Introduction
Tuberous sclerosis complex (TSC), an autosomal
dominant disorder of multiple organ systems involving the brain,
lung, kidney, skin and other organs (1), presents with a great variety of clinical
manifestations (2,3). Multiple and bilateral renal
angiomyolipomas are found in ~70–90% of adult patients with TSC as
reported by O'Callaghan et al and Rakowski et al
(4,5),
tend to grow slowly and often result in spontaneous bleeding when
tumor diameter is beyond 4 cm (1).
Although TSC can seriously affect the health of patients and cause
a heavy economic burden (6,7), it is difficult for a physician or
surgeon, particularly those with less experience, to make a
definitive diagnosis, not to mention to provide effective
management in a timely manner, when patients present with atypical
organ involvement or few systemic clinical features (8,9). The
clinical diagnostic criteria of TSC includes 11 major and 6 minor
features, and the diagnosis is difficult when patients' symptoms do
not fully align with the definitive diagnosis, which requires at
least two major features or one major feature with two or more
minor features (2). In these cases,
the family medical history may be useful. However, to the best of
our knowledge, the published literature on TSC genealogy has been
mostly comprised of case reports, and the maximum number of family
members was three in a single study (10,11),
revealing that data on TSC genealogy is lacking.
The present study performed retrospective detailed
analysis of the characteristics of clinical genetics, imaging
studies, laboratory tests and treatments in 6 patients with
TSC-associated renal angiomyolipoma (RAML) and their family
members. The study focused on renal involvement, which can
significantly affect the lives of TSC patients and leave 25–50% at
risk of hemorrhage (12), and aimed
to provide experiences of the diagnosis and treatment of TSC-RAML
for use in future clinical practice.
Materials and methods
General patient information
Within the 49 family members of the 6 pedigrees,
there were 18 TSC patients, including 11 TSC-RAML patients, 5 TSC
patients without RAML and 2 TSC patients without abdominal imaging
data. The 6 probands and their family members were all referred to
the Urological Surgery Clinic (Zhengzhou, China) between January
2012 and December 2014. Of these, 1 family was from The First
Affiliated Hospital of Zhengzhou University (Zhengzhou, Henan,
China) and the remaining 5 were from Peking Union Medical College
Hospital (Beijing, China). In total, 7 out of the 11 TSC-RAML
patients had a history of intermittent abdominal pain. Once
informed consent had been obtained from each patient, individual
data and the family history were collected in detail. The present
study was approved by the Ethics Committee of Peking Union Medical
College Hospital (Beijing, China).
Clinical data of patients
All TSC patients underwent blood routine
examinations and blood biochemistry analysis to assess the degree
of anemia and the function of the liver and kidneys. Computed
tomography and renal dynamic imaging were conducted in the TSC-RAML
patients to reevaluate the current situation with regard to renal
involvement and unilateral renal function. The 2 TSC patients
without abdominal imaging data refused to undergo the radiological
examinations. A TSC1/2 gene mutation was detected in 2 families
when blood samples were sent for high-throughput sequencing
analysis to the Beijing Genomics Institute (Shenzhen, China) in
accordance with the patients' wishes. Partial renal resection was
performed in 3 TSC-RAML patients due to the high risk of bleeding
with growth of the large renal lesions, which were relatively
independent and superficial. Another 2 TSC-RAML patients were
treated with mechanistic target of rapamycin (mTOR) inhibitor
(everolimus, 10 mg/day, in a single oral dose, for one year).
Immunohistochemical staining
The TSC-RAML specimens were fixed in 10% formalin
solution for 24 h at 4°C in the refrigerator, underwent
dehydration, transparent and wax immersion, and were sliced into 5
µm sections. Dewaxing and rehydration: each of xylene I and II for
20 min, 100% alcohol for 10 min, the each of 95, 80 and 70% alcohol
for 5 min. Sections were incubated in 3% hydrogen peroxide at 37°C
for 10 min to block and inactivate the endogenous peroxidase, and
boiled in 0.01 M citrate buffer (pH 6.0) for 15 min at 95°C, then
naturally cooled over 20 min for antigen retrieval. Hematoxylin and
eosin staining procedures were performed at room temperature for 60
min, and then observed under a light microscope at magnification,
×100, followed by immunohistochemical staining procedures: The
primary antibodies were: anti-p-mTOR (Ser2448; Santa Cruz
Biotechnology, Inc., Dallas, TX, USA; cat. no. sc-101738; 1:250),
anti-S6K1 (phospho T389; Abcam, Cambridge, UK; cat. no. ab126818;
1:500) and anti-eIF4EBP1 (phospho T70; Abcam; cat. no. ab75831;
1:200), and the horseradish peroxidase (HRP)-labeled secondary
antibody was goat anti-rabbit immunoglobulin G (Novoprotein,
Summit, NJ, USA; cat. no. AB501; 1:50). To each section, 50 µl of
each of the primary antibody (incubated for 1 h at 37°C) or
secondary antibody (incubated for 30 min at 37°C), HRP-labeled
streptavidin working solution (concentration: 0.5%) and
diaminobenzidine solution (concentration: 0.01%) were added
sequentially. The reaction was terminated with distilled water once
brown granules were observed using a light microscope at
magnification, ×100. The hematoxylin staining was then performed
again lasting 30 sec, and then put in double distilled water
lasting 5 min.
