Lung cancer remains the leading cause of
cancer-related death worldwide. During the last decade, the
treatment paradigm for non-small cell lung cancer (NSCLC) has been
significantly changed by targeted tyrosine kinase inhibitors (TKIs)
based on molecular features (1).
However, the limited response prevents patients from receiving the
benefits of the targeted therapy. For example, in the case of EGFR,
most patients gain resistance to gefitinib and erlotinib within a
median period of 14 months (2).
Overcoming the dilemma of recurrent resistance to TKIs is
challenging. PD-1/PD-L1 inhibitors are gaining attention for the
treatment of NSCLC. Published clinical data have shown that immune
checkpoint inhibitors (ICIs) exhibit little antitumor efficacy in
NSCLC with oncogene mutations (3,4).
Accumulating evidence has demonstrated that the response rate of
ICI is closely associated with the immune microenvironment
(5). Changes in the tumor immune
microenvironment during TKI treatment remain unclear. Therefore, a
better understanding of the tumor microenvironment (TME) during
targeted treatment is required to provide clues for functional
treatment strategies (6,7).
The present review summarizes the last 10 years of
research into the immune alterations occurring before and after
resistance to targeted therapy in NSCLC. Furthermore, the present
review summarizes how different components of the TME contribute to
TKI resistance as well as to the disease relapse and discusses
combination strategies to achieve long-lasting responses in
patients with NSCLC.
Numerous immune cells coexist in the TME, including
T and B lymphocytes, macrophages, polymorphonuclear cells, mast
cells, natural killer cells, dendritic cells and myeloid-derived
suppressor cells (MDSCs). These cell clusters can infiltrate into
the TME and alter it after targeted therapy (6).
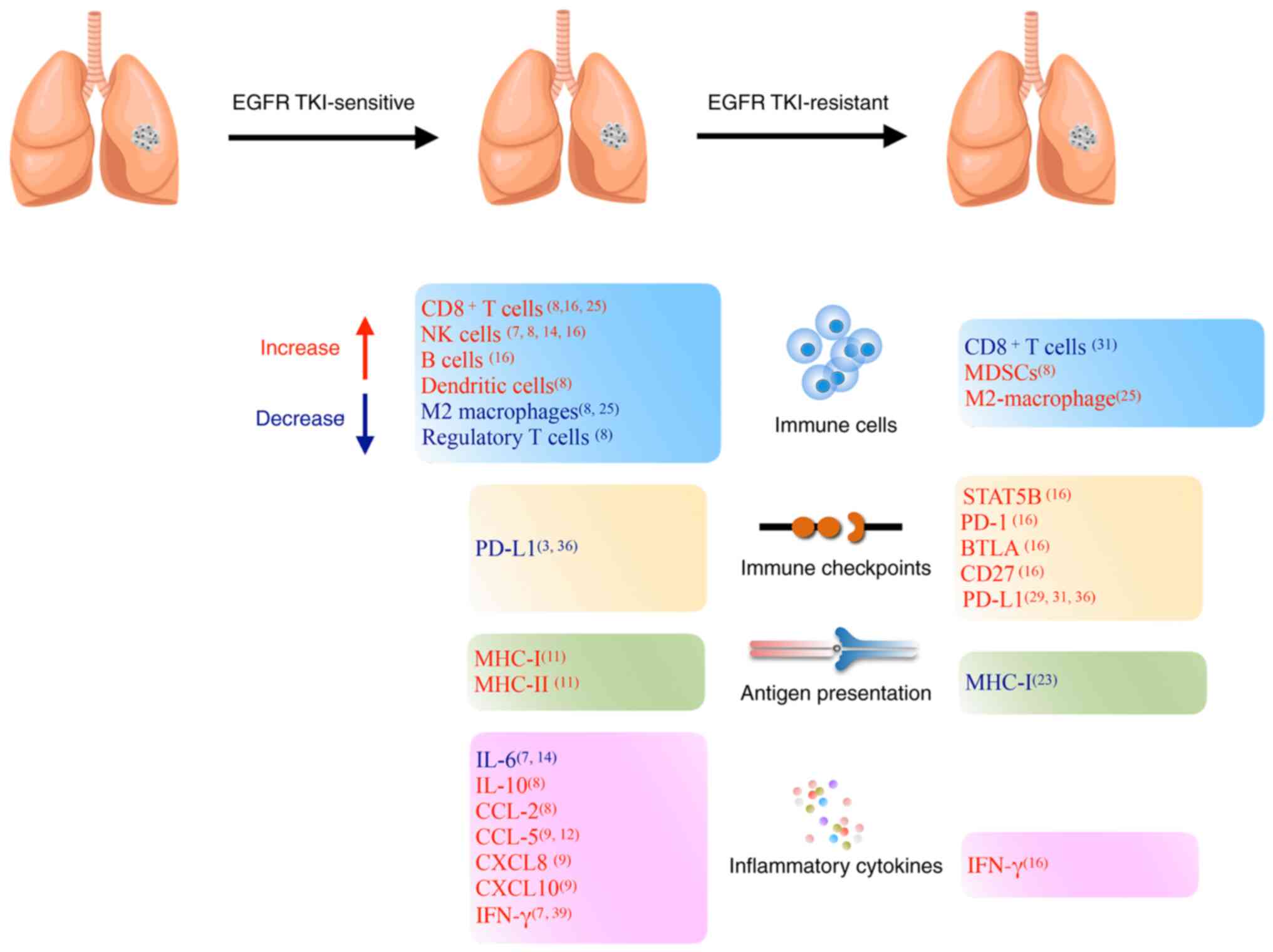
In mouse models with sensitive EGFR mutations,
erlotinib increases the infiltration of T lymphocytes and natural
killer cells other than B cells. Dendritic cells and macrophages
with increased MHC class II expression may enhance
antigen-presenting activity. The levels of immune checkpoints in
the TME were reduced (13).
Several EGFR downstream signaling pathways [IL-6/Janus kinase
