Introduction
Gastric cancer frequently spreads to the regional
lymph nodes, liver and lungs following surgery or late in the
clinical course (1). Gastric cancer
rarely shows dissemination to the bones, and the incidence of bone
metastasis due to gastric cancer is only 0.9–3.8% (1–4). Bone
metastasis is usually recognized as parallel disease recurrence
following surgery (1–3) or progression during follow-up, and
occurs in the late stage of the disease (2–4). Initial
(or simultaneous) presentation of bone metastasis, particularly in
asymptomatic gastric cancer, is extremely rare (5–8). The
present study describes two cases of gastric cancer initially
presenting with an increased serum alkaline phosphatase (ALP) level
without any clinical symptoms and as a swelling in the right
carpometacarpal joint of the thumb, respectively. The former case
showed diffuse spinal vertebral bone metastasis, while the latter
showed a single trapezium metastasis. The two cases were diagnosed
as metastatic gastric cancer on further examination. The present
study also describes the clinical courses and reviews the initial
bone metastases in patients with gastric cancer from the
literature.
Case report
Case 1
A 60-year-old woman with no significant past medical
history or symptoms was referred to Shinshu University Hospital
(Nagano, Japan) on April 2013 due to progressive increases in ALP
level that had been detected by routine health screening over a
period of 7 months. Physical examinations were unremarkable.
Laboratory findings indicated a markedly increased ALP level (4,917
IU/l; normal, <322 IU/l), but other findings were normal,
including the level of carcinoembryonic antigen (CEA; 1.9 mg/dl;
normal, <0.5 mg/dl). Bone scintigraphy showed multiple abnormal
uptake of radioactive material particularly in the lumbar vertebrae
(Fig. 1A). A review of computed
tomography (CT) (Fig. 1B) and
magnetic resonance imaging data showed multiple osteolytic bone
metastases, particularly in the lumbar vertebrae.
Fluorodeoxyglucose-positron emission tomography/CT (FDG-PET/CT)