Results
Clinical characteristics in
pedigrees
Pedigree charts of the 6 families are shown in
Fig. 1, including the 6 probands and
12 family members (female, 13; male, 5). The mean diagnostic age
was 34.22±17.73 years (Table I).
Within the 18 TSC patients, 15 cases were consistent with the
definite diagnosis criteria, and the remaining 3 were associated
with possible diagnosis criteria (13). The TSC-RAML patients accounted for
~61% (11/18) of the subjects, excluding the 2 cases without
abdominal imaging. The 6 probands were all patients with TSC-RAML
(female, 4; male, 2), with the diagnostic age ranging between 9 and
39 years (mean, 27.00±11.45 years). With regard to family location,
5 were from rural areas and 1 was from an urban area.
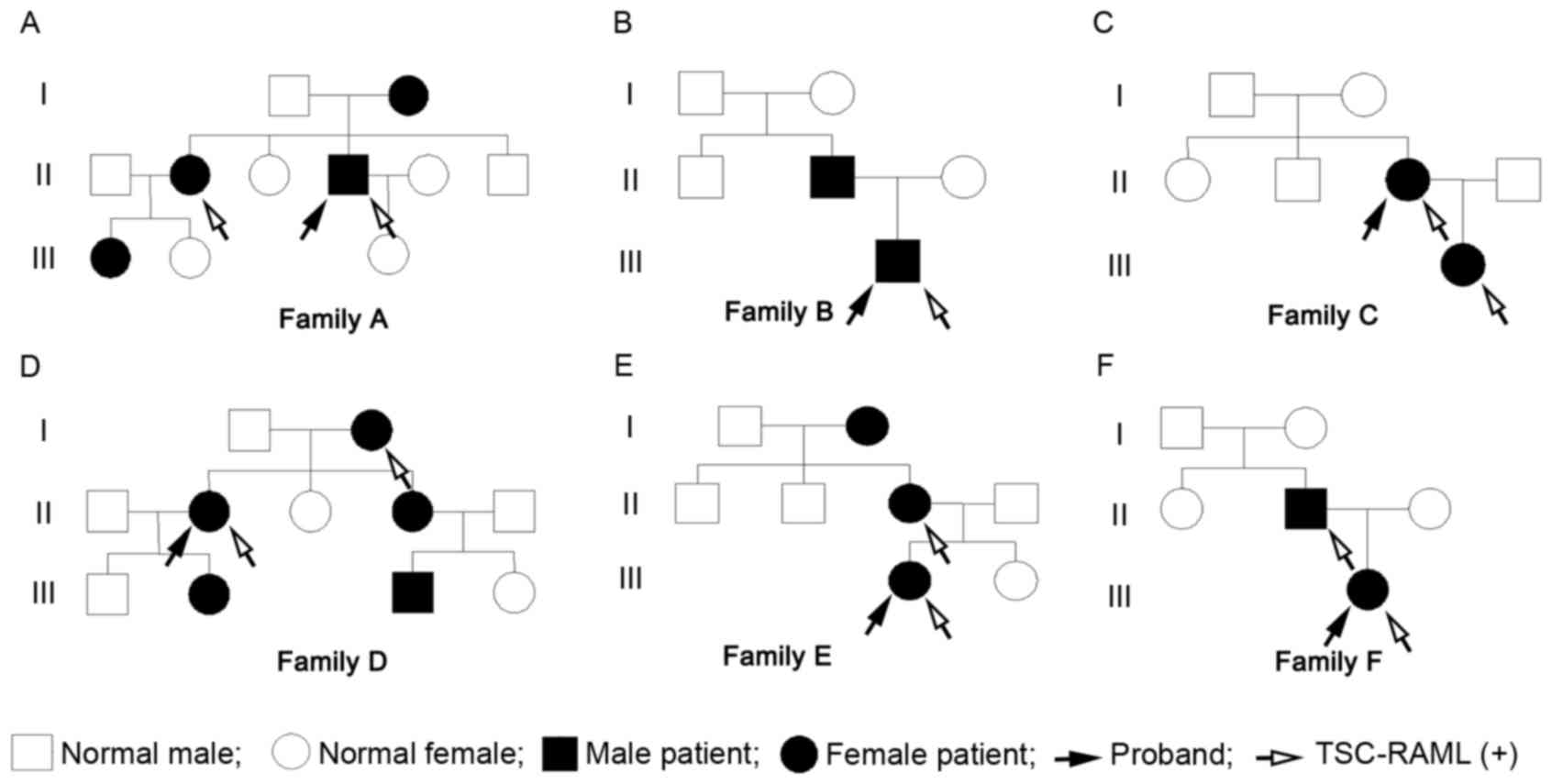 | Figure 1.(A-F) Pedigree charts of the 6
families. The pedigree charts include 18 TSC patients (female, 13;
male, 5), of which, 11 patients have been diagnosed with TSC-RAML
(female, 8; male, 3). The 6 probands are all TSC-RAML patients, of
which, just the patient from family CII is the first generation
with a pathogenic mutation, and the remaining 5 are inherited from
the previous generation. TSC-RAML, tuberous sclerosis
complex-associated renal angiomyolipoma. |
 | Table I.Characteristics of the 18 TSC
patients. |
Table I.
Characteristics of the 18 TSC
patients.
| Pedigree | Patient | Accord with definite
diagnosis (yes/no) | Age at TSC diagnosis,
years | Age at RAML
diagnosis, years | Maximum diameter of
TSC-RAML, cm | Urban/rural patient
location |
|---|
| Family A | 1 | Yes | 61 | Unknown | Unknown | Urban |
|
| 2 | Yes | 42 | 31 | 12.7 | Urban |
|
|
3a | Yes | 36 | 28 | 3.8 | Urban |
|
| 4 | No | 19 | – | – | Urban |
