Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most
common type of non-Hodgkin's lymphoma (NHL), accounting for ~30% of
all cases in Western Countries (1).
DLBCL is a rapidly developing cancer that may metastasize to other
areas of the body. Chemotherapy is the primary treatment for DLBCL,
demonstrating efficacy in ~66% of patients and leading to a
favorable prognosis (2,3). However, some patients may not respond
to these treatments or may experience a relapse following initial
treatment with standardized chemotherapy with rituximab plus
cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP)
(3–5), leading to the development of
relapsed/refractory DLBCL (r/r DLBCL). r/r DLBCL is a complex
condition frequently associated with a poor prognosis (6,7).
Although there are several treatment options available for patients
with r/r DLBCL, such as R-CHOP, epigenetic therapy and targeted
therapy, the therapeutic effects remain unsatisfactory (8).
Sintilimab is an immune checkpoint inhibitor (ICI)
that blocks programmed cell death protein 1 (PD-1) on the surface
of immune cells (9,10). PD-1 is a key checkpoint protein that
prevents the immune system from targeting healthy cells. However,
some tumor cells exploit this mechanism to evade immune
surveillance. Sintilimab aids the immune system in identifying and
attacking tumor cells by blocking PD-1 (9). Sintilimab has been approved in China
for the treatment of multiple cancer types, including classical
Hodgkin's lymphoma, advanced melanoma and non-small cell lung
cancer (10), and is often
administered in combination with other anticancer therapies
(11,12). While sintilimab has demonstrated
therapeutic efficacy against several types of advanced cancer, few
studies have reported its use in the treatment of r/r DLBCL
(13).
The present study describes the case of a patient
with r/r DLBCL who experienced partial remission following
treatment with four different regimens (R-CHOP, GemOx, selinexor
and sintilimab). Based on the detection of CD274
amplification via next-generation sequencing (NGS) and a high Tumor
Proportion Score (TPS) for programmed death-ligand 1 (PD-L1)
expression (95%) with the use of the commercially available PD-L1
IHC 22C3 pharmDx assay (Dako, Agilent Technologies, Inc.) (14), the patient was treated with
sintilimab. The present case study emphasizes the importance of NGS
technology in choosing treatment options for DLBCL. It also
proposes potential treatments for patients with refractory
DLBCL.
Case report
In March 2019, a 60-year-old male patient presented
to the Second Hospital of Dalian Medical University (Dalian, China)
with epigastric pain, without fever, night sweats or weight loss.
The patient had no history of abdominal disease. A computed
tomography (CT)-guided biopsy was performed on lesions present in
the hepatic hilar region. Subsequent pathological examination (Data
S1) indicated NHL (Fig. 1A), which
was specifically identified as DLBCL of non-germinal center origin
(non-GCB). Immunohistochemical (IHC) analysis of the biopsy
demonstrated the following results: CD3(−), Vimentin (partial +;
Fig. 1B), CD5(−), CD10(−), BCL-6
(40% +; Fig. 1C), multiple myeloma
1 (80% +; Fig. 1D), BCL-2 (90% +;
Fig. 1E), C-Myc (80% +; Fig. 1F), p53 (90% strong +; Fig. 1G), CD20 (diffuse strong +; Fig. 1H), CD30(−), CD21(−), Ki-67 (90% +;
Fig. 1I) and PD-L1 (−; Fig. 1J). According to a positron emission
tomography (PET)-CT scan, the tumor had metastasized to multiple
areas of the body, such as the mediastinum, the hilar region of the
liver, the superior and inferior borders of the posterior pancreas,
the retroperitoneum, the left hilum of the liver, the left pelvic
wall, the left parietal iliac vessels and lymph nodes, the spleen
and both lungs (Fig. 2B and C).
