Introduction
A model that explains the phenotypic and functional
heterogeneity of cancer cells within the same tumor is the cancer
stem cell (CSC) model. According to the CSC model, a tumor has a
hierarchical cellular structure, where a small population of
tumorigenic CSCs differentiates into non-stem cancer cells or
non-tumorigenic progeny (1). Cancer
stem cells are thought to possess stem-like properties of
self-renewal, and initiate and drive tumor growth and metastasis,
in addition to therapy resistance and recurrence following
conventional therapy (2). As genital
infection with human papillomaviruses (HPVs), in particular the
persistent infection of high-risk species (including HPV16 and 18),
promotes disease progression from cervical intraepithelial
neoplasia (CIN) to malignancy, the virus may interact with CSCs in
the epithelium of the uterine cervix (3,4).
In general, the cervix is composed of hard squamous
cells in the ectocervix, soft columnar cells in the endocervix and
metaplastic cells in the squamocolumnar junction, also known as the
transformation zone (5). Squamous and
columnar epithelial cells are regenerated by the active division of
stem-like reserve cells in the transformation zone, where cervical
cancer is hypothesized to originate (6,7). It has
been suggested that HPV enters the cell by distinct pathways,
including clathrin- or caveolar-mediated endocytosis, or
alternative routes in which tetraspanin-enriched microdomains are
involved (8). The dependence of HPV
infection on the activity of cyclin dependent kinases and
microtubule reorganization, suggests that the incorporation of the
viral genome into the nucleus of reserve cells may require the cell
to enter into mitosis (9). HPV may
program the cell to undergo symmetric division, by the disturbance
of asymmetric division, therefore allowing the cells to proliferate
and produce viral particles, but preventing them from
differentiation (10,11). Accordingly, reserve cells may be
converted to cervical CSCs by the interplay with high risk-HPV
viral oncogenes and cellular alterations during cervical
carcinogenesis (11). In fact, the
presence of CSCs in cervical carcinoma is detectable by using stem
cell markers. Early studies suggested that transcription factor
tumor protein p63 (p63) and cytokeratin 17 (KRT17) are markers for
reserve cells and reserve cell hyperplasia in the epithelium of
cervical lesions and are upregulated during HPV infection of
epithelial cells (10,12,13). Nanog
homeobox (NANOG), POU class 5 homeobox 1 (OCT4) and SRY-box 2
(SOX2) are key regulators of embryonic stem cells and incorporate
primarily into the regulatory network responsible for self-renewal
and pluripotency (14,15). NANOG is expressed in cervical lesions
but may not associate with the prognosis of cervical carcinoma
(16). Different isoforms of OCT4 are
expressed in cultured cells of cervical carcinoma, with the highest
level in HPV-positive cells (17,18).
Aldehyde dehydrogenase (ALDH), a stem cell marker for early
stem-cell differentiation, is detectable in cervical epithelial
lesions and carcinoma in addition to stem-like cells that are
isolated from cervical carcinoma cells (19–21).
Transcription factor twist family BHLH transcription factor 1
(Twist1) may serve a function in the disruption of
E-cadherin-mediated cell-cell adhesion and the induction of
epithelial-mesenchymal transition in cervical cancer stem-like
cells (20–23). These previous studies suggest that
cervical carcinoma or cell lines harbor a small population of CSCs
that are characterized by the expression of stem cell markers;
however, to date, the expression pattern of stem cell markers in
cervical carcinoma and precursor lesions have yet to be
well-characterized.
In the present study, the transcription and protein
expression of ALDH family member A1 (ALDH1A1), NANOG, OCT4, SOX2
and Twist1 in cervical lesions and blood plasma from patients with
squamous cell carcinoma (SCC) and its precursor lesion, CIN, were
detected using reverse transcription-quantitative polymerase chain
reaction (RT-qPCR), immunohistochemistry (IHC) and ELISA. The
results of the present study may contribute to current knowledge on
the association of cervical carcinogenesis with the regulation of
stem cell marker expression, and provide potential biomarkers for
the early prognosis, diagnosis and monitoring of cancer
treatment.
Materials and methods
Tissue specimens
The present study was approved and monitored by the
Ethics Committee of Xinjiang Medical University (Xinjiang, China).
All procedures performed in the present study were in accordance
with the Helsinki Declaration of 1975, as revised in 2000. Written
informed consent was obtained from all patients and healthy
individuals prior to the study, and all data were analyzed
anonymously. Patients diagnosed with cervical SCC, CIN and subjects
(negative control, NC) with a normal cervix were enrolled in the
present study, according to the diagnostic criteria of the World
Health Organization and the Chinese Medical Association as
described elsewhere (24). A total of
94 fresh tissue samples were sourced from patients and healthy
controls by routine biopsies and surgical operations at the
Department of Gynecology at the First Affiliated Hospital and The
Third Affiliated Cancer Hospital of Xinjiang Medical University
from March 2013 to June 2014. The specimens were pathologically
classified, and included 32 cases of cervical SCC, 30 cases of CIN
stages II–III and 32 cases of normal controls. CIN II and III are
classified as a high-grade squamous intraepithelial lesion, which
is considered a significant precancerous lesion, whereas CIN I, as
a low-grade squamous intraepithelial lesion, is considered a much
more benign lesion since most of these lesions regress; those
diagnosed at this stage (CIN I) were excluded from the present
study (24). Fresh tissue specimens
were frozen quickly in liquid nitrogen following resection and
stored at −80°C for six months or in liquid nitrogen storage for up
to two years.
For immunohistochemical (IHC) analysis, 116 cases of
paraffin-embedded cervical specimens (3-µm thickness) were obtained
from the specimen bank in the Pathology Department of the First
Affiliated Hospital of Xinjiang Medical University. These specimens
were selected following a case review by two experienced
pathologists, and these included 47 cases of SCC, 37 cases of CIN
stages II–III and 32 cases of NC.
For ELISA analysis, plasma samples from 85 Uighur
women were collected, including 40 cases of SCC, 28 cases of CIN
II–III and 17 cases of NC. A total of 3 ml blood samples were
obtained from each donor by venipuncture into evacuated blood
collection tubes that contained EDTA as an anticoagulant, and the
plasma was preserved at −80°C for further use following
centrifugation at 800 × g and 4°C for 10 min. The median age of
patients was 53 years (range 25–65 years), and normal controls were
age-matched to patients.
The clinical staging of patients was based on
guidelines established by the International Federation of
Gynecology and Obstetrics of 1994–1997, as revised in 1999 by
Pecorelli et al (25). Tumor
specimens were collected from patients with cancer who underwent
radical surgery for cervical SCC at clinical stages I–IIa.
