Introduction
Gastric cancer (GC) (1) is divided, according to the
classification of Lauren (2), into
intestinal, diffuse and mixed subtypes. In Western countries, GC
has exhibited a decreased incidence primarily as a result of
improvements in hygiene and food conservation in the last 50 years
(3). However, this decline holds true
essentially for the intestinal histotype only, whereas the
incidence rate of diffuse GC (DGC) is relatively stable (1).
Intestinal GC is generally associated with chronic
inflammation, and is frequently associated with chronic infection
by Helicobacter pylori (4).
Conversely, DGC is not associated with chronic inflammation. This
is certainly the case for patients with hereditary DGC (HDGC)
(5).
HDGC syndrome is defined on the basis of family
history of DGC, early onset of the disease or presence of DGC
associated with lobular breast cancer (LBC). The genetic alteration
linked to this syndrome is a germline mutation of the E-cadherin 1
(CDH1) gene. Its product, endothelial cadherin, is an
adhesion molecule crucial for maintaining epithelial cell polarity
and architectural structure (6). The
syndrome is characterized by an autosomal dominant transmission and
requires a second ‘hit’ (mutation, loss of heterozygosity,
methylation) to inactivate the wild-type allele (7–9).
Hereditary cancer syndromes are rare compared with
sporadic cancer, but their investigation is crucial, due to
different clinical management that mutation carriers warrant and
the implications for the disease-free relatives (6).
In the present study, two families are described who
were identified in a screening and genetic counseling program for
HDGC.
Case report
Subjects
Subjects who matched the HDGC condition based on the
criteria of Brooks-Wilson et al (10) and agreed to undergo genetic testing
signed an informed consent declaration and received genetic
counseling.
Molecular characterization
A mutational screening of the CDH1 gene was
previously carried out by complementary molecular approaches
including DNA sequencing, multiplex ligation-dependent probe
amplification, single-nucleotide primer extension, bisulfite
sequencing, reverse transcription-polymerase chain reaction and
bioinformatics tools (11). During
that screening, a c.688-1G>C mutation affecting mRNA splicing
and leading to a premature termination codon were identified in
case 1, whereas an intragenic deletion of exons 7 and 8 were
identified in case 2 (11).
Pathology
Biopsy and surgical specimens were fixed in 10%
neutral-buffered formalin (DDK Italia, Milan, Italy), equivalent to
~4% formaldehyde solution for 1–5 h at room temperature and
subsequently for another 5 h at 37°C. Following fixation, tissue
samples were dehydrated in an ethanol/xylene series and embedded
using fresh paraffin wax maintained at 55–60°C. Once embedded in
paraffin wax, samples were stored at room temperature (20–25°C)
prior to sectioning. Consecutive serial sections (4 µm) were cut
from the tissue block immediately prior to testing. Sections were
mounted on slides and dried for 12–24 h at room temperature or 1 h
at 60°C. Sections were subsequently deparaffinized and rehydrated
in a xylene/ethanol series. Histology was confirmed with
hematoxylin and eosin staining. Briefly, hematoxylin and eosin
staining was performed using a semi-automated instrument Tissue-Tek
Sakura (Sakura Finetek Europe B.V., Flemingweg, Netherlands) using
hematoxylin obtained from Bio Optica Milano SpA (Milan, Italy) and
eosin obtained from BDH Analytical Chemicals (Radnor, PA, USA).
