Introduction
Lung cancer continues to be a leading cause of
mortality in the western world (1).
The primary cause of mortality even following successful resection
of the primary tumour is metastatic spread (1,2). One major
route for lung cancer metastatic spread is the movement of
displaced cells through the circulation to distant sites (3). Circulating tumour cells (CTCs) are cells
that shed from the primary tumour and have been detected in the
peripheral blood of patients with cancer. Previous studies have
revealed that CTCs are heavily implicated in metastatic spread
(3,4).
Understanding CTC biology has become a fundamental part of cancer
research, as diagnostic blood assays for cancer are an area of
growing interest. A number of studies have presented evidence of
the utility of CTCs as potential cancer biomarkers for diagnostic
and prognostic purposes, which may serve as a minimally invasive
‘liquid biopsy’ for real-time diagnosis (5–7).
Therefore, the ability to isolate and evaluate these CTCs may allow
for a new method of cancer staging and to predict which patients
may exhibit an improved response to systemic treatments as opposed
to surgical excision alone.
Although blood to the lungs is supplied by the
pulmonary and bronchial arteries, the bronchial veins account for
very little venous drainage, with almost all blood returning to the
heart through the pulmonary veins. This single route for venous
drainage provides an excellent model for the assessment of CTCs,
through sampling blood returning from the tumour-bearing lobe to
the main circulation. Despite being a naturally effective model for
the study of CTCs, little is known regarding the presence of CTCs
in the blood draining from the tumour-bearing lobe and their
long-term impact on survival.
The aim of the current study was to quantify the
concentration of CTCs in blood obtained from the pulmonary vein and
from simultaneously assessed peripheral blood in patients with
detectable lung cancer. Other goals of the present study were to
determine the association between CTC detection and cancer stage,
histology, lung manipulation and other clinical parameters.
Materials and methods
Cell culture
A549 human lung carcinoma cells (American Type
Culture Collection, Manassas, VA, USA) were grown in advanced
Dulbecco's modified Eagle's medium (DMEM) containing high glucose,
non-essential amino acids, sodium pyruvate, phenol red and no
L-glutamine (Gibco; Thermo Fisher Scientific, Inc., Waltham, MA,
USA). The advanced DMEM was further supplemented with 1% (v/v)
penicillin and streptomycin solution (Invitrogen; Thermo Fisher
Scientific, Inc.) and 10% (v/v) foetal bovine serum (Invitrogen;
Thermo Fisher Scientific, Inc.). All cell cultures were maintained
in a humidified atmosphere in an incubator at 37°C containing 5%
CO2, with media being changed every 48 h to ensure
optimal growth.
Patients
Ethical approval was sought and granted for the
present study from the National Research Ethics Service, now the
Health Research Authority (reference no. 14/LO/1284). Patients
awaiting radical resection of primary non-small cell carcinoma of
the lung were recruited from Harefield Hospital (Royal Brompton and
Harefield Trust, Middlesex, UK) following informed consent.
Ten patients aged between 50 and 84 years old (mean
age, 64 years old) were enrolled between November 2014 and June
2015. Five patients were male and five were female. Seven patients
had a history of heavy cigarette smoking, with three having never
smoked. Two patients had known, although minimal, previous asbestos
exposure. No patients had received therapeutic or neoadjuvant
oncological treatments prior to surgery for lung cancer. Between
the patients, five tumours were located in the right lung (two
upper lobe, one middle lobe, 2 lower lobe) and five in the left (3
upper lobe, two lower lobe). Eight tumours were identified as
adenocarcinomas and two as squamous cell carcinomas. Tumours were
resected at various stages, with three staged at Ia, two at Ib, one
at IIa, three at IIb and one at IIIa. No patients had detectable
distant metastatic disease at resection. Nine patients underwent a
pulmonary lobectomy, with two procedures performed
thoracoscopically. One patient underwent a planned pneumonectomy.
In all cases the pulmonary vein was ligated prior to division of
pulmonary artery branches or bronchus.
