Introduction
Prostate cancer (PCa) is the most frequently
diagnosed malignancy and the second cause of cancer-associated
mortality in the USA. Until 2015, there were 220,800 estimated new
PCa cases, accounting for ~one-quarter of all new diagnoses and
27,540 estimated mortalities in the USA (1). The incidence and mortality rates of PCa
account for the second largest proportion of cancer in males
worldwide. In 2012, ~1.1 million cases worldwide were diagnosed
with PCa and 307,000 males succumb annually to the disease
(2). The scale of the PCa population
represents an economic burden on health care systems. Family
history, advanced age, testosterone, African-American ethnicity,
diet and environmental exposure are considered to influence the
development of PCa (3). Sutcliffe
et al (4) proposed that the
sexually transmitted diseases (STDs) may serve an important role in
the initiation of PCa. Viral infection may induce chronic and
recurrent inflammation of the prostate, and we hypothesize that
inflammation of the prostate induced by STDs may increase the risk
of PCa. Additionally, HPV has been recognized as the main
etiological factor in cervical cancer (5). The E6/E7 oncoproteins of HPV types 16
and 18 have been reported to immortalize prostate epithelial cells
(6).
HPV is a small, non-enveloped DNA virus with a
circular, double-stranded DNA genome of ~8 kb in size, for which
>140 HPV genotypes have been recognized and fully sequenced
(7). HPV is one of the most common
STDs worldwide (8). Nearly all
sexually active individuals may be infected by HPV at some point
during their lifetime (9). McNicol
and Dodd (10) first detected HPV DNA
in prostatic tissues using polymerase chain reaction (PCR) in 1990.
To date, a growing number of studies have been conducted to
investigate the association between HPV infection and PCa, as
summarized in a previous review by Ramezani et al (11). However, the association between HPV
infection and PCa has not been assessed clearly. The present study
performed a meta-analysis to investigate the association between
HPV infection and PCa risk.
Materials and methods
Search strategy
Electronic databases, including PubMed (https://www.ncbi.nlm.nih.gov/pubmed/),
Web of Science (http://login.webofknowledge.com/), Cochrane library
(http://www.cochranelibrary.com/),
Chinese National Knowledge Infrastructure (http://www.cnki.net/), China Wan Fang database
(http://www.wanfangdata.com.cn/) and
China Biomedical Literature Database (http://www.sinomed.ac.cn/), were searched for relevant
clinical articles published up until May 14, 2015. Research studies
were selected using the following keywords: ‘Prostate’, ‘HPV’ and
‘human papillomavirus’. Furthermore, reference lists of reviews or
studies identified in the literature search were hand-searched for
additional studies. There were no publication date
restrictions.
Study selection and inclusion
criteria
A published study was included in the present study
if it met the following requirements: i) A case-control study; ii)
conducted on human subjects and written in English or Chinese; iii)
no restrictions placed on patients' nationality, ethnicity or age;
and iv) histological diagnosis of cases and controls were
established. When duplicated studies were identified, only the
study published first or the study that provided more detailed
information was included (10,12–14).
Data extraction
All data were extracted independently and
crosschecked by two authors. The following information was obtained
from each study: First author, year of publication, geographical
region, type of tissue [paraffin-embedded fixed tissue (PET) or
fresh frozen tissue (FF)], HPV detection method, HPV subtypes and
the numbers of cases/controls and HPV-positive cases/controls.
Disagreements were resolved by discussion and consent with a third
author.
Quality assessment
The Newcastle-Ottawa Scale (NOS) was used to assess
the quality of individual studies (15). A maximum of 9 points was assigned to
each study, 4 for selection, 2 for comparability and 3 for
exposure. Scores of 0–3, 4–6 and 7–9 were regarded as low, moderate
and high quality, respectively (16).
Statistical analysis
A meta-analysis of the association between HPV
infection and the risk of PCa was performed, and odds ratios (ORs)
with 95% confidence intervals (CIs) were used as a common measure
across studies. Heterogeneity among studies was examined using
Cochran's Q test (P<0.10 indicated a high level of statistical
heterogeneity) and the I2 statistic (values of 25, 50
and 75% corresponding to low, moderate and high degrees of
heterogeneity, respectively) was additionally calculated (17). The random-effects model (DerSimonian
and Laird method) (18) took into
account when heterogeneity was present among studies. Otherwise, a
fixed-effects model (Mantel-Haenszel method) (19) was applied. Stratified pooled analyses
were subsequently performed according to the HPV detection method,
geographical region, publication year and type of tissue. To
evaluate the effect of one single study on the overall risk of PCa,
sensitivity analyses were performed by sequential omission of
individual studies and the robustness of the pooled estimate was
tested. For each pooled analysis, the publication bias was
determined from a Begg's (20) funnel
plot and Egger's (21) test for the
overall study. All analyses were performed using STATA, version
12.0 (Stata Corp LP, College Station, TX, USA). P<0.05
(two-tailed) was considered to indicate a statistically significant
difference.
Results
Eligible studies
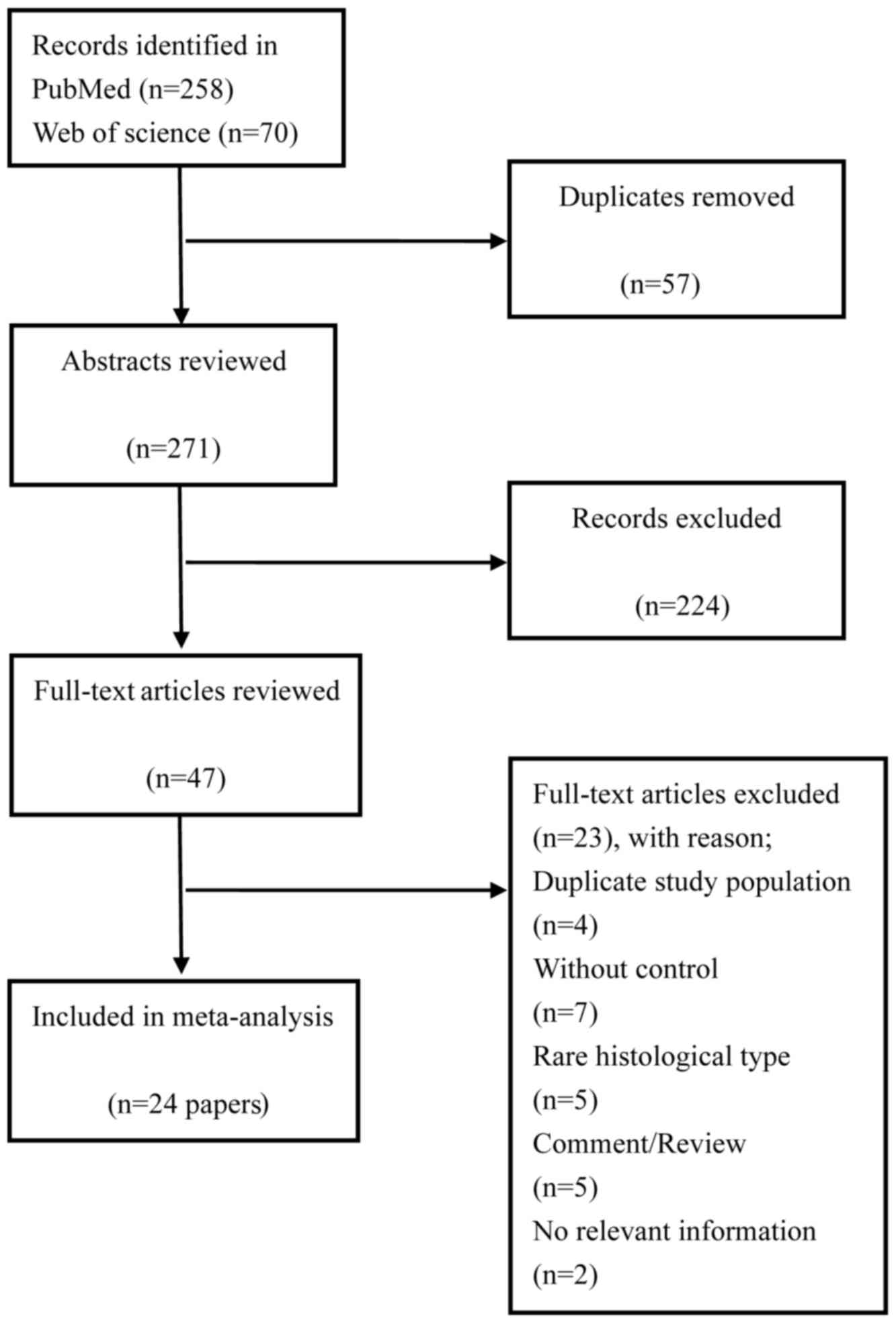
A total of 348 relevant citations were identified at
the initial search stage. Following the removal of the duplicates
(n=63), 238 studies were excluded based on titles and abstracts
review, mainly as they were not relevant to the present analysis.