Precancerous lesions were collected from patients with CIN stages
II–III as biopsies or from cervical conization. Normal controls
were obtained from patients without a history of cervical lesions
or any form of cancer who underwent a hysterectomy for nonmalignant
reasons during the same time period. Indications for hysterectomy
were fibroids, prolapsed uterus or adenomyosis, and primarily a
combination of fibroids with prolapse.
DNA extraction and HPV detection
Genomic DNA was extracted from fresh cervical
specimens using a QIAamp DNA Mini kit for tissue DNA (cat no.
51306; Qiagen, Inc., Valencia, CA, USA). Concentration and purity
of extracted DNA were measured using a spectrophotometer (NanoDrop
2000; Thermo Fisher Scientific, Inc., Waltham, MA, USA). HPV
infection of 8 high-risk HPV genotypes, including HPV 16, 18, 45,
31, 33, 52, 58 and 67, was determined by multi-fluorescent PCR
assay using the Real Quality RQ-HPV HR kit (cat no. RQ-22-120A; AB
Analitica SRL, Padua, Italy) containing specific primers for HPV16,
HPV18/45 and HPV31, and general primers for HPV33/45/52/58/67.
Following the activation of the polymerase at 95°C for 1 min, 40
cycles of the denaturation at 95°C for 15 sec, annealing at 57°C
for 30 sec and elongation at 72°C for 30 sec, were performed on the
ABI-7500 PCR System (Applied Biosystems; Thermo Fisher Scientific,
Inc.). The human β-actin gene was used as an internal control for
DNA quality.
RNA extraction and RT-qPCR
analysis
Fresh frozen tissues (~50 mg) were packed in
aluminum foil and pulverized by grinding under liquid nitrogen.
Total RNA was isolated from the powder by dissolving with
TRIzol® lysis buffer (Invitrogen; Thermo Fisher
Scientific, Inc., Waltham, MA, USA) followed by phenol/chloroform
extraction and ethanol precipitation. cDNA was synthesized from 1
µg of total mRNA by RT using a RevertAid kit (Fermentas; Thermo
Fisher Scientific, Inc.) at 42°C for 60 min. For RT-qPCR analysis,
primer pairs specific to the mRNA sequences of target genes and
suitable for use were designed and synthesized by Takara Bio
(Takara Biotechnology Co., Ltd., Dalian, China; Table I). Each cDNA sample (20 ng) was
analyzed in a 25 µl by RT-qPCR using SYBR Premix Ex Taq™
kit (TIi RNase H Plus; Takara Biotechnology Co., Ltd.) on an iQ5™
PCR system (Bio-Rad Laboratories, Inc., Hercules, CA, USA) and. The
thermocycling conditions were as follows: Initial denaturation at
95°C for 30 sec, followed by 40 cycles of denaturation at 95°C for
5 sec and synthesis at 60°C for 30 sec and a final incubation at
4°C for 10 min. Expression levels of target genes were quantified
using the 2−ΔΔCq method (26) using the software iQ5 Standard Edition
(Version 1.028; Bio-Rad Laboratories, Inc.), setting β-actin as an
internal control. Experiments were repeated in triplicate for each
sample.
 | Table I.List of primers used in reverse
transcription-quantitative polymerase chain reaction analysis. |
Table I.
List of primers used in reverse
transcription-quantitative polymerase chain reaction analysis.
| Gene | Accession
number | Forward primer
(5′-3′) | Reverse primer
(5′-3′) | Product (bp) |
|---|
| ALDH1A1 | NM_000689 |
TTGTCCAGCCCACAGTGTTCTC |
TGTCTTTGGTAAACACTCCTGCTGA | 168 |
| OCT4 | NM_002701.4 |
GTGCCGTGAAGCTGGAGAA |
TGGTCGTTTGGCTGAATACCTT | 192 |
| NANOG | NM_024865 |
CCTGTGATTTGTGGGCCTGA |
CTCTGCAGAAGTGGGTTGTTTG | 168 |
| SOX2 | NM_003106 |
GTGAGCGCCCTGCAGTACAA |
GCGAGTAGGACATGCTGTAGGTG | 82 |
| TWIST1 | NM_000474 |
CAGCTACGCCTTCTCGGTCT |
CTGTCCATTTTCTCCTTCTCTGG | 138 |
| β-actin | NM_001101.3 |
CATCCGTAAAGACCTCTATGCCAAC |
ATGGAGCCACCGATCCACA | 171 |
IHC analysis
The paraffin-embedded tissues were sectioned into
3-µm slices. The IHC staining was performed with the streptavidin
peroxidase-conjugated method using primary rabbit polyclonal
antibodies recognizing target proteins ALDH1 (cat. no. ab23375;
Abcam, Cambridge, UK) and OCT3/4 (cat. no. PA5-27438; Thermo Fisher
Scientific Inc.) at 1:200 dilutions, and IHC kits containing
biotin-labeled goat anti-rabbit secondary antibody (cat. no.
ZB-2010; Beijing Zhongshan Golden Bridge Biotechnology Co. Ltd.;
OriGene Technologies, Beijing, China) at the 1:300 dilution
according to titration experiments and the manufacturer's protocol.
Briefly, tissue sections were dewaxed in 100% xylene and rehydrated
in ethanol at 100, 85 and 75% gradients and each for 5 min at room
temperature, and washed with distilled water at room temperature
followed by antigen retrieval with heating in the microwave oven
for 15 min at 95°C in EDTA buffer (pH 8.0). Subsequent to cooling
and rinsing in distilled water, endogenous peroxidase activity was
blocked by incubating sections for 15 min in 3%
H2O2 at room temperature followed by rinsing
in 0.01 M PBS (pH 7.4) for 10 min. Following treatment at room
temperature with the protein blocking solution provided by the IHC
kits for 10 min, the sections were incubated with the primary
antibodies in a humid chamber overnight at 4°C. Then, the sections
were washed with PBS three times and incubated with the secondary
antibody for 15 min at room temperature. The staining was
visualized with the DAB Kit (Beijing Zhongshan Golden Bridge
Biotechnology Co. Ltd.; OriGene Technologies). Negative controls
were treated with PBS instead of primary antibodies. All tissue
sections were counterstained using 100% hematoxylin at room
temperature for up to 30 sec, in accordance with the preliminary
experiments. PBS was used in place of the primary antibody as a
negative control. For evaluation, stained tissue sections were
scored under a light microscope (magnifications, ×20 and ×40) by
two experienced pathologists. The results were scored on a scale of
0 to 3 by an estimation of the percentage and intensity of positive
staining in 5 fields each time using a previously described method
for evaluation and interpretation of IHC staining (27). A mean percentage of positive staining
was calculated according to the number of positively stained cells
in each field and time and scored as 0 for negativity, 1 for 0 to
30% positivity, 2 for >30 to 60% positivity and 3 for >60%
positivity. Positive staining intensity was scored as 0 for a
negative signal, 1 for weak signal intensity, 2 for moderate signal
intensity and 3 for high signal intensity. A consensus number
between the two investigators was reached for each tissue slice. An
overall score was calculated by the addition of the two scores and
the overall scores were classified according to the following
categories: i) 0–2, a loss of expression or weak expression; ii)
3–4, moderate expression and iii) 5–6, strong expression.