All blood samples were taken in the operating
theatre after the patient was anaesthetised and the process is
illustrated in Fig. 1. Briefly, the
baseline sample was taken from a peripheral vein or artery prior to
the incision. Following intraoperative assessment of surgical
resectability, a second sample was collected from the pulmonary
vein draining the lobe-bearing tumour prior to the surgical
division of the pulmonary vein. When the planned surgical
intervention with systematic lymph dissection was completed, a
third sample was collected from the pulmonary vein stump. A final
sample was obtained three days postoperatively from the peripheral
vein, together with routine clinical blood sampling.
Processing of blood samples using
ScreenCell®
ScreenCell® filtration device technology
(ScreenCell, Paris, France) was utilised as previously described
(1). Blood sample processing is
illustrated in Fig. 1. Briefly, all
blood samples were collected in 3 ml EDTA bottles, inverted,
incubated in 7 ml of fixative buffer (ScreenCell, Paris, France)
and then filtered through the Cytology ScreenCell® device. Filters
were then separated and captured cells stained with haematoxylin
and eosin (H&E). All H&E stained slides were then viewed by
a consultant pathologist and cells manually counted with a
microscope and documented.
Immuocytochemistry analysis of A549
human lung carcinoma cells
A549 human lung carcinoma cells (America Type
Culture Collection, Manassas, VA, USA) were grown in T75 flasks to
90% confluency. For this proof-of-principle experiment, ~50 A549
cells were inoculated into either 3 ml of blood from a healthy
volunteer or 3 ml of PBS solution with lymphocytes added. In the
latter case, ~50 lymphocytes were taken from healthy volunteer
blood by means of density gradient centrifugation. A549 cells were
collected using the Countess Automated Cell Counter (Invitrogen;
Thermo Fisher Scientific, Inc.) and stained with trypan blue
(Invitrogen; Thermo Fisher Scientific, Inc.). Media was aspirated
from the cells in the flask, which were then incubated with 2 ml of
TrypLE™ Express (Invitrogen; Thermo Fisher Scientific, Inc.) and
manually agitated. The cells were resuspended in 3 ml of
appropriate media to produce a 5 ml cell suspension, of which 1 ml
was removed. An equal volume of cell suspension was mixed with 0.4%
trypan blue stain, which is selectively absorbed by dead cells, and
applied to a Countess™ cell counting chamber slide. Three cell
count readings were obtained and an average value calculated.
Approximately 50 cells were then added to PBS or human blood. The
appropriate volume of cells was washed with 5 ml of PBS
(Invitrogen; Thermo Fisher Scientific, Inc., Waltham, MA, USA), and
then treated with 4% paraformaldehyde on ice for 3 min. The primary
antibody used was a monoclonal mouse anti-human cytokeratin AE1/3
clone (catalogue no., M351529-2; Dako; Agilent Technologies, Inc.,
Santa Clara, CA, USA). A 1:50 dilution was prepared, as instructed
by the ScreenCell® protocol. The antibody was diluted in a solution
of Tris-buffered saline (TBS) and 1% bovine serum albumin
(Invitrogen; Thermo Fisher Scientific, Inc.), and 70 µl of antibody
solution was added to each filter at 4°C overnight. Following
primary antibody incubation, the filters were washed twice for 1
min in TBST (1:10 dilution of Tween-20:TBS). Excess liquid was
blotted and the filters were returned to the humidifying chamber on
slides with 70 µl of horseradish peroxidase (HRP)-conjugated
biotinylated anti-mouse secondary antibody at a 1:1,000 dilution
(catalogue no., K4065; Dako EnVision+ kit; Agilent Technologies,
Inc.) for 40 min at room temperature. Following secondary antibody
incubation, filters were washed twice for 1 min in TBST, and excess
liquid blotted off. A 3,3′-diaminobenzidine (DAB) -chromogen
solution was mixed (20 µl of DAB to 1 ml of DAB solution; Dako
EnVision+ kit) and 70 µl of the solution was added to each filter
prior to incubation for 10 min at room temperature in the
humidifying chamber. This was followed by the washing of filters in
distilled water for 1 min. The filters were then placed on Whatman
paper and allowed to dry at room temperature for 15 min prior to
light microscopy of positively stained cancer cells.
Statistical analysis
Captured data was analysed using GraphPad prism
version 5 (San Diego, CA, USA) with significance set at
P<0.05.