revealed multiple bone metastases, including pubic, rib and lumbar
vertebrae metastases, with no other abnormal FDG uptake except in
these bone lesions. Needle biopsy of the left iliac bone was
performed and the histological findings showed adenocarcinoma with
the formation of large vacuoles full of mucin that displace the
nucleus to the cell's periphery suggesting signet cell carcinoma
(Fig. 2A and B). The specimen was
fixed in 20% neutral-buffered formalin and decalcified in 10%
formic acid for one day at room temperature. The decalcified
specimen block was then embedded in paraffin, sliced into sections
of 4-µm thickness, and stained with hematoxylin and eosin for 90
min at room temperature. The images were captured with an Olympus
BX51 microscope (objective, ×40) and Olympus DP70 camera.
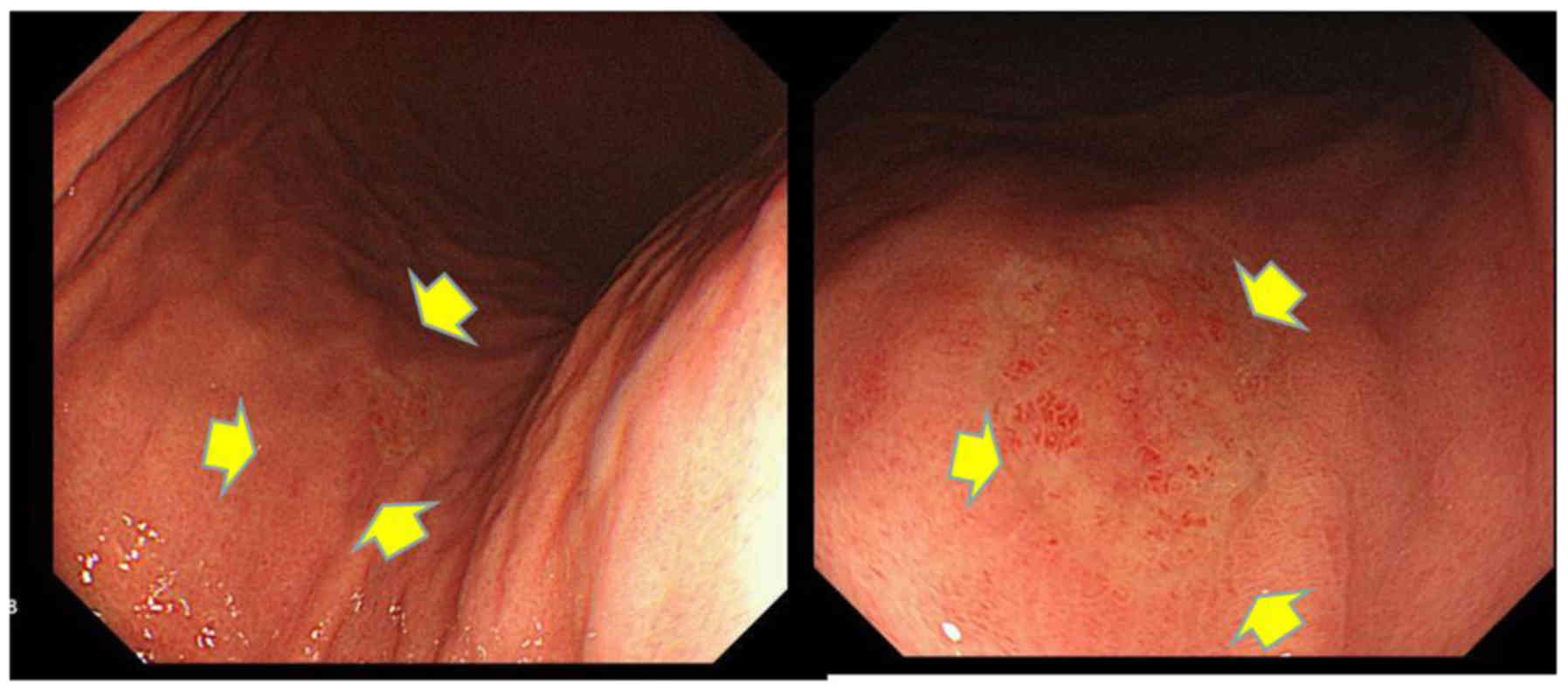
Histological findings (Fig. 2C and D)
of a small flat depressed lesion in the middle gastric body area,
which was revealed by esophagogastroduodenoscopy (Fig. 3), revealed the presence of similar
signet cell carcinoma in gastric mucosa with those in iliac bone as
aforementioned. Therefore, a diagnosis of gastric signet cell
carcinoma with multiple bone metastases was made.
Immunohistochemical analysis for epidermal growth factor receptor 2
(HER2) was negative in this case. The patient received combined
chemotherapy of cisplatin (80 mg/m2, day 8
postoperatively) plus S-1 (80 mg/m2, day 1–21
postoperatively) followed by S-1 monotherapy (80 mg/m2,
day 1–28 every 6 weeks), and denosumab (a fully human monoclonal
antibody that inhibits receptor activator of nuclear factor-κB
ligand, 120 mg once every 6 weeks). Subsequent to six cycles of
cisplatin plus S-1 therapy, gastrointestinal endoscopic findings
confirmed scarring of the primary gastric cancer, and the ALP was
determined to have returned to a normal level (189 IU/l). The
disease was controlled with S-1 monotherapy over 1 year, but the
patient finally developed disseminated intravascular coagulation
(DIC) and liver metastasis, and succumbed 2 years after
diagnosis.