ELISA
Plasma levels of ALDH1 and OCT4 were determined in
blood samples from patients and controls by 96-well plate sandwich
ELISA using commercially available kits for ALDH1 (cat. no.
SEE824Hu) and OCT4 (cat. no. SEA424Hu; both Uscn Life Sciences,
Inc., Wuhan, China) according to the manufacturer's protocol. The
quantification of the relative plasma content was based on the
standard curves derived from standard substances (proteins) of
ALDH1 and OCT4 supplied with the indicated kits, in which the
absolute concentration of each protein was known.
Statistical analysis
Statistical analysis was performed using SPSS
(version 17.0; SPSS Inc., Chicago, IL, USA). All P-values were
two-sided, and P<0.05 was considered to indicate a statistically
significant difference. All data was presented as the mean ±
standard deviation. Data derived from the results of RT-qPCR and
ELISA tests were compared for statistical differences. Between and
within group analysis were carried out using one-way ANOVA followed
by Dunnett's post-hoc test. Continuous data derived from IHC
scoring was analyzed using Mann-Whitney U test.
Results
Transcription of stem cell markers in
cervical carcinoma and its precursor lesions
The present study focused on five stem cell markers,
including ALDH1A1, OCT4, NANOG, SOX2 and Twist1, which are
considered to be potential biomarkers for cervical carcinoma as
previously reported (16–23). The transcription of genes encoding
these proteins was analyzed in tissue specimens from patients with
SCC, CIN II–III and NC using RT-qPCR using primer pairs specific
for mRNA sequences. The data indicated an increase in the
transcription of these genes with the progression of cervical
cancer (Fig. 1, Table II). Statistical analysis confirmed
significant differences in the expression of all five genes in SCC
tissues compared with NC tissues (P<0.05). In addition,
significant differences were detected in the expression of ALDH1A1,
OCT4 and NANOG in CIN II–III tissues compared with NC tissues
(P<0.05). There were also significant differences detected in
ALDH1A1 and OCT4 expression in SCC tissues compared with CIN II–III
tissues (P<0.05). These findings indicate that cervical
carcinogenesis may be characterized by the upregulation of stem
cell markers, in particular the differential expression of ALDH1A1
and OCT4 in SCC tissues compared with its precursor lesions and
normal cervical tissue.
 | Figure 1.mRNA expression patterns of five
genes, including ALDH1A1, NANOG, OCT4, SOX2 and Twist1 in SCC, CIN
II–III and NC tissues analyzed by reverse
transcription-quantitative polymerase chain reaction. *P<0.05
vs. NC; #P<0.05 vs. CIN. ALDH1A1, aldehyde
dehydrogenase 1 family member A1; NANOG, nanog homeobox; OCT4, POU
class 5 homeobox 1; SOX2, SRY-box 2; Twist1, twist family BHLH
transcription factor 1; SCC, cervical squamous cell carcinoma; CIN,
cervical intraepithelial neoplasia; NC, negative controls. |
| Table II.mRNA expression levels of five stem
cell markers in cervical lesions as determined by reverse
transcription-quantitative polymerase chain reaction. |
Table II.
mRNA expression levels of five stem
cell markers in cervical lesions as determined by reverse
transcription-quantitative polymerase chain reaction.
|
| Relative mRNA
expression level (mean ± standard deviation) | One-way analysis of
variance (P-value) |
|---|
|
|
|
|
|---|
| Markers | NC (n=32) | CIN II–III
(n=30) | SCC (n=32) | F-value | P-value | SCC vs. NC | CIN vs. NC | SCC vs. CIN |
|---|
| ALDH1A1 | 0.458±0.047 | 1.076±0.055 | 1.733±0.068 | 10.943 | <0.0001 | <0.0001 | 0.031 | 0.022 |
| NANOG | 0.267±0.090 | 1.676±0.036 | 2.318±0.058 | 6.825 | 0.003 | 0.001 | 0.019 | 0.272 |
| OCT4 | 0.034±0.006 | 1.555±0.031 | 3.482±0.216 | 19.723 | <0.0001 | <0.0001 | 0.009 | 0.001 |
| SOX2 | 0.521±0.176 | 1.461±0.022 | 1.949±0.156 | 4.281 | 0.020 | 0.006 | 0.069 | 0.338 |
| TWIST1 | 0.476±0.130 | 0.615±0.072 | 1.114±0.142 | 3.384 | 0.043 | 0.017 | 0.613 | 0.061 |
Among the 94 cases of fresh tissue specimens, HPV
infection was detected in 64 cases with qPCR using probes for
HPV16, 31, 18/45, and 33/52/58/67 (Table III). Of these 64 cases, 32 cases of
SCC, 24 cases of CIN II–III and 8 cases of normal controls (NC)
were positive for HPV16 infection, including several cases
co-infected by HPV16 and other HPV species. Due to high HPV
positivity, in particular the predominance of HPV16 infection in
SCC (32/32) and CIN II–III (24/30) and the HPV negativity of NC
(24/32), the data of HPV detection was not suitable for analyses
for the association of gene expression with HPV16 infection.
Nevertheless, due to the contrast between HPV16 positive cervical
lesions and HPV-negative normal controls, it is hypothesized that a
regulation of stem cell markers independent of HPV16 infection was
integrated into the result of RT-qPCR (Table II).
| Table III.HPV genotyping of cervical
specimens. |
Table III.
HPV genotyping of cervical
specimens.
| Samples | HPV16 | HPV16/18/45 | HPV16/31 |
HPV16/33/52/58/67 |
|---|
| NC (n=32) | 6 | 2 | n.d. | n.d. |
| CIN II–III
(n=30) | 20 | 4 | n.d. | n.d. |
| SCC (n=32) | 20 | 3 | 3 | 6 |
Verification of ALDH1A1 and OCT4
expression by immunohistochemistry
To validate the results of the RT-qPCR analysis, the
protein expression of ALDH1A1 and OCT4 in 116 cases of
formalin-fixed and paraffin-embedded tissue specimens of SCC, CIN
II–III and NC were analyzed by immunohistochemical analysis.
Positive staining for ALDH1A1 and OCT4 was localized in the
cytoplasm of cervical epithelial or carcinoma cells (Fig. 2). Statistical analysis revealed that
the strong and moderate positive staining of ALDH1A1 was
significantly increased in CIN II–III and SCC compared with NC and
from CIN II–III to SCC (P<0.05; Table
IV). Although a weak staining of OCT4 was observed in a number
of the specimens from SCC, CIN II–III and NC, moderate staining of
OCT4 was significantly increased in SCC compared with CIN II–III
and NC (P<0.05). These results indicated that the transcription
and protein expression of ALDH1A1 and OCT4 is increased during the
development of cervical carcinoma and its precursor lesions
compared with normal tissues.
| Table IV.Immunohistochemical staining analyses
of ALDH1A1 and OCT4 expression in cervical lesions. |
Table IV.