Thus, the patient was diagnosed with stage IV DLBCL (not otherwise
specified, non-GCB) with an International Prognosis Index of 3
based on guidelines of Chinese Society of Clinical Oncology (CSCO)
for lymphoid malignancies (Version 2019). The diagnosis and
treatment timeline of the patient is shown in Fig. 2A.
 | Figure 1.H&E and IHC staining of the
lesions in the hepatic hilar region. (A) H&E staining of the
hepatic hilar region (magnification, ×200). IHC staining revealed
that lesions in the hepatic hilar region were positive for (B)
Vimentin (partial), (C) BCL-6 (40%), (D) MUM1 (80%), (E) BCL-2
(90%), (F) C-Myc (80%), (G) p53 (90%), (H) CD20 (diffuse strong)
and (I) Ki-67 (90%), and (J) negative for PD-L1 (scale bar, 100
µm). IHC, immunohistochemical; MUM1, multiple myeloma 1; PD-L1,
programmed death-ligand 1. |
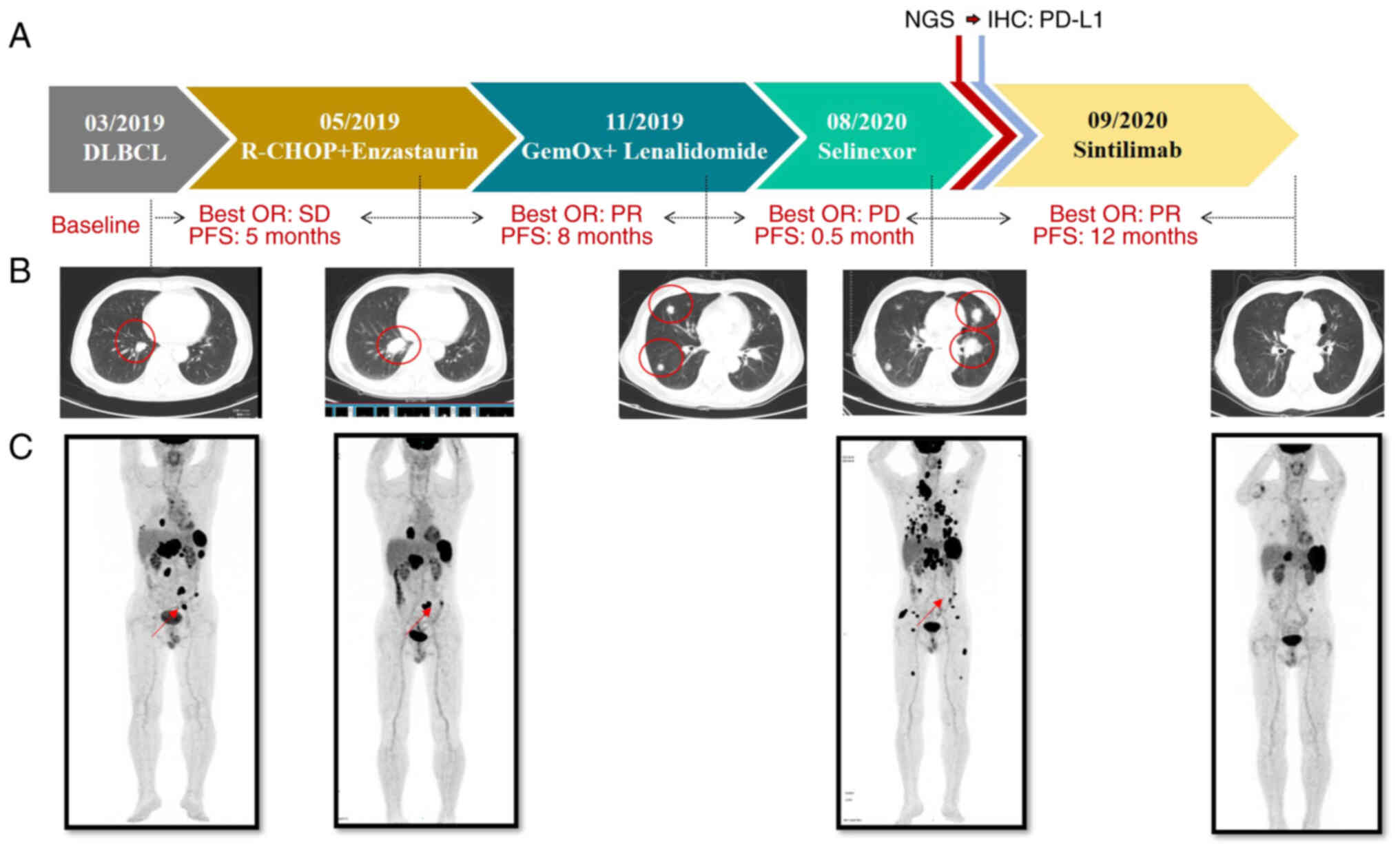 | Figure 2.Treatment course and representative
clinical images. (A) Disease timeline demonstrating the
various treatment regimens administered to the patient and the
corresponding clinical response. (B) Chest-CT and
(C) positron emission tomography-CT scans demonstrating the
disease progression following treatment. CT, computed tomography;
DLBCL, diffuse large B-cell lymphoma; IHC, immunohistochemical;
NGS, next-generation sequencing; OR, objective response; PD,
progressive disease; PD-L1, programmed death-ligand 1; PFS,
progression-free survival; PR, partial response; SD, stable
disease. |
According to the National Comprehensive Cancer
Network guidelines (Version 4.2019), it is standard clinical
practice for patients with stage IV DLBCL to participate in a
clinical trial (15). Thus, the
patient participated in a clinical trial (trial no. CTR20171560) in
May 2019, and received an initial treatment of R-CHOP (rituximab
586 mg on d1, CTX 1.17 g on d2, ADM 78.2 mg on d2, VCR 2 mg on d2
and PDN 100 mg on d2-6 every 21 days) plus enzastaurin (500 mg
every day). After three cycles of chemotherapy, stable disease was
observed, and after six cycles of chemotherapy, a PET-CT scan
indicated tumor shrinkage in the pancreas, peritoneum and
retroperitoneum. However, the tumor in the left parietal iliac