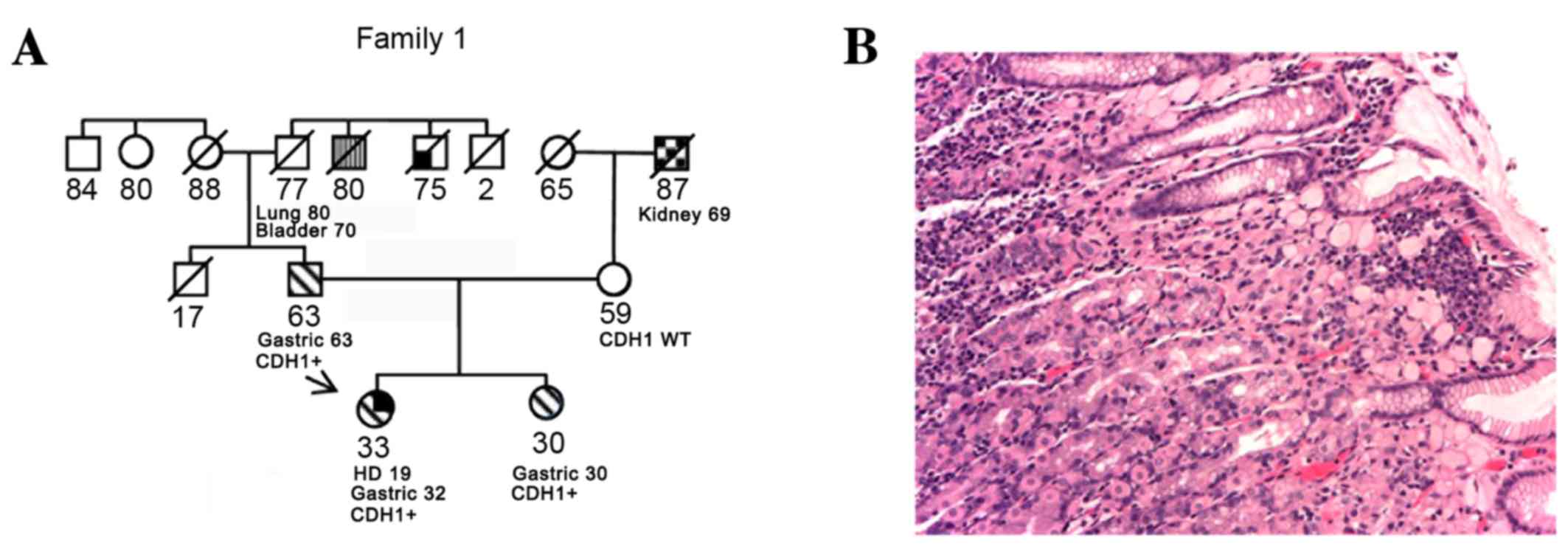
Case 1
A 32 years old female was diagnosed with Hodgkin's
lymphoma at 19 years of age, and was treated with mantle
radiotherapy and chemotherapy (Adriamycin, bleomycin, vinblastine
and dacarbazine), with no relapses. At 32 years of age, she
received a diagnosis of DGC and was treated with total gastrectomy
[final stage pT3 pN1 G4 (p, pathology; T, tumor; N, node; G,
grade)] followed by chemotherapy with 6 cycles of capecitabine and
oxaliplatin. A local relapse was detected using computed
tomography, 18 months following chemotherapy. The patient was
treated with a surgical resection of the left colic flexure,
surrenectomy and splenectomy. A second line of chemotherapy was
initiated with 8 cycles of irinotecan and capecitabine. Even though
the pedigree was silent at that time, due to her young age, she was
offered genetic counseling and was tested for CDH1. The
results revealed a pathogenic splicing mutation (11). As there was no family history of
gastric cancer, her parents were tested. Her 63-year-old father was
identified to be a carrier of the same mutation; subsequently, her
30-year-old sister was tested and was also found to be a carrier of
the same mutation. Both relatives underwent gastroscopy, according
to the gastroscopy protocol for mutation carriers, which included
36 random biopsies, 6 for each gastric anatomical region. All of
the father's tissue samples were negative, whereas the sister had a
positive sample for signet ring gastric cancer (SRGC). She
underwent total gastrectomy with a subsequent diagnosis of SRGC of
the cardia and gastric body (pT1a pN0 G3). The father elected to
monitor the stomach annually instead of undergoing a prophylactic
gastrectomy. At his second endoscopic assessment, one biopsy sample
was identified to be positive for SRGC. At the final pathological
report following total gastrectomy, DGC of pT1a pN0 G2 of the
fundus was identified (Fig. 1).
The sisters were included in an intensive
breast-screening program with mammography ultrasound and magnetic
resonance imaging.