(JAK)/STAT3, NF-κB, and phospho-ERK1/2/phospho-c-Jun] regulate
PD-L1 expression in tumor cells (3,7). An
NSCLC specimen study illustrated that PD-L1 expression was
downregulated after 4 weeks of gefitinib treatment (14). EGFR TKI treatment led to a decrease
in PD-1, cytotoxic T lymphocyte-associated antigen 4 and T cell
immunoglobulin and mucin domain-containing protein 3 expression in
T cells in mouse models (8). EGFR
TKIs and anti-PD-1 antibody combination treatment produced no
synergistic antitumor effect in an in vitro co-culture
system (3). Reduced expression of
immune checkpoints within the TME may explain these clinical
observations (15).
ALK inhibitors have been reported to increase
T-lymphocyte infiltration. Recently, whole-exome and RNA sequencing
indicated that immune-related genes were altered in response to ALK
TKI treatment. Antigen presentation genes, IFN-γ signaling genes,
inhibitory checkpoint genes, and stimulatory checkpoint genes
increased apparently after response to ALK TKIs (Table I) (16).
In conclusion, short-term exposure to TKIs not only
eliminates tumor cells, but also modulates immune-mediated
cytotoxicity in the TME during the initial response period. One
study provided a rationale for the potential combination of
erlotinib and immunotherapies for the treatment of lung carcinomas
in first-line treatment (17).
However, other pre-clinical studies confirmed that synergistic
effects of EGFR-TKIs combined with anti-PD-1 antibody were not
present in an in vitro co-culture system (3). According to the latest edition of the
National Comprehensive Cancer Network guidelines for NSCLC
(18), PD-1/PD-L1 inhibitor may
not be recommended for EGFR+/ALK+ NSCLC due
to the negative results generated in a retrospective study
(19). Therefore, TKI monotherapy
is preferred for oncogene-driven NSCLC in the first-line
treatment.
After the long-term use of TKIs, the positive
therapeutic response is reversed, especially when resistance
emerges. Under the selective pressure of targeted therapy, certain
tumor cells evade the host immunity through a variety of intrinsic
mechanisms. Multiple signaling pathways and related molecules
comprise the complexity of the TME. In summary, a wide range of
immunosuppressive mechanisms may evolve the acquired resistance to
TKIs (20,21).