vessels increased from 1.3×0.8 to 2.0×1.1 cm, and the tumor in the
spleen increased from 3.5×2.1 to 7.5×5.3 cm. In addition, the size
of both pulmonary tumors had increased (Fig. 2B). Thus, the clinical response was
evaluated as progressive disease in the case of r/r DLBCL. The
subsequent treatment plan for the patient was based on the progress
of the patient over time. In November 2019, the chemotherapy
regimen was changed to GemOx (gemcitabine 1.6 g and oxaliplatin 150
mg on d1 every 14 days) plus lenalidomide (25 mg on d1-d14 every 21
days). After four cycles of this treatment, a partial response (PR)
was achieved (Fig. 2B). At this
time, the patient only underwent a chest CT to assess the treatment
effectiveness and did not have a PET-CT in line with the preference
of the patient. In August 2020, the disease progressed, with
symptoms of abdominal pain, hoarseness, choking and a wet cough.
Results of a subsequent PET-CT scan revealed a significant increase
in the number and size of lesions, as well as an overall increase
in metabolism and bone marrow involvement (Fig. 2C). Thereafter, the patient
participated in another clinical trial (trial no.
ATG-010-DLBCL-001) and was administered selinexor (ATG-010) (60 mg
twice weekly with food). However, the response was not
significant.
To explore new therapeutic treatments, a liver
biopsy sample collected in March 2019 was further analyzed in
September 2020, using NGS via the GeneseeqPrime® panel,
which allowed for the targeted enrichment of 437 cancer-related
genes (Supplementary methods).
This NGS was performed by Nanjing Geneseeq Technology Inc. The
results of the NGS revealed the presence of MYD88
(c.794T>C, p.L265P) and CD79B (c.586T>C, p.Y196H)
variants in the primary liver lesion (Table I), indicating that the patient had
the MYD88/CD79B-mutated (MCD) subtype of DLBCL, which
is associated with poor survival (2). A Bruton's tyrosine kinase (BTK)
inhibitor was suggested as a treatment option; however, the patient
declined due to financial concerns.
 | Table I.Genetic alterations detected by
targeted next-generation sequencing of the right cervical lymph
node and liver metastasis lesions, and the plasma sample. |
Table I.