From a full-text review of potentially relevant papers (n=47), 23
studies were excluded based on the following reasons: A total of 4
studies (10,12–14)
included the same data as previous articles (22,23), 7
studies lacked a control group (24–30) and 2
studies did not offer the pathological tissue information (31,32);
others used bladder cancer cells (33), PCa cells (34) or expressed prostate secretion as the
experiment material (35). The last 2
studies were unavailable for analysis (36,37).
Finally, 24 papers (6,22,23,38–58)
were included in the meta-analysis. The papers included were
published between February, 1990 and January, 2015. A detailed
flowchart of the selection process is presented in Fig. 1.
Study characteristics
The characteristics of all included studies are
presented in Table I. These studies
were published between 1990 and 2015 and comprised 971 PCa cases in
total. The majority of the studies originated from Asia (n=8)
(38,40,43–45,48,51,56),
Europe (n=7) (22,39,42,47,50,53,55)
and North America (n=5) (23,49,52,54,57),
and the remaining studies originated from South America (n=1)
(46) and Oceania (n=2) (6,41). For the
type of PCa or BPH tissue, half of the included studies used
formalin-fixed PET (38–42,44,46,48,52,56,57)
whereas the others use frozen sections (6,22,23,43,47,49–51,53–55).
A total of 2,056 cases were included in the 24 studies
investigating the association between HPV infection and risk of PCa
(971 were in the case group and 1,085 were in the control group).
Within the eligible studies, the prevalence of HPV DNA in PCa
varied from 0% (45,48–50,58) to 75%
(55).
 | Table I.Characteristics of studies included
in the meta-analysis. |
Table I.
Characteristics of studies included
in the meta-analysis.
|
|
|
|
|
| Case (n=971) | Controls
(n=1,085) |
|---|
|
|
|
|
|
|
|
|
|---|
| Author/(Refs.),
year | Country | Sample | Detection
method | HPV type
detected | n/Total n | % | n/Total n | % |
|---|
| McNicol and Dodd
(23), 1991 | Canada | FF | PCR, type-specific
primers | 16,18 | 14/27 | 51.9 | 34/56 | 60.7 |
| Masood et al
(58), 1991 | USA | FFPE | ISH |
6,11,16,18,31,35 | 0/20 | 0.0 | 0/20 | 0.0 |
| Rotola et al
(55), 1992 | Italy | FF | PCR, specific
primers | 16 | 6/8 | 75.0 | 14/17 | 82.3 |
| Anwar et al
(56), 1992 | Japan | PET | PCR, type-specific
primers | 16,18,33 | 28/68 | 41.2 | 0/10 | 0.0 |
| Ibrahim et
al (57), 1992 | USA | PET | PCR | 16 | 6/24 | 25.0 | 0/16 | 0.0 |
| Dodd et al
(54), 1993 | Canada | FF | PCR | 16 | 3/7 | 42.9 | 5/10 | 50.0 |
| Moyret-Lalle et
al (53), 1995 | France | FF | PCR,
type-specific | 16.18 | 9/17 | 52.9 | 7/22 | 31.8 |
| Suzuki et al
(51), 1996 | Japan | FF | PCR, consensus
primers | 16 | 8/51 | 15.7 | 0/51 | 0.0 |
| Wideroff et
al (52), 1996 | USA | PET | PCR, consensus
primers |
6,11,16,18,31,33,45 | 7/56 | 12.5 | 4/42 | 9.5 |
| Anderson et
al (50), 1997 | UK | FF | PCR, type-specific
and general primers | 16 | 0/14 | 0.0 | 0/10 | 0.0 |
| Noda et al
(48), 1998 | Japan | PET | PCR, consensus
primers | 16 | 0/38 | 0.0 | 3/71 | 4.2 |
| Strickler et
al (49), 1998 | USA | FF | PCR | 11,16,18,
51,56 | 0/63 | 0.0 | 0/61 | 0.0 |
| Serth et al
(22), 1999 | Germany | FF | PCR | 16 | 10/47 | 21.3 | 1/37 | 2.7 |
| Carozzi et
al (47), 2004 | Italy | FF | PCR |
6,11,16,18,31,33,35,45,52,58 | 17/26 | 65.4 | 12/25 | 48.0 |
| Leiros et al
(46), 2005 | Argentina | PET | PCR | 11.16 | 17/41 | 41.5 | 0/30 | 0.0 |
| Gazzaz and Mosli
(45), 2009 | Saudi Arabia | FF | Hybrid Capture |
6,11,16,18,31,33,35,39,40 | 0/6 | 0.0 | 0/50 | 0.0 |
| Chen et al
(6), 2011 | Australia | FF | PCR,
type-specific | 18 | 7/51 | 13.7 | 3/11 | 27.3 |
| Aghakhani et
al (44), 2011 | Iran | PET | PCR, general
primers | 6,11,16,18 | 13/104 | 12.5 | 8/104 | 7.7 |
| Tachezy et
al (42), 2012 | Czech Republic | PET | PCR, general
primers | 16 | 1/51 | 2.0 | 2/95 | 2.1 |
| Salehi and Hadavi
(43), 2012 | Iran | FF | PCR, consensus
primers | NR | 3/68 | 4.4 | 0/85 | 0.0 |
| Whitaker et
al (41), 2013 | Australia | PET | PCR, type-specific
primers | 18 | 7/10 | 70.0 | 2/10 | 20.0 |
| Ghasemian et
al (40), 2013 | Iran | PET | PCR, general
primers | NR | 5/29 | 17.2 | 8/167 | 4.8 |
| Michopoulou et
al (39), 2014 | Greece | PET | PCR, general
primers | 16,18,31 | 8/50 | 16.0 | 1/30 | 3.3 |
| Singh et al
(38), 2015 | India | PET | PCR, type-specific
primers | 6,11,16,18 | 39/95 | 41.1 | 11/55 | 20.0 |
Study quality
Table II demonstrated
the quality of the included studies. NOS scores ranged from
6–8.
| Table II.Study quality. |
Table II.