A decrease in cytotoxic T cell populations was
observed in EGFR inhibitor-resistant lung adenocarcinoma when
compared with that in the initial biopsy from an identical patient
(22). Some resistant tumors are
deficient for MHC class I as a result of decreased mRNA levels and
related genes (23). Thus,
targeted treatment may influence different aspects of tumor antigen
presentation and T-cell effector function. Mitogen-activated
protein kinase is the most common compensatory signaling pathway
responsible for the development of acquired resistance (24). In the examination of tumor
biopsies, cytotoxic T cells are found to decrease after TKI
resistance and T-cell infiltration. Tregs are the main component of
the TME. Conversely, the number of macrophages, especially those
expressing indoleamine 2,3-dioxygenase 1 (IDO1), increase with
disease progression (25).
MDSCs are immature myeloid cells that mainly inhibit
T-cell activation; they help create a favorable environment for
tumor survival. In an in vivo study an increased percentage
of MDSCs was detected during long-term use of EGFR-TKI in mouse
models (8,26). Recruitment and expansion of MDSCs
were detected in the serum of patients with NSCLC who achieved EGFR
TKI resistance, compared with the baseline (27). In the TME, MDSCs impair host
antitumor immunity and the effect of immunotherapy (28).
PD-L1 expression levels in tumor cells were found to
notably increase after gefitinib treatment in a subset of patients
(29). PD-L1 is a well-known
immune checkpoint gene, and knockout of PD-L1 helps to restore the
function of human cytotoxic T lymphocytes (30,31).
The histological transformation of the tumor and metastasis sites
affects the PD-L1 expression levels after resistance (32). In one study, paired analysis
indicated that tumors with TPS ≥50% increased from 14 to 28% after
acquired resistance, especially obvious in the EGFR T790M-negative
tumor (31). High expression
levels of PD-L1 have been reported to be a negative prognostic
marker (33) and although lung
cancer cells develop resistance to EGFR TKIs, EGFR phosphorylation
is still suppressed in the resistant cells. However, the downstream
ERK signaling is reactivated upon drug resistance, leading to PD-L1
restoration (34,35). Several studies have revealed that
PD-L1 is a downstream target of the EGFR pathway, which is
interceded via the IL-6/JAK/STAT3, NF-κB, and
phospho-ERK1/2/phospho-c-Jun pathways (3,36–38).
Single-cell RNA sequencing of biopsy samples showed that
immunosuppressive genes, such as IDO1, kynureninase and quinolinate
phosphoribosyltransferase levels were elevated in TKI-resistant
tumors compared with those in naïve tumors (25). Dynamic changes are shown in
Figure 1.
Limited data have been reported on the impact of ALK
inhibitors on the TME after resistance in ALK-positive NSCLC. A
preclinical study explored the changes in the tumor immune
microenvironment in mouse models. The results indicated that
ALK-positive NSCLC was as an immune ‘desert’ before the initiation
of targeted therapy (39). After
resistance to ceritinib the immunogenic features of TME changed,
including increased PD-L1 expression levels, increased number of
functionally impaired CD8+ T cells, antigen-presenting
cells, Tregs and MDSCs, and increased IFN-γ secretion. RNA
sequencing analysis revealed increased transcription of
IFN-γ-related genes, Treg-related genes and immune suppressive
macrophage-related genes. However, whole-exome sequencing revealed
no obvious difference in tumor mutation burden and T cell receptor
clonality between untreated and resistant ALK-positive tumors
(39). Thus, due to the lack of
immunogenicity and impaired antitumor immunity, ICIs are expected
to be less effective in ALK-TKI-resistant tumors.
In conclusion, along with the emergence of acquired
resistance, the TME begins to gain immunosuppressive features, such
as the presence of inhibitory ligands, restoration of the MDSCs and
Tregs, impaired functions of tumor-infiltrating lymphocytes,
decreased antigen presentation, increased level of IFN-γ and
increased immune checkpoint molecules (Table I) (8). Subsequently, immune evasion and
T-cell exhaustion lead to disease progression (40). The potential mechanisms that are
involved in these changes include: i) The reactivation of EGFR
downstream signaling pathways; ii) the secretion of tumor-related
exosomes by EGFR-mutated cells; and iii) the induction of MHC
expression. The change in the TME indicates the possibility of
initiating combination strategies in resistant patients.
At present, ICIs have achieved great success in the
treatment area of lung cancer and are considered ideal for
combination treatment. According to preclinical data, combination
of EGFR-TKIs with ICIs showed promising antitumor effect in a mouse
model (41–43). Two retrospective studies suggested
that nivolumab had a favorable response rate in NSCLC, especially
in EGFR T790M-negative disease (44).