Genetic alterations detected by
targeted next-generation sequencing of the right cervical lymph
node and liver metastasis lesions, and the plasma sample.
| Gene | Mutation | Genotype | Plasma, % | FFPE: Lymph node,
% | FFPE: Liver
metastasis |
|---|
| CD79B | p.Y196H | c.586T>C | - | 38.5 | 49.2% |
| MYD88 | p.L265P | c.794T>C | - | 56.1 | 58.4% |
| CD274 | Amplification | - | - | - | CN: 106.4 |
|
PDCD1LG2 | Amplification | - | - | - | CN: 77.3 |
| KRAS | Amplification | - | - | - | CN: 4.1 |
| TP53 | p.R175H | c.524G>A | - | 86.0 | 63.5% |
| TP53 | p.V216M | c.646G>A | - | - | 24.6% |
| BRCA1 | p.K339Rfs*2 | c.1016del | - | - | 17.9% |
| MYC | Fusion:IGH~MYC | IGH~MYC: exon2 | - | 22.9 | 1.5% |
| PPM1D | p.Q571* | c.1711C>T | 1.8 | - | - |
| PRDM1 | p.K235* | c.703A>T | - | 54.2 | 47.6% |
| AKT1 | p.R370H | c.1109G>A | - | - | 14.8% |
| ASXL3 | p.P1765S | c.5293C>T | - | 44.4 | 47.6% |
| BCL2 |
p.A43_148delinsRM |
c.127_144delinsCGCATG | - | - | 13.7% |
| BRIP1 | p.Q634H | c.1902G>C | - | - | 22.0% |
| BTG2 | p.A155T | c.463G>A | - | 46.8 | 51.8% |
| BTG2 | p.H52Y | c.154C>T | - | 28.6 | 30.2% |
| CD274 | p.1258M | c.774C>G | - | 15.1 | 14.8% |
| CHEK2 | p.G159E | c.476G>A | 3.1 | - | - |
| CIITA | p.1255F | C.763A>T | 5.1 | - | - |
| DICER1 | p.L987V | c.2959C>G | 1.2 | - | - |
| DTX1 |
p.V26_H34delinsY |
c.76_100delinsT | - | 8.2 | 22.5% |
| EP300 | p.P157A | c.469C>G | - | 13.9 | 21.6% |
| ETS1 | p.D6N | c.16G>A | - | 51.3 | 52.0% |
| ETV6 | p.K11N | c.33G>C | - | 70.7 | 74.2% |
| FAS | P.D108G | c.323A>G | - | 53.3 | 64.6% |
| H1-4 | p.G70D | c.209G>A | - | 47.6 | 40.8% |
| INPP5D | p.S27T | c.80G>C | - | 41.7 | 27.0% |
| LYST | p.M1647T | c.4940T>C | - | 30.4 | 27.3% |
| MSH6 | p.H1351Y | c.4051C>T | - | 25.9 | - |
| MYC | p.S388R | c.1164C>G | - | 29.1 | - |
| NFKBIA | p.A133T | c.397G>A | - | 35.3 | 21.7% |
| PIM1 | p.E226K | c.676G>A | - | 60.7 | 46.4% |
| PIM1 | p.S45R | c.135C>A | - | 28.0 | 19.8% |
| PIM1 | p.P124S | c.370C>T | - | 15.1 | 20.1% |
| PIM1 | p.K274_L275del | c.821_826del | - | 11.7 | - |
| PIM1 | c.345 355+8del | c.345 355+8del | - | - | 15.0% |
| PIM1 |
c.513+1_513+19delinsCTGAGGAGT |
c.513+1_513+19delinsCTGAGGAGT | - | - | 14.7% |
| ROS1 | p.P1756S | c.5266C>T | - | - | 31.7% |
| STIL | p.N1056S | c.3167A>G | - | - | 12.6% |
| TBL1XR1 | p.A416P | c.1246G>C | - | 35.3 | 20.8% |
The condition of the patient deteriorated, with
severe hoarseness, difficulty swallowing water and the presence of
a neck swelling; thus, a biopsy was performed on the neck swelling.