Immunohistochemical staining analyses
of ALDH1A1 and OCT4 expression in cervical lesions.
| A, ALDH1A1 |
|---|
|
|---|
| Samples | − | + | ++ | +++ | P-value |
|---|
| NC (n=33) | 8 | 18 | 7 | 0 |
<0.0001a |
|
| CIN II–III
(n=37) | 11 | 4 | 19 | 3 | 0.028b |
|
| SCC (n=47) | 5 | 0 | 25 | 17 |
<0.0001b |
<0.0001c |
|
| B, OCT4 |
|
| Samples | − | + | ++ | +++ | P-value |
|
| NC (n=33) | 20 | 12 | 1 | 0 | 0.001a |
|
| CIN II–III
(n=37) | 19 | 13 | 5 | 0 | 0.138b |
|
| SCC (n=47) | 16 | 14 | 17 | 0 |
<0.0001b | 0.029c |
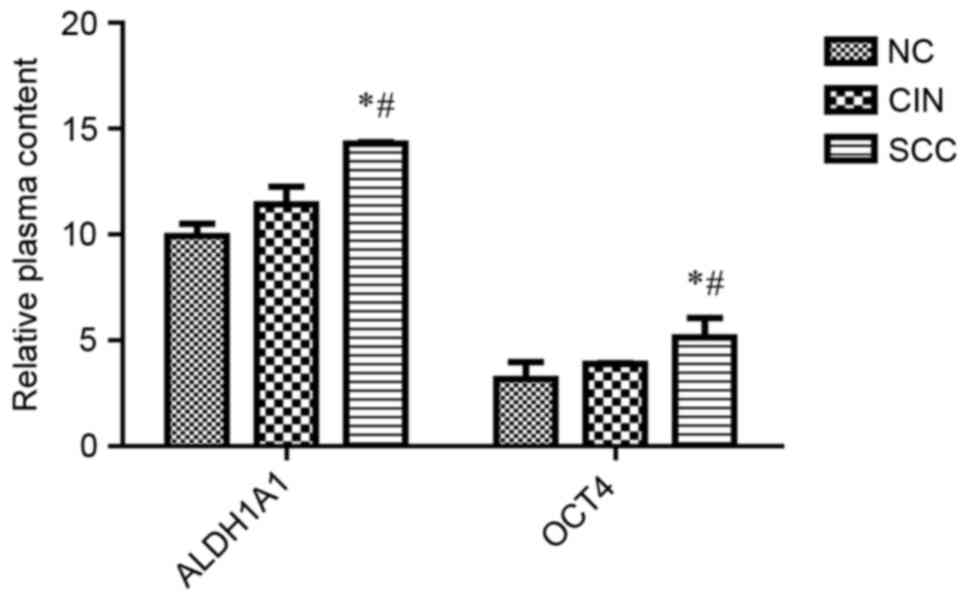
Upregulation of ALDH1A1 and OCT4 in
circulating blood plasma with the development of cervical
carcinoma
To evaluate the potential of ALDH1A1 and OCT4 as
biomarkers for non-invasive diagnosis, the levels of these proteins
in 85 cases of plasma samples from patients with SCC and CIN and
healthy subjects were detected (Table
V). The ELISA analysis indicated significantly higher levels of
ALDH1A1 and OCT4 in the plasma of patients with SCC compared with
patients with CIN II–III and healthy controls (P<0.05), but
there was no significant difference between patients with CIN
II–III and healthy controls (P>0.05; Fig. 3). Therefore, the quantitative increase
of these proteins in plasma may serve as biomarkers for cervical
carcinoma.
| Table V.Plasma levels of ALDH1A1 and OCT4 in
healthy controls and patients with cervical lesions as analyzed
using ELISA. |
Table V.
Plasma levels of ALDH1A1 and OCT4 in
healthy controls and patients with cervical lesions as analyzed
using ELISA.
|
| Plasma protein
level (ng/ml) | One-way analysis of
variance (P-value) |
|---|
|
|
|
|
|---|
| Markers | NC (n=17) | CIN II–III
(n=28) | SCC (n=40) | F-value | P-value | SCC vs. NC | CIN vs. NC | SCC vs. CIN
II–III |
|---|
| ALDH1A1 | 9.923±0.585 | 11.432±0.818 | 14.287±0.069 | 3.449 | 0.034 | 0.034 | 0.759 | 0.034 |
| OCT4 | 3.170±0.808 | 3.885±0.033 | 5.143±0.914 | 5.946 | 0.004 | 0.032 | 0.553 | 0.002 |
Discussion
The concept of cancer stem cells in human tumors
opens up novel research directions on how cancer is initiated and
how cancer cells are capable of switching from dormancy to
malignancy, and challenges previous understanding of tumor
recurrence, angiogenesis, metastasis and drug resistance (28–30).
Accordingly, the studies on stem cell markers have notably shifted
from focusing on the function of the markers in embryonic
development to their involvement in tumorigenesis (31–33). In
previous studies, cervical CSCs were most frequently identified and
characterized in cell lines of cervical carcinoma by detection of
stem cell markers, including p63, KRT17, ALDH1, OCT4, NANOG, SOX2
and Twist1 (12,16,17,21,22).
However, the expression profile of these stem cell markers in
cervical lesions has yet to be intensively studied (5). Furthermore, the application of stem cell
markers for clinical diagnosis is limited due to the lack of
sufficient validation studies. In the present study, it was
revealed that the transcription and protein expression of ALDH1A1
and OCT4 were significantly upregulated in cervical lesions from
patients with CIN II–III and SCC compared with normal controls, and
also significantly higher in the plasma of patients with SCC
compared with healthy controls. In the case of NANOG, SOX2 and
Twist1, the transcription of these genes in SCC tissues was
significantly higher compared with NC, but no significant
difference was identified in CIN II–III compared with SCC or
NC.
As ALDH1 and OCT 4 are considered as biomarkers for
embryonic and/or cancer stem cells (14,20), the
results of the present study indicate that the deregulation of
these two proteins in cervical lesions reflects the function of
CSCs or cancer cells with stem-like properties during cervical
carcinogenesis (14,21). However, the outcome of the association
analysis between the gene expression and HPV infection may be
limited due to the high HPV16 positivity of SCC and CIN specimens
in comparison with normal controls negative for HPV infection.