Study quality.
|
| Selection | Comparability | Exposure |
|
|---|
|
|
|
|
|
|
|---|
| Author/(Refs.),
year | Adequate definition
of cases | Representativeness
of case | Selection of
controls | Definition of
controls | Control for
important factors or additional factors | Ascertainment of
exposure | Same method of
ascertainment for subjects | Non-response
rate | Total score |
|---|
| McNicol and Dodd
(23), 1991 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 7 |
| Masood et al
(58), 1991 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 7 |
| Rotola et al
(55), 1992 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 6 |
| Anwar et al
(56), 1992 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Ibrahim et
al (57), 1992 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 7 |
| Dodd et al
(54), 1993 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 7 |
| Moyret-Lalle et
al (53), 1995 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Suzuki et al
(51), 1996 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Wideroff et
al (52), 1996 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Anderson et
al (50), 1997 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 6 |
| Noda et al
(48), 1998 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 6 |
| Strickler et
al (49), 1998 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Serth et al
(22), 1999 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Carozzi et
al (47), 2004 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Leiros et al
(46), 2005 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 6 |
| Gazzaz and Mosli
(45), 2009 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Chen et al
(6), 2011 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Aghakhani et
al (44), 2011 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 6 |
| Tachezy et
al (42), 2012 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Salehi and Hadavi
(43), 2012 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 5 |
| Whitaker et
al (43), 2013 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 6 |
| Ghasemian et
al (40), 2013 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Michopoulou et
al (39), 2014 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 6 |
| Singh et al
(38), 2015 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
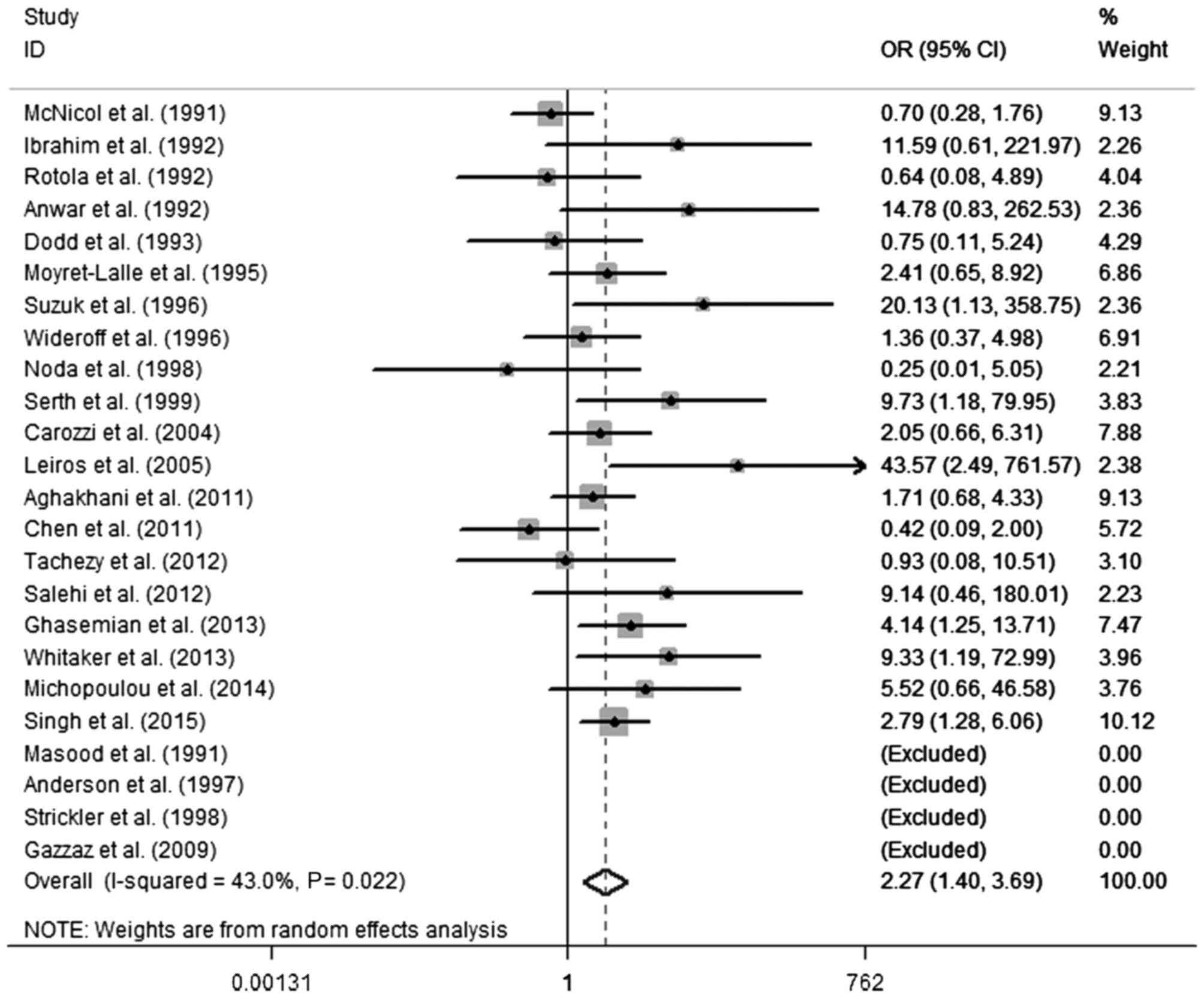
Meta-analysis results
According to the results of the heterogeneity test,
there was moderate heterogeneity between the included studies (Q
test, P=0.022; I2=43.0%). A random-effects model was
selected to evaluate the pooled OR (Fig.
2). The pooled OR of HPV infection was 2.27 (95% CI, 1.40–3.69)
in PCa compared with the control, indicating a significant
association between HPV infection and PCa. To investigate the
sources of heterogeneity, a random-effects meta-regression analysis
was performed, including the following variables: HPV DNA detection
method, geographical region, publication year and type of tissue.
Table III presents the results of
the meta-regression for these variables. No statistical
significance was identified regarding the differences for the
various subgroups and the P-values for publication years,
geographical regions and types of tissue were 0.53, 0.08 and 0.21,
respectively. A significantly increased PCa risk was revealed in
HPV infection when HPV DNA was detected by PCR-based methods (OR,
2.27; 95% CI, 1.40–3.69); however, no significance was identified
by non-PCR methods. Using non-PCR-based methods, the result was
negative in the cases and the controls. When the ORs were pooled by
region, heterogeneity was present in Oceania (P=0.018;
I2=82.8%). A statically significant association was
observed between HPV and PCa in Asia (OR, 2.96; 95% CI, 1.56–5.64)
and Europe (OR, 2.29; 95% CI, 1.17–4.47); however, no significant
difference was demonstrated in North America (OR, 1.05; 95% CI,
0.47–2.36) or Oceania (OR, 1.84; 95% CI, 0.09–38.64). Notably, a
significantly increased risk was revealed in publications since the
year 2000 (OR, 2.65; 95% CI, 1.47–4.85) and there was no
significant difference prior to the year 2000 (OR, 1.92; 95% CI,
0.85–4.35). Similarly, an increased PCa risk when HPV infection was
present in formalin-fixed PET samples was demonstrated (OR, 2.98;
95% CI, 1.68–5.30), but not in fresh frozen tissue (OR, 1.62; 95%
CI, 0.75–3.74).
| Table III.Summary of results. |
Table III.