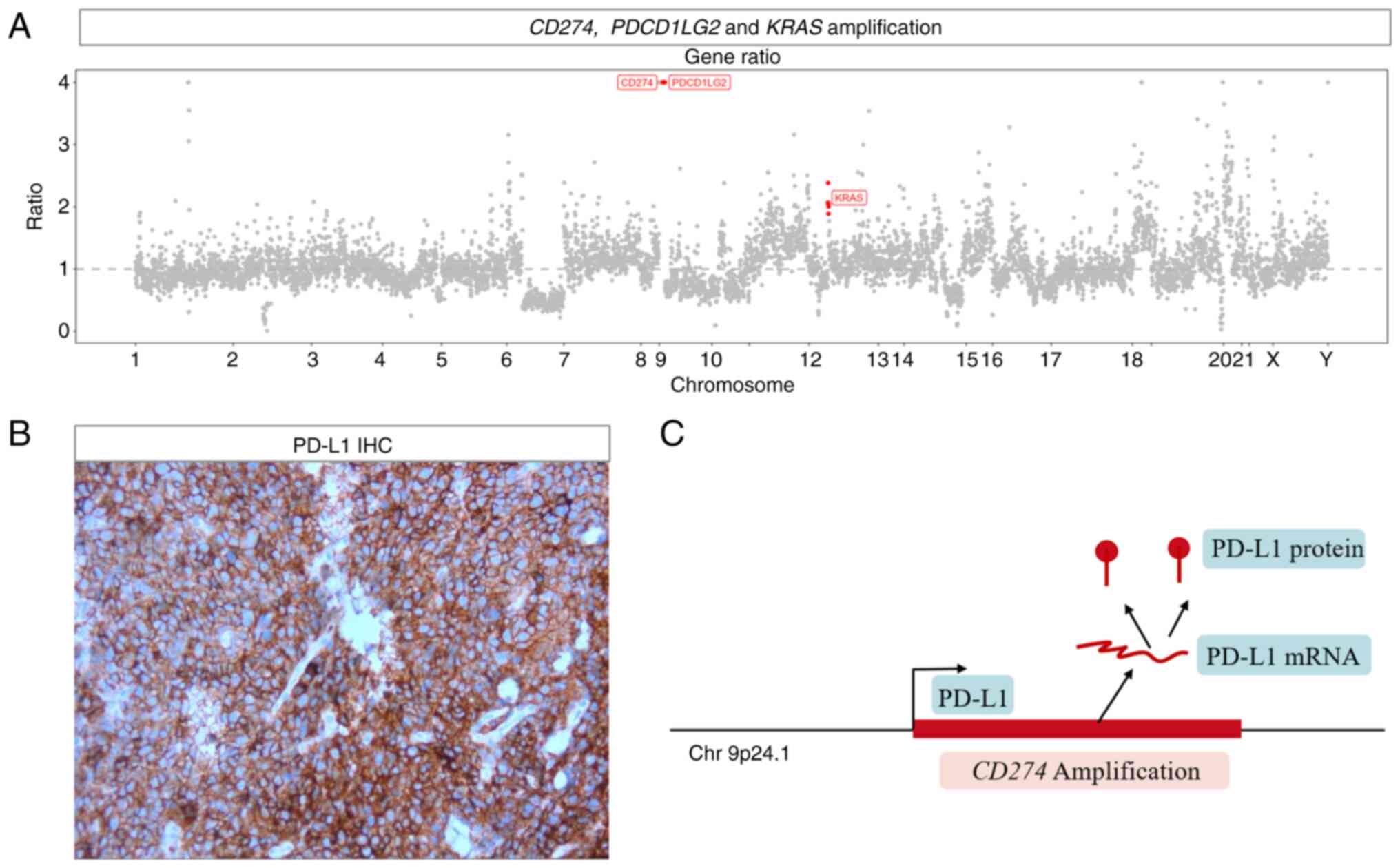
Pathological analysis confirmed the diagnosis of DLBCL. NGS
analysis of the lymph node sample revealed amplifications of
CD274, PDCD1LG2 and KRAS (Fig. 3A). IHC confirmed the high expression
levels of PD-L1 with TPS of 95%, which is encoded by CD274
(Fig. 3B). NGS testing was also
conducted on plasma samples simultaneously and it was found the
PPM1D Q571* mutation. This mutation was not detected in the
lymph node sample, suggesting it may have originated from other
lesions. The patient was therefore recommended immunotherapy with
sintilimab (200 mg each day/21 days). The effects of sintilimab
were assessed as PR after four cycles, and the response lasted for
12 months of follow-up. During the follow-up, the condition of the
patient was partially improved. The treatment was well-tolerated
with a slight decrease in leukocyte levels and no major
immune-related adverse events (irAEs). The patient benefitted from
sintilimab and there were no better treatment options available at
that time, thus the patient continued with this treatment. During a
telephone follow-up in November 2022, it was discovered that the
patient had passed away. As no tests were conducted immediately
before or after the death of the patient, the cause of death
remains unknown.