Results
Screening for lung carcinoma cells
with the ScreenCell® filtration device
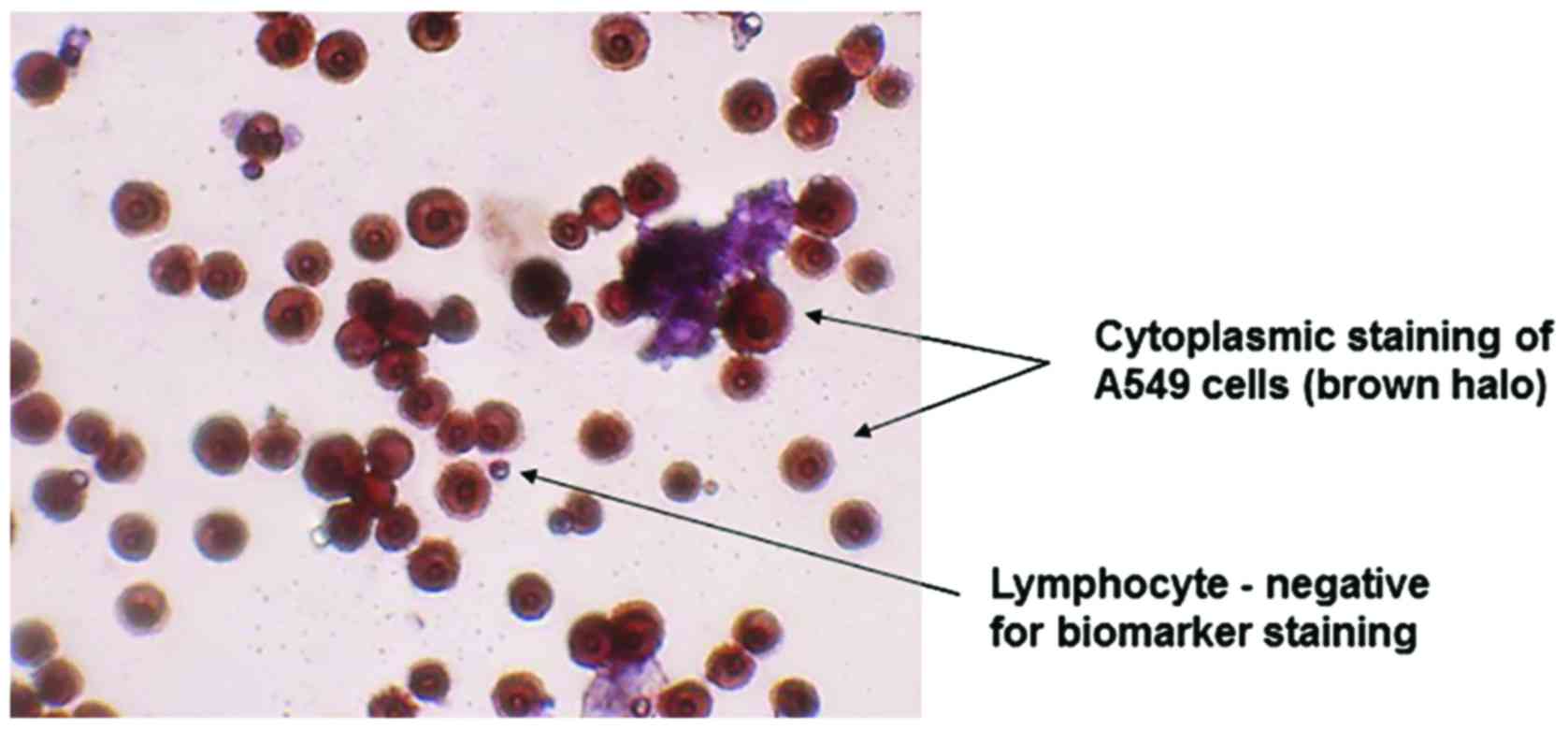
In order to validate the ScreenCell® filtration
device, A549 human lung carcinoma cells were utilised, as this cell
line tests positive for AE1/3. The results of this experiment
identified a strong positive AE1/3 cytoplasmic staining of
inoculated A549 cells, whereas lymphocytes were negative for AE1/3
staining and markedly smaller in size (Fig. 2).