Nevertheless, as the expression levels of stem cell markers were
analyzed in SCC and CIN compared with the normal controls in the
present study, it was suggested that the expression of stem cell
markers potentially regulated by HPV16 infection may be reflected
in the RT-qPCR results, and presumably in IHC analyses of tissue
specimens that were not tested for HPV infection. Therefore,
independent analyses, in particularly in vitro studies,
associated with HPV16 infection are required to validate the
outcome of the present study.
The ALDH family has 19 different isoforms that are
localized in the cytoplasm, mitochondria or nucleus, and serve
crucial functions in cellular protection by the oxidation of
intracellular aldehydes, which induces resistance to a number of
alkylation agents used in cancer therapy (34). Among them, ALDH1A1, ALDH1A2, ALDH1A3
and ALDH8A1 participate in the oxidation of retinol to retinoic
acid in the cytoplasm, which in turn translocate into the nucleus
and initiates the transcription of genes involved in early
stem-cell differentiation (35,36). In
addition, ALDH1A1 may contribute to the majority of ALDH activity
in CSCs (37). The predominant
expression of ALDH1A1 has been associated with ALDH activity in
prostate and thyroid cancer (38,39). In
the case of 6 ALDH1 isoenzymes, ALDH1A1 may be a major contributor
of ALDH1 activity and a biomarker for predicting the poor survival
of patients with breast cancer (40).
High levels of ALDH1A1 and ALDH1A3 expression are associated with
malignant transformation to lung adenocarcinoma (41). Little is known about the regulation of
ALDH1A1 expression in cervical lesions, but the function of ALDH in
cervical CSCs or cervical carcinoma has been described in a number
of studies: CSCs that are isolated and enriched from cervical
carcinoma cell lines with high ALDH activity or ALDH1 positivity
exhibit enhanced stem-like properties of self-renewal, high
tumorigenicity and resistance to cisplatin treatment compared with
those with low ALDH activity or negative for ALDH1 expression
(20,21). ALDH-positivity and expression levels
are increased in tumor specimens of the uterine cervix, and
therefore ALDH may serve as a predictive marker for poor prognosis,
poor clinical outcome and resistance to chemotherapy in patients
with cervical carcinoma (42–44). Corresponding with these results, the
results of the present study also revealed that the upregulation of
ALDH1A1 in the progression of precancerous lesions (CIN II–III) to
cervical carcinoma. This indicates that ALDH1A1 may be a potential
biomarker for the early diagnosis of cervical carcinoma.
OCT4 is a well-established stem cell factor that
cooperates with SOX2 in maintaining the self-renewal and
pluripotency of human and mouse embryonic stem cells (45,46). The
loss of OCT4 expression or downregulation is associated with stem
cell differentiation (47). OCT4 is
detected in tumor-initiating cells or stem-like cancer cells
enriched from tumor tissues or cell lines, indicating its function
in tumorigenesis, metastasis and resistance to anticancer therapies
(48). The co-expression of OCT4 with
SOX2 has been detected in CIN but not in SCC, and the elevated
expression of OCT4 in the absence of SOX2 is associated with the
poor prognosis of patients with cervical carcinoma (49). However, the upregulation of both OCT4
and SOX2 in cervical carcinoma and its precursor lesions was
detected in the present study by RT-qPCR. Consistent with the
findings in the present study, a number of previous studies suggest
that SOX2 functions cooperatively with other dosage-sensitive
transcription factors, including OCT4 and NANOG, in order to
maintain the regulatory networks responsible for self-renewal and
to repress differentiation programs in embryonic stem cells
(50,51). These studies indicate that the
expression profile of OCT4 and SOX2 and NANOG may serve as
biomarkers for the prognosis of cervical carcinoma.
Genital infection by HPVs, in particular by
oncogenic high-risk HPV types (including HPV 16 and 18), is
generally known to be the primary etiological factor in cervical
carcinogenesis (52). However, the
effects of HPV detection in cervical specimens are constantly
debated in studies on cervical carcinoma, as the majority of HPV
infections are transient and harmless or eliminated by the host
immunity (4). Even persistent
infections have a relatively long latent period prior to the
induction of cancer, indicating that HPV testing alone is not
sufficient in the prognosis of cervical carcinoma (3). Therefore, HPV-based cancer prognoses may
require the use of auxiliary diagnostic biomarkers that are present
during HPV-induced carcinogenesis (53). However, based on the results of HPV
genotyping performed in the present study, it was difficult to
define the association between the expression of target genes and
HPV infection as the majority of cases of SCC and CIN II–III were
positive for HPV and most of the normal controls were HPV-negative.
Nevertheless, the potential effects of HPV infection on the
expression of stem cell markers have been described in previous
studies. In cervical cancer cells, HPV16 may activate OCT4
expression, which in turn induces the expression of miR-125b that
targets BCL2 antagonist/killer 1 and consequently leads to the
suppression of apoptosis (54,55).
Stem-like cancer cells isolated from primary cervical tumors or
cell lines express OCT4 together with NANOG and SOX2 and have
sphere-forming and self-renewal abilities, which are abolished by
the suppression of HPV-coding E6 protein (56). This suggests that independent analyses
are required in order to reveal the potential mechanism of the
regulation of stem cell markers by HPV infection.
In biomarker discovery, the sensitivity and
specificity as well as the convenience of diagnosis for physicians
should be taken into account. Due to its invasive and metastatic
potential, CSCs may be able to spread from primary tumors and
survive in the circulating blood by evading immune surveillance,
and subsequently form metastases (57). Accordingly, the determination of a
stem cell marker that is released from circulating CSCs may become
a fast and direct approach to plasma-based diagnosis of cancer.
A previous study reported that ALDH1 is elevated in
the blood of patients with non-small-cell lung cancer prior to
surgery but is not detectable in post-operative samples (58). The detection of serum ALDH1A1 has been
suggested to have a predictive value in monitoring the chemotherapy
of patients with primary and metastatic breast cancer (59). Additionally, high levels of serum OCT4
and NANOG are detectable in patients with hepatocellular carcinoma
and hepatitis B virus infection (60).
It is also important for the detection of stem cell
markers with a tumor origin to take into account the complexity of
stem cells, multipotent stem-like cells or progenitor cells in the
blood circulation. Notably, the blood contains highly heterogenic
populations of vascular-resident stem or progenitor cells with
proliferative capacity and clonogenicity, including mesenchymal
stem cells, pericytes, endothelial progenitor cells and smooth
muscle progenitor cells, which serve important functions in
vascular homeostasis (61). These
cells are either derived from the bone marrow and other sources or
frequently released from the vascular endothelium to the blood by
hemodynamic forces, including fluid shear stress and cyclic strain
or pathologic processes during heart and vascular diseases
(62,63). In addition, mesenchymal stem cells are
multipotent and are able to differentiate into vascular smooth
muscle cells and endothelial cells (64). High ALDH activity may be detected in
human bone marrow-derived mesenchymal stromal cells with
multipotent stromal and pro-vascular regenerative functions
(65). Consistent with these
findings, the results of the present study indicate that the
increased levels of ALDH1A1 in the blood may, to a high extent,
contribute to cervical carcinogenesis, and therefore ALDH1A1 may be
used as a marker to distinguish patients with cervical carcinoma
from normal controls.
