Introduction
Ovarian cancer is known to develop in approximately
1% of women with endometriosis (1).
Endometriosis might be related to an increased risk of EAOC, but
the underlying mechanism remains unclear (2). Current screening modalities for
detecting differences between patients with benign ovarian
endometrioma (OE) and EAOC include transvaginal ultrasounds and
serum CA125 levels. CA125 is the most commonly used serum marker to
predict the presence of ovarian cancer, but the specificity of
CA125 is low (3). Recent
retrospective study demonstrated that the preoperative CA125 value
was not useful for detecting patients with malignant transformation
of endometriosis (4). So far, no
sensitive serum biomarker has been characterized. Furthermore, the
important preoperative findings for a diagnosis of malignant change
is the presence of endometriotic lesions with worrisome features,
including a mural nodule, a solid mass, a thickened wall, and a
cyst size of >7~8 cm, or rapid cyst growth at ultrasonography
(1). If EAOC shows a lack of mural
nodules in its early stages, this tumor causes great diagnostic
difficulties. At present, early and accurate clinical noninvasive
prediction of malignant transformation remains challenging. We will
summarize the accumulated current status of knowledge of recent
advances in the various imaging modalities for the noninvasive
diagnosis of EAOC. Growth in current knowledge of carcinogenesis
facilitates strategies for early diagnosis, appropriate management,
and disease monitoring.
Materials and methods
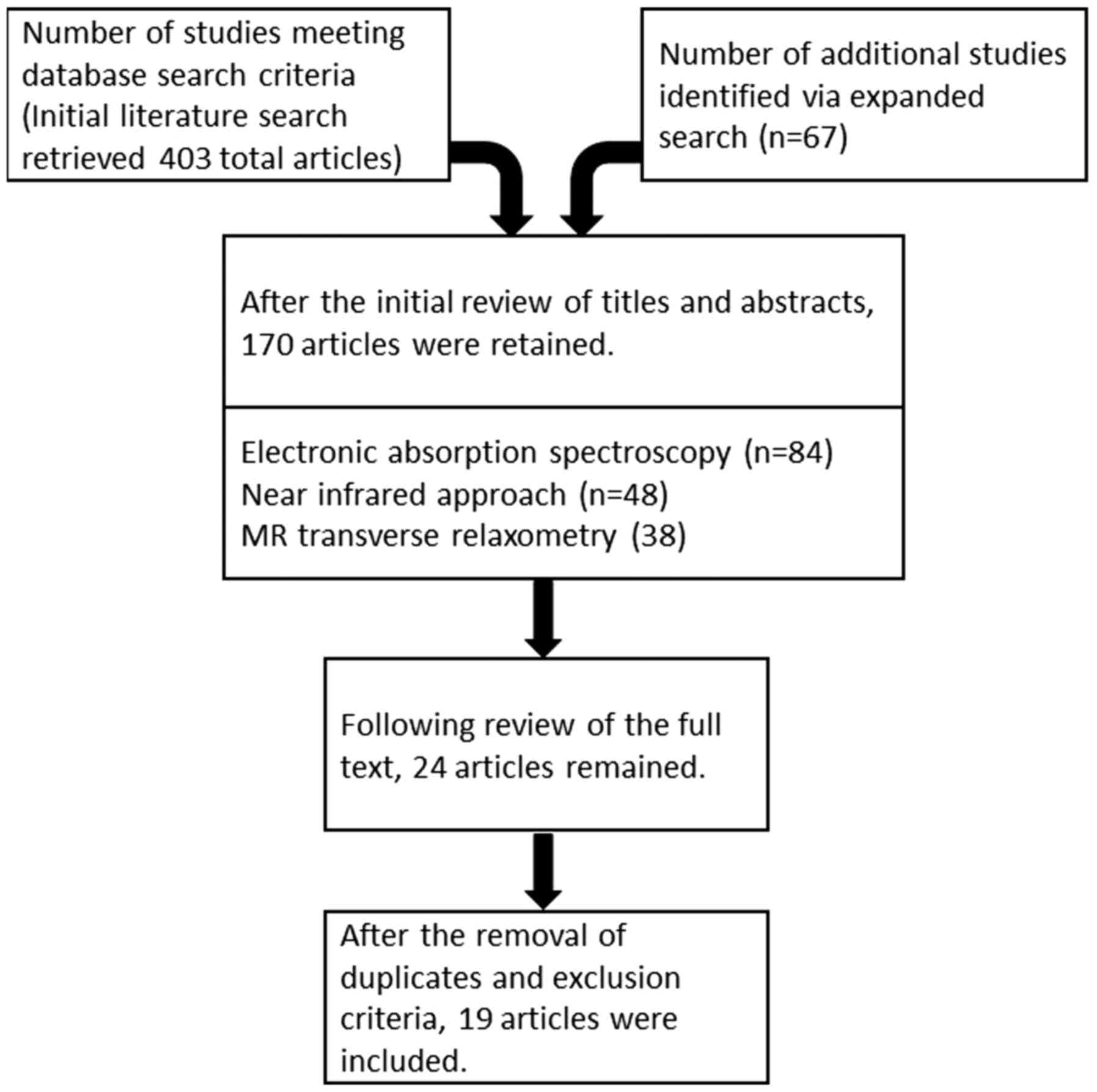
A computerized literature search was conducted to
identify relevant studies reported in the English language. We
collected a comprehensive literature search from PubMed and Embase
database up to April 2018, combining the keywords ‘endometriosis’,
‘endometriosis-associated ovarian cancer’, ‘endometrioid
carcinoma’, ‘clear cell carcinoma’, ‘diagnosis’, ‘discrimination’,
‘hemoglobin’ and ‘iron’. A variety of combinations of these terms
were used, depending on which database was searched. Furthermore,
the references of each article were searched to identify
potentially relevant studies. Publications of original studies and
review papers were included, while those documenting opinions,
points of view or anecdotes were discarded. The flow chart of the
literature search is presented in Fig.