Summary of results.
| Parameter | Studies, n | Study design | Case/control | OR (95% CI) | P-value | P-value of
heterogeneity | I2,
% |
P-valuea |
|---|
| Total | 24 | Case-control | 971/1085 | 2.27
(1.40–3.69) | 0.001 | 0.022 | 43.0 |
|
| HPV DNA
methods |
|
|
|
|
|
|
| NA |
|
PCR | 22 | Case-control | 945/1015 | 2.27
(1.40–3.69) | 0.001 | 0.022 | 43.0 |
|
| No
PCR | 2 | Case-control | 26/70 | NA | NA | NA | NA |
|
| Year of
publication |
|
|
|
|
|
|
| 0.53 |
|
1990–1999 | 13 | Case-control | 440/423 | 1.92
(0.85–4.35) | 0.117 | 0.046 | 47.7 |
|
|
2000–2015 | 11 | Case-control | 531/662 | 2.65
(1.47–4.87) | 0.001 | 0.113 | 37.0 |
|
| Geographical
region |
|
|
|
|
|
|
| 0.08 |
|
Asia | 8 | Case-control | 459/539 | 2.96
(1.56–5.64) | 0.001 | 0.257 | 22.6 |
|
|
Europe | 7 | Case-control | 213/236 | 2.29
(1.17–4.47) | 0.015 | 0.457 | 0.0 |
|
| North
America | 6 | Case-control | 197/205 | 1.05
(0.47–2.36) | 0.904 | 0.298 | 18.6 |
|
| South
America | 1 | Case-control | 41/30 | 43.57
(2.49–761.57) | 0.010 | NA | NA |
|
|
Oceania | 2 | Case-control | 61/21 | 1.84
(0.09–38.67) | 0.694 | 0.018 | 82.8 |
|
| Type of tissue |
|
|
|
|
|
|
| 0.21 |
|
Frozen | 12 | Case-control | 385/435 | 1.62
(0.75–3.74) | 0.216 | 0.052 | 48.0 |
|
|
Formalin-fixed | 12 | Case-control | 586/650 | 2.98
(1.68–5.30) | 0.000 | 0.184 | 27.3 |
|
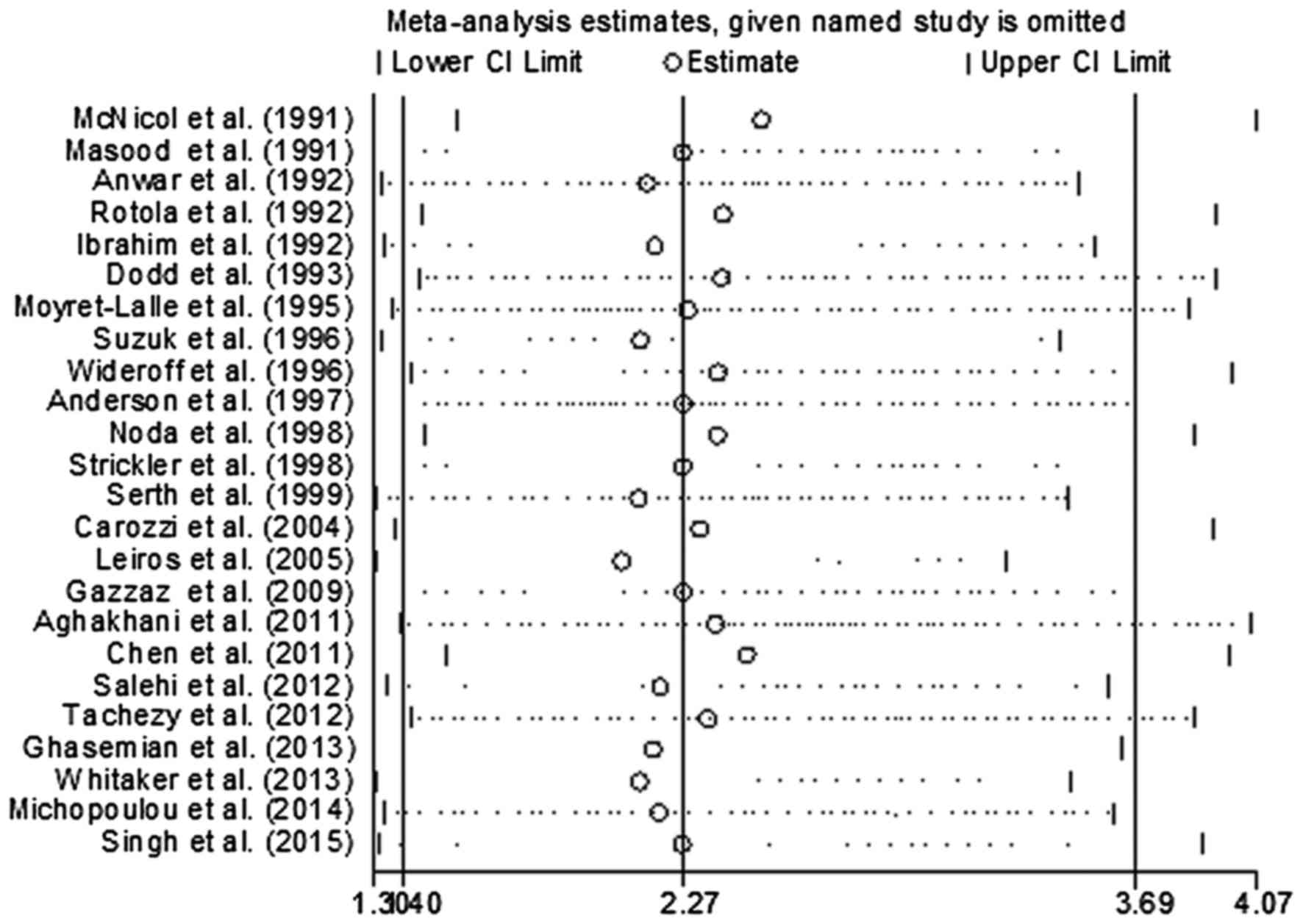
In order to evaluate the influence of each study on
the pooled OR, individual studies were sequentially removed from
the meta-analysis. Fig. 3 presents
the results of the sensitivity analysis. The pooled ORs were stable
and demonstrated statistical significance using the fixed-effects
model, prior to and following deletion of any signal study.
Together, the data indicated that the results of this meta-analysis
were reliable and were not overly affected by one of the 24
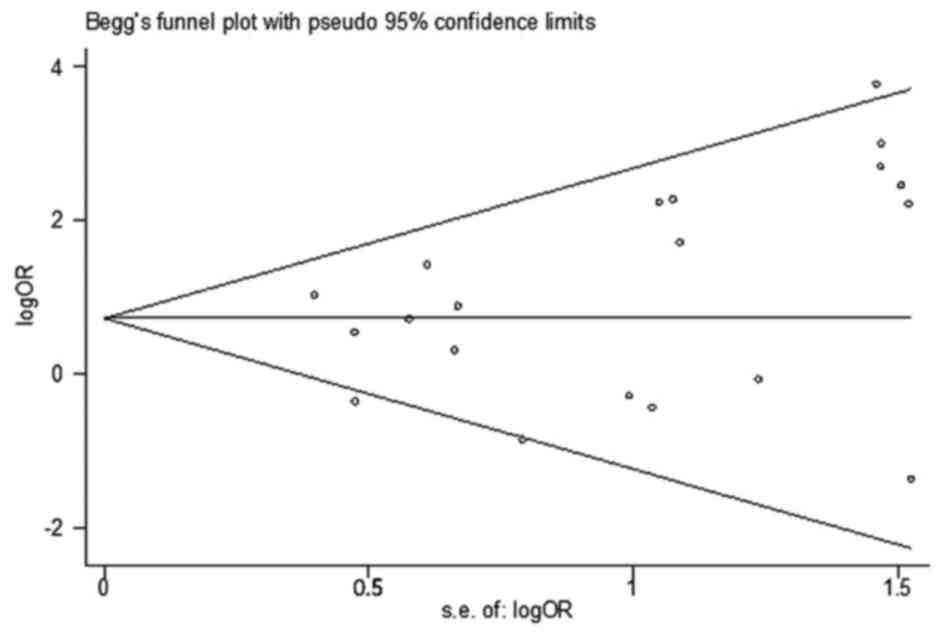
studies. The funnel plot did not reveal evidence of asymmetry
(Fig. 4), and Egger's and Begg's
tests indicated that there was no evidence of publication bias
(P=0.183 and P=0.135, respectively).