In first-line treatment, a phase Ib study
investigated the safety and efficacy of durvalumab in combination
with gefitinib. However, this study was halted due to liver
dysfunction. The objective response rate was 77.8% (45). The KEYNOTE-021 study evaluated the
safety of the combination of erlotinib or gefitinib and
pembrolizumab. Compared with erlotinib, pembrolizumab plus
gefitinib increased the incidence of toxicity and resulted in
treatment discontinuation. The overall objective response rate was
41.7% (46).
In second-line treatment, the response rate of
combination therapy between nivolumab and erlotinib was 15% and the
response lasted as long as 38.2 months. A total of 20% of the
participants experienced grade three toxicities (47). Long-term analysis of a phase Ib
study of erlotinib plus atezolizumab showed tolerable adverse
effects of combination therapy, with a median overall survival time
of 32.7 months (48). In the
TATTON trial, the objective response rate was 42% in the
osimertinib and durvalumab group. The most common adverse events
were arm rash, vomiting and diarrhea (49). Another phase III trial, CAURAL,
reported that 64% (9/14) of participants responded to osimertinib
and durvalumab. The main toxicity presented as a rash (50). Unfortunately, the TATTON and CAURAL
trials were terminated by AstraZeneca owing to the increased
incidence of interstitial lung disease (51). Related data were collected from the
FAERS database, where 70 patients with NSCLC were treated with
EGFR-TKI plus nivolumab, and the incidence of interstitial
pneumonitis was 25.7% (52).
Due to the lack of immunogenicity, preclinical and
clinical data have indicated that PD-1/PD-L1 inhibitors combined
with ALK inhibitors are not superior to ALK inhibitors alone, and
the incidence of drug-related hepatotoxicity has increased
(39,53). However, carefully selected drugs
for combination therapy, such as avelumab plus lorlatinib, could
produce antitumor activity with an acceptable safety profile
(54).
Recent studies have shown that the response rate to
PD-1/PD-L1 inhibitors is closely associated with PD-L1 expression
levels, tumor-infiltrating lymphocytes, gut microbiota, and the
levels of IFN-γ, TGF-β, VEGF-A, IL-6, IL-10 and other biomarkers
(8,55). In TKI-resistant patients with
favorable immune features, there should be more confidence in
attempting combined therapy with ICIs and TKIs.
It is known that the host immunity undergoes dynamic
changes following TKI treatment. During the response period,
cytotoxic immune cells accumulate in the TME and contribute to the
formation of an inflammatory TME. Once the acquired resistance
develops, immunosuppressive cells as well as immune checkpoints
begin to increase and function in the TME, which is a critical
mechanism for tumor progression. Although the response rate of ICIs
shows negative results in advanced oncogene-driven NSCLC at
frontline treatment, the combination of targeted therapy and
immunotherapy remains a feasible strategy to achieve synergistic
effects in selected resistant patients. Combination treatment has
been explored in multiple studies, and preliminary data have shown
both positive and negative results. Thus, extensive exploration is
still needed to confirm the selection criteria of patient subgroups
and the toxicity profiles of EGFR-TKIs plus ICIs. At present,
reagents targeting MDSCs, Tregs, IL-8, TGF-β and related pathways
remain underexplored as compared with the revolutionary effect of
ICIs in lung cancer. In the future, the precisely selected regimens
for combination therapy should be further investigated in carefully
designed xenograft models and clinical trials.
Not applicable.
Funding: No funding was received.
Not applicable.
LJ performed the literature search and drafted the
manuscript. JYL conceived the review and revised the manuscript.
Both authors have read and approved the manuscript. Data sharing is
not applicable.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Cappuzzo F: Therapy options for advanced
NSCLC. In: Guide to Targeted Therapies: Treatment Resistance in
Lung Cancer. Springer International Publishing; Cham: pp. 5–25.
