Introduction
Approximately 20–30% of breast cancers ultimately
metastasize or recur. The treatments for metastatic or recurrent
breast cancer (MBC) are diverse, and treatment innovations have
improved the prognosis and life expectancy of MBC patients
(1). More than 20 years ago, only
2–3% of MBC patients achieved a clinical complete response (cCR)
and the 10-year survival rate was only about 5% (2–5),
http://ganjoho.jp/reg_stat/). Today, the
10-year survival rate of MBC is 15.6%, and the 5-year survival rate
is 32.6%, according to the Research Group of the Japanese National
Cancer Research Center (6).
Treatment innovations in the past 10 years include
the use of small molecule inhibitors and anti-human epidermal
growth factor receptor 2 (HER2) antibodies. In recent clinical
trials including anti-HER2 therapy, 10–20% of patients with
metastatic breast cancer achieved a cCR (7–9). However,
the factors responsible for a cCR are not known, nor is it known
when patients discontinue treatment once a cCR is achieved. Owing
to potential adverse events, unnecessary treatments should be
avoided.
In recent years, many research groups have
investigated the value of anticancer immune responses and the
hematological components of the systemic inflammatory response
specifically for use in predicting outcome. Some studies have
evaluated the prognostic and predictive importance of
tumor-infiltrating lymphocytes (TILs) in breast cancer (10,11). And
some have reported that the combination of the hematological
components of the systemic inflammatory response, as the
neutrophil-lymphocyte ratio (NLR) have prognostic value in a
variety of cancers (12–16).
Therefore, the aim of this study is to analyze the
association between cCR and overall survival (OS), and TILs or NLR
might be prognositic factor in metastatic breast cancer.
Patients and methods
Patients
A hundred and seventy-one patients with
histologically or clinically confirmed MBC who were consecutively
treated at the Shiga Medical Center for Adults (Moriyama, Shiga,
Japan) between 2011 and 2017 (Table
I). Patients had either de novo MBC, a recurrence of a local
breast cancer, or distant metastases that appeared after treatment
of the primary cancer. Medical records were reviewed in detail.
Patients who achieved a cCR were defined as those with no evidence
of disease after treatment for MBC (i.e., no evidence of clinical
or radiological disease according to the Response Evaluation
Criteria in Solid Tumors and as evaluated via computed tomography,
magnetic resonance imaging, or positron emission tomography). The
frequency and modality of radiographic imaging were at the
discretion of the treating physician.
 | Table I.Characteristics of patients with
metastatic or recurrent breast cancer. |
Table I.
Characteristics of patients with
metastatic or recurrent breast cancer.
| Variable | All patients
(n=171) | cCR (n=32) | non-cCR (n=139) | P-value |
|---|
| Follow-up period
(months) |
|
|
| 0.135 |
|
Median | 44 | 60 | 47 |
|
|
Range | 0–271 | 1–247 | 0–271 |
|
| Age at primary breast
cancer (y.o.) |
|
|
| 0.142 |
|
Median | 55 | 52 | 55 |
|
|
Range | 29–89 | 32–75 | 29–89 |
|
| Age at metastatic
breast cancer (y.o.) |
|
|
| 0.232 |
|
Median | 59 | 57 | 59 |
|
|
Range | 31–92 | 32–81 | 31–92 |
|
| Disease stage at
primary diagnosis, no. (%) |
|
|
| 0.003 |
| Stage
0 | 4 (2.3) | 2 (6.3) | 2 (1.4) |
|
| Stage
I | 24 (14.0) | 11 (34.3) | 13 (9.4) |
|
| Stage
II | 42 (24.6) | 5 (15.6) | 37 (26.6) |
|
| Stage
III | 46 (27.0) | 8 (25.0) | 38 (27.3) |
|
| Stage
IV | 38 (22.2) | 4 (12.5) | 34 (24.5) |
|
|
Unknown | 17 (9.9) | 2 (6.3) | 15 (10.8) |
|
| Histology, no.
