in breast cancer cells compared with benign breast lesions (mammary
dysplasia and breast fibroadenoma), which is consistent with the
results from a previous study by Berclaz et al (26). Therefore, increased Axl expression may
facilitate tumorigenesis and the progression of breast cancer.
Furthermore, it may be developed as a method of distinguishing
between malignant and benign breast lesions.
The current study demonstrates that Axl
overexpression correlates with histological grade in breast cancer.
Ahmed et al (27) previously
suggested that increased Axl expression was associated with the
malignant grade of breast cancer. However, the current study did
not find any association between Axl overexpression and other
invasive indicators, such as tumor size, lymph node metastasis, TNM
staging, HER-2, and Ki-67.
The results of previous studies are conflicting
regarding the association between Axl expression and ER status in
breast cancer. D'Alfonso et al (28) investigated 569 cases of breast cancer
and suggested that there was no relationship between Axl expression
and ER status. Ahmed et al (27) reported that high expression of Axl was
associated with ER negativity, whereas, Berclaz et al
(26) suggested that Axl expression
was significantly associated with ER status; Axl expression was
confined to ER positive tumors, however, not all ER positive tumors
expressed the Axl protein. It was therefore hypothesized that ER
mediates the upregulation and activation of Axl, and inhibits cell
apoptosis by overexpressing Bcl-2 (an anti-apoptotic gene), leading
to the malignant characteristics observed in tumor cells (26).
The results of the current study were similar to
those obtained by Berclaz et al (26), however, a minority of ER negative
tumors were also identified as overexpressing Axl. The link between
Axl expression and ER status remains contentious, and further
research investigating larger samples are warranted.
The current study demonstrated that Axl expression
is positively correlated with PR status. This differs from the
results of previous studies (26,27), and
suggests that there is a relationship between Axl expression and PR
status. However, the mechanism behind this relationship remains
unclear. Furthermore, it was demonstrated that Axl expression was
higher in cases of luminal breast cancer than non-luminal cases,
contrary to previous reports by Ahmed et al (27) and Neve et al (29). This may be due to the association
between luminal subtype and ER status in breast cancer.
Patient follow-up demonstrated that there was no
correlation between Axl expression and the prognosis of breast
cancer, contrary to previous reports (26). This suggests that Axl expression is
not associated with the clinical outcome of luminal and non-luminal
type breast cancer. However, a correlation between Axl expression
and breast cancer prognosis may indeed exist. The follow-up time in
the present study was short, as the 5-year survival rate of
patients with breast cancer is relatively high [currently 90.6% for
those diagnosed in 2006 (30)]. A
larger sample size with a longer follow-up time is required to make
more concrete conclusions. Non-luminal (triple-negative and Basal)
breast cancer is clinically more aggressive, with higher rates of
recurrence and worse prognostic outcomes, compared with other types
of breast cancer (31–33). The current study demonstrated that Axl
expression was higher in luminal type breast cancer and positively
correlated with histological grade. Luminal breast cancer often
presents a better prognostic outcome, however the cancer
histological grade positively correlates with tumor malignancy.
Therefore, further study is required to determine whether there is
a significant association between expression of Axl and the
prognosis of patients with luminal type breast cancer.
In conclusion, the present study demonstrated that
Axl is highly expressed in breast cancer tissues and is associated
with poorly differential tumors, indicating that it serves an
important role in the carcinogenesis and development of breast
cancer. High Axl expression was significantly correlated with ER
and PR status, indicating that Axl may contribute to the
upregulation of ER and PR. However, its exact mechanism of action
warrants further investigation. No obvious connection was
demonstrated between levels of Axl expression and the prognosis of
patients with breast cancer. Whether Axl expression is correlated
with the prognosis of luminal type breast cancer patients requires
further investigation. In the future, if a significant correlation
is proven; Axl may be a promising biomarker for breast cancer
malignancy and prognosis.
References
|
1
|
Al-Muhtaseb S: Serum and saliva protein
levels in females with breast cancer. Oncol Lett. 8:2752–2756.
2014.PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2016. CA Cancer J Clin. 66:7–30. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen W, Zheng R, Zhang S, Zhao P, Zeng H
and Zou X: Report of cancer incidence and mortality in China, 2010.