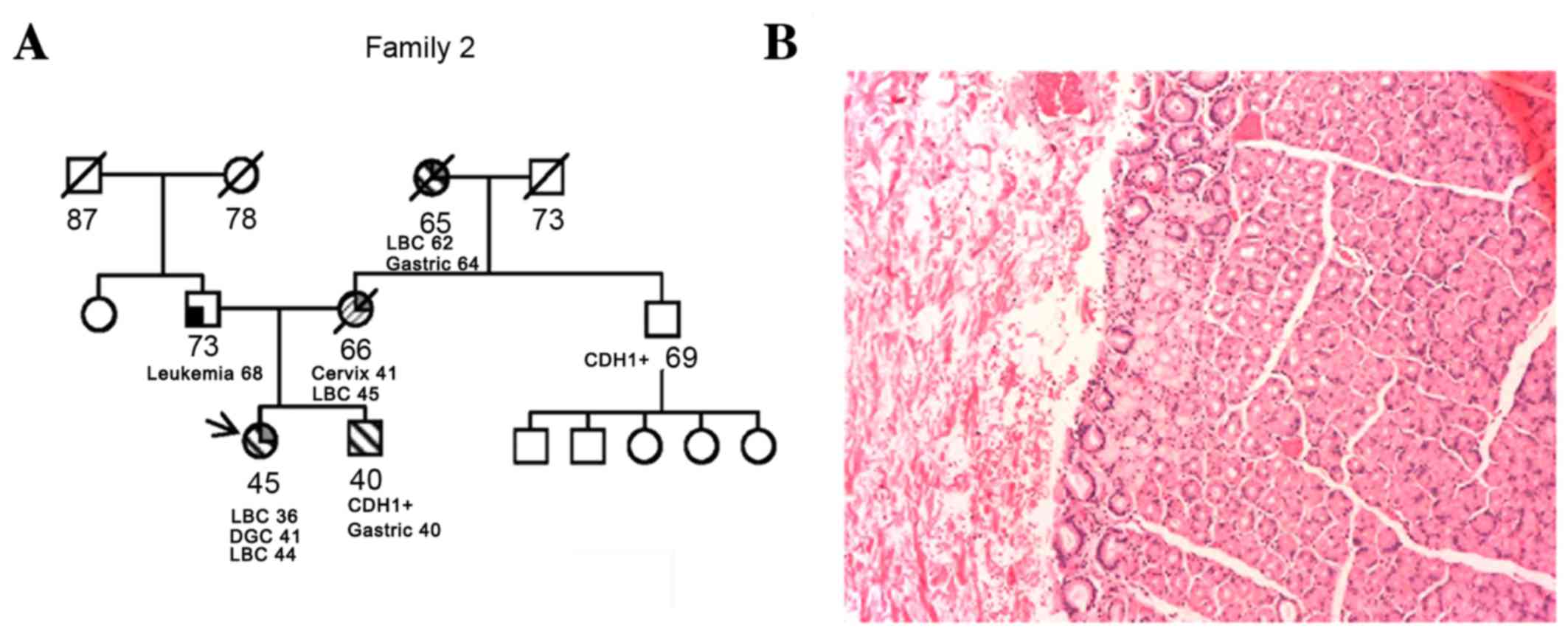
Case 2
A 36-year-old female was diagnosed with LBC at 36
years of age, and underwent a nipple-sparing mastectomy. The final
pathological staging was pT1c pN0 G2 LBC, estrogen- and
progesterone-receptor positive, human epidermal growth factor
2/neu-negative and 15% proliferation marker protein Ki-67. As
adjuvant treatment, the patient received 5 years of tamoxifen and
ovarian suppression with luteinizing hormone-releasing hormone
analogue. Due to the patient's young age and family history (her
mother and grandmother were also diagnosed with LBC at 45 and 62
years of age, respectively), she was offered genetic counseling and
tested for breast cancer susceptibility genes 1 and 2, which were
shown to be wild-type. As her maternal grandmother was diagnosed
with DGC at 64 years of age, documented with a pathological report,
a CDH1 molecular test was performed. This test revealed a
pathogenic deletion of exons 7–8 of CDH1 (11). The patient underwent gastroscopy with
36 random biopsies, all of which were negative. Following genetic
counseling, she decided to undergo prophylactic gastrectomy. The
final pathological report post-surgery was positive for a small
SRGC pT1a pN0 G3. The family history suggested that the mutation
was inherited from the mother's side (the mother was already
deceased). The molecular test was proposed to the brother and the
maternal uncle. Results identified that each of these relatives
were carriers of the same deletion. The 41-year-old brother
underwent a gastroscopy that exhibited positivity for SRGC, with a
final post-total gastrectomy staging of pT1a pN0 G3 (Fig. 2). The patient's 69-year-old uncle was
completely asymptomatic and declined to undergo gastroscopy. At a
subsequent follow-up visit by the female patient, the proband was
diagnosed with a contralateral LBC and the patient underwent a
mastectomy with a pathological report of a pT1c pN0 G2 LBC.