2015
|
|
2
|
Rosell R, Moran T, Queralt C, Porta R,
Cardenal F, Camps C, Majem M, Lopez-Vivanco G, Isla D, Provencio M,
et al: Screening for epidermal growth factor receptor mutations in
lung cancer. N Engl J Med. 361:958–967. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen N, Fang W, Zhan J, Hong S, Tang Y,
Kang S, Zhang Y, He X, Zhou T, Qin T, et al: Upregulation of PD-L1
by EGFR activation mediates the immune escape in EGFR-driven NSCLC:
Implication for optional immune targeted therapy for NSCLC patients
with EGFR mutation. J Thorac Oncol. 10:910–923. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lisberg A, Cummings A, Goldman JW,
Bornazyan K, Reese N, Wang T, Coluzzi P, Ledezma B, Mendenhall M,
Hunt J, et al: A phase II study of pembrolizumab in EGFR-mutant,
PD-L1+, tyrosine kinase inhibitor naive patients with advanced
NSCLC. J Thorac Oncol. 13:1138–1145. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kumagai S, Togashi Y, Kamada T, Sugiyama
E, Nishinakamura H, Takeuchi Y, Vitaly K, Itahashi K, Maeda Y,
Matsui S, et al: The PD-1 expression balance between effector and
regulatory T cells predicts the clinical efficacy of PD-1 blockade
therapies. Nat Immunol. 21:1346–1358. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dong ZY, Zhang JT, Liu SY, Su J, Zhang C,
Xie Z, Zhou Q, Tu HY, Xu CR, Yan LX, et al: EGFR mutation
correlates with uninflamed phenotype and weak immunogenicity,
causing impaired response to PD-1 blockade in non-small cell lung
cancer. Oncoimmunology. 6:e13561452017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Soo RA, Lim SM, Syn NL, Teng R, Soong R,
Mok TSK and Cho BC: Immune checkpoint inhibitors in epidermal
growth factor receptor mutant non-small cell lung cancer: Current
controversies and future directions. Lung Cancer. 115:12–20. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jia Y, Li X, Jiang T, Zhao S, Zhao C,
Zhang L, Liu X, Shi J, Qiao M, Luo J, et al: EGFR-targeted therapy
alters the tumor microenvironment in EGFR-driven lung tumors:
Implications for combination therapies. Int J Cancer.
145:1432–1444. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mascia F, Mariani V, Girolomoni G and
Pastore S: Blockade of the EGF receptor induces a deranged
chemokine expression in keratinocytes leading to enhanced skin
inflammation. Am J Pathol. 163:303–312. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kim H, Kim SH, Kim MJ, Kim SJ, Park SJ,
Chung JS, Bae JH and Kang CD: EGFR inhibitors enhanced the
susceptibility to NK cell-mediated lysis of lung cancer cells. J
Immunother. 34:372–381. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Im JS, Herrmann AC, Bernatchez C, Haymaker
C, Molldrem JJ, Hong WK and Perez-Soler R: Immune-modulation by
epidermal growth factor receptor inhibitors: Implication on
Anti-tumor immunity in lung cancer. PLoS One. 11:e01600042016.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Paul T, Schumann C, Rüdiger S, Boeck S,
Heinemann V, Kächele V, Steffens M, Scholl C, Hichert V,
Seufferlein T and Stingl JC: Cytokine regulation by epidermal
growth factor receptor inhibitors and epidermal growth factor
receptor inhibitor associated skin toxicity in cancer patients. Eur
J Cancer. 50:1855–1863. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Venugopalan A, Lee MJ, Niu G,
Medina-Echeverz J, Tomita Y, Lizak MJ, Cultraro CM, Simpson RM,
Chen X, Trepel JB and Guha U: EGFR-targeted therapy results in
dramatic early lung tumor regression accompanied by imaging
response and immune infiltration in EGFR mutant transgenic mouse
models. Oncotarget. 7:54137–54156. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sheng J, Fang W, Liu X, Xing S, Zhan J, Ma
Y, Huang Y, Zhou N, Zhao H and Zhang L: Impact of gefitinib in
early stage treatment on circulating cytokines and lymphocytes for
patients with advanced non-small cell lung cancer. Onco Targets
Ther. 10:1101–1110. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gainor JF, Shaw AT, Sequist LV, Fu X,
Azzoli CG, Piotrowska Z, Huynh TG, Zhao L, Fulton L, Schultz KR, et
al: EGFR mutations and ALK rearrangements are associated with low
response rates to PD-1 pathway blockade in non-small cell lung
cancer: A retrospective analysis. Clin Cancer Res. 22:4585–4593.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fang Y, Wang Y, Zeng D, Zhi S, Shu T,
Huang N, Zheng S, Wu J, Liu Y, Huang G, et al: Comprehensive
analyses reveal TKI-induced remodeling of the tumor immune
microenvironment in EGFR/ALK-positive non-small-cell lung cancer.