| Family B | 1 | Yes | 43 | – | – | Rural |
|
|
2a | Yes | 9 | 14 | 10.3 | Rural |
| Family C |
1a | Yes | 34 | 34 | 16 | Rural |
|
| 2 | Yes | 12 | 12 | 1.2 | Rural |
| Family D | 1 | Yes | 60 | 56 | 5.9 | Rural |
|
|
2a | Yes | 39 | 37 | 10.4 | Rural |
|
| 3 | No | 35 | – | – | Rural |
|
| 4 | Yes | 16 | – | – | Rural |
|
| 5 | No | 12 | – | – | Rural |
| Family E | 1 | Yes | 68 | Unknown | Unknown | Rural |
|
| 2 | Yes | 45 | 43 | 7.2 | Rural |
|
|
3a | Yes | 24 | 22 | 32.5 | Rural |
| Family F | 1 | Yes | 41 | 27 | 16.3 | Rural |
|
|
2a | Yes | 20 | 21 | 10 | Rural |
Imaging and laboratory
examinations
The unilateral glomerular filtration rate in each of
the 11 TSC-RAML patients ranged between 27.20 and 60.10 ml/min
(mean, 42.55±9.73 ml/min, normal, 40~60 ml/min), the serum
creatinine level ranged between 40.00 and 90.00 µmol/l (mean,
64.84±16.15 µmol/l; normal, male: 44–132 µmol/l, female: 70–106
µmol/l), the hemoglobin concentration ranged between 76.00 and
140.00 g/l (mean, 107.73±21.04 g/l; normal, male: 120–160 g/l,
female: 110–150 g/l) and the maximum diameter of the TSC-RAMLs
ranged between 1.20 and 32.50 cm (mean, 11.48±8.40 cm). In families
B and C, the maximum diameters of the tumors of the proband and
their family members were 10.3 and 0 cm, and 16 and 1.2 cm,
respectively, and the pathogenic gene mutations were TSC1
c.733C>T and TSC2 c.788_789insC, respectively. There were also a
number of non-pathogenic mutations (Table II). The systolic blood pressure
ranged between 70.00 and 138.00 mmHg (mean, 108.00±20.59 mmHg;
normal, <120 mmHg), and the diastolic blood pressure ranged
between 40.00 and 83.00 mmHg (mean, 64.91±13.01 mmHg; normal,
<80 mmHg).
| Table II.TSC gene mutations in two
families. |
Table II.