Discussion
Families in whom a deleterious genetic mutation runs
require genetic counseling, clinical surveillance and the possible
recommendation of prophylactic surgery. HDGC is characterized by a
lifetime DGC risk of 80% in males and 90% in females, combining the
risk of DGC and LBC (12,13).
In Case 1, the family is notably similar to another
case where a different de novo CDH1 mutation was reported
and the proband also exhibited a previous Hodgkin's lymphoma
(14). Although conclusions cannot be
drawn from only two cases, it may be hypothesized that HDGC has an
increased sensitivity to radiation damage, with rapid onset of the
disease after radiotherapy, a condition well documented in
Li-Fraumeni syndrome (15).
In Case 2, an essential point is the degree of
thoroughness warranted when reconstructing family history in order
to perform the appropriate molecular tests. Indeed, it is
increasingly evident that LBC can be developed in carriers of the
CDH1 mutation (16,17).
A number of issues require addressing. One is the
role of screening gastroscopy, as the nature of DGC makes it
difficult to observe cancer lesions at the gastric mucosa level,
and multiple random biopsies may not detect an early GC. On the
other hand, it is not clear when these early lesions may progress
to the point where they become clinically relevant. This issue is
crucial and should be comprehensively examined, in order to better
counsel whether and when to pursue prophylactic surgery.
Furthermore, the time between the initiation of the carcinogenesis
process and clinically relevant cancer may allow chemopreventive
strategies to be developed and undertaken, even though, compared
with other organs, far fewer studies have been performed and few
hypotheses have been drawn which focus on sporadic GC (18,19).
Another issue is the prognosis of these tumors. It has been
suggested that a generic family history for GC may define a less
aggressive cancer, compared with the pure sporadic cancer (20,21);
however, recently, overall survival rate of CDH1 mutation
carriers has been indicated to be worse compared with patients
exhibiting wild-type CDH1, with 4 vs. 13% for 5-year
survival rate (22).
On the basis of the two cases reported in the
present study, the importance of young age at cancer diagnosis
should be underlined, even in a family with no known history of
cancer, and genetic testing for LBC must be considered, even though
the proband may not meet the most stringent selection criteria
(10,17,22).
A better knowledge of the natural history of
diseases that develop in CDH1 carriers may assist in
improving the counseling process and the development of preventive
strategies in order to delay, or even circumvent, prophylactic
gastrectomy or any other prophylactic surgery.
Acknowledgements
The authors of the present study would like to
acknowledge support from the Italian Ministry of Health. M.M. was a
recipient of a Giovanni Magni postdoctoral fellowship from the
Adriano Buzzati-Traverso Foundation.
References
|
1
|
Crew KD and Neugut AI: Epidemiology of
gastric cancer. World J Gastroenterol. 12:354–362. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lauren P: The two histological main types
of gastric carcinoma: Diffuse and so-called intestinal-type
carcinoma. An attempt at a histo-clinical classification. Acta
Pathol Microbiol Scand. 64:31–49. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Howson CP, Hiyama T and Wynder EL: The
decline in gastric cancer: Epidemiology of an unplanned triumph.
Epidemiol Rev. 8:1–27. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sepulveda AR: Helicobacter, Inflammation,
and Gastric Cancer. Curr Pathobiol Rep. 1:9–18. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yakirevich E and Resnick MB: Pathology of
gastric cancer and its precursor lesions. Gastroenterol Clin North
Am. 42:261–284. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kluijt I, Siemerink EJ, Ausems MG, van Os
TA, de Jong D, Simões-Correia J, van Krieken JH, Ligtenberg MJ,
Figueiredo J, van Riel E, et al: CDH1-related hereditary diffuse
gastric cancer syndrome: Clinical variations and implications for
counseling. Int J Cancer. 131:367–376. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Humar B, Blair V, Charlton A, More H,
Martin I and Guilford P: E-cadherin deficiency initiates gastric
signet-ring cell carcinoma in mice and man. Cancer Res.