Discussion
HPV is one of the most commonly diagnosed sexually
transmitted infections (STIs) worldwide (59). McNicol and Dodd (10) were the first to detect HPV DNA in
prostatic tissue using PCR analysis in 1990. To date, a growing
number of studies have been conducted to investigate the
association between HPV infection and PCa risk, but results of
these studies have often been controversial (11). Generally, HPV infection results in
inflammation (60). A previous early
study expounded that inflammation is a critical component of tumor
progression (61). In the majority of
cases, HPV infections are often asymptomatic or self-limited;
however, a small number of cases result in a serious burden
(62). At present, the majority of
studies have focused on female HPV infection (63). However, men can be infected by HPV
which is associated with a variety of cancer subtypes, including
anal, penile and oral cancer (64).
Men serve a key role in spreading HPV to male and female sexual
partners (65). A previous study
reported a higher rate of PCa in men with a history of exposure to
gonorrhea, HPV or any STD (66).
HPV has been established as the main etiological
factor in cervical cancer (5) and the
association between HPV infection and other types of cancer,
including oropharynx (67), breast
cancer (68), head and neck cancer
(69) and bladder cancer (70), has been studied. Grulich and Vajdic
(71) demonstrated that HPV infection
induced a marked increase in the prevalence of cervical cancer in
immune-compromised patients but not in the prevalence of PCa. The
role of HPV may be different in these two types of cancer. Vieira
et al (72) suggested that HPV
E6 may induce repression of apolipoprotein B mRNA editing enzyme
catalytic subunit 3B (APOBEC3B; A3B) gene transcription by
functional inactivation of p53 in HPV-positive cervical cancer.
Conversely, a previous study indicated that A3B
overexpression existed not only in PCa, but also in normal prostate
tissues (73), which suggested that
there may be a nonsense mutation of A3B in normal prostate
tissues. Suzuki et al (51)
indicated that p53 gene mutation or the presence of HPV E6 was
involved in the development of PCa, but there was no association
between p53 mutation and HPV DNA integration. Similarly, Leiros
et al (46) revealed that p53
codon 72 allelic frequencies were not observed in prostate
hyperplasia and PCa with or without HPV infection. Another previous
study (43) demonstrated a similar
conclusion. Furthermore, Cantalupo et al (74) investigated The Cancer Genome Atlas
database, and revealed a robust expression level of HPV18
genes in cervical cancer tissue samples. They also identified
HPV18 transcripts in colon, rectum and normal kidney tissue
samples; however, the HPV18 gene expression level was lower
compared with that in cervical cancer tissues. The present study
also demonstrated that HPVs detected in PCa were found at low
levels in certain patients. Overall, HPV may serve various roles in
the development of cervical and PCa, and further high quality
studies are required.
In a meta-analysis study published in 2011, Lin
et al (75) concluded that the
causal role of HPV in prostate cancer remained doubtful, as the
pooled results of DNA detection method and serologic assays
(antibody) were negative; however, no statistical significance was
observed in serological assays. The result was positive when the
analysis was limited to HPV detection of type 16 infection in PCa
tissues (75). Serological testing
has the following limitations: i) Antibody cross-reactivity; ii) it
is difficult to establish a temporal association between infection
and cancer; iii) numerous individuals could be infected by HPV
throughout their lifetime, so the control group may be positive;
iv) based on a number of etiological studies, it is commonly agreed
that HPV does not induce a generalized viremia; and v) only
persistent infections induce pathological alterations and
serological detection indicates HPV exposure rather than the exact
site of infection (76). As a result,
studies that used peripheral blood cells and serology were excluded
in the present meta-analysis. A similar study by Bae (77) was published in Epidemiology and Health
on February 11, 2015, applying a ‘snowballing search strategy’ to
search relevant studies from published papers (75,78).
Although this method saved energy, studies should be identified
again, as different studies have varying inclusion criteria.
Additionally, numerous problems remain unsolved: Firstly, whether
the risk of PCa with HPV infection varies in different histological
types; and secondly, the varied specificity and sensitivity in
various HPV DNA detection methods may affect the risk estimation
between HPV infection and PCa. Thus, the present study evaluated
the association between PCa and HPV infection by considering the
heterogeneity of the major associated parameters, including
detection method, study region and histological type.
Certain factors may contribute to the variability of
results with regard to evaluating the association of HPV infection
and PCa. In the present meta-analysis study, stratified analyses
were performed according to geographical region, publication year,
HPV detection method and type of tissue. The results showed that
there were no differences in HPV detection method, geographical
region, publication year or type of tissue. The present study
suggested a moderate geographical variation in HPV prevalence and
association strengths with PCa. A moderate variation of the pooled
OR results for various geographical regions was demonstrated and
heterogeneity was present in Oceania (P=0.018;
I2=82.8%), this may be due to the difference resulting
from genetic background, environmental risk factors, including
smoking, sexual behavior and other ethnic and cultural differences,
as well as other unknown sources. A previous study reported the
worldwide prevalence of cervical HPV DNA and also revealed a higher
HPV detection rate in Asia and Europe, followed by America
(including South American and North American) (79). This analysis suggested that the risks
of PCa with HPV infection increased significantly in Asia and
Europe, but not in North America and Oceania. The increase is
regionally consistent with the association between bladder cancer
and HPV infection (70).
In the present meta-analysis, the studies that used
PCR-based methods to detect HPV DNA demonstrated a higher
sensitivity compared with non-PCR-based methods. This statement
could be certified by two specific studies, which employed
non-PCR-based methods to detect HPV DNA and obtained negative
results in the cases and the controls (45,58). For
the PCR-based methods with variation in the types of HPV primers
used, type-specific primers may be more sensitive to detect 200 bp
shorter HPV DNA sequences compared with consensus primers to
amplify 450-bp fragments. The variations in the sensitivity of HPV
detection may be due to the differences in amplification efficiency
between various types of HPV primers. Therefore, it is possible
that the detection rates of HPV using HPV type-specific PCR primers
may be higher compared with those using other PCR primers. A
similar phenomenon was reported in bladder and ovarian cancer
(70,80). This premise is supported by the
findings in the present study.
With regard to the publication year, study size was
similar prior to and following the year 2000. A significantly
increased risk was demonstrated following 2000 (OR, 2.65; 95% CI,
1.47–4.85) and no significant difference was found prior to 2000
(OR, 1.92; 95% CI, 0.85–4.35). With the development of science and
technology, the detection method is becoming increasingly sensitive
(81). Publication year is a crude
evaluation, but this information was not available in previous
studies.
Half of the included studies used PET to detect HPV
DNA. PET and FF were used for pathological and molecular diagnosis.
FF is considered to have the highest quality; however, it is a
challenge to isolate highly degraded and cross-linked nucleic acids
from FF PET samples for molecular analysis, mainly due to DNA
degradation in PET (82). Long DNA
fragments are difficult to amplify by consensus primers from PET
and type-special primers may be more sensitive for detecting HPV
DNA sequences (83). However, the
present study revealed that samples from PET had a higher point
estimate of OR compared with those from FF samples. This phenomenon
may primarily be due to the fact that PET is more easily
contaminated than FF. Previous early studies reported that HPV DNA
existed on fomites and various medical surfaces (84,85).
Future studies should investigate the association between HPV and
PCa, in which the aforementioned factors should be taken into
account to acquire a more realistic result.