OncoImmunology. 10:19510192021. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dominguez C, Tsang KY and Palena C:
Short-term EGFR blockade enhances immune-mediated cytotoxicity of
EGFR mutant lung cancer cells: Rationale for combination therapies.
Cell Death Dis. 7:e23802016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
National Comprehensive Cancer Network
(NCCN), . The NCCN Clinical Practice Guidelines in Oncology,
Non-small Cell Lung Cancer (version 1.2021). NCCN; Plymouth
Meeting, PA: 2021, https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf
|
|
19
|
Mazieres J, Drilon A, Lusque A, Mhanna L,
Cortot AB, Mezquita L, Thai AA, Mascaux C, Couraud S, Veillon R, et
al: Immune checkpoint inhibitors for patients with advanced lung
cancer and oncogenic driver alterations: Results from the
IMMUNOTARGET registry. Ann Oncol. 30:1321–1328. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Junttila MR and de Sauvage FJ: Influence
of tumour micro-environment heterogeneity on therapeutic response.
Nature. 501:346–354. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Klemm F and Joyce JA: Microenvironmental
regulation of therapeutic response in cancer. Trends Cell Biol.
25:198–213. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kawana S, Saito R, Miki Y, Kimura Y, Abe
J, Sato I, Endo M, Sugawara S and Sasano H: Suppression of tumor
immune microenvironment via microRNA-1 after epidermal growth
factor receptor-tyrosine kinase inhibitor resistance acquirement in
lung adenocarcinoma. Cancer Med. 10:718–727. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Garrido G, Rabasa A, Garrido C, López A,
Chao L, García-Lora AM, Garrido F, Fernández LE and Sánchez B:
Preclinical modeling of EGFR-specific antibody resistance:
Oncogenic and immune-associated escape mechanisms. Oncogene.
33:3129–3139. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chapman PB: Mechanisms of resistance to
RAF inhibition in melanomas harboring a BRAF mutation. Am Soc Clin
Oncol Educ Book. doi: 10.1200/EdBook_AM.2013.33.e80.
|
|
25
|
Maynard A, McCoach CE, Rotow JK, Harris L,
Haderk F, Kerr DL, Yu EA, Schenk EL, Tan W, Zee A, et al:
Therapy-induced evolution of human lung cancer revealed by
single-cell RNA sequencing. Cell. 182:1232–1251.e22. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wu X, Tang J, Liu X, Ma Q, Deng Q, Li K,
Zhang B and Wang Y: A38 Gemcitabine improves suppressive immune
microenvironment induced by long-term treatment with EGFR-TKIs:
Implications for combination chemotherapy and immunotherapy. J
Thoracic Oncol. 15 (Suppl):S252020. View Article : Google Scholar
|
|
27
|
Tang J, Liu X, Gong Y, Zhu J, Huang M,
Ding Z, Yu M, Tie Y, Li Q and Wang Y: Epidermal growth factor
receptor tyrosine kinase inhibitors (EGFR-TKIs) impact on immune
microenvironment in non-small cell lung cancer (NSCLC). J Clin
Oncol. 36:e211542018. View Article : Google Scholar
|
|
28
|
Parker KH, Beury DW and Ostrand-Rosenberg
S: Myeloid-derived suppressor cells: Critical cells driving immune
suppression in the tumor microenvironment. Adv Cancer Res.