69:2050–2056. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Oliveira C, Sousa S, Pinheiro H, Karam R,
Bordeira-Carrico R, Senz J, Kaurah P, Carvalho J, Pereira R, Gusmão
L, et al: Quantification of epigenetic and genetic 2nd hits in CDH1
during hereditary diffuse gastric cancer syndrome progression.
Gastroenterology. 136:2137–2148. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nakayama S, Sasaki A, Mese H, Alcalde RE,
Tsuji T and Matsumura T: The E-cadherin gene is silenced by CpG
methylation in human oral squamous cell carcinomas. Int J Cancer.
93:667–673. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Brooks-Wilson AR, Kaurah P, Suriano G,
Leach S, Senz J, Grehan N, Butterfield YS, Jeyes J, Schinas J,
Bacani J, et al: Germline E-cadherin mutations in hereditary
diffuse gastric cancer: Assessment of 42 new families and review of
genetic screening criteria. J Med Genet. 41:508–517. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Molinaro V, Pensotti V, Marabelli M,
Feroce I, Barile M, Pozzi S, Laghi L, Serrano D, Bernard L, Bonanni
B and Ranzani GN: Complementary molecular approaches reveal
heterogeneous CDH1 germline defects in Italian patients with
hereditary diffuse gastric cancer (HDGC) syndrome. Genes
Chromosomes Cancer. 53:432–445. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Pharoah PD, Guilford P and Caldas C:
International Gastric Cancer Linkage Consortium: Incidence of
gastric cancer and breast cancer in CDH1 (E-cadherin) mutation
carriers from hereditary diffuse gastric cancer families.
Gastroenterology. 121:1348–1353. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kaurah P, MacMillan A, Boyd N, Senz J, De
Luca A, Chun N, Suriano G, Zaor S, Van Manen L, Gilpin C, et al:
Founder and recurrent CDH1 mutations in families with hereditary
diffuse gastric cancer. JAMA. 297:2360–2372. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shah MA, Salo-Mullen E, Stadler Z, Ruggeri
JM, Mirander M, Pristyazhnyuk Y and Zhang L: De novo CDH1 mutation
in a family presenting with early-onset diffuse gastric cancer.
Clin Genet. 82:283–287. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Salmon A, Amikam D, Sodha N, Davidson S,
Basel-Vanagaite L, Eeles RA, Abeliovich D and Peretz T: Rapid
development of post-radiotherapy sarcoma and breast cancer in a
patient with a novel germline ‘de-novo’ TP53 mutation. Clin Oncol
(R Coll Radiol). 19:490–493. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
McVeigh TP, Choi JK, Miller NM, Green AJ
and Kerin MJ: Lobular breast cancer in a CDH1 splice site mutation
carrier: Case report and review of the literature. Clin Breast
Cancer. 14:e47–e51. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Corso G, Figueiredo J, Biffi R, Trentin C,
Bonanni B, Feroce I, Serrano D, Cassano E, Annibale B, Melo S, et
al: E-cadherin germline mutation carriers: Clinical management and
genetic implications. Cancer Metastasis Rev. 33:1081–1094. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Tan VP and Wong BC: Gastric cancer
chemoprevention: The current evidence. Gastroenterol Clin North Am.
42:299–316. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yadav SK, Sah AK, Jha RK, Sah P and Shah
DK: Turmeric (curcumin) remedies gastroprotective action.
Pharmacogn Rev. 7:42–46. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yatsuya H, Toyoshima H, Mizoue T, Kondo T,
Tamakoshi K, Hori Y, Tokui N, Hoshiyama Y, Kikuchi S, Sakata K, et
al: Family history and the risk of stomach cancer death in Japan:
Differences by age and gender. Int J Cancer. 97:688–694. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Han MA, Oh MG, Choi IJ, Park SR, Ryu KW,
Nam BH, Cho SJ, Kim CG, Lee JH and Kim YW: Association of family
history with cancer recurrence and survival in patients with
gastric cancer. J Clin Oncol. 30:701–708. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
van der Post RS, Vogelaar IP, Manders P,
van der Kolk LE, Cats A, van Hest LP, Sijmons R, Aalfs CM, Ausems
MG, Gómez Garcia EB, et al: Accuracy of hereditary diffuse gastric
cancer testing criteria and outcomes in patients with a germline
mutation in CDH1. Gastroenterology. 149:897–906.e19. 2015.
View Article : Google Scholar : PubMed/NCBI
|