1.
Noninvasive techniques and novel
modalities for discrimination of EAOC from benign OE
The aim of this review was to discuss an effective
and noninvasive diagnostic tool for discrimination between EAOC and
benign OE. EAOC is thought to arise from endometriosis and should
be considered in the differential diagnosis of a pelvic mass
(2). Most important is to make the
discrimination between malignant and benign lesions preoperatively.
Ultrasound is used to differentiate solid lesions from simple
cysts. Typical ultrasound features of EAOC include
well-circumscribed masses with mural nodules resembling
‘xiaolongbao’ (Personal communication from Prof. Dr. Mikami Y.
Kumamoto University). However, the overlapping appearances of
benign and malignant lesions make ultrasound less useful in
differentiating malignant lesions, resulting in a large number of
surgery for benign tumors (5).
Therefore, ultrasonic morphological features are not relevant for
the discrimination between EAOC and benign OE with mural nodules.
Zhou and Hua (6), recently
demonstrated that times of pregnancy >1.5, tumor size >8.3
cm, and the presence of uterine leiomyoma and multiple foci of
endometriosis were independent risk factors for EAOC. Tanase et
al (5), identified the patient
demographics, clinical features and preoperative MR imaging
characteristics helpful to the differential diagnosis between EAOC
and benign OE with mural nodules. A majority (~80%) of the mural
nodular lesions of benign OE showed the pattern described as ‘cyst
with retracted blood clots’. Malignant transformation typically
manifests as cystic lesions with mural nodules, with various (low,
intermediate and high) signal intensities on T1-weighted images,
high-signal intensity on T2-weighted images, and a lower proportion
of shading in women undergoing screening MR imaging. Malignant
mural nodules was also found in the anterior location of the cyst
(5). When compared to subjects with
benign nodules, the patients with malignant mural nodules were
older (>43 years), had larger cyst diameters (>7.9 cm) and
larger mural nodule sizes (Height of mural nodules >1.5 cm), and
were more likely to exhibit a taller than wider lesion
(height-width ratio of mural nodules >0.9). ‘Height of mural
nodules >1.5 cm’ was the most valuable predictor for
discriminating EAOC from benign OE (AUC, 0.99; 95% CI, 0.97–1.0;
sensitivity 95.0%, specificity 95.2%).
The differential diagnosis between EAOC with
predominantly cystic appearances and benign OE is difficult and
require quantitative parameters that reflect the metabolic and