(%) |
|
|
| 0.619 |
| Invasive
ductal | 148 (86.4) | 30 (93.8) | 118 (84.9) |
|
| Invasive
lobular | 7 (4.1) | 0 (0.0) | 7 (5.0) |
|
|
Mixed | 3 (1.8) | 0 (0.0) | 3 (2.2) |
|
|
Sarcoma | 1 (0.6) | 0 (0.0) | 1 (0.7) |
|
|
Other | 9 (5.3) | 2 (6.2) | 7 (5.0) |
|
|
Unknown | 3 (1.8) | 0 (0.0) | 3 (2.2) |
|
| Receptor status,
no. (%) |
|
|
| 0.358 |
|
ER+/HER2- | 93 (54.4) | 19 (59.4) | 74 (53.2) |
|
|
ER+/HER2+ | 23 (13.5) | 4 (12.5) | 19 (13.7) |
|
|
ER-/HER2+ | 20 (11.7) | 6 (18.8) | 14 (10.1) |
|
|
ER-/HER2- | 28 (16.4) | 2 (6.3) | 26 (18.7) |
|
|
Unknown | 7 (4.0) | 1 (3.0) | 6 (4.3) |
|
| Ki-67 labeling
index |
|
|
| 0.885 |
| Median,
SD | 20.3±19.6 | 20.5±23.7 | 20.9±18.6 |
|
|
Range | 1.5–90 | 1.5–90 | 2–80 |
|
| Site No. of
metastasis/recurrence |
|
|
|
<0.001 |
| 1 | 52 (30.4) | 25 (78.1) | 27 (19.4) |
|
| 2 | 48 (28.1) | 6 (18.8) | 42 (30.2) |
|
| ≥3 | 71 (41.5) | 1 (3.1) | 70 (50.4) |
|
| No. of visceral
metastasis PgR status |
|
|
|
<0.001 |
| 0 | 51 (29.8) | 25 (78.1) | 26 (18.7) |
|
| 1 | 76 (44.5) | 6 (18.8) | 70 (50.4) |
|
| 2 | 40 (23.4) | 1 (3.1) | 39 (28.1) |
|
| 3 | 4 (2.3) | 0 (0.0) | 4 (2.8) |
|
| NLR at diagnosis of
metastasis/recurrence |
|
|
|
<0.001 |
| Median,
SD | 2.44±1.97 | 1.46±0.35 | 2.66±2.16 |
|
|
Range | 0.83–17.50 | 0.93–2.77 | 0.83–17.50 |
|
In patients with primary stage IV disease, the
abundance of TILs was approximated by examining hematoxylin- and
eosin-stained tumor samples under medium power (100×). This
examination was limited to patients with stage IV disease because
they did not receive prior treatments, which might have affected
the TIL score. All samples were reviewed by pathologists. TIL score
was defined as the percentage of the tumor and adjacent stroma area
infiltrated by lymphocytes; the scores were classified as low
(<10%), intermediate (≥10%, 50%>) or high (≥50%) (10,11).
Immunohistochemistry was performed to identify the antigens (CD4
and CD8) in the cell membranes of the TILs. Furthermore,
neutrophils are easily affected by factors like infection or
therapeutic exposure. In order to minimize the effects of treatment
or tumor progression, NLRs were determined in blood samples at
diagnosis.
The study design was approved by Ethics Review Board
of Shiga Medical Center for Adults according to the Declaration of
Helsinki.
Statistics
Qualitative data were examined for differences
between the cCR and non-cCR groups; both patient and tumor
characteristics were examined, and the chi-square test was used. OS
was defined as the interval between the date of diagnosis and the
date of the last follow-up or death from any cause. OS was
calculated using Kaplan-Meier estimates, and differences in OS were
evaluated using the log-rank test. A P-value <0.05 was
considered significant. A multivariable Cox proportional hazards
regression model was used to identify OS-associated factors. To
estimate effects of each factor, hazard ratios with 95% confidence
intervals were calculated. Data were analyzed using Stat Mate V for
Win & Mac Hybrid software (ATMS Co., Ltd, Tokyo, Japan).
Results
The median follow-up time for the 171 patients with
MBC in our study was 44 months (range, 0–271 months). Thirty-two
(18.7%) patients, including 10 patients with
HER2+-disease (5.8%), had a cCR, with no evidence of
disease or a secondary recurrence for 40 months (range, 0–200
months); no patient died during 40 months. All cCR patient
terminated treatment after the first or second line of MBC therapy.
Most of them had multiple metastatic sites, limited to median 2
organs (range, 1–3 organs). The median time to achieve a cCR was 20
months (range, 0–85 months). Although patients who had achieved cCR
included patients who had undergone metastatic site resection
without systemic therapy, usually their main therapy was systemic
therapy. Compared with non-cCR patients, cCR patients had fewer
sites of metastases or recurrences (P<0.001), fewer visceral
metastases (P<0.001), and a lower NLR (P<0.001) and were
diagnosed with primary breast cancer at an earlier stage
(P=0.003).
Among the 120 (70.2%) patients with visceral
metastases, 7 patients (5.8%) achieved a cCR: 5 patients received
systemic therapy without surgery, and 2 patients underwent
resection for brain and lung metastases, respectively. In patients
with visceral metastases, the NLR at diagnosis was significantly
lower in the cCR (n=7) than the non-cCR group (n=25, P<0.001).
The characteristics of patients with visceral metastasis are
summarized in Table II.
| Table II.Characteristics of patients with
visceral metastases. |
Table II.