Isolation of CTCs from the blood
samples of patients with lung cancer
Using the ScreenCell® filtration device, CTCs were
detected in 80% of the initial peripheral preoperative blood
samples and 100% of the central pulmonary vein blood samples taken
from the tumour-bearing lobe prior to division (Table I). There was a significant increase
(P=0.04) in the volume of CTCs between the baseline and preligation
sampling (Fig. 3). Occurring in the
majority of patients tested, this finding supports the hypothesis
that the surgical manipulation of the lung, and therefore primary
tumour, results in an increased CTC concentration in the blood.
Following resection, however, this volume quickly returned to a
level close to the baseline, with a range similar to that detected
preoperatively (Fig. 3). There was no
significant change in the volume of CTCs between baseline levels
and either initial post-surgery concentrations (P=0.99) or those
three days postoperatively (P=0.5). All ten patients, regardless of
preoperative levels of CTCs, were observed to have tumour cells in
their peripheral blood three days following resection. Eight
patients were identified to have large clusters of CTCs (>5
cells) in pulmonary vein blood samples following lung manipulation,
with a further patient having smaller clusters. Five of these
patients had no detectable clusters in their baseline sample
(Fig. 4).
 | Table I.Number of CTCs detected at each stage
of the investigation. |
Table I.
Number of CTCs detected at each stage
of the investigation.
|
| Number of detected
CTCs |
|---|
|
|
|
|---|
| Blood sample
type | Mean, n | Range, n | Patients, % |
|---|
| Peripheral vessel
prior to surgery | 22.2 | 0–100 | 80 |
| Pulmonary vein
draining the tumour-bearing lobe prior to resection | 65.1 | 8–200 | 100 |
| Pulmonary vein
following resection | 19.4 | 0–100 | 80 |
| Peripheral vessel 3
days post-resection | 23.5 | 2–100 | 100 |
There was no significant difference between the mean
number of CTCs detected in squamous cell carcinoma or
adenocarcinoma (P=0.71) and no difference in the mean number of
CTCs between current smokers, ex-smokers and non-smokers (P=0.89)
(data not shown). The number of CTCs collected at any stage of
surgery had no correlation with the nodal status of the patient,
tumour size or overall staging of the tumour (data not shown).
At the end of the study, nine patients were alive
and disease-free. One patient succumbed to heart disease >1 year
following the surgery. The same patient was identified to have a
metastatic deposit of lung cancer in the femur prior to death. The
post-resection pathological staging of this patient's
adenocarcinoma of the lung was T2bN2 (stage IIIa), the highest
stage of any of the studied patients. Looking specifically at this
patient's CTC findings, despite having operatively confirmed N2
disease, his baseline CTC count was 0 cells/mm3 (data
not shown). This rose during lung manipulation to 40
cells/mm3 at preligation, fell post-resection to 25
cells/mm3. and the patient's final blood sample
exhibited 3 cells/mm3 (data not shown). Although not
alone in the increase in CTC count from baseline during resection,
this patient was one of only two patients who had no appreciable
circulating tumour cells preoperatively. Despite a rise in CTC
count, no significant association between the late development of
distant metastatic deposits of the tumour and preoperative,
intraoperative or postoperative concentrations of CTCs was observed
in the present study.
Discussion
Metastatic spread is unpredictable and remains
poorly understood. A well-described and researched area is that of
tumour cell entry and movement in the general vasculature (2). Migrating tumour cells from the blood are
commonly referred to as CTCs and have been heavily implicated in
the development of metastases (8).
The underlying mechanisms of tumour cell dispersion from the
primary tumour are not fully understood; however, it has been
speculated that even simple physical exertion may cause this
dispersion (9). As observed in the
current study, detectable levels of CTCs circulate at rest. To this
end, the general consensus amongst surgeons is to divide the
pulmonary vein during resection as an early treatment step.
Several early studies (10–12)
indicated that tumour manipulation during surgical resection may
contribute to tumour cell dispersion into the pulmonary vein, with
increased volumes of CTCs detected in blood from the pulmonary vein
of patients who had little or no baseline CTC count (10). However, this manipulation is typically
essential to perform a resection. In a more recent study, which
evaluated 42 patient samples, blood was collected from the
tumour-draining pulmonary vein at the end of the surgical procedure
and analysed for CTCs (13). The
authors' concluded that the CTCs appeared to have been mobilised as
a result of surgery and that this may allow their further
dissemination (13). The current
study supports this finding, with 5/10 patients demonstrating a
rise in CTC count intraoperatively, with two of these patients
previously having no detectable CTCs at baseline readings.