biochemical state of cyst fluid, which are translated into disease
diagnosis. When compared to subjects with benign OE, cyst fluid
analysis revealed low concentrations of Hb and iron-related
compounds in EAOC (7). This
observation reveals the possibility of early detection of
biochemical changes before morphological variations are captured
through ultrasonographic and MRI diagnosis. Investigators
highlighted practical applications of measuring these metabolic and
biochemical markers for discrimination between benign and malignant
endometriosis (7–9). Since the cyst fluid sampling is not a
serum-based test, noninvasive techniques for assessment of cyst
fluid levels of Hb-related compounds are clinically required. Hb
displays absorption spectra in the visible and UV regions (10). The specific spectroscopic changes are
invaluable for diagnostic applications of the concentration of Hb
(10). Such novel diagnostic
modalities include electronic absorption spectroscopy, near
infrared approach and MR transverse relaxometry.
Identification of cyst fluid
hemoglobin species by electronic absorption spectroscopy
Iwabuchi et al (11), reported the potential of electronic
absorption spectroscopy for evaluating the biochemical changes
through a metallobiologic diagnosis. Absorbance based approaches
have been developed for measuring Hb and iron-related compounds in
biological samples (12). It is a
well-known fact that a multi-wavelength spectrophotometric method
provides a noninvasive and real-time measurement of Hb
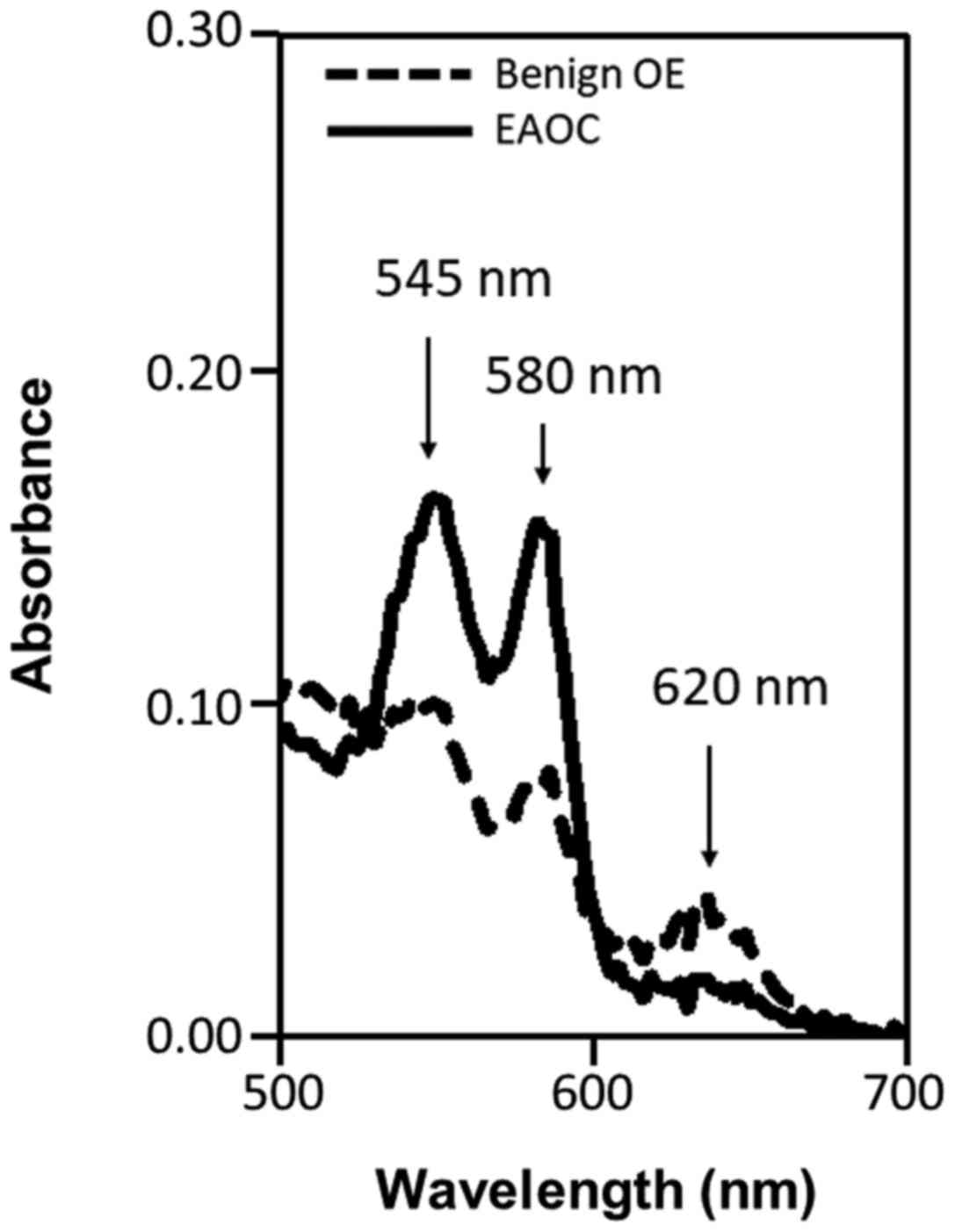
concentration (13). Fig. 2 shows representative absorption
spectra of cyst fluid samples obtained from benign OE and EAOC.
OxyHb is comprised of large-amplitude two peak components of
wavelengths of 540 and 580 nm, while metHb has strong absorption
than oxyHb, from 610 to 630 nm (11).
Absorption spectral curve of metHb shows one absorption peak at 620
nm (11). They hypothesized that the
characteristic change at 620 nm or the 620 nm/580 nm ratio would be
used to determine relative metHb concentration or the metHb/oxyHb
ratio, respectively. Relative concentrations of Hb species can be
calculated from the absorption spectra. The 620/580 nm absorption
ratio was significantly lower in the cyst fluid of patients with
EAOC than in that of patients with benign cysts (0.389±0.266 vs.
0.666±0.188, P=0.021) (11). The
sensitivity, specificity, positive predictive value, and negative
predictive value for predicting EAOC were 62.5, 100.0, 100.0, and
92.1%, respectively (11). From this
data, metHb is rich in the cyst fluid of OE and is a specific