Characteristics of patients with
visceral metastases.
| Variables | All patients
(n=120) | cCR (n=7) | non-cCR
(n=113) | P-value |
|---|
| Follow-up period
(months) |
|
|
| 0.153 |
|
Median | 44 | 98 | 40 |
|
|
Range | 0–247 | 13–247 | 0–171 |
|
| Age at primary
breast cancer (y.o.) |
|
|
| 0.222 |
|
Median | 55 | 49 | 55 |
|
|
Range | 29–89 | 32–61 | 29–89 |
|
| Age at metastatic
breast cancer (y.o.) |
|
|
| 0.077 |
|
Median | 59 | 50 | 59 |
|
|
Range | 31–89 | 32–61 | 31–89 |
|
| Disease stage at
primary diagnosis, no. (%) |
|
|
| 0.942 |
| Stage
0 | 2 (1.7) | 0 (0.0) | 2 (1.8) |
|
| Stage
I | 10 (8.3) | 1 (14.2) | 9 (8.0) |
|
| Stage
II | 33 (27.5) | 2 (28.6) | 31 (27.4) |
|
| Stage
III | 33 (27.5) | 2 (28.6) | 31 (27.4) |
|
| Stage
IV | 30 (25.0) | 2 (28.6) | 28 (24.8) |
|
|
Unknown | 12 (10.0) | 0 (0.0) | 12 (10.6) |
|
| Histology, no.
(%) |
|
|
| 0.964 |
|
Invasive ductal | 106 (88.4) | 7 (100.0) | 99 (87.6) |
|
|
Invasive lobular | 4 (3.3) | 0 (0.0) | 4 (3.5) |
|
|
Mixed | 1 (0.8) | 0 (0.0) | 1 (0.9) |
|
|
Sarcoma | 1 (0.8) | 0 (0.0) | 1 (0.9) |
|
|
Other | 6 (5.0) | 0 (6.2) | 6 (5.3) |
|
|
Unknown | 2 (1.7) | 0 (0.0) | 2 (1.8) |
|
| Receptor status,
no. (%) |
|
|
| 0.983 |
|
ER+/HER2- | 65 (54.2) | 4 (57.1) | 61 (54.0) |
|
|
ER+/HER2+ | 15 (12.5) | 1 (14.3) | 14 (12.4) |
|
|
ER-/HER2+ | 14 (11.7) | 1 (14.3) | 13 (11.5) |
|
|
ER-/HER2- | 22 (18.3) | 1 (14.3) | 21 (18.6) |
|
|
Unknown | 4 (3.3) | 0 (0.0) | 4 (3.5) |
|
| Ki-67 labeling
index |