128:95–139. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Han JJ, Kim DW, Koh J, Keam B, Kim TM,
Jeon YK, Lee SH, Chung DH and Heo DS: Change in PD-L1 expression
after acquiring resistance to gefitinib in EGFR-mutant
non-small-cell lung cancer. Clin Lung Cancer. 17:263–270.e2. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Peng S, Wang R, Zhang X, Ma Y, Zhong L, Li
K, Nishiyama A, Arai S, Yano S and Wang W: EGFR-TKI resistance
promotes immune escape in lung cancer via increased PD-L1
expression. Mol Cancer. 18:1652019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Isomoto K, Haratani K, Hayashi H, Shimizu
S, Tomida S, Niwa T, Yokoyama T, Fukuda Y, Chiba Y, Kato R, et al:
Impact of EGFR-TKI treatment on the tumor immune microenvironment
in EGFR mutation-positive non-small cell lung cancer. Clin Cancer
Res. 26:2037–2046. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Suda K, Murakami I, Yu H, Kim J, Ellison
K, Rivard CJ, Mitsudomi T and Hirsch FR: Heterogeneity in immune
marker expression after acquisition of resistance to EGFR kinase
inhibitors: Analysis of a case with small cell lung cancer
transformation. J Thorac Oncol. 12:1015–1020. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang A, Wang HY, Liu Y, Zhao MC, Zhang HJ,
Lu ZY, Fang YC, Chen XF and Liu GT: The prognostic value of PD-L1
expression for non-small cell lung cancer patients: A
meta-analysis. Eur J Surg Oncol. 41:450–456. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Ercan D, Xu C, Yanagita M, Monast CS,
Pratilas CA, Montero J, Butaney M, Shimamura T, Sholl L, Ivanova
EV, et al: Reactivation of ERK signaling causes resistance to EGFR
kinase inhibitors. Cancer Discov. 2:934–947. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Jiang L, Guo F, Liu X, Li X, Qin Q, Shu P,
Li Y and Wang Y: Continuous targeted kinase inhibitors treatment
induces upregulation of PD-L1 in resistant NSCLC. Sci Rep.
9:37052019. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Akbay EA, Koyama S, Carretero J, Altabef
A, Tchaicha JH, Christensen CL, Mikse OR, Cherniack AD, Beauchamp
EM, Pugh TJ, et al: Activation of the PD-1 pathway contributes to
immune escape in EGFR-driven lung tumors. Cancer Discov.
3:1355–1363. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Zhang N, Zeng Y, Du W, Zhu J, Shen D, Liu
Z and Huang JA: The EGFR pathway is involved in the regulation of
PD-L1 expression via the IL-6/JAK/STAT3 signaling pathway in
EGFR-mutated non-small cell lung cancer. Int J Oncol. 49:1360–1368.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Lin K, Cheng J, Yang T, Li Y and Zhu B:
EGFR-TKI down-regulates PD-L1 in EGFR mutant NSCLC through
inhibiting NF-κB. Biochem Biophys Res Commun. 463:95–101. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Pyo KH, Lim SM, Park CW, Jo HN, Kim JH,
Yun MR, Kim D, Xin CF, Lee W, Gheorghiu B, et al: Comprehensive
analyses of immunodynamics and immunoreactivity in response to
treatment in ALK-positive non-small-cell lung cancer. J Immunother
Cancer. 8:e0009702020. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Philip M and Schietinger A: Beyond
genomics: Multidimensional analysis of cancer therapy resistance.
Trends Immunol. 36:665–667. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sugiyama E, Togashi Y, Takeuchi Y, Shinya
S, Tada Y, Kataoka K, Tane K, Sato E, Ishii G, Goto K, et al:
Blockade of EGFR improves responsiveness to PD-1 blockade in
EGFR-mutated non-small cell lung cancer. Sci Immunol.
5:eaav39372020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Liu Z, Han C, Dong C, Shen A, Hsu E, Ren
Z, Lu C, Liu L, Zhang A, Timmerman C, et al: Hypofractionated EGFR
tyrosine kinase inhibitor limits tumor relapse through triggering
innate and adaptive immunity. Sci Immunol. 4:eaav64732019.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Creelan BC, Yeh TC, Kim SW, Nogami N, Kim
DW, Chow LQM, Kanda S, Taylor R, Tang W, Tang M, et al: A Phase 1
study of gefitinib combined with durvalumab in EGFR TKI-naive
patients with EGFR mutation-positive locally advanced/metastatic
non-small-cell lung cancer. Br J Cancer. 124:383–390. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Haratani K, Hayashi H, Tanaka T, Kaneda H,
Togashi Y, Sakai K, Hayashi K, Tomida S, Chiba Y, Yonesaka K, et
al: Tumor immune microenvironment and nivolumab efficacy in EGFR
mutation-positive non-small-cell lung cancer based on T790M status
after disease progression during EGFR-TKI treatment. Ann Oncol.