biomarker for discriminating EAOC from benign OE. Iwabuchi et
al (11), reported that heme iron
is abundant in the cyst fluid of benign OE, therefore, autoxidation
might be the main process accomplishing the MetHb increases:
Hb-Fe2+ (oxyHb) + O2 → Hb-Fe3+ (metHb) + O2-.
Previous studies showed that the patients with EAOC had much lower
levels of Hb and iron-related compounds compared with those with
benign OE (7,8). EAOC allows the rapid reduction of metHb
possibly through the conversion of metHb into oxyHb (in vivo
autoreduction). Glutathione, an antioxidant overexpressed in EAOC,
is shown to be responsible for the conversion of metHb to oxyHb
(14,15). The difference in the metHb-to-oxyHb
ratio between benign and malignant endometriosis supports the
hypothesis that this is not a consequence of the simple dilution of
the cyst fluids.
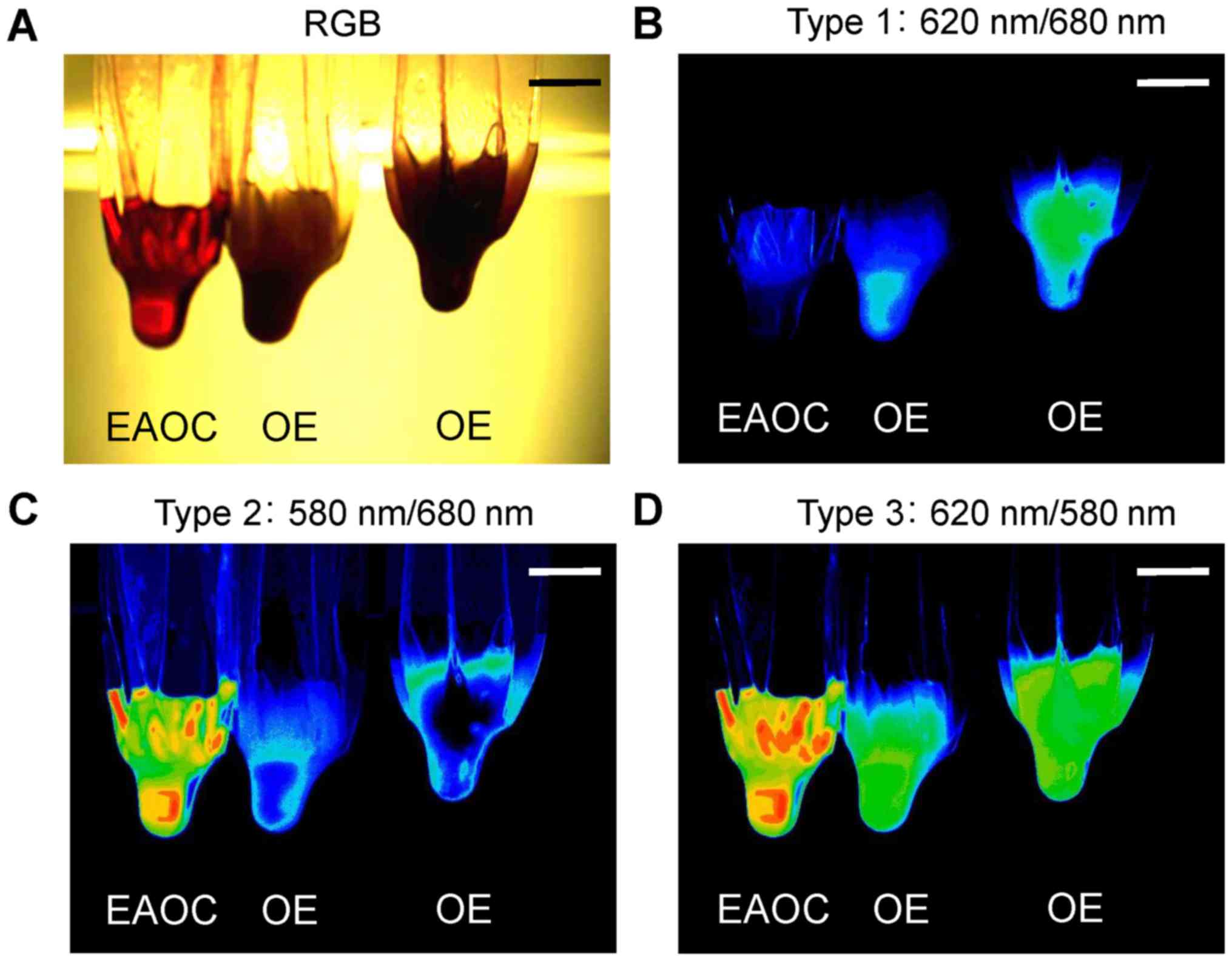
Furthermore, these authors proposed that an optical
method using light from halogen sources in a simple imaging setup
would provide reliable visualization of metHb and oxyHb content in
a cyst fluid sample. A simple and inexpensive optical imaging
system is composed of three functional modules: The visible light
stimulator, the image acquisition module with specific bandpass
filters as a wavelength selector, and the image processing unit
(11). Fig.
3 provides a representative ex-vivo color changes of the
cyst fluid samples that could be distinguished by the human eye on
any specimen (11). This optical
imaging system could allow visual detection of color changes by
monitoring specific wavelengths in the absorption spectra. Visible
light exhibited the limited penetration depth in biological tissue,
thus restricting the application of this optical imaging method for
disease diagnosis.
Identification of cyst fluid
hemoglobin species by near infrared approach
A near-infrared light can overcome the main
limitation of visible light imaging, indicating beneficial effects
in applications in humans. Kawahara et al (16), used noninvasive near-infrared
spectrophotometric method to determine cyst fluid absorption and
scattering coefficients and absolute cyst fluid Hb and total iron
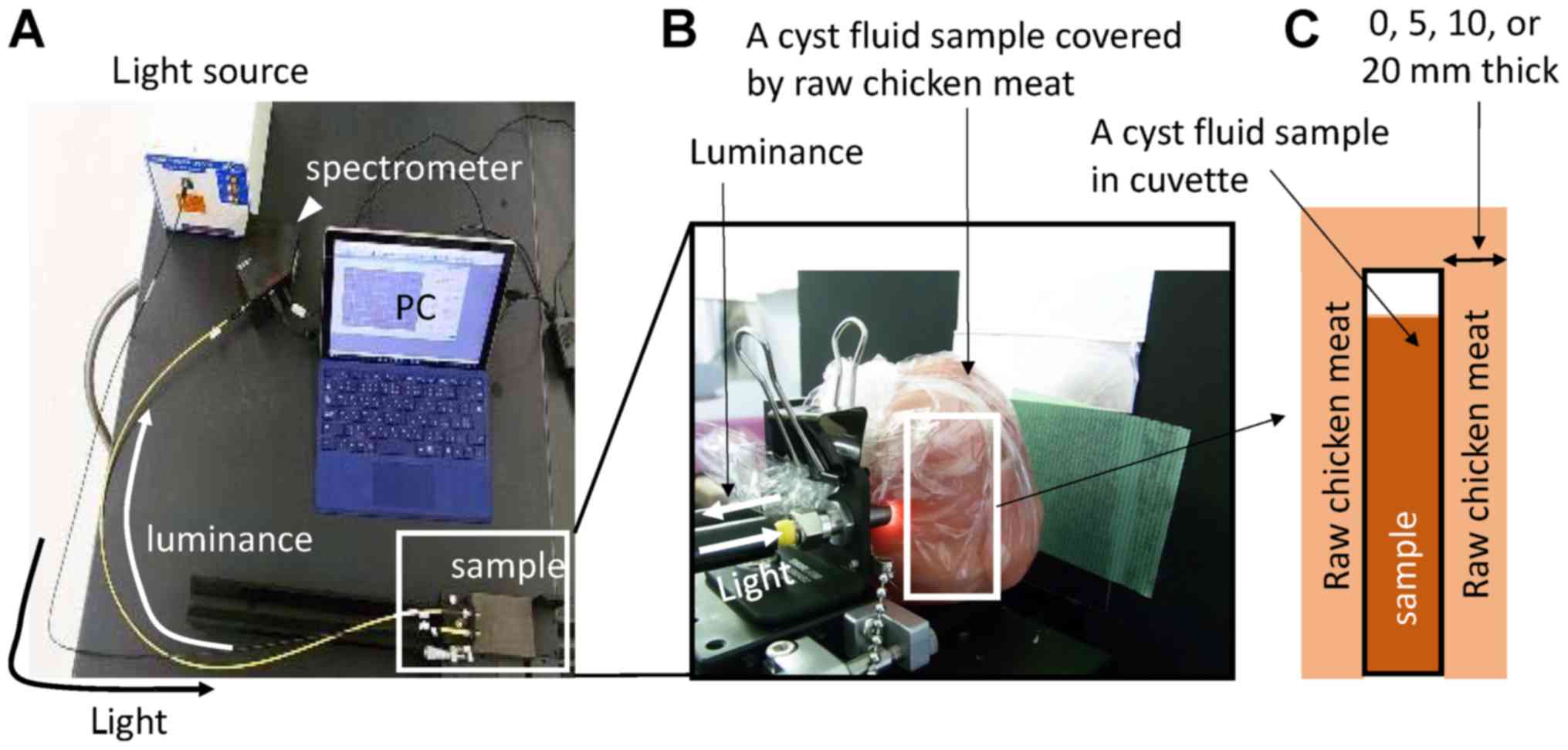
concentrations. This study provided the design, characterization,
performance, and preclinical validation of a broadband
near-infrared spectroscopic system for determining total iron
concentration of a biological sample. The system is composed of
five functional modules: the light stimulator, measuring
instrument, photoelectric detection, the image acquisition module,
and the image signal processing (Fig.