TSC gene mutations in two
families.
| Pedigree | Patient | Gene | Mutation | Pathogenicity |
|---|
| Family B | Proband | TSC1 | c.733C>T | Pathogenic |
|
|
| TSC1 |
c.2626-4_-3insTT | Non-pathogenic |
|
|
| TSC2 | c.5161-9C>T | Non-pathogenic |
|
|
| TSC2 | p.Asp1734Asp | Non-pathogenic |
|
| Family member | TSC1 | c.733C>T | Pathogenic |
| Family C | Proband | TSC2 | c.788_789insC | Pathogenic |
|
|
| TSC1 | c.1631G>A | Non-pathogenic |
|
| Family member | TSC2 | c.788_789insC | Pathogenic |
|
|
| TSC2 | c.856A>G | Non-pathogenic |
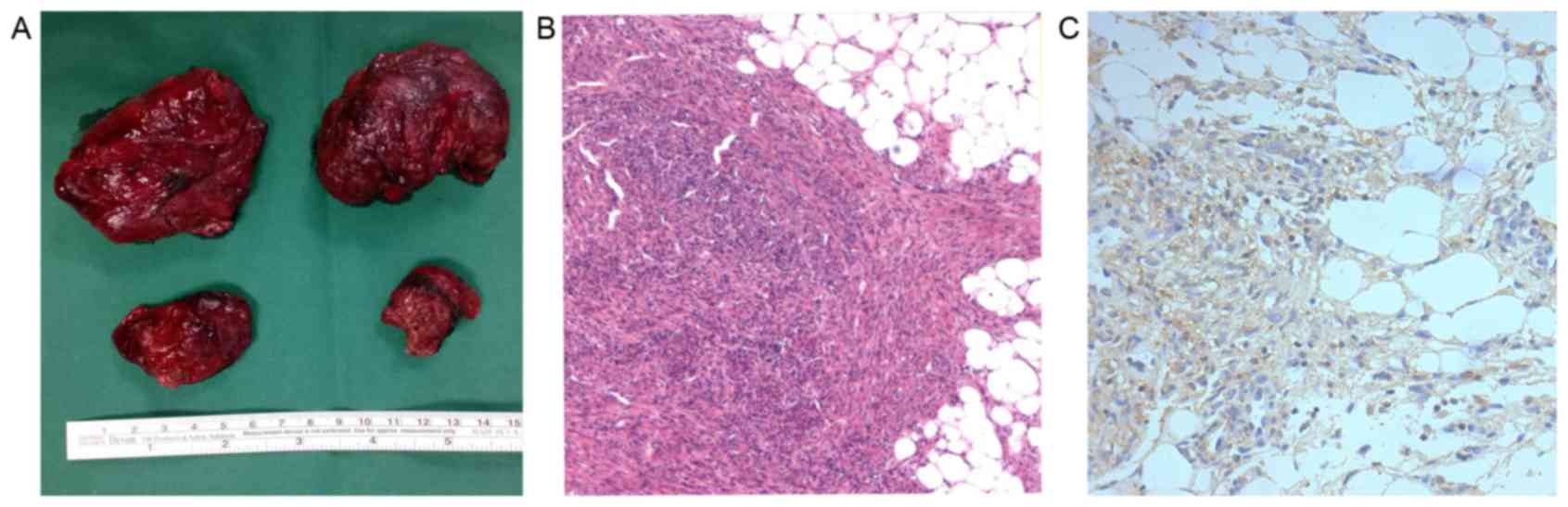
Surgical treatment and
immunohistochemical staining
Due to a high risk of bleeding, as well as the
relatively isolated and protruding nature of the RAMLs, 3 patients
underwent a partial nephrectomy by means of open surgery,
preserving the normal renal tissue as much as possible.
Pathological results showed a large number of smooth muscle cells
and fat cells, as well as certain malformed blood vessels and
aneurysms in part of the visual field. Immunohistochemistry
determined the positive expression of p-mTOR in the TSC-RAML
tissues, particularly in the cells of the vascular wall (Fig. 2).