To the best of our knowledge, the number of previous
studies on the detection of OCT4 in the blood of patients with
cancer is limited. In the present study, there were no significant
differences between the plasma levels of ALDH1 and OCT4 in patients
with CIN II–III and normal controls. However, the plasma levels of
ALDH1 and OCT4 significantly increased in patients with cervical
carcinoma compared with CIN II–III and controls. These results were
consistent with the findings from IHC, which revealed that in
specimens from normal subjects, the expression of ALDH1 and OCT4
proteins was negative, whereas the expression of these proteins was
moderate or strongly positive in cervical carcinoma. Additionally,
the differences in expression of ALDH1 and OCT4 proteins between
specimens from normal subjects and patients with cervical carcinoma
were statistically significant. Therefore, OCT4 may additionally
contribute to the diagnosis and prognosis of cervical carcinoma,
when its detection is combined with the detection of ALDH1 and
other biomarkers.
NANOG expression is detectable in embryonic stem
cells, embryonic limb bud cells and embryonal carcinoma cells
(66,67). The expression of NANOG is elevated at
advanced clinical stages of breast cancer, glioma and bladder
cancer, which may be associated with poor prognosis (68). The results of the present study
revealed that NANOG transcription was significantly increased in
tissues from patients with SCC or CIN compared with controls, but
the expression was not significantly different between specimens
from patients with SCC and CIN. In addition, a previous study also
indicated that the high expression of NANOG in cervical lesions may
not be associated with the prognosis of cervical carcinoma
(16). Accordingly, NANOG expression
was not additionally analyzed by IHC and plasma-based ELISA
experiments. However, the combined detection of ALDH, OCT4 and
NANOG markers may improve the accuracy and specificity of the
biomarker profile for diagnosis of cervical carcinoma.
In conclusion, it was demonstrated that ALDH1A1 and
OCT4 were upregulated in cervical carcinoma tissues and its
precursor lesions at the level of mRNA and protein, as well as in
blood plasma, which represents the protein levels in the whole
body. Notably, the samples subjected to analysis by RT-qPCR, IHC
and ELISA were obtained from three independent populations of
patients and controls, which may increase the feasibility and
accuracy of quantitative verification. Despite the limited
prognostic potential of ALDH1A1 and OCT4 in the blood-based
detection, it may be suggested that the combined detection of these
proteins at the level of transcription, protein expression and in
the blood circulation may provide an auxiliary profile for the
prognosis, diagnosis and monitoring of the treatment of cervical
carcinoma.
Cervical cancer is a challenge for the Uighur female
population in Xinjiang, China, where there is a high incidence rate
(490–560/100,000) accompanied with the prevalence of HPV infection
(69,70). In accordance with preliminary data,
the case detection rate of cervical carcinoma accounts for ~20% of
all patients diagnosed with cancer in Xinjiang (71). Therefore, further validation of this
profiling, and further in-depth studies on the association of the
altered expression of stem cell markers with HPV infection by other
approaches, will contribute to establishing an auxiliary diagnostic
profile for HPV-based cancer prognosis and greatly benefit the
women in areas with a high prevalence, including Uighur women in
China.
Acknowledgements
Not applicable.
Funding
The present study was supported by grants from the
Natural Science Foundation of China (grant no. 81360321) and the
Natural Science Fund for Young Scholars of Xinjiang Uighur
Autonomous Region China (grant. no. 2017D01C139). The funders had
no role in the study design, data collection, analysis, decision to
publish or preparation of the manuscript.
Availability of data and materials
The datasets generated and/or analysed during this
study are available from the corresponding author on reasonable
request.
Authors' contributions
AA designed the research. WT, RY and LS performed
the research. MR and RY were responsible for clinical diagnosis and
sample collection. DL contributed to data collection and
statistical analysis. AA and WT wrote the manuscript. All the
authors read and approved the final manuscript.
Ethics approval and consent to
participate
Te present study was approved and monitored by the
Ethics Committee of Xinjiang Medical University (Urumqi, China).
All procedures performed in this study were followed in accordance
with the Helsinki Declaration of 1975, as revised in 2000 (5). Written informed consent was obtained
from all patients and healthy individuals prior to the study, and
all data were analyzed anonymously.
Patient consent for publication
Written informed consent was obtained from all
individual participants included in the present study.
Competing interests
All authors declare that they have no competing
interest.
References
|
1
|
Meacham CE and Morrison SJ: Tumour
heterogeneity and cancer cell plasticity. Nature. 501:328–337.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Islam F, Gopalan V, Smith RA and Lam AK:
Translational potential of cancer stem cells: A review of the
detection of cancer stem cells and their roles in cancer recurrence
and cancer treatment. Exp Cell Res. 335:135–147. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ferenczy A and Franco E: Persistent human
papillomavirus infection and cervical neoplasia. Lancet Oncol.
3:11–16. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tindle RW: Immune evasion in human
papillomavirus-associated cervical cancer. Nat Rev Cancer. 2:59–65.
2002. View
Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chhabra R: Cervical cancer stem cells:
Opportunities and challenges. J Cancer Res Clin Oncol.
141:1889–1897. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
López J, Valdez-Morales FJ,
Benitez-Bribiesca L, Cerbón M and Carrancá AG: Normal and cancer
stem cells of the human female reproductive system. Reprod Biol
Endocrinol. 11:532013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Herfs M, Yamamoto Y, Laury A, Wang X,
Nucci MR, McLaughlin-Drubin ME, Münger K, Feldman S, McKeon FD,
Xian W and Crum CP: A discrete population of squamocolumnar
junction cells implicated in the pathogenesis of cervical cancer.
Proc Natl Acad Sci USA. 109:10516–10521. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Letian T and Tianyu Z: Cellular receptor
binding and entry of human papillomavirus. Virol J. 7:22010.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pyeon D, Pearce SM, Lank SM, Ahlquist P
and Lambert PF: Establishment of human papillomavirus infection
requires cell cycle progression. PLoS Pathog. 5:e10003182009.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Quade BJ, Yang A, Wang Y, Sun D, Park J,
Sheets EE, Cviko A, Federschneider JM, Peters R, McKeon FD and Crum
CP: Expression of the p53 homologue p63 in early cervical
neoplasia. Gynecol Oncol. 80:24–29. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sell S: On the stem cell origin of cancer.
Am J Pathol. 176:2584–2494. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Martens JE, Arends J, Van der Linden PJ,
De Boer BA and Helmerhorst TJ: Cytokeratin 17 and p63 are markers
of the HPV target cell, the cervical stem cell. Anticancer Res.