4A). They used cyst fluid samples obtained from surgery in an
ex vivo setting. An aliquot of cyst fluid sample was
transferred to a disposable cuvette. To estimate sufficient barrier
penetration, the prepared cuvette was covered with a commercially
available chicken with a different thickness (0, 5, 10 and 20 mm)
(Fig. 4B and C) (16). This model mimics the anatomical
structure, including vaginal wall layer and tumor surface layer.
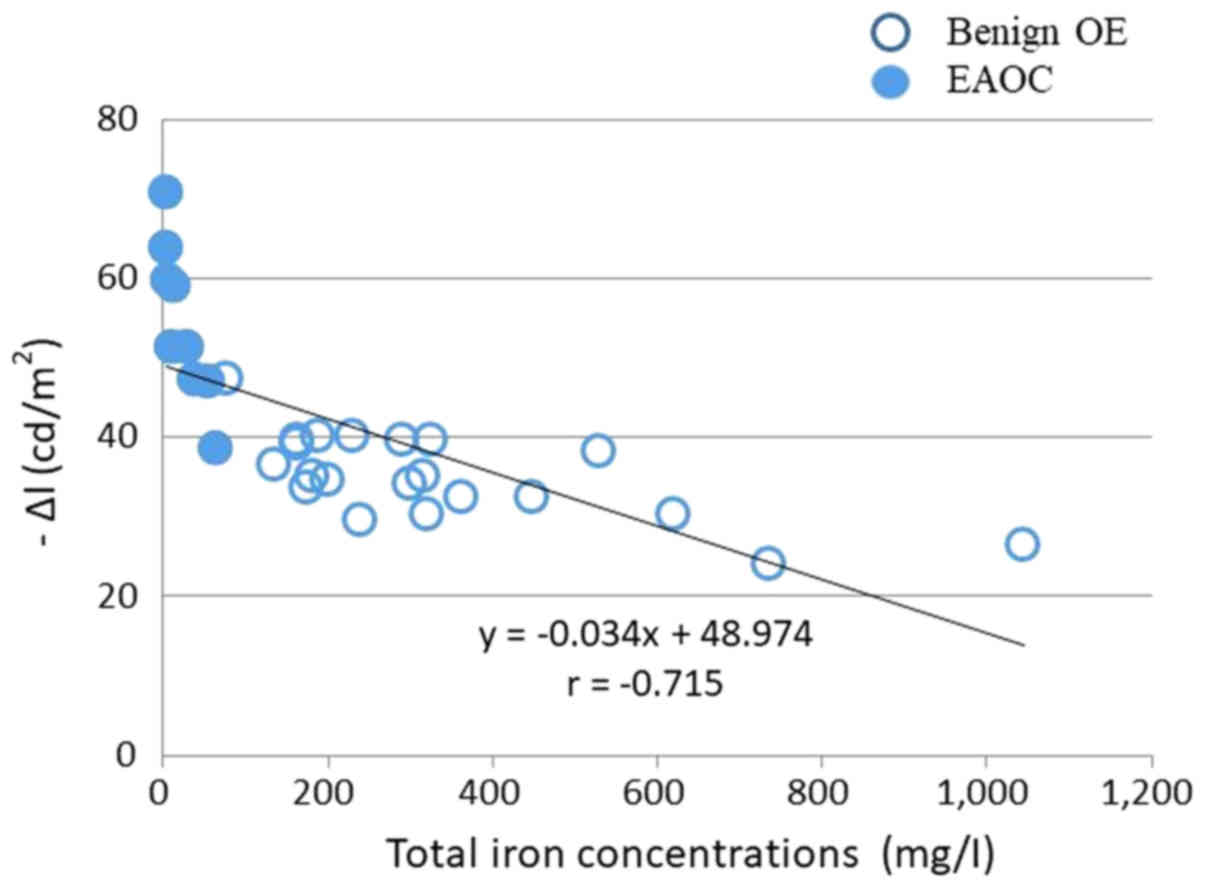
The light reflected from each cyst fluid sample [change in
luminance, -Δl (cd/m2)] was spectrally measured by a CCD
camera with a band-path filter (800 nm) via the optical
spectroscopic imaging apparatus. The imaging results, -Δl, for the
ex-vivo specimens obtained with a near-infrared spectroscopy
were compared to the results of total iron concentrations. The
study uncovered that the change in luminance (− Δl,
cd/m2) of cystic fluid from the EAOC group was
significantly higher compared with that of the OE group (Fig. 5). The-Δl level exhibits significant
negative correlation with total iron concentration and could serve
as a simple, rapid and accurate method to discriminate EAOC from
benign OE, with high sensitivity (85%) and specificity (95%)
(16). A 800 nm near infrared light
reached the depth of 2 cm and delivered approximately 5% of the
surface power density. This ex-vivo study provided a
powerful near-infrared approach for quantitative discrimination of
benign and malignant cyst fluids. Recent advances in the field of
metallobiology would highlight the potential for future clinical
application of near infrared approach.