Numerous potential limitations should be
acknowledged in the present meta-analysis. Firstly, PCa is
multifactorial in etiology, the present meta-analysis was unable to
analyze family history, diet, smoking or age, which were also risk
factors of PCa, as few of these factors were recorded in the
studies that were included. Secondly, a number of limitations also
appeared in the detection method of HPV in prostatic tissue: i) Due
to the high sensitivity of PCR, contaminated specimens may induce a
false positive result, particularly in the earliest studies. Future
studies should avoid contamination and record the quality control
measures. ii) DNA detection could only determine the current
infection status, if a pathogen infected a tissue using a
hit-and-run mechanism (86), it may
not be detected at the time of analysis. iii) The results may vary
depending on the location of the tissue sampling. Finally, for the
control group of the included studies, only one study mentioned
that the partial normal prostate sample was obtained from autopsy
(56) and the majority of the
remaining studies included patients with benign prostate
hyperplasia (BHP). BHP is the enlargement of the prostate gland by
increased tissue mass in the transition zone of the prostate, a
prevalent, chronic and progressive disease (87). Preliminary works reported that 11–44%
of BHP progressed to PCa within 7 years (88–90). HPV
infection was also identified in the BHP tissue samples of the
included studies. The present study acknowledged that transrectal
ultrasound-guided biopsy of the prostate and identification by
pathological examination were not 100% sensitive, and that cases of
PCa may have been missed. It was not possible to obtain completely
normal prostate tissues. Prostate-specific antigen (PSA) testing
offered the doctor an opportunity to screen asymptomatic patients;
increased levels of serum PSA may indicate PCa. PSA monitoring
should be undertaken in a monitoring period could assist in
identifying PCa and BHP.
A lack of publication bias suggested that such an
association is not an artifact of unpublished negative studies.
Furthermore, the association between HPV infection and risk of PCa
persists, and remains statistically significant in sensitivity
analyses based on various exclusion criteria, which indicated that
the results of the present study are robust.
The overall results of the present meta-analysis
provided evidence that HPV infection significantly increased the
risk of PCa. Tissue-based methods (such as PCR, in situ
hybridization and immunohistochemistry) and serological assays
(such as enzyme-linked immunosorbent assays and immunofluorescence
detection) are basic approaches applied in current research.
Further novel laboratory techniques should be performed to confirm
the present findings, and the pathogenesis and prognostic role of
HPV in PCa requires further investigation, which may lead to a
novel horizon. The HPV vaccine, which has already been applied
against cervical cancer, may be a novel approach to prevent
PCa.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant no. 81271917).
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015. CA Cancer J Clin. 65:5–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ferlay J, Soerjomataram I, Dikshit R, Eser
S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer
incidence and mortality worldwide: Sources, methods and major
patterns in GLOBOCAN 2012. Int J Cancer. 136:E359–E386. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hoffman RM: Clinical practice. Screening
for prostate cancer. N Engl J Med. 365:2013–2019. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sutcliffe S, Nevin RL, Pakpahan R, Elliott
DJ, Cole SR, De Marzo AM, Gaydos CA, Isaacs WB, Nelson WG, Sokoll
LJ, et al: Prostate involvement during sexually transmitted
infections as measured by prostate-specific antigen concentration.
Br J Cancer. 105:602–605. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
de Villiers EM, Wagner D, Schneider A,
Wesch H, Miklaw H, Wahrendorf J, Papendick U and zur Hausen H:
Human papillomavirus infections in women with and without abnormal
cervical cytology. Lancet. 2:703–706. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chen AC, Waterboer T, Keleher A, Morrison
B, Jindal S, McMillan D, Nicol D, Gardiner RA, McMillan NA and
Antonsson A: Human papillomavirus in benign prostatic hyperplasia
and prostatic adenocarcinoma patients. Pathol Oncol Res.
17:613–617. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tommasino M: The human papillomavirus
family and its role in carcinogenesis. Semin Cancer Biol. 26:13–21.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Onon TS: History of human papillomavirus,
warts and cancer: What do we know today? Best Pract Res Clin Obstet
Gynaecol. 25:565–574. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Videla S, Darwich L, Cañadas M, Clotet B
and Sirera G: Incidence and clinical management of oral human
papillomavirus infection in men: A series of key short messages.
Expert Rev Anti Infect Ther. 12:947–957. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
McNicol PJ and Dodd JG: Detection of human
papillomavirus DNA in prostate gland tissue by using the polymerase
chain reaction amplification assay. J Clin Microbiol. 28:409–412.
1990.PubMed/NCBI
|
|
11
|
Ramezani A, Banifazl M, Eslamifar A and
Aghakhani A: Association between human papillomavirus infection and
risk of prostate cancer. Iranian J Pathol. 1:3–7. 2011.
|
|
12
|
Kuczyk M, Serth J, Machtens S and Jonas U:
Detection of viral HPV 16 DNA in prostate cancer and benign
prostatic hyperplasia by quantitative PCR-directed analysis.
Prostate Cancer Prostatic Dis. 3 Suppl 1:S232000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kuczyk M, Serth J, Machtens S and Jonas U:
Detection viral HPV 16 DNA in prostate cancer and benign prostatic
hyperplasia by quantitative PCR-directed analysis. Prostate Cancer
Prostatic Dis. 3 Suppl 1:S232000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
McNicol PJ and Dodd JG: Detection of
papillomavirus DNA in human prostatic tissue by Southern blot
analysis. Can J Microbiol. 36:359–362. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Stang A: Critical evaluation of the
Newcastle-Ottawa scale for the assessment of the quality of
nonrandomized studies in meta-analyses. Eur J Epidemiol.
25:603–605. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhou Q, Luo ML, Li H, Li M and Zhou JG:
Coffee consumption and risk of endometrial cancer: A dose-response
meta-analysis of prospective cohort studies. Sci Rep. 5:134102015.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Higgins JP and Thompson SG: Quantifying
heterogeneity in a meta-analysis. Stat Med. 21:1539–1558. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
DerSimonian R and Kacker R: Random-effects
model for meta-analysis of clinical trials: An update. Contemp Clin
Trials. 28:105–114. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mantel N and Haenszel W: Statistical
aspects of the analysis of data from retrospective studies of
disease. J Natl Cancer Inst. 22:719–748. 1959.PubMed/NCBI
|
|
20
|
Begg CB and Mazumdar M: Operating
characteristics of a rank correlation test for publication bias.
Biometrics. 50:1088–1101. 1994. View
Article : Google Scholar : PubMed/NCBI
|
|
21
|
Egger M, Smith G Davey, Schneider M and
Minder C: Bias in meta-analysis detected by a simple, graphical
test. BMJ. 315:629–634. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Serth J, Panitz F, Paeslack U, Kuczyk MA
and Jonas U: Increased levels of human papillomavirus type 16 DNA
in a subset of prostate cancers. Cancer Res. 59:823–825.
1999.PubMed/NCBI
|
|
23
|
McNicol PJ and Dodd JG: High prevalence of
human papillomavirus in prostate tissues. J Urol. 145:850–853.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Smelov V, Ouburg S, Pleijster J, Smelova
N, Van Moorselaar RJA and Morre SA: Detection of Hr-Hpv Dna in the
prostate of men with prostate cancer. Eur Urol Suppl. 8:2612009.
View Article : Google Scholar
|
|
25
|
Balis V, Sourvinos G, Soulitzis N,
Giannikaki E, SofraS F and Spandidos DA: Prevalence of BK virus and
human papillomavirus in human prostate cancer. Int J Biol Marker.
22:245–251. 2007. View Article : Google Scholar
|
|
26
|
Saad F, Gu K, Jean-Baptiste J, Gauthier J
and MesMasson AM: Absence of human papillomavirus sequences in
early stage prostate cancer. Can J Urol. 6:834–838. 1999.PubMed/NCBI
|
|
27
|
Sarkar FH, Sakr WA, Li YW, Sreepathi P and
Crissman JD: Detection of human papillomavirus (HPV) DNA in human
prostatic tissues by polymerase chain reaction (PCR). Prostate.