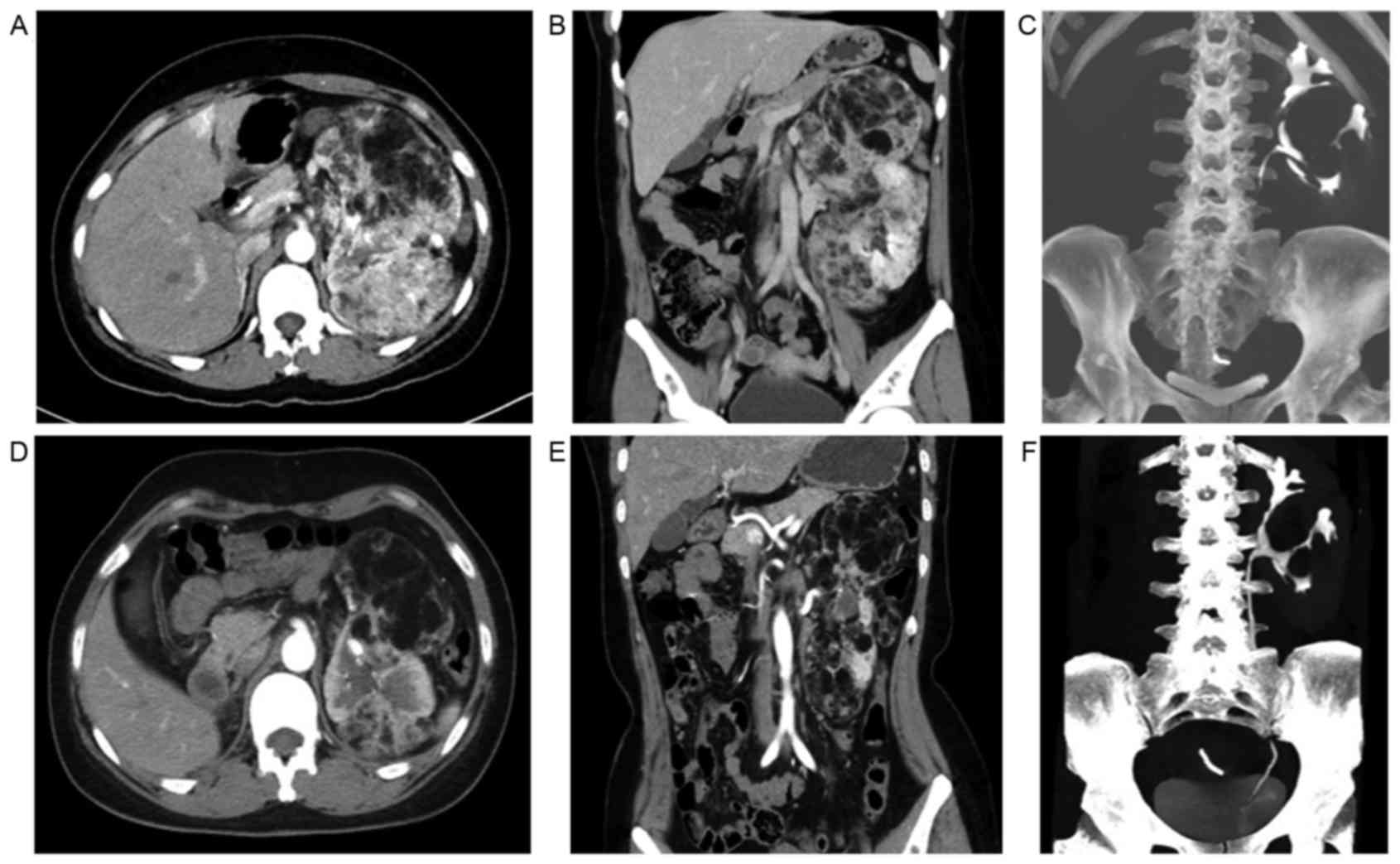
Everolimus treatment
Until the time of data collection, 2 of the TSC-RAML
patients had been treated with everolimus (10 mg/day, in a single
oral dose) for 3 months. The intermittent abdominal pain
disappeared completely, and the abdominal circumference of 1
patient was reduced by >3 cm compared with the initial data 3
months ago (measured while fasting in the morning). The maximum
diameter of the TSC-RAML decreased by 4.90 and 5.30 cm,
respectively, in the 2 patients, and the morphology of the renal
collecting system became more regular when compared with the
baseline data (Fig. 3). Changes to
the facial angiofibromas in 1 patient are shown in Fig. 4, from which it can be observed that
the angiofibromas had become much flatter, smaller and lighter in
color compared with those prior to therapy.