At present, the cystic mass with mural nodules was
virtually always surgically removed to exclude malignancy, which
can lead to over-diagnosis and over-treatment. On the other hand,
pre-malignant lesions without a mural nodule may pose a diagnostic
challenge on routine ultrasonography. We believe that noninvasive
near-infrared spectroscopy monitoring can help to identify women
who should undergo surgery before the appearance of malignant
morphological features in outpatient settings. More studies are
needed for better characterization of its diagnostic value and
potential for clinical application.
Identification of cyst fluid
hemoglobin species by MR transverse relaxometry
There has been increasing interest in noninvasive
assessment of tissue iron overload (17). For example, liver and heart iron
content was reliably quantified by measurement of the transverse
magnetic relaxation rate R2 or R2* value using complex chemical
shift-encoded MR examination (18).
Yoshimoto et al (9),
hypothesized that the MR transverse relaxometry technique would be
applied to detect the change of total iron concentration in
endometriotic cyst fluid. This idea came from the prior studies
showing a positive correlation between tissue iron levels and MR
transverse relaxometry (17–20). They evaluated for the first time the
correlation between MR transverse relaxometry and the cyst fluid
total iron, heme iron and free iron levels in patients with OE and
its malignant tumor to assess whether this method can predict EAOC
from benign OE (9). Fig. 6 represent conventional MR images (A-D)
and MR transverse relaxometry images (E and F) created from the
quantitative scan. The preliminary in vivo R2 value was
8-fold lower in EAOC than in benign OE (G and H) (9). They draw attention to MR transverse
relaxometry as important for the diagnosis of malignant
transformation. In a prospective study at a single tertiary
institution, Yoshimoto et al (9), determined and analyzed the R2 values by
MR transverse relaxometry. Consequently, the in vivo R2
values in the EAOC group (n=12) were significantly lower than those
in the benign OE group (n=34) (benign OE, 24.4±9.8 vs. EAOC,
8.7±4.5, P<0.05) (9). In the EAOC
group, the in vivo R2 values decreased 2.7-fold compared to
the benign OE group. The optimal predictive cutoff value was 12.1,
giving a sensitivity and specificity of 86 and 94%, respectively.
Taken together, the presented MR relaxometry might be a noninvasive
preoperative prediction tool and showed a favorable predictive
accuracy for the malignant transformation, but the implementation
of MR imaging in the outpatient clinic is occasionally difficult.
Further clinical study and multicenter validation are needed to
establish a non-invasive tool for early diagnosis and acquire
high-level evidence for its clinical application.
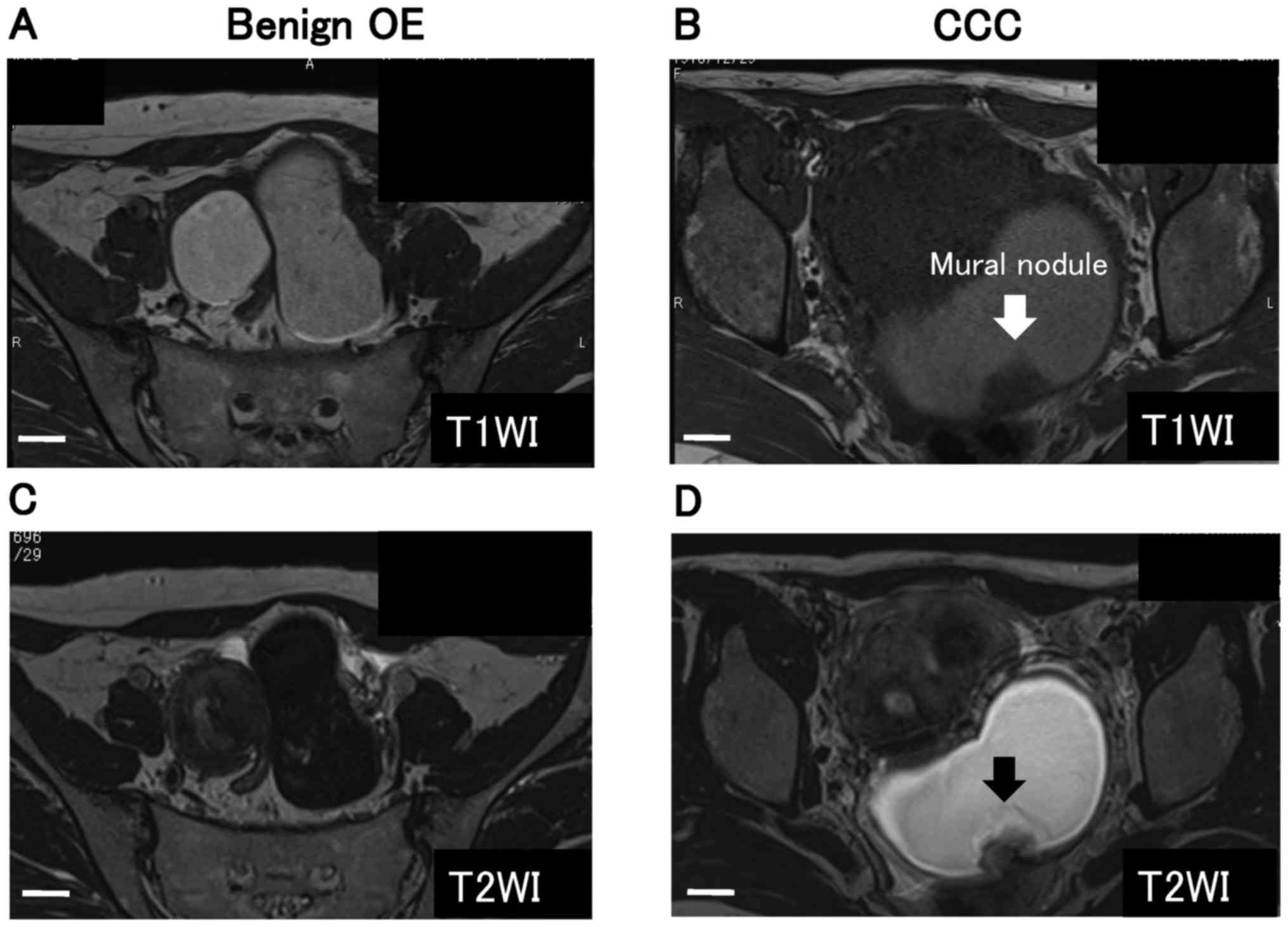 | Figure 6.A direct comparison between
conventional MR images and MR transverse relaxometry images. MR
images represent an benign ovarian endometrioma in a 36-year-old
woman (A, C, E and G) and a CCC in a 59-year-old woman (B, D, F and
H). Axial T1WI (A) and T2WI (C) show a large, bilateral and
unilocular well-defined endometriotic cystic mass. Axial T1WI (B)
and T2WI (D) show a large, unilateral and unilocular well-defined
malignant cystic mass with an irregular mural nodule. E and F are
examples of MR transverse relaxometry in patients with benign OE
and EAOC, respectively. A radiologist drew regions of interest
(ROI, voxel) for the analysis. Images are subsequently processed to
estimate the R2 relaxation rate at each voxel. In this technique,
several spin-echo images are acquired with increasing echo times
(ms). MR transverse relaxometry data is plotted regarding R2 as a
function of the time. The bottom G and H show in vivo R2
relaxation time: The patient with benign OE (G, R2=40.51) and the
patient with EAOC (H, R2=4.90). Scale bar, 1 cm. CCC, clear cell
carcinoma; T1WI, T1-weighted imaging; T2WI, T2-weighted imaging;
ROI, region of interest; OE, ovarian endometrial. |
Discussion
The purpose of this review is to discuss the current
and future available methods for diagnosis of malignant
transformation of endometriosis. Noninvasive tests and candidate
biomarkers of early detection of the malignant transformation are
essential for disease monitoring and accurate diagnosis. Malignant
cystic tumors, including EAOC, may be associated with worrisome
features (e.g., mural nodule of various types and thick septa) on
ultrasonography, CT and MR images. The presence of mural nodules is