28:1532–1539. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Gibbons DL, Chow LQ, Kim DW, Kim SW, Yeh
T, Song X, Jiang H, Taylor R, Karakunnel J and Creelan B: 57O
Efficacy, safety and tolerability of MEDI4736 [durvalumab (D)], a
human IgG1 anti-programmed cell death-ligand-1 (PD-L1) antibody,
combined with gefitinib (G): A phase I expansion in TKI-naïve
patients (pts) with EGFR mutant NSCLC. J Thoracic Oncol. 11
(Suppl):S792016. View Article : Google Scholar
|
|
46
|
Yang JC, Gadgeel SM, Sequist LV, Wu CL,
Papadimitrakopoulou VA, Su WC, Fiore J, Saraf S, Raftopoulos H and
Patnaik A: Pembrolizumab in combination with erlotinib or gefitinib
as first-line therapy for advanced NSCLC with sensitizing EGFR
mutation. J Thorac Oncol. 14:553–559. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Gettinger S, Hellmann MD, Chow LQM,
Borghaei H, Antonia S, Brahmer JR, Goldman JW, Gerber DE, Juergens
RA, Shepherd FA, et al: Nivolumab plus erlotinib in patients with
EGFR-mutant advanced NSCLC. J Thorac Oncol. 13:1363–1372. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Rudin C, Cervantes A, Dowlati A, Besse B,
Ma B, Costa D, Schmid P, Heist R, Villaflor V, Sarkar I, et al:
MA15.02 long-term safety and clinical activity results from a phase
Ib study of erlotinib plus atezolizumab in advanced NSCLC. J
Thoracic Oncol. 13 (Suppl):S4072018. View Article : Google Scholar
|
|
49
|
Oxnard GR, Yang JC, Yu H, Kim SW, Saka H,
Horn L, Goto K, Ohe Y, Mann H, Thress KS, et al: TATTON: A
multi-arm, phase Ib trial of osimertinib combined with selumetinib,
savolitinib, or durvalumab in EGFR-mutant lung cancer. Ann Oncol.
31:507–516. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Yang JC, Shepherd FA, Kim DW, Lee GW, Lee
JS, Chang GC, Lee SS, Wei YF, Lee YG, Laus G, et al: Osimertinib
plus durvalumab versus osimertinib monotherapy in EGFR
T790M-positive NSCLC following previous EGFR TKI therapy: CAURAL
brief report. J Thorac Oncol. 14:933–939. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Gourd K: AstraZeneca halts two lung cancer
drug trials. Lancet Respir Med. 3:9262015. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Oshima Y, Tanimoto T, Yuji K and Tojo A:
EGFR-TKI-associated interstitial pneumonitis in nivolumab-treated
patients with non-small cell lung cancer. JAMA Oncol. 4:1112–1115.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Patel SP, Pakkala S, Pennell NA, Reckamp
KL, Lanzalone S, Polli A, Tarazi J and Robert-Vizcarrondo F: Phase
Ib study of crizotinib plus pembrolizumab in patients with
previously untreated advanced non-small cell lung cancer with ALK
translocation. Oncologist. 25:562–e1012. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Shaw AT, Felip E, Bauer TM, Besse B,
Navarro A, Postel-Vinay S, Gainor JF, Johnson M, Dietrich J, James
LP, et al: Lorlatinib in non-small-cell lung cancer with ALK or
ROS1 rearrangement: An international, multicentre, open-label,
single-arm first-in-man phase 1 trial. Lancet Oncol. 18:1590–1599.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Yi M, Jiao D, Xu H, Liu Q, Zhao W, Han X
and Wu K: Biomarkers for predicting efficacy of PD-1/PD-L1
inhibitors. Mol Cancer. 17:1292018. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Serizawa M, Takahashi T, Yamamoto N and
Koh Y: Combined treatment with erlotinib and a transforming growth
factor-β type I receptor inhibitor effectively suppresses the
enhanced motility of erlotinib-resistant non-small-cell lung cancer
cells. J Thorac Oncol. 8:259–269. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Masuda C, Yanagisawa M, Yorozu K, Kurasawa
M, Furugaki K, Ishikura N, Iwai T, Sugimoto M and Yamamoto K:
Bevacizumab counteracts VEGF-dependent resistance to erlotinib in
an EGFR-mutated NSCLC xenograft model. Int J Oncol. 51:425–434.
2017. View Article : Google Scholar : PubMed/NCBI
|