Ann Transl Med. 2:612014.PubMed/NCBI
|
|
4
|
O'Bryan JP, Frye RA, Cogswell PC, Neubauer
AA, Kitch B, Prokop C, Espinosa R III, Le Beau M, Earp HT and Liu
ET: axl, a transforming gene isolated from primary human myeloid
leukemia cells, encodes a novel receptor tyrosine kinase. Mol Cell
Biol. 11:5016–5031. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Korshunov V: Axl-dependent signalling: A
clinical update. Clin Sci (Lond). 122:361–368. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Li Y, Jia L, Ren D, Liu C, Gong Y, Wang N,
Zhang X and Zhao Y: Axl mediates tumor invasion and
chemosensitivity through PI3K/Akt signaling pathway and is
transcriptionally regulated by slug in breast carcinoma. IUBMB
Life. 66:507–518. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yanagita M, Arai H, Nakano T, Ohashi K,
Mizuno K, Fukatsu A, Doi T and Kita T: Gas6 induces mesangial cell
proliferation via latent transcription factor STAT3. J Biol Chem.
276:42364–42369. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tai K, Shieh Y, Lee C, Shiah S and Wu C:
Axl promotes cell invasion by inducing MMP-9 activity through
activation of NF-kappaB and Brg-1. Oncogene. 27:4044–4055. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lim J and Thiery J: Epithelial-mesenchymal
transitions: Insights from development. Development. 139:3471–3486.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wu CW, Li AF, Chi CW, Lai CH, Huang CL, Lo
SS, Lui WY and Lin WC: Clinical significance of AXL kinase family
in gastric cancer. Anticancer Res. 22:1071–1078. 2002.PubMed/NCBI
|
|
11
|
Ishikawa M, Sonobe M, Nakayama E,
Kobayashi M, Kikuchi R, Kitamura J, Imamura N and Date H: Higher
expression of receptor tyrosine kinase Axl, and differential
expression of its ligand, Gas6, predict poor survival in lung
adenocarcinoma patients. Ann Surg Oncol. 20:(Suppl 3). S467–S476.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sayan A, Stanford R, Vickery R, Grigorenko
E, Diesch J, Kulbicki K, Edwards R, Pal R, Greaves P,
JarielEncontre I, et al: Fra-1 controls motility of bladder cancer
cells via transcriptional upregulation of the receptor tyrosine
kinase AXL. Oncogene. 31:1493–1503. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Avilla E, Guarino V, Visciano C, Liotti F,
Svelto M, Krishnamoorthy G, Franco R and Melillo R: Activation of
TYRO3/AXL tyrosine kinase receptors in thyroid cancer. Cancer Res.
71:1792–1804. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Koorstra JB, Karikari CA, Feldmann G,
Bisht S, Rojas PL, Offerhaus GJ, Alvarez H and Maitra A: The Axl
receptor tyrosine kinase confers an adverse prognostic influence in
pancreatic cancer and represents a new therapeutic target. Cancer
Biol Ther. 8:618–626. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Craven RJ, Xu LH, Weiner TM, Fridell YW,
Dent GA, Srivastava S, Varnum B, Liu ET and Cance WG: Receptor
tyrosine kinases expressed in metastatic colon cancer. Int J
Cancer. 60:791–797. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wu W, Bi C, Credille KM, Manro JR, Peek
VL, Donoho GP, Yan L, Wijsman JA, Yan SB and Walgren RA: Inhibition
of tumor growth and metastasis in non-small cell lung cancer by
LY2801653, an inhibitor of several oncokinases, including MET. Clin
Cancer Res. 19:5699–5710. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mahadevan D, Cooke L, Riley C, Swart R,
Simons B, Croce K Della, Wisner L, Iorio M, Shakalya K, Garewal H,
et al: A novel tyrosine kinase switch is a mechanism of imatinib
resistance in gastrointestinal stromal tumors. Oncogene.