Discussion
TSC is caused by pathogenic mutation of the
tumor-suppressing genes, TSC1 or TSC2, which encode hamartin and
tuberin, respectively, and normally down-regulate mTOR complex 1
(mTORC1). Once a pathogenic mutation occurs in either TSC1 or TSC2,
the dysfunction of hamartin-tuberin complex will terminate its
negative regulation of the activation of mTORC1 and its downstream
regulators, resulting in TSC (14,15).
TSC can be diagnosed by either genetic or clinical
diagnostic criteria according to the updated recommendations of the
2012 International Tuberous Sclerosis Complex Consensus Conference
(11). However, although experts have
agreed that identification of a pathogenic mutation in either TSC1
or TSC2 is an independent diagnostic criterion, 10–30% of TSC
patients have no pathogenic mutation, which means that a normal
result does not exclude TSC (13,16,17).
Additionally, due to the relatively high medical costs and
technical constraints, the use of clinical diagnostic criteria,
including 11 major features and 6 minor features, remain the main
diagnostic method.
However, the majority of TSC-RAML patients, who may
have marked clinical signs and symptoms, including recurrent
abdominal pain, reduced appetite, weight loss, an abdominal mass or
progressive abdominal expansion, are not diagnosed as early as
possible or treated in a timely manner. In the present study, the
mean diagnostic age of the 6 probands was 27 years, and that of the
18 TSC patients was ~34 years, suggesting that diagnosis and
treatment occurs relatively late. The main causes of this may be as
follows: i) The relative lack of knowledge about TSC, leading to a
non-comprehensive understanding of the rare and variable nature of
the disease by doctors; ii) a relatively remote place of residence,
resulting in limited access to good health resources; iii) the
extremely variable characteristics of TSC, meaning that it cannot
easily be identified when patient symptoms do not fully accord with
the definitive diagnosis: Two major features or one major feature
with two or more minor features (13). In the present study, 5 families were
from rural areas, and 16.67% of TSC patients met the possible
diagnostic criteria, with a final definite diagnosis benefiting
from the contribution of the family history.
TSC is an autosomal dominant genetic disease, and
the genetic diversity of the current cohort is shown in Fig. 1. There were 18 TSC patients in the 6
pedigrees, accounting for only ~37% of subjects, and 11 with
TSC-RAML, accounting for only ~22%. Within the TSC patients,
TSC-RAML cases account for ~61%, which is similar to the data
(55–80%) reported by De Waele et al (18). The maximum diameters of TSC-RAML also
varied widely among individuals in the present study, ranging from
1.2 to 32.50 cm (mean, 11.48±8.40 cm), even amongst those with the
same pathogenic mutation. Results of genetic testing in families B
and C revealed that the proband and their family members not only
had the same pathogenic mutation, but that they also had other
different non-pathogenic mutations, which could not lead to
nucleotide changes, but may interfere with gene transcription and
protein synthesis, thereby affecting the activity of the mTOR
signaling pathway and promoting or inhibiting cell
proliferation.
Although lesions are multiple and bilateral in
almost all TSC-RAML patients, with relatively large diameters that
result in pelvicaliceal deformation and renal contour
disappearance, it appears that there is little impact on renal
function. In the 11 TSC-RAML patients, the mean serum creatinine
was nearly 65 µmol/l, and the mean unilateral renal glomerular
filtration rate was ~42 ml/min; these were in the normal range.
Even for the patient with the largest TSC-RAML (diameter, 32.50
cm), the serum creatinine level was 40.00 µmol/l, and the
unilateral renal glomerular filtration rate was 27.20 ml/min (left)
and 60.10 ml/min (right), respectively. Nevertheless, the
concentration of hemoglobin gradually decreases with the increasing
diameter of the renal lesions; for example, it was 75.00 g/l in the
patient with the largest TSC-RAML, which is lower than the mean
level of 111.19±25.04 g/l. This results from the intermittent
bleeding as the renal lesions grow, since such patients present
mostly with a history of recurrent abdominal pain, and even
multiple aneurysm formation and intralesional hemorrhage in RAMLs
have been confirmed in certain patients by imaging.