|
|
| 0.352 |
| Median
± SD | 22.3±19.6 | 13.3±20.6 | 23.2±18.9 |
|
|
Range | 1.5–80 | 1.5–50 | 2–80 |
|
| Site no. of
metastasis/recurrence |
|
|
| 0.006 |
| 1 | 17 (14.2) | 3 (42.9) | 14 (12.4) |
|
| 2 | 36 (30.0) | 4 (57.1) | 32 (28.3) |
|
| ≥3 | 67 (55.8) | 0 (0.0) | 67 (59.3) |
|
| NLR at diagnosis of
metastasis/recurrence |
|
|
|
<0.001 |
| Median
± SD | 2.84±2.31 | 1.29±0.10 | 2.92±2.34 |
|
|
Range | 0.83–17.50 | 1.21–1.40 | 0.83–17.50 |
|
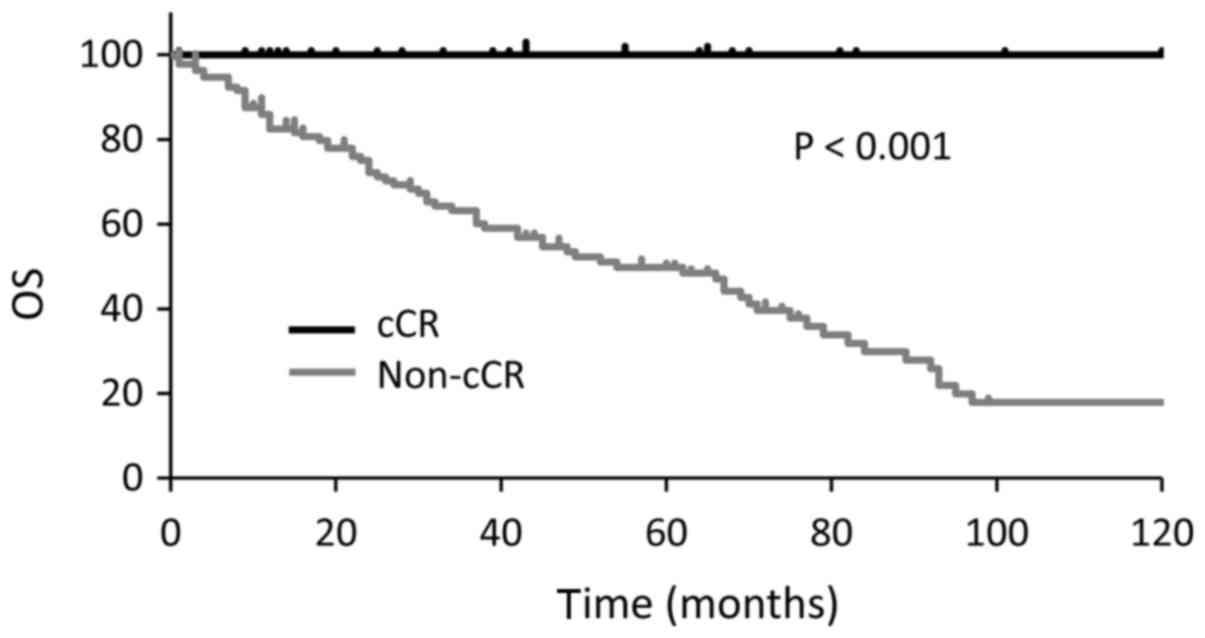
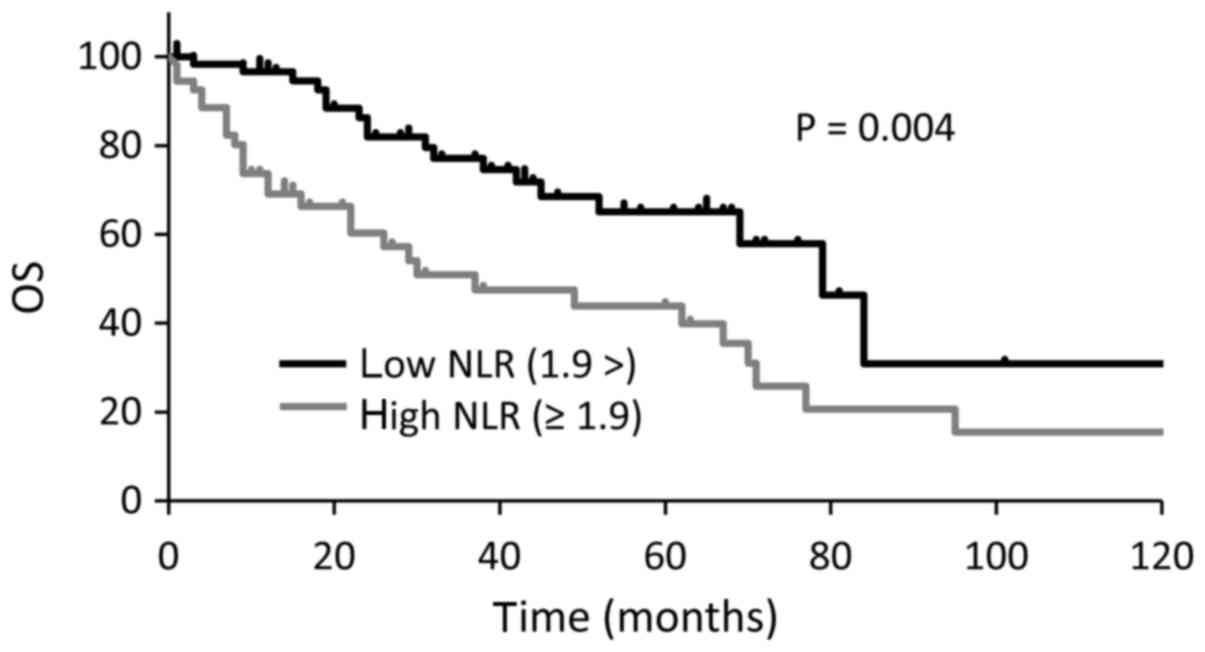
Median OS were longer in cCR group than non-cCR
group (P<0.001; Fig. 1). OS was
also longer in patients with a low NLR (<1.9) than in those with
a high NLR (≥1.9) at the time of MBC diagnosis (33 vs. 79 months,
P=0.004; Fig. 2). In the multivariate
analysis, a high NLR was associated with worse OS (P=0.0218; hazard
ratio, 1.75; 95% confidence interval, 1.09–2.85; Table III). Three patients with a high NLR
achieved a cCR, none of three had visceral metastases, and all of
them received multidisciplinary therapy consisting of systemic
therapy and local resection.
| Table III.Multivariate analysis of factors
associated with overall survival. |
Table III.
Multivariate analysis of factors
associated with overall survival.
| Variable | HR | 95% CI | P-value |
|---|
| Non-cCR | 2.27 | 0.87–5.94 | 0.0955 |
| Primary stage
IV | 1.14 | 0.64–2.03 | 0.6495 |
| Metastatic sites
no. ≥3 | 1.79 | 0.95–3.36 | 0.0714 |
| Visceral sites no.