Case 2
A 62-year-old man presented with a swelling in the
right carpometacarpal (CMC) joint of the thumb. Conservative
treatment for thumb CMC osteoarthritis had been performed for 3
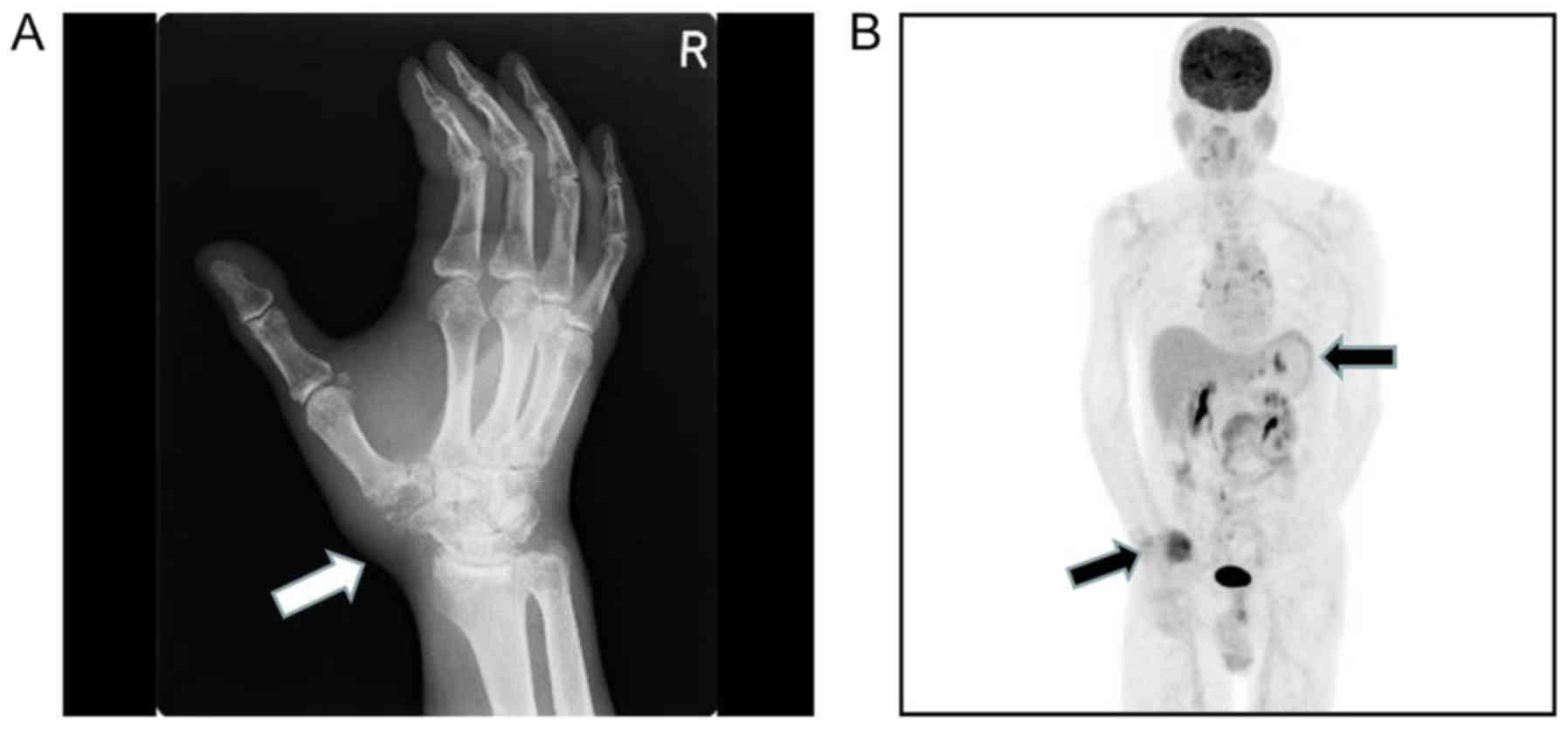
months. However, radiographic findings revealed an osteolytic
lesion in the trapezium, with resorption of almost the whole of the
trapezium (Fig. 4A) and referred to
Shinshu University Hospital on October 2014. Needle biopsy was
performed and histopathological examination was performed as
described previously, and indicated the presence of tubular
adenocarcinoma. FDG-PET/CT revealed positive accumulation of FDG in
the trapezium and epigastrium (Fig.
4B). Based on the results of FDG-PET, an
esophagogastroduodenoscopy was performed and showed an advanced and
ulcerative tumor (Fig. 5A). The
results of histological examination of the gastric specimens were
consistent with those in the trapezium as aforementioned. The serum
CEA level was normal (3.2 mg/ml). No other distant metastases were
found. Therefore, a diagnosis of advanced gastric adenocarcinoma
with a single metastasis to the CMC joint of the thumb was made.
Immunohistochemical analysis for HER2 was negative in this case.
Radiotherapy (3 Gy/10 fractions; total, 30 Gy) to the metastatic
CMC area was performed. The patient was treated with six cycles of
systemic chemotherapy with cisplatin (60 mg/m2 day 8)
and S-1 (80 mg/m2 day 1–21), followed by S-1 (80
mg/m2, day 1–28, every 6 weeks) maintenance therapy,
which resulted in a partial response of the primary lesion to the
chemotherapy (Fig. 5B). The patient
visited Shinshu University every 6 weeks for S-1 maintenance
therapy and remains alive 2 years after the initiation of
chemotherapy without any signs of recurrence.