As the clinical features of TSC-RAML are bilateral
and multiple in nature, and as the volume of RAMLs tends to
increase gradually with age (19),
renal function should be preserved as much as possible in the
treatment process. Therapies such as selective arterial
embolization, partial nephrectomy and ablation are not preferred as
the first-line therapies (20),
unless the patients are at an extremely high risk of bleeding, or
have experienced repeated spontaneous bleeding or active bleeding
with ineffective conservative treatment. Only 3 patients in the
present study underwent partial nephrectomy due to the high risk of
bleeding, and the pathological results showed the positive
expression of p-mTOR, indicating the excessive activation of the
mTOR signaling pathway, which also has been confirmed in TSC brain
and skin lesions (21,22). Bissler et al (23) reported preliminary results of the
clinical efficacy and safety of everolimus, which is an inhibitor
of the mTOR signaling pathway, on RAML in patients with TSC or
sporadic lymphangiomyomatosis, having demonstrated a significant
reduction in AML volume and safety for oral administration
(23). A sustained reduction in RAML
volume with continued everolimus treatment was also confirmed in
later results (24). In the present
study, following treatment with everolimus for 3 months, the
maximum diameter of TSC-RAML in the 2 patients decreased by 4.90
and 5.30 cm, respectively, the intermittent abdominal pain
disappeared completely and the facial angiofibromas improved.
In conclusion, as a rare autosomal dominant genetic
disease, TSC cannot be easily diagnosed or treated in a timely
manner due to its variability, the relative lack of TSC data and
the level of local medical services. The growth of TSC-RAML may
increase the risk of bleeding and reduce the level of hemoglobin,
but it does not greatly affect renal function. Individual
differences in TSC-RAML exist even in cases with the same
pathogenic gene mutation, probably as a result of the presence of
other non-pathogenic gene mutations that do not encode proteins but
regulate the translation process. The results of the present study
suggested that p-mTOR expression was positive in TSC-RAML, as
determined by immunohistochemical analysis, and the results of
previous clinical trials and the present study also demonstrated
the promising clinical efficacy of everolimus. Therefore, mTOR
inhibitors may be an optimal therapy for treating TSC, allowing
surgical intervention to be used only for cases with a high risk of
bleeding or unexpected hemorrhage.
Acknowledgements
The authors would like to thank Dr Y. Cai, from the
Department of Urology, Peking Union Medical College Hospital,
Chinese Academy of Medical Sciences and Peking Union Medical
College (Beijing, China), for support by providing the medical
records of the TSC-RAML patients in the present study.
Glossary
Abbreviation
Abbreviations:
|
TSC-RAML
|
tuberous sclerosis complex-associated
renal angiomyolipoma
|
References
|
1
|
Curatolo P, Bombardieri R and Jozwiak S:
Tuberous sclerosis. Lancet. 372:657–668. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Krueger DA and Northrup H; International
Tuberous Sclerosis Complex Consensus Group, . Tuberous sclerosis
complex surveillance and management: Recommendations of the 2012
international tuberous sclerosis complex consensus conference.
Pediatr Neurol. 49:255–265. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Rosser T, Panigrahy A and McClintock W:
The diverse clinical manifestations of tuberous sclerosis complex:
A review. Semin Pediatr Neurol. 13:27–36. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
O'Callaghan FJ, Noakes MJ, Martyn CN and
Osborne JP: An epidemiological study of renal pathology in tuberous
sclerosis complex. BJU Int. 94:853–857. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rakowski SK, Winterkorn EB, Paul E, Steele
DJ, Halpern EF and Thiele EA: Renal manifestations of tuberous
sclerosis complex: Incidence, prognosis and predictive factors.
Kidney Int. 70:1777–1782. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Demuth D, Nasuti P, Lucchese L, Gray L,
Pinnegar A and Magestro M: Economic impact of patients with
tuberous sclerosis complex (tsc) in the Uk: A retrospective
database analysis in the clinical practice research datalink
(Cprd). Value in Health. 17:A1372014. View Article : Google Scholar
|
|
7
|
Rentz AM, Skalicky AM, Liu Z, Wheless JW,
Dunn DW, Frost MD, Nakagawa J, Magestro M and Prestifilippo J:
Tuberous sclerosis complex: A survey of health care resource use
and health burden. Pediatr Neurol. 52:435–441. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kakkar A, Vallonthaiel AG, Sharma MC, Bora
G, Panda A and Seth A: Composite renal cell carcinoma and
angiomyolipoma in a patient with Tuberous sclerosis: A diagnostic
dilemma. Can Urol Assoc J. 9:E507–E510. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Falsafi P, Taghavi-Zenouz A,
Khorshidi-Khiyavi R, Nezami N and Estiar MA: A case of tuberous
sclerosis without multiorgan involvement. Glob J Health Sci.