22:171–180. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Serfling U, Ciancio G, Zhu WY, Leonardi C
and Penneys NS: Human papillomavirus and herpes virus DNA are not
detected in benign and malignant prostatic tissue using the
polymerase chain reaction. J Urol. 148:192–194. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Effert PJ, Frye RA, Neubauer A, Liu ET and
Walther PJ: Human papillomavirus types 16 and 18 are not involved
in human prostate carcinogenesis: Analysis of archival human
prostate cancer specimens by differential polymerase chain
reaction. J Urol. 147:192–196. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tu H, Jacobs SC, Mergner WJ and Kyprianou
N: Rare incidence of human papillomavirus types 16 and 18 in
primary and metastatic human prostate cancer. Urology. 44:726–731.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Martinez-Fierro ML, Leach RJ, Gomez-Guerra
LS, Garza-Guajardo R, Johnson-Pais T, Beuten J, Morales-Rodriguez
IB, Hernandez-Ordoñez MA, Calderon-Cardenas G, Ortiz-Lopez R, et
al: Identification of viral infections in the prostate and
evaluation of their association with cancer. BMC Cancer.
10:3262010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Silvestre RV, Leal MF, Demachki S, Nahum
MC, Bernardes JG, Rabenhorst SH, Mde A Smith, Mello WA, Guimarães
AC and Burbano RR: Low frequency of human papillomavirus detection
in prostate tissue from individuals from Northern Brazil. Mem Inst
Oswaldo Cruz. 104:665–667. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sinclair AL, Nouri AM, Oliver RT, Sexton C
and Dalgleish AG: Bladder and prostate cancer screening for human
papillomavirus by polymerase chain reaction: Conflicting results
using different annealing temperatures. Br J Biomed Sci.
50:350–354. 1993.PubMed/NCBI
|
|
34
|
Maitland NJ, Macintosh CA, Schmitz C and
Lang SH: Immortalization of human prostate cells with the human
papillomavirus type 16 E6 gene. Methods Mol Med. 88:275–285.
2004.PubMed/NCBI
|
|
35
|
Smelov V, Gorelov A, Pleijster J,
Savicheva A, Pena S and Morre S: The relevance of HPV infection in
men with chronic inflammation of the prostate. Eur Urol Suppl.
6:712007. View Article : Google Scholar
|
|
36
|
Terris MK and Peehl DM: Human
papillomavirus detection by polymerase chain reaction in benign and
malignant prostate tissue is dependent on the primer set utilized.
Urology. 50:150–156. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Pascale M, Pracella D, Barbazza R,
Marongiu B, Roggero E, Bonin S and Stanta G: Is human
papillomavirus associated with prostate cancer survival? Dis
Markers. 35:607–613. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Singh N, Hussain S, Kakkar N, Singh SK,
Sobti RC and Bharadwaj M: Implication of high risk Human
papillomavirus HR-HPV infection in prostate cancer in Indian
population-A pioneering case-control analysis. Sci Rep. 5:78222015.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Michopoulou V, Derdas SP, Symvoulakis E,
Mourmouras N, Nomikos A, Delakas D, Sourvinos G and Spandidos DA:
Detection of human papillomavirus (HPV) DNA prevalence and p53
codon 72 (Arg72Pro) polymorphism in prostate cancer in a Greek
group of patients. Tumour Biol. 35:12765–12773. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Ghasemian E, Monavari SH, Irajian GR,
Nodoshan MR Jalali, Roudsari RV and Yahyapour Y: Evaluation of
human papillomavirus infections in prostatic disease: A
cross-sectional study in Iran. Asian Pac J Cancer Prev.
14:3305–3308. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Whitaker NJ, Glenn WK, Sahrudin A, Orde
MM, Delprado W and Lawson JS: Human papillomavirus and Epstein Barr
virus in prostate cancer: Koilocytes indicate potential oncogenic
influences of human papillomavirus in prostate cancer. Prostate.
73:236–241. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Tachezy R, Hrbacek J, Heracek J, Salakova
M, Smahelova J, Ludvikova V, Svec A, Urban M and Hamsikova E: HPV
persistence and its oncogenic role in prostate tumors. J Med Virol.
84:1636–1645. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Salehi Z and Hadavi M: Analysis of the
codon 72 polymorphism of TP53 and human papillomavirus infection in
Iranian patients with prostate cancer. J Med Virol. 84:1423–1427.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Aghakhani A, Hamkar R, Parvin M, Ghavami
N, Nadri M, Pakfetrat A, Banifazl M, Eslamifar A, Izadi N, Jam S
and Ramezani A: The role of human papillomavirus infection in
prostate carcinoma. Scand Int J Infect Dis. 43:64–69. 2011.
View Article : Google Scholar
|
|
45
|
Gazzaz FS and Mosli HA: Lack of detection
of human papillomavirus infection by hybridization test in
prostatic biopsies. Saudi Med J. 30:633–637. 2009.PubMed/NCBI
|
|
46
|
Leiros GJ, Galliano SR, Sember ME, Kahn T,
Schwarz E and Eiguchi K: Detection of human papillomavirus DNA and
p53 codon 72 polymorphism in prostate carcinomas of patients from
Argentina. BMC Urol. 5:152005. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Carozzi F, Lombardi FC, Zendron P,
Confortini M, Sani C, Bisanzi S, Pontenani G and Ciatto S:
Association of human papillomavirus with prostate cancer: Analysis
of a consecutive series of prostate biopsies. Int J Biol Marker.
19:257–261. 2004. View Article : Google Scholar
|
|
48
|
Noda T, Sasagawa T, Dong Y, Fuse H, Namiki
M and Inoue M: Detection of human papillomavirus (HPV) DNA in
archival specimens of benign prostatic hyperplasia and prostatic
cancer using a highly sensitive nested PCR method. Urol Res.
26:165–169. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Strickler HD, Burk R, Shah K, Viscidi R,
Jackson A, Pizza G, Bertoni F, Schiller JT, Manns A, Metcalf R, et
al: A multifaceted study of human papillomavirus and prostate
carcinoma. Cancer. 82:1118–1125. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Anderson M, Handley J, Hopwood L, Murant
S, Stower M and Maitland NJ: Analysis of prostate tissue DNA for
the presence of human papillomavirus by polymerase chain reaction,
cloning, and automated sequencing. J Med Virol. 52:8–13. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Suzuki H, Komiya A, Aida S, Ito H, Yatani
R and Shimazaki J: Detection of human papillomavirus DNA and p53
gene mutations in human prostate cancer. Prostate. 28:318–324.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Wideroff L, Schottenfeld D, Carey TE,
Beals T, Fu G, Sakr W, Sarkar F, Schork A, Grossman HB and Shaw MW:
Human papillomavirus DNA in malignant and hyperplastic prostate
tissue of black and white males. Prostate. 28:117–123. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Moyret-Lalle C, Marcais C, Jacquemier J,
Moles JP, Daver A, Soret JY, Jeanteur P, Ozturk M and Theillet C:
ras, p53 and HPV status in benign and malignant prostate tumors.
Int J Cancer. 64:124–129. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Dodd JG, Paraskevas M and McNicol PJ:
Detection of human papillomavirus 16 transcription in human
prostate tissue. J Urol. 149:400–402. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Rotola A, Monini P, Di Luca D, Savioli A,
Simone R, Secchiero P, Reggiani A and Cassai E: Presence and
physical state of HPV DNA in prostate and urinary-tract tissues.
Int J Cancer. 52:359–365. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Anwar K, Nakakuki K, Shiraishi T, Naiki H,
Yatani R and Inuzuka M: Presence of ras oncogene mutations and
human papillomavirus DNA in human prostate carcinomas. Cancer Res.
52:5991–5996. 1992.PubMed/NCBI
|
|
57
|
Ibrahim GK, Gravitt PE, Dittrich KL,
Ibrahim SN, Melhus O, Anderson SM and Robertson CN: Detection of
human papillomavirus in the prostate by polymerase chain reaction
and in situ hybridization. J Urol. 148:1822–1826. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Masood S, Rhatigan RM, Powell S, Thompson
J and Rodenroth N: Human papillomavirus in prostatic cancer: No
evidence found by in situ DNA hybridization. South Med J.