a potentially suitable marker for differentiating EAOC from benign
OE, and is important for making decisions about surgical
interventions. Cases of EAOC without mural nodules are very rare,
because malignant transformation in its early stage usually remains
undetected by conventional imaging modalities such as ultrasound,
CT and MRI.
Currently available serum-based tests, including
CA125, have been disappointing (4).
Arakawa et al (21), reported
that serum Tissue Factor Pathway Inhibitor-2 (TFPI2) levels were
elevated only in patients with CCC among epithelial ovarian cancer.
The preliminary study demonstrated that patients with endometriosis
presented mild-to-moderate elevation of serum CA125 levels, but may
be characterized by normal serum levels of TFPI2 (21). This study suggests that TFPI2 may be
useful for discriminating CCC from benign OE. Further investigation
of TFPI2 as the serum biomarker is encouraged.
Advances in understanding the pathogenesis of
endometriosis malignancy, based on biological and biochemical
concepts, have brought about new approaches in EAOC diagnosis and
management. The levels of the Hb and iron-related compounds in the
cyst fluid samples significantly changed between the benign OE and
EAOC. We present a review of various noninvasive techniques being
currently utilized in preclinical studies or being developed for
future applications (7,8). Imaging modalities discussed include
electronic absorption spectroscopy, near infrared approach and MR
transverse relaxometry. The diagnosis of EAOC might be more
accurately achieved in combination of the conventional imaging
methods and the use of novel noninvasive methods: i) Combination of
transvaginal ultrasonography and near infrared approach and ii)
combination of MRI and MR transverse relaxometry. A new device,
consisting of transvaginal ultrasound-guided near infrared system
(composite-type optical ultrasonography), will be developed to
noninvasively measure the cyst fluid Hb levels that could be an
important instrument for clinical use in an office setting.
Long-term goal is to explore the clinical value of composite-type
near infrared-based optical system in diagnosis of the malignant
transformation of endometriosis. Considering conveniency for
medical doctors, it is useful to use composite-type optical
ultrasonography when they identify the morphological changes in
benign OE. Such a device will make the early diagnosis more
accurate. Noninvasive tests may allow for consideration of
avoidance of diagnostic surgery and help to identify women who
should undergo surgery before the appearance of malignant
morphological features in outpatient settings.
The article will highlight recent efforts in
multimodal imagings, including electronic absorption spectroscopy,
near infrared metallobiology approach and MR transverse
relaxometry, and discuss to provide an outlook on future research
directions. To better understand the implications of pathogenesis,
we require various techniques including clinical, morphological,
and molecular assessments. In addition to standard anatomic MRI, MR
relaxometry is a noninvasive imaging technique that can assess the
iron concentration at the molecular level. In the near future, a
comprehensive MRI study would provide quantification of not only
iron, but also oxyhemoglobin and methemoglobin contents. In fact,
the study by Iwabuchi et al (11), showed that electronic absorption
spectroscopy can assess the relative concentrations of hemoglobin
species. Therefore, there is increasing interest in the role of MR
relaxometry for diagnosis of malignant transformation of
endometriosis. To say the least, combining MR relaxometry with MRI
may help in assessing the early diagnosis of malignant
transformation. This may allow MR relaxometry to go beyond the
current role of MRI.
In conclusion, special emphasis is given to recent
advances in the imaging modalities for the noninvasive diagnosis of
malignant transformation of endometriosis.
Acknowledgements
Not applicable.
Funding
The present study was supported by JSPS KAKENHI
(grant no. JP16K11150) and Tohoku Bureau of Economy, Trade and
Industry (Tohoku grant no. 1607028).
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors' contributions
YY, NK and KO collected data regarding the
epigenetic and genetic abnormalities, and underlying mechanism of
endometriosis transformation using the PubMed database. NK, KO and
CY performed the literature search and supervised the study. HK and
CY made substantial contributions to the conception of the study.