There was no statistically significant difference
found in pre- and post-operative levels of lung CTCs, as evaluated
using the ScreenCell® technique. This lack of increase in the
concentration of CTCs may be due to the surgical technique not
dislodging a significant volume of cells, the metastatic potential
of lung cancer or the sensitivity of the ScreenCell® system. A
recent study, utilising the CellSearch® method (Janssen
Diagnostics, LLC, South Raritan, NJ, USA) of cell detection,
concluded that there was a significant increase in the CTC count of
pulmonary vein blood following surgical manipulation of a tumour
(14). These findings are supported
by the results of the present study.
There are several commercially available systems
that use a variety of techniques to identify CTCs. The present
study used a size-based filtration system produced by ScreenCell®,
due to its simplicity, speed and the benefit that it eliminates any
antibody bias that may be introduced by other techniques. Hou et
al (15) identified a strong
correlation between an increased CTC count and poor patient
survival. The current study did not validate these findings for
non-small cell lung carcinoma.
The investigation of CTCs is not isolated to lung
cancer, with the technology being utilised in numerous cancer
types. Breast cancer was one of the first types of cancer to be
investigated. Multiple studies have found a correlation between a
high baseline CTC concentration and poor progression-free survival
(16–19). In addition, reducing the level of
breast cancer CTCs detectable in the blood has been identified to
be a good marker of response to treatment, a correlation also
demonstrated in colorectal cancer (16–19). As
demonstrated in numerous studies, a more advanced tumour stage has
been associated with a higher CTC count in the peripheral blood
(16–19). CTCs are detectable at an early tumour
stages at varying levels, allowing the potential use of CTC
analysis as a method for early diagnosis (3,4).
In conclusion, although a significant rise in CTCs
was detected between the initial sample of peripheral blood taken
and the operative sample obtained prior to pulmonary vein ligation,
it was not possible to identify an association between CTC count
and distant metastatic spread of the tumour. To the best of our
knowledge, no prior studies have investigated the impact of
intraoperative dissemination of CTCs into the systemic vasculature,
for either short-term inflammatory responses or long-term patient
survival. Although an increase in CTC concentration was identified
to have no clinical impact in the present study, no recommendation
can be made at this stage. Future studies may study a larger cohort
of patients, in order to better define the rate of sensitivity and
specificity of using the ScreenCell® filtration device in patients
with lung cancer. Moreover, the ScreenCell® filtration device has
been used successfully for detection of CTCs for breast cancer, in
addition to head and neck cancer. Therefore, future studies using
the ScreenCell® filtration device may generate novel data on CTC
isolation from a wide repertoire of cancer types.
Acknowledgements
The present study was supported by the Cryotherapy
Research Charity (grant no. G0029).
References
|
1
|
Desitter I, Guerrouahen BS, Benali-Furet
N, Wechsler J, Jänne PA, Kuang Y, Yanagita M, Wang L, Berkowitz JA,
Distel RJ, et al: A new device for rapid isolation by size and
characterization of rare circulating tumor cells. Anticancer Res.