Discussion
According to 3 case reports, initial clinical
manifestations associated with bone metastasis are extremely rare
in patients with gastric cancer (6–8). In the
present study, increased ALP levels were noted by routine
laboratory survey in case 1, without any symptoms associated with
bone involvement, and swelling in the right CMC joint of the thumb
due to trapezium metastasis was noted in case 2. The clinical
manifestations of bone metastasis observed in these cases are
extremely rare as the initial signs of asymptomatic gastric cancer.
Clinical physicians should be aware of the possibility of initial
bone involvement in patients with gastric cancer.
Kim et al (5)
summarized the findings in patients with initial bone metastasis in
gastric cancer and reported that bone metastasis is often
accompanied by lymphangitic lung metastasis, pleural metastasis,
leptomeningeal metastasis, a primary tumor involving more than
two-thirds of the stomach and hematological abnormalities,
including DIC or elevated ALP. In addition, the most common
histological type was signet cell carcinoma. ALP is known to be the
most predictive biological marker for the presence of bone
metastasis in gastric cancer (9). In
the present study, in case 1, the signet cell carcinoma
histological type and elevated level of ALP were consistent with
these predictors of initial bone metastasis in gastric cancer.
However, the patient was asymptomatic and presented with no other
metastatic sites. In addition, endoscopic findings indicated a
small abnormality so-called occult primary tumor in case 1. These
cases suggested that gastric cancer should be considered in
patients with elevated ALP without any clinical symptoms. A search
for similar case reports in PubMed (https://www.ncbi.nlm.nih.gov/pubmed/) using the terms
‘occult gastric cancer’, ‘bone metastasis’ or ‘ALP’ did not find
any similar cases. Thus, although the clinical manifestations in
case 1 were quite unique, it should be emphasized that gastric
cancer is a possible disease in patients with elevated ALP.
The most frequent sites of bone metastasis are the
vertebrae, followed by the ribs, scapulae, lower extremities and
upper extremities (10–12). In the present study, the location and
single metastasis to the trapezium in case 2 is noteworthy. To the
best of our knowledge, this is the first report of a single
metastasis from gastric cancer to the trapezium. Although
endoscopic findings of the primary lesion showed advanced gastric
cancer, a single trapezium metastasis without any other distant
spread is extremely rare in gastric cancer.
Riihimäki et al (13) reported that gastric cancer patients
with bone metastasis showed the poorest median survival time
compared with those with metastases in other sites, including the
thorax, liver or other regions of the abdomen. In addition,
patients with initial (simultaneous) bone metastasis in gastric
cancer exhibited significantly poorer overall survival time
following the diagnosis of gastric cancer compared with late-phase
bone metastasis (3,5,10).
However, survival time following diagnosis of bone metastasis in
gastric cancer was slightly longer in the initial bone metastasis
patients compared with that in those with late-phase bone
metastasis (5). Several studies
indicated that systemic chemotherapy could improve survival, even
in patients with initial bone metastasis of gastric cancer
(3–5,14). In the
two cases presented in the present study, cisplatin plus S-1, a
standard chemotherapy regimen for advanced gastric cancer (15), was effective for disease control.
Subsequent to chemotherapy, the ALP level returned to normal in
case 1 and the gastric tumor was undetectable on endoscopy in case
2, which may indicate a favorable clinical outcome in each case.
Thus, these results suggest that cisplatin plus S-1 is a useful
chemotherapeutic regimen for gastric cancer with bone
metastasis.
In summary, the present cases indicated that gastric
cancer exhibits a variety of clinical features with regard to bone
metastasis, particularly in the initial clinical presentation of
the disease. In addition, the cases indicated the importance of the
detection of potential gastric cancer in patients with an initial
presentation of bone metastasis. Thus, gastric cancer should be
considered in the differential diagnosis in patients initially
presenting with single or multiple bone metastases.
Acknowledgements
Not applicable.
Funding
No funding was received for the present case
study.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
DG, TF, TK, NS, AS, KM and TK contributed to the
treatment of the two cases, and DG and TK wrote the manuscript.