≥2 | 1.07 | 0.62–1.86 | 0.7968 |
| NLR≥1.90 | 1.75 | 1.09–2.85 | 0.0218 |
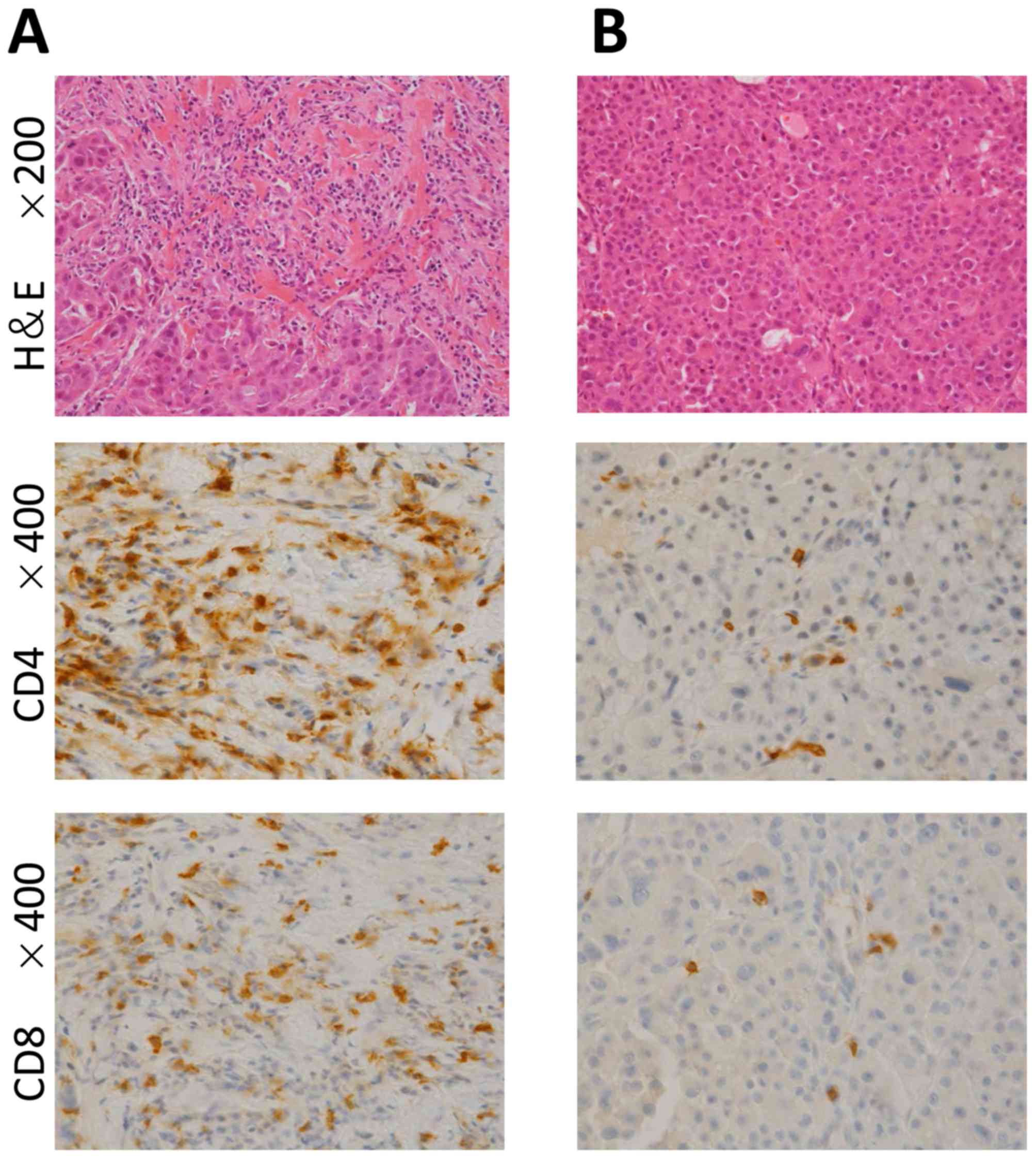
Core needle biopsy samples were obtained from 26
stage IV MBC patients before treatment (Table IV). Two patients had synchronous
bilateral breast cancers. Lymphocyte infiltration was scored as
high [≥50%; (Fig. 3A), intermediate
(≥10%, 50%>), and low (<10%; (Fig.
3B)]. Focusing on 4 patients with triple-negative disease, all
of them belonged to low TILs and resulted in non-cCR.
| Table IV.Clinicopathological implications of
TILs for patients with primary stage IV disease. |
Table IV.