31:427–441. 2011.PubMed/NCBI
|
|
2
|
Fidler IJ: The pathogenesis of cancer
metastasis: The ‘seed and soil’ hypothesis revisited. Nat Rev
Cancer. 3:453–458. 2003. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Delloye-Bourgeois C, Fitamant J, Paradisi
A, Cappellen D, Douc-Rasy S, Raquin MA, Stupack D, Nakagawara A,
Rousseau R, Combaret V, et al: Netrin-1 acts as a survival factor
for aggressive neuroblastoma. J Exp Med. 206:833–847. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Nagrath S, Sequist LV, Maheswaran S, Bell
DW, Irimia D, Ulkus L, Smith MR, Kwak EL, Digumarthy S, Muzikansky
A, et al: Isolation of rare circulating tumour cells in cancer
patients by microchip technology. Nature. 450:1235–1239. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Munzone E, Botteri E, Sandri MT, Esposito
A, Adamoli L, Zorzino L, Sciandivasci A, Cassatella MC, Rotmensz N,
Aurilio G, et al: Prognostic value of circulating tumor cells
according to immunohistochemically defined molecular subtypes in
advanced breast cancer. Clin Breast Cancer. 12:340–346. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhang S, Lu Z, Unruh AK, Ivan C, Baggerly
KA, Calin GA, Li Z, Bast RC Jr and Le XF: Clinically relevant
microRNAs in ovarian cancer. Mol Cancer Res. 13:393–401. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Krebs MG, Hou JM, Sloane R, Lancashire L,
Priest L, Nonaka D, Ward TH, Backen A, Clack G, Hughes A, et al:
Analysis of circulating tumor cells in patients with non-small cell
lung cancer using epithelial marker dependent and independent
approaches. J Thorac Oncol. 7:306–315. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hiltermann TJ, Pore MM, Van den Berg A,
Timens W, Boezen HM, Liesker JJ, Schouwink JH, Wijnands WJ, Kerner
GS, Kruyt FA, et al: Circulating tumor cells in small-cell lung
cancer: A predictive and prognostic factor. Ann Oncol.
23:2937–2942. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fidler IJ: Tumour heterogeneity and the
biology of cancer invasion and metastasis. Cancer Res.
38:2651–2660. 1978.PubMed/NCBI
|
|
10
|
Scheinin TM and Koivuniemi AP: The
occurrence of cancer cells in blood. Surgery. 51:652–657.
1962.PubMed/NCBI
|
|
11
|
Lee VW, Chiang T and Deodar SD: Bioassay
for quantifying circulating tumour cells in a syngenic mouse model.
Cancer Res. 36:2053–2058. 1976.PubMed/NCBI
|
|
12
|
Karl A, Tritschler S, Hofmann S, Stief CG
and Schindlbeck C: Perioperative search for circulating tumor cells
in patients undergoing radical cystectomy for bladder cancer. Eur J
Med Res. 14:487–490. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yao X, Williamson C, Adalsteinsson VA,
D'Agostino RS, Fitton T, Smaroff GG, William RT, Wittrup KD and
Love JC: Tumor cells are dislodged into the pulmonary vein during
lobectomy. J Thorac Cardiovasc Surg. 148:3224–3231. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hashimoto M, Tanaka F, Yoneda K, Takuwa T,
Matsumoto S, Okumura Y, Kondo N, Tsubota N, Tsujimura T, Tabata C,
et al: Significant increase in circulating tumour cells in
pulmonary venous blood during surgical manipulation in patients
with primary lung cancer. Interact Cardiovasc Thorac Surg.
18:775–783. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hou JM, Greystoke A, Lancashire L,
Cummings J, Ward T, Board R, Amir E, Hughes S, Krebs M, Hughes A,
et al: Evaluation of circulating tumor cells and serological cell
death biomarkers in small cell lung cancer patients undergoing
chemotherapy. Am J Pathol. 175:808–816. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hayes DF, Cristofanilli M, Budd GT, Ellis
MJ, Stopeck A, Miller MC, Matera J, Allard WJ, Doyle GV and
Terstappen LW: Circulating tumor cells at each follow-up time point
during therapy of metastatic breast cancer patients predict
progression-free and overall survival. Clin Cancer Res.
12:4218–4224. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cristofanilli M, Hayes DF, Budd GT, Ellis
MJ, Stopeck A, Reuben JM, Doyle GV, Matera J, Allard WJ, Miller MC,
et al: Circulating tumor cells: A novel prognostic factor for newly
diagnosed metastatic breast cancer. J Clin Oncol. 23:1420–1430.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Krebs MG, Hou JM, Ward TH, Blackhall FH
and Dive C: Circulating tumour cells: Their utility in cancer
management and predicting outcomes. Ther Adv Med Oncol. 2:351–365.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cohen SJ, Punt CJ, Iannotti N, Saidman BH,
Sabbath KD, Gabrail NY, Picus J, Morse M, Mitchell E, Miller MC, et
al: Relationship of circulating tumor cells to tumor response,
progression-free survival, and overall survival in patients with
metastatic colorectal cancer. J Clin Oncol. 26:3213–3221. 2008.
View Article : Google Scholar : PubMed/NCBI
|