24:771–775. 2004.PubMed/NCBI
|
|
13
|
Mighty KK and Laimins LA: p63 is necessary
for the activation of human papillomavirus late viral functions
upon epithelial differentiation. J Virol. 85:8863–8869. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang Z, Oron E, Nelson B, Razis S and
Ivanova N: Distinct lineage specification roles for NANOG, OCT4 and
SOX2 in human embryonic stem cells. Cell Stem Cell. 10:440–454.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hattori N, Imao Y, Nishino K, Hattori N,
Ohgane J, Yagi S, Tanaka S and Shiota K: Epigenetic regulation of
Nanog gene in embryonic stem and trophoblast stem cells. Genes
Cells. 12:387–396. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ye F, Zhou C, Cheng Q, Shen J and Chen H:
Stem-cell-abundant proteins Nanog, Nucleostemin and Musashi1 are
highly expressed in malignant cervical epithelial cells. BMC
cancer. 8:1082008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Liu D, Zhou P, Zhang L, Wu G, Zheng Y and
He F: Differential expression of Oct4 in HPV-positive and
HPV-negative cervical cancer cells is not regulated by DNA
methyltransferase 3A. Tumour Biol. 32:941–950. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Li SW, Wu XL, Dong CL, Xie XY, Wu JF and
Zhang X: The differential expression of OCT4 isoforms in cervical
carcinoma. PLoS One. 10:e01180332015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yao T, Chen Q, Zhang B, Zhou H and Lin Z:
The expression of ALDH1 in cervical carcinoma. Med Sci Monit.
17:HY21–HY26. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Rao QX, Yao TT, Zhang BZ, Lin RC, Chen ZL,
Zhou H, Wang LJ, Lu HW, Chen Q, Di N and Lin ZQ: Expression and
functional role of ALDH1 in cervical carcinoma cells. Asian Pac J
Cancer Prev. 13:1325–1331. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Liu SY and Zheng PS: High aldehyde
dehydrogenase activity identifies cancer stem cells in human
cervical cancer. Oncotarget. 4:2462–2475. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Li J and Zhou BP: Activation of
beta-catenin and Akt pathways by Twist are critical for the
maintenance of EMT associated cancer stem cell-like characters. BMC
Cancer. 11:492011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lin J, Liu X and Ding D: Evidence for
epithelial-mesenchymal transition in cancer stem-like cells derived
from carcinoma cell lines of the cervix uteri. Int J Clin Exp
Pathol. 8:847–855. 2015.PubMed/NCBI
|
|
24
|
Saslow D, Runowicz CD, Solomon D, Moscicki
AB, Smith RA, Eyre HJ and Cohen C: American Cancer, Society:
American Cancer Society guideline for the early detection of
cervical neoplasia and cancer. CA Cancer J Clin. 52:342–362. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pecorelli S, Benedet JL, Creasman WT and
Shepherd JH: FIGO staging of gynecologic cancer. 1994–1997 FIGO
Committee on Gynecologic Oncology. International Federation of
Gynecology and Obstetrics. Int J Gynaecol Obstet. 65:243–249. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2 (-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mason DY: Immunocytochemical analysis of
human tissueOxford Textbook of Pathology. Oxford University Press;
Oxford: 2. pp. 2275–2284. 1992
|
|
28
|
Ping YF and Bian XW: Consice review:
Contribution of cancer stem cells to neovascularization. Stem
Cells. 29:888–894. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
29
|
Facompre N, Nakagawa H, Herlyn M and Basu
D: Stem-like cells and therapy resistance in squamous cell
carcinomas. Adv Pharmacol. 65:235–265. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Patel P and Chen EI: Cancer stem cells,
tumor dormancy, and metastasis. Front Endocrinol (Lausanne).
3:1252012.PubMed/NCBI
|
|
31
|
Andrews TE, Wang D and Harki DA: Cell
surface markers of cancer stem cells: Diagnostic macromolecules and
targets for drug delivery. Drug Deliv Transl Res. 3:121–142. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Xia P: Surface markers of cancer stem
cells in solid tumors. Curr Stem Cell Res Ther. 9:102–111. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Allegra A, Alonci A, Penna G, Innao V,
Gerace D, Rotondo F and Musolino C: The cancer stem cell
hypothesis: A guide to potential molecular targets. Cancer Invest.
32:470–495. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sladek NE: Human aldehyde dehydrogenases:
Potential pathological, pharmacological, and toxicological impact.
J Biochem Mol Toxicol. 17:7–23. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Chute JP, Muramoto GG, Whitesides J,
Colvin M, Safi R, Chao NJ and McDonnell DP: Inhibition of aldehyde
dehydrogenase and retinoid signaling induces the expansion of human
hematopoietic stem cells. Proc Natl Acad Sci USA. 103:11707–11712.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Marcato P, Dean CA, Giacomantonio CA and
Lee PW: Aldehyde dehydrogenase: Its role as a cancer stem cell
marker comes down to the specific isoform. Cell Cycle.
10:1378–1384. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Tomita H, Tanaka K, Tanaka T and Hara A:
Aldehyde dehydrogenase 1A1 in stem cells and cancer. Oncotarget.
7:11018–11032. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Le Magnen C, Bubendorf L, Rentsch CA,
Mengus C, Gsponer J, Zellweger T, Rieken M, Thalmann GN, Cecchini
MG, Germann M, et al: Characterization and clinical relevance of
ALDHbright populations in prostate cancer. Clin Cancer Res.
19:5361–5371. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Kurashige T, Shimamura M, Yasui K,
Mitsutake N, Matsuse M, Nakashima M, Minami S, Eguchi S and
Nagayama Y: Studies on the expression of aldehyde dehydrogenase in
normal and cancerous tissues of thyroids. Horm Metab Res.
47:194–199. 2015.PubMed/NCBI
|
|
40
|
Wu S, Xue W, Huang X, Yu X, Luo M, Huang
Y, Liu Y, Bi Z, Qiu X and Bai S: Distinct prognostic values of
ALDH1 isoenzymes in breast cancer. Tumour Biol. 36:2421–2426. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Patel M, Lu L, Zander DS, Sreerama L, Coco
D and Moreb JS: ALDH1A1 and ALDH3A1 expression in lung cancers:
Correlation with histologic type and potential precursors. Lung
Cancer. 59:340–349. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Hou T, Zhang W, Tong C, Kazobinka G, Huang
X, Huang Y and Zhang Y: Putative stem cell markers in cervical
squamous cell carcinoma are correlated with poor clinical outcome.