Clinicopathological implications of
TILs for patients with primary stage IV disease.
| No. | Age | ER/HER2 | Ki-67 (%) | Metastatic
site | TILs | Outcome | f/u (months) | Other
information |
|---|
| 1 | 66 | +/− | 20 | Bone, lung, LN | Low | PD | 16 |
|
| 2 | 67 | +/− (rt.) | 2 | Lung | Low | SD | 19 | Bilateral |
|
|
| +/− (lt.) | 2 | Lung | Low | SD | 19 |
|
| 3 | 65 | +/− | 20 | Lung | Low | SD | 50 |
|
| 4 | 85 | +/− | 50 | Lung | Low | PR | 11 |
|
| 5 | 59 | +/− | 7.5 | Bone, lung, LN | Intermediate | SD | 15 |
|
| 6 | 68 | +/− | 20 | Bone | Low | cCR | 29 |
|
| 7 | 59 | +/− | 5 | Bone, liver,
LN | Low | Deceased | 10 | ILC |
| 8 | 89 | +/− | 10 | Bone, lung | Low | Deceased | 10 | ILC |
| 9 | 80 | +/− | 10 | Bone | Low | PD | 57 |
|
| 10 | 56 | +/− | 4 | Contralateral
breast, bone, pleura, LN, peritoneum | Intermediate | Deceased | 7 | ILC |
| 11 | 58 | +/− | / | Bone, pleura,
lung | Low | Deceased | 43 | IMPC |
| 12 | 61 | +/− | 40 | Bone, liver | Low | Deceased | 4 |
|
| 13 | 61 | +/− | 1.5 | Lung | Low | cCR | 69 |
|
| 14 | 66 | +/− | / | Bone, lung, liver,
LN | Low | Deceased | 66 |
|
| 15 | 54 | +/− | / | Bone, pleura,
pericardiac membrane | Intermediate | Deceased | 62 |
|
| 16 | 44 | +/− (rt.) | 2 | Bone | Intermediate | PD | 14 | Bilateral |
|
| 44 | +/+ (lt.) | 3 | Bone | Intermediate | PD | 14 |
|
| 17 | 64 | +/+ | 10 | Bone, liver | Low | PR | 3 |
|
| 18 | 36 | +/+ | 30 | Bone, lung | Low | PR | 19 |
|
| 19 | 62 | −/+ | 50 | Lung, liver | Intermediate | SD | 48 |
|
| 20 | 56 | −/+ | 90 | Contralateral
LN | Low | cCR | 14 | Fig. 3B |
| 21 | 32 | −/+ | 50 | Lung, LN | High | cCR | 38 | Fig. 3A |
| 22 | 57 | −/+ | 40 | Bone, pleura, LN,
contralateral breast, local | Intermediate | PD | 37 |
|
| 23 | 75 | −/− | 5 | Bone, lung, liver,
muscle | Low | Deceased | 4 |
|
| 24 | 87 | −/− | 7.5 | Bone | Low | SD | 2 |
|
| 25 | 60 | −/− | / | Pleura, local | Low | Deceased | 67 |
|
| 26 | 85 | −/− | / | Lung, peritoneum,
LN | Low | SD | 1 |
|
Discussion
MBC accounts for most breast cancer-associated
deaths. However, some patients with MBC achieve a cCR and survive
for a long time after multidisciplinary treatment. Owing to new
agents and therapies, the prognosis for MBC has been improving
(1).
In the present study, patients who achieved a cCR
survived for a longer period of time than those who did not
(Fig. 1). Compared with patients in
the non-cCR group, those in the cCR group were diagnosed with
primary breast cancer at an earlier stage and had fewer number of
recurrent or metastatic sites, and a lower NLR (Table I). Over half of the patients in cCR
group acquired NED status after local resection of lymph node
metastases or oligometastases. Thus, volume reduction is an
instrumental in achieving a cCR, irrespective of phenotype or Ki-67
status. Most important strategy is appropriate primary disease
control. Table II shows that the cCR
group tended to have a small number of metastatic sites and a low
NLR, even if visceral metastases were present. Seven patients who
had a cCR had visceral metastases, 5 of 7 received systemic therapy
without surgery. Although the number of patients with visceral
metastases who achieved a cCR is small, these patients are expected
to increase along with new drugs development. Since trastuzumab was
developed in the 1990's, improvement of anti-HER2 therapy has been
remarkable. An increase of the patients who achieve a cCR,
especially HER2+ patients, is expected in the
future.
Our study verified the prognostic value of NLR in
MBC, as reported by others (12–16).
Additionally, patients with a high NLR achieved a cCR by
multidisciplinary therapy combined with, local resection and
systemic therapy. Neutrophils play an important role in the
metastatic microenvironment (17–19). It is
generally believed that neutrophils dynamically regulate cancer
progression and metastasis. Resection of metastatic sites where the
immune system does not target cancer cells is a reasonable
strategy.