7:124–131. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Xue G, Han X, Ren S and Yue X: An Analysis
of 11 Cases of Tuberous Sclerosis from Three Genealogies. Chin J
Neuroimmunol and Neurol. 6:249–252. 1999.
|
|
11
|
Zhang Y, Gan J, Pu Z, Xu Mm, Wang LF, Li
YH and Liu ZG: TSC1 R509X mutation in a chinese family with
tuberous sclerosis complex. Neuromolecular Med. 17:202–208. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dixon BP, Hulbert JC and Bissler JJ:
Tuberous sclerosis complex renal disease. Nephron Exp Nephrol.
118:e15–e20. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Northrup H and Krueger DA; International
Tuberous Sclerosis Complex Consensus Group, . Tuberous sclerosis
complex diagnostic criteria update: Recommendations of the 2012
international tuberous sclerosis complex consensus conference.
Pediatr Neurol. 49:243–254. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tee AR, Manning BD, Roux PP, Cantley LC
and Blenis J: Tuberous sclerosis complex gene products, Tuberin and
Hamartin, control mTOR signaling by acting as a GTPase-activating
protein complex toward Rheb. Curr Biol. 13:1259–1268. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wataya-Kaneda M: Mammalian target of
rapamycin and tuberous sclerosis complex. J Dermatol Sci.
79:93–100. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sancak O, Nellist M, Goedbloed M,
Elfferich P, Wouters C, Maat-Kievit A, Zonnenberg B, Verhoef S,
Halley D and van den Ouweland A: Mutational analysis of the TSC1
and TSC2 genes in a diagnostic setting: Genotype--phenotype
correlations and comparison of diagnostic DNA techniques in
Tuberous Sclerosis Complex. Eur J Hum Genet. 13:731–741. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Au KS, Williams AT, Roach ES, Batchelor L,
Sparagana SP, Delgado MR, Wheless JW, Baumgartner JE, Roa BB,
Wilson CM, et al: Genotype/phenotype correlation in 325 individuals
referred for a diagnosis of tuberous sclerosis complex in the
United States. Genet Med. 9:88–100. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
De Waele L, Lagae L and Mekahli D:
Tuberous sclerosis complex: The past and the future. Pediatr
Nephrol. 30:1771–1780. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Seyam RM, Bissada NK, Kattan SA, Mokhtar
AA, Aslam M, Fahmy WE, Mourad WA, Binmahfouz AA, Alzahrani HM and
Hanash KA: Changing trends in presentation, diagnosis and
management of renal angiomyolipoma: Comparison of sporadic and
tuberous sclerosis complex-associated forms. Urology. 72:1077–1082.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
DiMario FJ Jr, Sahin M and
Ebrahimi-Fakhari D: Tuberous sclerosis complex. Pediatr Clin North
Am. 62:633–648. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ruppe V, Dilsiz P, Reiss CS, Carlson C,
Devinsky O, Zagzag D, Weiner HL and Talos DM: Developmental brain
abnormalities in tuberous sclerosis complex: A comparative tissue
analysis of cortical tubers and perituberal cortex. Epilepsia.
55:539–550. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chan JY, Wang KH, Fang CL and Chen WY:
Fibrous papule of the face, similar to tuberous sclerosis
complex-associated angiofibroma, shows activation of the mammalian
target of rapamycin pathway: Evidence for a novel therapeutic
strategy? PLoS One. 9:e894672014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bissler JJ, Kingswood JC, Radzikowska E,
Zonnenberg BA, Frost M, Belousova E, Sauter M, Nonomura N,
Brakemeier S, de Vries PJ, et al: Everolimus for angiomyolipoma
associated with tuberous sclerosis complex or sporadic
lymphangioleiomyomatosis (EXIST-2): A multicentre, randomised,
double-blind, placebo-controlled trial. Lancet. 381:817–824. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bissler JJ, Kingswood JC, Radzikowska E,
Zonnenberg BA, Frost M, Belousova E, Sauter M, Nonomura N,
Brakemeier S, de Vries PJ, et al: Everolimus for renal
angiomyolipoma in patients with tuberous sclerosis complex or
sporadic lymphangioleiomyomatosis: Extension of a randomized
controlled trial. Nephrol Dial Transplant. 31:111–119. 2015.
View Article : Google Scholar : PubMed/NCBI
|