HK contributed to the study design and interpretation of included
research studies. All authors read and approved the final version
of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kobayashi H, Sumimoto K, Kitanaka T,
Yamada Y, Sado T, Sakata M, Yoshida S, Kawaguchi R, Kanayama S,
Shigetomi H, et al: Ovarian endometrioma-risks factors of ovarian
cancer development. Eur J Obstet Gynecol Reprod Biol. 138:187–193.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Brinton LA, Sakoda LC, Sherman ME,
Frederiksen K, Kjaer SK, Graubard BI, Olsen JH and Mellemkjaer L:
Relationship of benign gynecologic diseases to subsequent risk of
ovarian and uterine tumors. Cancer Epidemiol Biomarkers Prev.
14:2929–2935. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nicklin J, Janda M, Gebski V, Jobling T,
Land R, Manolitsas T, McCartney A, Nascimento M, Perrin L, Baker
JF, et al: The utility of serum CA-125 in predicting extra-uterine
disease in apparent early-stage endometrial cancer. Int J Cancer.
131:885–890. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Taniguchi F, Harada T, Kobayashi H,
Hayashi K, Momoeda M and Terakawa N: Clinical characteristics of
patients in Japan with ovarian cancer presumably arising from
ovarian endometrioma. Gynecol Obstet Invest. 77:104–110. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tanase Y, Kawaguchi R, Takahama J and
Kobayashi H: Factors that differentiate between
endometriosis-associated ovarian cancer and benign ovarian
endometriosis with mural nodules. Magn Reson Med Sci. 17:231–237.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhou Y and Hua KQ: Ovarian endometriosis:
Risk factor analysis and prediction of malignant transformation.
Prz Menopauzalny. 17:43–48. 2018.PubMed/NCBI
|
|
7
|
Yoshimoto C, Iwabuchi T, Shigetomi H and
Kobayashi H: Cyst fluid iron-related compounds as useful markers to
distinguish malignant transformation from benign endometriotic
cysts. Cancer Biomark. 15:493–439. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yamaguchi K, Mandai M, Toyokuni S,
Hamanishi J, Higuchi T, Takakura K and Fujii S: Contents of
endometriotic cysts, especially the high concentration of free
iron, are a possible cause of carcinogenesis in the cysts through
the iron-induced persistent oxidative stress. Clin Cancer Res.
14:32–40. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yoshimoto C, Takahama J, Iwabuchi T,
Uchikoshi M, Shigetomi H and Kobayashi H: Transverse relaxation
rate of cyst fluid can predict malignant transformation of ovarian
endometriosis. Magn Reson Med Sci. 16:137–145. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nagai M, Mizusawa N, Kitagawa T and
Nagatomo S: A role of heme side-chains of human hemoglobin in its
function revealed by circular dichroism and resonance Raman
spectroscopy. Biophys Rev. 10:271–284. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Iwabuchi T, Yoshimoto C, Shigetomi H and
Kobayashi H: Cyst fluid hemoglobin species in endometriosis and its
malignant transformation: The role of metallobiology. Oncol Lett.
11:3384–3388. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Oh JY, Hamm J, Xu X, Genschmer K, Zhong M,
Lebensburger J, Marques MB, Kerby JD, Pittet JF, Gaggar A and Patel
RP: Absorbance and redox based approaches for measuring free heme
and free hemoglobin in biological matrices. Redox Biol. 9:167–177.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Colquhoun DA, Forkin KT, Durieux ME and
Thiele RH: Ability of the Masimo pulse CO-Oximeter to detect
changes in hemoglobin. J Clin Monit Comput. 26:69–73. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lopes-Coelho F, Gouveia-Fernandes S,
Gonçalves LG, Nunes C, Faustino I, Silva F, Félix A, Pereira SA and
Serpa J: HNF1β drives glutathione (GSH) synthesis underlying
intrinsic carboplatin resistance of ovarian clear cell carcinoma
(OCCC). Tumour Biol. 37:4813–4829. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Harris IS, Treloar AE, Inoue S, Sasaki M,
Gorrini C, Lee KC, Yung KY, Brenner D, Knobbe-Thomsen CB, Cox MA,
et al: Glutathione and thioredoxin antioxidant pathways synergize
to drive cancer initiation and progression. Cancer Cell.
27:211–222. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kawahara N, Yamada Y, Ito F, Hojo W,
Iwabuchi T and Kobayashi H: Discrimination of malignant
transformation from benign endometriosis using a near-infrared
approach. Exp Ther Med. 15:3000–3005. 2018.PubMed/NCBI
|
|
17
|
Fischer R and Harmatz PR: Non-invasive
assessment of tissue iron overload. Hematology Am Soc Hematol Educ
Program. 215–221. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wood JC, Enriquez C, Ghugre N, Tyzka JM,
Carson S, Nelson MD and Coates TD: MRI R2 and R2* mapping
accurately estimates hepatic iron concentration in
transfusion-dependent thalassemia and sickle cell disease patients.
Blood. 106:1460–1465. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Argyropoulou MI and Astrakas L: MRI
evaluation of tissue iron burden in patients with beta-thalassaemia
major. Pediatr Radiol. 37:1191–1200. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Verlhac S, Morel M, Bernaudin F, Béchet S,
Jung C and Vasile M: Liver iron overload assessment by MRI R2*
relaxometry in highly transfused pediatric patients: An agreement
and reproducibility study. Diagn Interv Imaging. 96:259–264. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Arakawa N, Kobayashi H, Yonemoto N,
Masuishi Y, Ino Y, Shigetomi H, Furukawa N, Ohtake N, Miyagi Y,
Hirahara F, et al: Clinical Significance of tissue factor pathway
inhibitor 2, a serum biomarker candidate for ovarian clear cell
carcinoma. PLoS One. 11:e01656092016. View Article : Google Scholar : PubMed/NCBI
|