To assess the relationship between the tumor
microenvironment and therapeutic effects, we focused on TILs
because a high serous NLR might reflect local lymphocyte invasion.
We examined lymphocyte infiltration in patients with stage IV
disease (Table IV); because they
were treatment-naïve, and their TIL scores were
treatment-unrelated. Twenty-eight specimens from 26 patients were
available for review. Assessment of the 4 patients (3 low TILs; 1
high TILs) who achieved a cCR [estrogen receptor
(ER)+/HER2−, 2 patients;
ER−/HER2+, 2 patients] showed that the TIL
score had no prognostic value in MBC. According to previous
reports, the TIL score is a prognostic marker in HER2+
breast cancers (20), as well as
triple-negative breast cancers (TNBC) in the both neoadjuvant and
adjuvant settings (11,21,22).
Because all TNBC patients in this study showed low TILs, the
relationship between prognosis of TNBC patients and high TILs could
not be evaluated.
We did not evaluate the biopsy samples from all
metastatic sites. This would be of interest because metastatic
cancer cells have different characteristics from primary cancer
cells (23). Additionally, TILs
review was performed in core needle biopsy samples histologically.
Strictly, core needle biopsy was not standard approarch for TILs
evaluation (10).
In our study, 43 of the 137 patients with primary
stage I–III breast cancer experienced recurrence during adjuvant
therapy; the phenotypes of tumors were
ER+/HER2− (29 patients),
ER+/HER2+ (9 patients),
ER−/HER2+ (1 patient), and
ER−/HER2− (4 patients). In these patients,
recurrence is thought to be mainly from tumor-related factors
(e.g., resistance to systemic therapy) rather than host-related
factors. Because recent whole-exosome and transcriptome analysis
revealed that one of the most important mechanism in acquired drug
resistance in breast cancer therapy is mutation in cancer cells,
not in host normal cells (24,25).
Host-related factors such as individual adherence to therapy,
ability of drug metabolism, activity of drug degrading enzyme are
also important. However, appropriate adjuvant systemic therapy is
especially needed regarding the high mutation activity of tumor
related to drug-resistance.
In conclusion our study showed cCR and low NLRs
associate with extended survival times in patients with MBC.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HT, WT and FY designed the study. MS and YY
contributed to the evaluation of TIL scoring and the
immunohistochemistry analysis of CD4 and CD8. HT performed survival
analysis and multivariate analysis of the other data.
Ethics approval and consent to
participate
The present study was approved by the Ethics Review
board of the Shiga Medical Center for Adults.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
cCR
|
clinical complete response
|
|
ER
|
estrogen receptor
|
|
HER2
|
human epithelial growth factor
receptor 2
|
|
MBC
|
metastatic breast or recurrent breast
cancer
|
|
NLR
|
neutrophil-lymphocyte ratio
|
|
OS
|
overall survival
|
|
TIL
|
tumor-infiltrating lymphocyte
|
References
|
1
|
Tsuji W, Teramukai S, Ueno M, Toi M and
Inamoto T: Prognostic factors for survival after first recurrence
in breast cancer: A retrospective analysis of 252 recurrent cases
at a single institution. Breast Cancer. 21:86–95. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Giordano SH, Buzdar AU, Smith TL, Kau SW,
Yang Y and Hortobagyi GN: Is breast cancer survival improving?
Cancer. 100:44–52. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gennari A, Conte P, Rosso R, Orlandini C
and Bruzzi P: Survival of metastatic breast carcinoma patients over
a 20-year period: A retrospective analysis based on individual
patient data from six consecutive studies. Cancer. 104:1742–1750.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Greenberg PA, Hortobagyi GN, Smith TL,
Ziegler LD, Frye DK and Buzdar AU: Long-term follow-up of patients
with complete remission following combination chemotherapy for
metastatic breast cancer. J Clin Oncol. 14:2197–2205. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Falkson G, Gelman RS, Leone L and Falkson
CI: Survival of premenopausal women with metastatic breast cancer.