BMC Cancer. 15:7852015. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Yao T, Wu Z, Liu Y, Rao Q and Lin Z:
Aldehyde dehydrogenase 1 (ALDH1) positivity correlates with poor
prognosis in cervical cancer. J Int Med Res. 42:1038–1042. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Xie Q, Liang J, Rao Q, Xie X, Li R, Liu Y,
Zhou H, Han J, Yao T and Lin Z: Aldehyde dehydrogenase 1 expression
predicts chemoresistance and poor clinical outcomes in patients
with locally advanced cervical cancer treated with neoadjuvant
chemotherapy prior to radical hysterectomy. Ann Surg Oncol.
23:163–170. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Chen X, Xu H, Yuan P, Fang F, Huss M, Vega
VB, Wong E, Orlov YL, Zhang W, Jiang J, et al: Integration of
external signaling pathways with the core transcriptional network
in embryonic stem cells. Cell. 133:1106–1117. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Kim J, Chu J, Shen X, Wang J and Orkin SH:
An extended transcriptional network for pluripotency of embryonic
stem cells. Cell. 132:1049–1061. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Zeineddine D, Hammoud AA, Mortada M and
Boeuf H: The Oct4 protein: More than a magic stemness marker. Am J
Stem Cells. 3:74–82. 2014.PubMed/NCBI
|
|
48
|
Boyer LA, Lee TI, Cole MF, Johnstone SE,
Levine SS, Zucker JP, Guenther MG, Kumar RM, Murray HL, Jenner RG,
et al: Core transcriptional regulatory circuitry in human embryonic
stem cells. Cell. 122:947–956. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Rizzino A: Concise review: The Sox2-Oct4
connection: Critical players in a much larger interdependent
network integrated at multiple levels. Stem Cells. 31:1033–1039.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Liedtke S, Stephan M and Kögler G: Oct4
expression revisited: Potential pitfalls for data misinterpretation
in stem cell research. Biol Chem. 389:845–850. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Wang YJ and Herlyn M: The emerging roles
of Oct4 in tumor-initiating cells. Am J Physiol Cell Physiol.
309:C709–C718. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Wang YD, Cai N, Wu XL, Cao HZ, Xie LL and
Zheng PS: OCT4 promotes tumorigenesis and inhibits apoptosis of
cervical cancer cells by miR-125b/BAK1 pathway. Cell Death Dis.
4:e7602013. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Echelman D and Feldman S: Management of
cervical precancers: a global perspective. Hematol Oncol Clin North
Am. 26:31–44. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Kim BW, Cho H, Choi CH, Ylaya K, Chung JY,
Kim JH and Hewitt SM: Clinical significance of OCT4 and SOX2
protein expression in cervical cancer. BMC Cancer. 15:10152015.
View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Liu D, Zhou P, Zhang L, Zheng Y and He F:
HPV16 activates the promoter of Oct4 gene by sequestering HDAC1
from repressor complex to target it to proteasomal degradation. Med
Hypotheses. 79:531–534. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Tyagi A, Vishnoi K, Mahata S, Verma G,
Srivastava Y, Masaldan S, Roy BG, Bharti AC and Das BC: Cervical
cancer stem cells selectively overexpress HPV oncoprotein E6 that
controls stemness and self-renewal through upregulation of HES1.
Clin Cancer Res. 22:4170–4184. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Yang MH, Imrali A and Heeschen C:
Circulating cancer stem cells: The importance to select. Clin
Cancer Res. 27:437–449. 2015.
|
|
58
|
Cao YT, Li JH, Wang YT, Fu YW and Xu J:
Serum ALDH1A1 is a tumor marker for the diagnosis of non-small cell
lung cancer. Tumori. 100:214–218. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Sladek NE, Kollander R, Sreerama L and
Kiang DT: Cellular levels of aldehyde dehydrogenases (ALDH1A1 and
ALDH3A1) as predictors of therapeutic responses to
cyclophosphamide-based chemotherapy of breast cancer: A
retrospective study. Rational individualization of
oxazaphosphorine-based cancer chemotherapeutic regimens. Cancer
Chemother Pharmacol. 49:309–321. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Chang TS, Wu YC, Chi CC, Su WC, Chang PJ,
Lee KF, Tung TH, Wang J, Liu JJ, Tung SY, et al: Activation of
IL6/IGFIR confers poor prognosis of HBV-related hepatocellular
carcinoma through induction of OCT4/NANOG expression. Clin Cancer
Res. 21:201–210. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Bobryshev YV, Orekhov AN and Chistiakov
DA: Vascular stem/progenitor cells: Current status of the problem.
Cell Tissue Res. 362:1–7. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Krenning G, Barauna VG, Krieger JE,
Harmsen MC and Moonen JR: Endothelial plasticity: Shifting
phenotypes through force feedback. Stem Cells Int.
2016:97629592016. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Minhajat R, Nilasari D and Bakri S: The
role of endothelial progenitor cell in cardiovascular disease risk
factors. Acta Med Indones. 47:340–347. 2015.PubMed/NCBI
|
|
64
|
Gu W, Hong X, Potter C, Qu A and Xu Q:
Mesenchymal stem cells and vascular regeneration. Microcirculation.
24:2017.doi: 10.1111/micc.12324. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Sherman SE, Kuljanin M, Cooper TT, Putman
DM, Lajoie GA and Hess DA: High aldehyde dehydrogenase activity
identifies a subset of human mesenchymal stromal cells with
vascular regenerative potential. Stem Cells. 35:1542–1553. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Constantinescu S: Stemness, fusion and
renewal of hematopoietic and embryonic stem cells. J Cell Mol Med.
7:103–112. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Hattori N, Imao Y, Nishino K, Hattori N,
Ohgane J, Yagi S, Tanaka S and Shiota K: Epigenetic regulation of
Nanog gene in embryonic stem and trophoblast stem cells. Genes
Cells. 12:387–396. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Ben-Porath I, Thomson MW, Carey VJ, Ge R,
Bell GW, Regev A and Weinberg RA: An embryonic stem cell-like gene
expression signature in poorly differentiated aggressive human
tumors. Nat Genet. 40:499–507. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
69
|
Suzuke L, Peng YH, Zhou K, et al: The
analysis of pathogenetic tendency of cervical cancer in various
ethnic women in Xinjiang. J Xinjiang Med Univ. 29:569–571. 2006.(In
Chinese).
|
|
70
|
Abudoukadeer A, Niyazi M, Aikula A,
Kamilijian M, Sulaiman X, Mutailipu A and Abudula A: Association of
EBV and HPV co-infection with the development of cervical cancer in
ethnic Uyghur women. Eur J Gynaecol Oncol. 36:546–550.
2015.PubMed/NCBI
|
|
71
|
Zhang GQ, LIU KJ, Lai XJ, et al:
Distribution of malignant tumor patients in hospital from 1989 to
2002 in the Affiliated Tumor Hospital of Xinjiang Medical
University. J Xinjiang Med Univ. 26:393–395. 2003.(In Chinese).
|