Ethics approval and consent to
participate
Written informed consent for the publication of any
associated data and accompanying images was obtained from the
patients or their guardians.
Patient consent for publication
Written informed consent for the publication of any
associated data and accompanying images was obtained from the
patients or their guardians.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Guadagni S, Catarci M, Kinoshitá T,
Valenti M, De Bernardinis G and Carboni M: Causes of death and
recurrence after surgery for early gastric cancer. World J Surg.
21:434–439. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nakamura K, Tomioku M, Nabeshima K and
Yasuda S: Clinicopathologic features and clinical outcomes of
gastric cancer patients with bone metastasis. Tokai J Exp Clin Med.
39:193–198. 2014.PubMed/NCBI
|
|
3
|
Turkoz FP, Solak M, Kilickap S, Ulas A,
Esbah O, Oksuzoglu B and Yalcin S: Bone metastasis from gastric
cancer: The incidence, clinicopathological features, and influence
on survival. J Gastric Cancer. 14:164–172. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Park HS, Rha SY, Kim HS, Hyung WJ, Park
JS, Chung HC, Noh SH and Jeung HC: A prognostic model to predict
clinical outcome in gastric cancer patients with bone metastasis.
Oncology. 80:142–150. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kim YJ, Kim SH, Kim JW, Lee JO, Kim JH,
Bang SM, Lee JS and Lee KW: Gastric cancer with initial bone
metastasis: A distinct group of diseases with poor prognosis. Eur J
Cancer. 50:2810–2821. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Basheer A, Daniel J and Padhi S:
Compressive myeloradiculopathy from bony metastasis as the initial
presentation of poorly differentiated adenocarcinoma stomach-a case
report. Australas Med J. 6:515–519. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mohandas KM, Swaroop VS, Krishnamurthy S,
Desai DC, Dhir V, Pradhan SA, Jagannath P and Desouza LJ: Unusual
bone metastasis as the initial symptom of gastric cancer-a report
of four cases. Indian J Cancer. 30:146–150. 1993.PubMed/NCBI
|
|
8
|
Cao X, Cui F, Wei J, Wang Q, Deng LC, Liu
BR and Shen WS: Hearing loss due to metastasis of gastric cancer to
temporal bone: A case report. Oncol Lett. 11:1305–1308. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lim SM, Kim YN, Park KH, Kang B, Chon HJ,
Kim C, Kim JH and Rha SY: Bone alkaline phosphatase as a surrogate
marker of bone metastasis in gastric cancer patients. BMC Cancer.
16:3852016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Silvestris N, Pantano F, Ibrahim T,
Gamucci T, De Vita F, Di Palma T, Pedrazzoli P, Barni S, Bernardo
A, Febbraro A, et al: Natural history of malignant bone disease in
gastric cancer: Final results of a multicenter bone metastasis
survey. PLoS One. 8:e744022013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mikami J, Kimura Y, Makari Y, Fujita J,
Kishimoto T, Sawada G, Nakahira S, Nakata K, Tsujie M and Ohzato H:
Clinical outcomes and prognostic factors for gastric cancer
patients with bone metastasis. World J Surg Oncol. 15:82017.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ahn JB, Ha TK and Kwon SJ: Bone metastasis
in gastric cancer patients. J Gastric Cancer. 11:38–45. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Riihimäki M, Hemminki A, Sundquist K,
Sundquist J and Hemminki K: Metastatic spread in patients with
gastric cancer. Oncotarget. 7:52307–52316. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lee J, Lim T, Uhm JE, Park KW, Park SH,
Lee SC, Park JO, Park YS, Lim HY, Sohn TS, et al: Prognostic model
to predict survival following first-line chemotherapy in patients
with metastatic gastric adenocarcinoma. Ann Oncol. 18:886–891.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Koizumi W, Narahara H, Hara T, Takagane A,
Akiya T, Takagi M, Miyashita K, Nishizaki T, Kobayashi O, Takiyama
W, et al: S-1 plus cisplatin versus S-1 alone for first-line
treatment of advanced gastric cancer (SPIRITS trial): A phase III
trial. Lancet Oncol. 9:215–221. 2008. View Article : Google Scholar : PubMed/NCBI
|