Long-term follow-up of eastern cooperative group and cancer and
leukemia group B studies. Cancer. 66:1621–1629. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rahman ZU, Frye DK, Smith TL, Asmar L,
Theriault RL, Buzdar AU and Hortobagyi GN: Results and long term
follow-up for 1581 patients with metastatic breast carcinoma
treated with standard dose doxorubicin-containing chemotherapy: A
reference. Cancer. 85:104–111. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Burstein HJ, Keshaviah A, Baron AD, Hart
RD, Lambert-Falls R, Marcom PK, Gelman R and Winer EP: Trastuzumab
plusvinorelbine or taxane chemotherapy for HER2-overexpressing
metastatic breast cancer: The trastuzumab and vinorelbine or taxane
study. Cancer. 110:965–972. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Baselga J, Cortés J, Kim SB, Im SA, Hegg
R, Im YH, Roman L, Pedrini JL, Pienkowski T, Knott A, et al:
Pertuzumab plus trastumab plus docetaxel for metastatic breast
cancer. N Engl J Med. 366:109–119. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Verma S, Miles D, Gianni L, Krop IE,
Welslau M, Baselga M, Pegram M, Oh DY, Diéras V, Guardino E, et al:
Trastuzumab emtansine for HER2-positive advanced breast cancer. N
Engl J Med. 367:1783–1791. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Salgado R, Denkert C, Demaria S, Sirtaine
N, Klauschen F, Prineri G, Wienert S, Van den Eynden G, Baehner FL,
Penault-Llorca F, et al: The evaluation of tumor-infiltrating
lymphocytes (TILs) in breast cancer: Recommendations by an
International tils working group 2014. Ann Oncol. 26:259–271. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hida AI and Ohi Y: Evaluation of
tumor-infiltrating lymphocytes in breast cancer; proposal of a
simpler method. Ann Oncol. 26:23512015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jia W, Wu J, Jia H, Yang Y, Zhang X, Chen
K and Su F: The peripheral blood neutrophl-to-lymphocyte ratio is
superior to the lymphocyte-to-monocyte ratio for predicting the
long-term survival of triple-negative breast cancer patients. PLoS
One. 10:e01430612015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Orditura M, Galizia G, Diana A, Saccone C,
Cobellis L, Ventriglia J, Iovino F, Romano C, Morgillo F, Mosca L,
et al: Neutrophil to lymphocyte ratio (NLR) for prediction of
distant metastasis-free survival (DMFS) in early breast cancer: A
propensity score-matched analysis. ESMO Open. 1:e0000382016.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Iwase T, Sangai T, Sakakibra M, Sakakibra
J, Ishigami E, Hayama S, Nakagawa A, Masuda T, Tabe S and Nagashima
T: An increased neutrophil-to-lymphocyte ratio predicts poorer
survival following recurrence for patients with breast cancer. Mol
Clin Oncol. 6:266–270. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ethier JL, Desautels D, Templeton A, Shah
PS and Amir E: Prognostic role of neutrophil-to-lymphocyte ratio in
breast cancer. A systematic review and meta-analysis. Breast Cancer
Res. 19:22017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Guthrie GJ, Charles KA, Roxburgh CS,
Horgan PG, McMillan DC and Clarke SJ: The systemic
inflammation-based neutrophil-lymphocyte ratio: Experience in
patients with cancer. Crit Rev Oncol Hematol. 88:218–230. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Acharyya S and Massague J: Arresting
supporters: Targeting neutrophils in metastasis. Cell Res.
26:273–274. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bird L: Tumour immunology: Neutrophils
help tumours spread. Nat Rev Immunol. 16:74–75. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wculek SK and Malanchi I: Neutrophils
support lung colonization of metastasis-initiating breast cancer
cells. Nature. 528:413–417. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Dieci MV, Mathieu MC, Guarneri V, Conte P,
Delaloge S, Andre F and Goubar A: Prognostic and predictive value
of tumor-infiltrating lymphocytes in two phase III randomized
adjuvant breast cancer trials. Ann Oncol. 26:1698–1704. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Castaneda CA, Mittendorf E, Casavilca S,
Wu Y, Castillo M, Arboleda P, Nunez T, Guerra H, Barrionuevo C,
Dolores-Cerna K, et al: Tumor infiltrating lymphocytes in triple
negative breast cancer receiving neoadjuvant chemotherapy. World J
Clin Oncol. 7:387–394. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hida AI, Sagara Y, Yotsumoto D, Kaemitsu
S, Kawano J, Baba S, Rai Y, Oshiro Y, Aogi K, Sagara Y and Ohi Y:
Prognostic and predictive impacts of tumor-infiltrating lymphocytes
differ between Triple-negative and HER2-positive breast cancers
treated with standard systemic therapies. Breast Cancer Res Treat.
158:1–9. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lambert AW, Pattabiraman DR and Weinberg
RA: Emerging biological principles of metastasis. Cell.
168:670–691. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Robinson DR, Wu YM, Vats P, Su F, Lonigro
RJ, Cao X, Kalyana-Sundaram S, Wang R, Ning Y, Hodges L, et al:
Activating ESR1 mutations in hormone-resistant metastatic breast
cancer. Nat Genet. 45:1446–1451. 2013. View
Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zardavas D, Phillips WA and Loi S: PIK3CA
mutations in breast cancer: Reconciling findings from preclinical
and clinical data. Breast Cancer Res. 16:2012014. View Article : Google Scholar : PubMed/NCBI
|