26:3909–3919. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Martinelli E, Martini G, Cardone C,
Troiani T, Liguori G, Vitagliano D, Napolitano S, Morgillo F,
Rinaldi B, Melillo R, et al: AXL is an oncotarget in human
colorectal cancer. Oncotarget. 6:23281–23296. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Edge SB, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: AJCC cancer staging manual. 649. Springer;
New York: 2010
|
|
20
|
Goldhirsch A, Winer EP, Coates AS, Gelber
RD, PiccartGebhart M, Thurlimann B and Senn HJ: Panel members:
Personalizing the treatment of women with early breast cancer:
Highlights of the St Gallen International Expert Consensus on the
Primary Therapy of Early Breast Cancer 2013. Ann Oncol.
24:2206–2223. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Carlson RW, Moench SJ, Hammond ME, Perez
EA, Burstein HJ, Allred DC, Vogel CL, Goldstein LJ, Somlo G,
Gradishar WJ, et al: HER2 testing in breast cancer: NCCN Task Force
report and recommendations. J Natl Compr Canc Netw. 4:(Suppl 3).
S1–S22; quiz S23-S24. 2006.
|
|
22
|
Shiozawa Y, Pedersen EA, Patel LR, Ziegler
AM, Havens AM, Jung Y, Wang J, Zalucha S, Loberg RD, Pienta KJ and
Taichman RS: GAS6/AXL axis regulates prostate cancer invasion,
proliferation and survival in the bone marrow niche. Neoplasia.
12:116–127. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Song X and Wang H, Logsdon CD, Rashid A,
Fleming JB, Abbruzzese JL, Gomez HF, Evans DB and Wang H:
Overexpression of receptor tyrosine kinase Axl promotes tumor cell
invasion and survival in pancreatic ductal adenocarcinoma. Cancer.
117:734–743. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bellosta P, Zhang Q, Goff S and Basilico
C: Signaling through the ARK tyrosine kinase receptor protects from
apoptosis in the absence of growth stimulation. Oncogene.
15:2387–2397. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Holland SJ, Powell MJ, Franci C, Chan EW,
Friera AM, Atchison RE, McLaughlin J, Swift SE, Pali ES, Yam G, et
al: Multiple roles for the receptor tyrosine kinase axl in tumor
formation. Cancer Res. 65:9294–9303. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Berclaz G, Altermatt HJ, Rohrbach V,
Kieffer I, Dreher E and Andres AC: Estrogen dependent expression of
the receptor tyrosine kinase axl in normal and malignant human
breast. Ann Oncol. 12:819–824. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ahmed L, Nalwoga H, Arnes J, Wabinga H,
Micklem D and Akslen L: Increased tumor cell expression of Axl is a
marker of aggressive features in breast cancer among African women.
APMIS. 123:688–696. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
D'Alfonso TM, Hannah J, Chen Z, Liu Y,
Zhou P and Shin SJ: Axl receptor tyrosine kinase expression in
breast cancer. J Clin Pathol. 67:690–696. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Neve R, Chin K, Fridlyand J, Yeh J,
Baehner F, Fevr T, Clark L, Bayani N, Coppe J, Tong F, et al: A
collection of breast cancer cell lines for the study of
functionally distinct cancer subtypes. Cancer Cell. 10:515–527.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chen L, Linden H, Anderson B and Li C:
Trends in 5-year survival rates among breast cancer patients by
hormone receptor status and stage. Breast Cancer Res Treat.
147:609–616. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Haffty B, Yang Q, Reiss M, Kearney T,
Higgins S, Weidhaas J, Harris L, Hait W and Toppmeyer D:
Locoregional relapse and distant metastasis in conservatively
managed triple negative early-stage breast cancer. J Clin Oncol.
24:5652–5657. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Dent R, Trudeau M, Pritchard KL, Hanna WM,
Kahn HK, Sawka CA, Lickley LA, Rawlinson E, Sun P and Narod SA:
Triple-negative breast cancer: Clinical features and patterns of
recurrence. Clin Cancer Res. 13:4429–4434. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Rakha E, ElSayed M, Green A, Lee A,
Robertson J and Ellis I: Prognostic markers in triple-negative
breast cancer. Cancer. 109:25–32. 2007. View Article : Google Scholar : PubMed/NCBI
|