84:235–236. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Colón-López V, Ortiz AP, Del Toro-Mejías
LM, García H, Clatts MC and Palefsky J: Awareness and knowledge of
human papillomavirus (HPV) infection among high-risk men of
Hispanic origin attending a sexually transmitted infection (STI)
clinic. BMC Infect Dis. 12:3462012. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Baker R, Dauner JG, Rodriguez AC, Williams
MC, Kemp TJ, Hildesheim A and Pinto LA: Increased plasma levels of
adipokines and inflammatory markers in older women with persistent
HPV infection. Cytokine. 53:282–285. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Coussens LM and Werb Z: Inflammation and
cancer. Nature. 420:860–867. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Mendoza N, Hernandez PO and Tyring SK: HPV
vaccine update: New indications and controversies. Skin Therapy
Lett. 16:1–3. 2011.PubMed/NCBI
|
|
63
|
Hopkins TG and Wood N: Female human
papillomavirus (HPV) vaccination: Global uptake and the impact of
attitudes. Vaccine. 31:1673–1679. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Colón-López V, Ortiz AP and Palefsky J:
Burden of human papillomavirus infection and related comorbidities
in men: Implications for research, disease prevention and health
promotion among Hispanic men. P R Health Sci J. 29:232–240.
2010.PubMed/NCBI
|
|
65
|
de Lima Rocha MG, Faria FL, Goncalves L,
Mdo C Souza, Fernandes PÁ and Fernandes AP: Prevalence of DNA-HPV
in male sexual partners of HPV-infected women and concordance of
viral types in infected couples. PLoS One. 7:e409882012. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Taylor ML, Mainous AG III and Wells BJ:
Prostate cancer and sexually transmitted diseases: A meta-analysis.
Fam Med. 37:506–512. 2005.PubMed/NCBI
|
|
67
|
Jayaprakash V, Reid M, Hatton E, Merzianu
M, Rigual N, Marshall J, Gill S, Frustino J, Wilding G, Loree T, et
al: Human papillomavirus types 16 and 18 in epithelial dysplasia of
oral cavity and oropharynx: A meta-analysis, 1985–2010. Oral Oncol.
47:1048–1054. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Li N, Bi X, Zhang Y, Zhao P, Zheng T and
Dai M: Human papillomavirus infection and sporadic breast carcinoma
risk: A meta-analysis. Breast Cancer Res Treat. 126:515–520. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
O'Rorke MA, Ellison MV, Murray LJ, Moran
M, James J and Anderson LA: Human papillomavirus related head and
neck cancer survival: A systematic review and meta-analysis. Oral
Oncol. 48:1191–1201. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Li N, Yang L, Zhang Y, Zhao P, Zheng T and
Dai M: Human papillomavirus infection and bladder cancer risk: A
meta-analysis. J Infect Dis. 204:217–223. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Grulich AE and Vajdic CM: The epidemiology
of cancers in human immunodeficiency virus infection and after
organ transplantation. Semin Oncol. 42:247–257. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Vieira VC, Leonard B, White EA, Starrett
GJ, Temiz NA, Lorenz LD, Lee D, Soares MA, Lambert PF, Howley PM
and Harris RS: Human papillomavirus E6 triggers upregulation of the
antiviral and cancer genomic DNA deaminase APOBEC3B. MBio. 5(pii):
e02234–e14. 2014.PubMed/NCBI
|
|
73
|
Gwak M, Choi YJ, Yoo NJ and Lee S:
Expression of DNA cytosine deaminase APOBEC3 proteins, a potential
source for producing mutations, in gastric, colorectal and prostate
cancers. Tumori. 100:112e–117e. 2014.PubMed/NCBI
|
|
74
|
Cantalupo PG, Katz JP and Pipas JM: HeLa
nucleic acid contamination in the cancer genome atlas leads to the
misidentification of human papillomavirus 18. J Virol.
89:4051–4057. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Lin Y, Mao Q, Zheng X, Yang K, Chen H,
Zhou C and Xie L: Human papillomavirus 16 or 18 infection and
prostate cancer risk: A meta-analysis. Ir J Med Sci. 180:497–503.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Simen-Kapeu A, Surcel HM, Koskela P,
Pukkala E and Lehtinen M: Lack of association between human
papillomavirus type 16 and 18 infections and female lung cancer.
Cancer Epidemiol Biomarkers Prev. 19:1879–1881. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Bae JM: Human papillomavirus 16 infection
as a potential risk factor of prostate cancer: An adaptive
meta-analysis. Epidemiol Health. 37:e20150052015. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Hrbacek J, Urban M, Hamsikova E, Tachezy R
and Heracek J: Thirty years of research on infection and prostate
cancer: No conclusive evidence for a link. A systematic review.
Urol Oncol. 31:951–965. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Bruni L, Diaz M, Castellsagué X, Ferrer E,
Bosch FX and de Sanjosé S: Cervical human papillomavirus prevalence
in 5 continents: Meta-analysis of 1 million women with normal
cytological findings. J Infect Dis. 202:1789–1799. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Svahn MF, Faber MT, Christensen J, Norrild
B and Kjaer SK: Prevalence of human papillomavirus in epithelial
ovarian cancer tissue. A meta-analysis of observational studies.
Acta Obstet Gynecol Scand. 93:6–19. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Abreu AL, Souza RP, Gimenes F and
Consolaro ME: A review of methods for detect human papillomavirus
infection. Virol J. 9:2622012. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Kalmár A, Péterfia B, Wichmann B, Patai
ÁV, Barták BK, Nagy ZB, Furi I, Tulassay Z and Molnár B: Comparison
of automated and manual DNA isolation methods for DNA methylation
analysis of biopsy, fresh frozen and formalin-fixed,
paraffin-embedded colorectal cancer samples. J Lab Autom.
20:642–651. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Mori S, Nakao S, Kukimoto I,
Kusumoto-Matsuo R, Kondo K and Kanda T: Biased amplification of
human papillomavirus DNA in specimens containing multiple human
papillomavirus types by PCR with consensus primers. Cancer Sci.
102:1223–1227. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Strauss S, Sastry P, Sonnex C, Edwards S
and Gray J: Contamination of environmental surfaces by genital
human papillomaviruses. Sex Transm Infect. 78:135–138. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Ferenczy A, Bergeron C and Richart RM:
Human papillomavirus DNA in fomites on objects used for the
management of patients with genital human papillomavirus
infections. Obstet Gynecol. 74:950–954. 1989.PubMed/NCBI
|
|
86
|
Iwasaka T, Hayashi Y, Yokoyama M, Hara K,
Matsuo N and Sugimori H: ‘Hit and run’ oncogenesis by human
papillomavirus type 18 DNA. Acta Obstet Gynecol Scand. 71:219–223.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Thorpe A and Neal D: Benign prostate
hyperplasia. Lancet. 361:1359–1367. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Boddy JL, Pike DJ and Malone PR: A
seven-year follow-up of men following a benign prostate biopsy. Eur
Urol. 44:17–20. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Brossner C, Madersbacher S, de Mare P,
Ponholzer A, Al-Ali B and Rauchenwald M: Follow-up of men obtaining
a six-core versus a ten-core benign prostate biopsy 7 years
previously. World J Urol. 23:419–421. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Durkan GC and Greene DR: Elevated serum
prostate specific antigen levels in conjunction with an initial
prostatic biopsy negative for carcinoma: Who should undergo a
repeat biopsy? BJU Int. 83:34–38. 1999. View Article : Google Scholar : PubMed/NCBI
|