Discussion
DLBCL is a type of cancer originating from B cells,
a type of white blood cell that produces antibodies (16). DLBCL is the most frequent form of
NHL in adults, accounting for ~30% of all cases in Western
Countries (1). While the majority
of patients with DLBCL respond well to chemotherapy, some may
require alternative treatments.
In the present case, the patient was diagnosed with
r/r DLBCL. The cell-of-origin typing indicated a non-GCB subtype
and NGS further confirmed the MCD genotype, which is typically
associated with a poor prognosis. The mutated MYD88 protein
activates downstream NF-κB signaling pathways, which in turn
promote tumor cell viability and proliferation (17). In early phase clinical trials, drugs
such as BTK inhibitors, demonstrate efficacy against aberrant MYD88
signaling (18). However, the
patient described in the present study was unable to access BTK
inhibitors due to financial constraints.
After three lines of chemotherapy, the remaining
treatment options for the patient remained limited. The patient was
eventually treated with sintilimab based on the high PD-L1
expression levels and the NGS results indicating CD274
amplification, and the response was satisfactory. Notably,
CD274 amplification and PD-L1 expression were not detected
in the liver lesion upon initial diagnosis; however, these factors
were observed in the cervical lymph node metastases following
progression after multiple therapies. These results may be
indicative of a resistance mechanism.
Despite being a relatively uncommon variation in
DLBCL, CD274 amplification may impact disease progression
and clinical response. CD274 amplification is associated
with an upregulation of PD-L1, a protein that controls the activity
of immune cells through binding to PD-1 receptors (Fig. 3C). Upregulation of PD-L1 in DLBCL
promotes tumor growth by inhibiting the immune response against
cancer cells. The results of previous studies have demonstrated
that genomic level variations that cause PD-L1 upregulation include
gene rearrangements involving the 9p24.1 gene locus, which contains
the CD274 (PD-L1), PDCD1LG2 (PD-L2) and JAK2
genes, or 9p24.1 copy gains and amplifications (19,20).
Other variations, such as SP140 and PD-L1
translocation, PD-L1 and PD-L2 inversion, and
translocations between PD-L1 and IGH, PIM1 or
TP63 (19), may also
contribute to PD-L1 upregulation. These alterations were shown to
be greatly enriched in the activated B cell-like/non-GCB subtype
and were highly associated with high PD-L1 protein expression
levels (21). Furthermore, patients
with these molecular features demonstrated notable therapeutic
responses to PD-1 inhibitors (22).
In addition to PD-L1 expression, previous studies have also
investigated the effects of the immune microenvironment and
tumor-infiltrating lymphocytes on anti-PD-1 immunotherapies, and
the results demonstrated that both the PD-1/PD-L1 and CD73/A2aR
signaling pathways promoted an immunosuppressive microenvironment
in DLBCL, affecting patient response to PD-1 inhibitors (23).
In the present study, the patient responded well to
sintilimab monotherapy, in terms of tumor response and prognosis.
However, not all patients respond to such treatment, and some may
experience serious side effects, such as irAEs. Official guidelines
of instructions for sintilimab injection (2020) state that the
adverse effects of sintilimab are pneumonia, diarrhea, colitis,
hepatitis, nephritis, endocrinology diseases, skin AEs, infusion
reactions and other irAEs (24). If
patients experience severe adverse reactions, sintilimab treatment
should be stopped, and suitable symptomatic treatment may be
administered. The results of previous studies demonstrated that
anti-PD-1 drugs, either administered as a monotherapy or in
combination regimens, exhibit limited efficacy in the treatment of
patients with r/r DLBCL (25–28).
In a phase I clinical trial, nivolumab exhibited antitumor activity
in 11 patients with r/r DLBCL, with an objective response rate
(ORR) of 36% (25). In a phase II
clinical trial, nivolumab was used in the treatment of 121 patients
with DLBCL, and the ORR was <10%. In the same trial, in cohorts
with and without autologous hematopoietic cell transplantation, the
median progression-free survival (PFS) time was 1.9 and 1.4 months,
respectively, and the median overall survival (OS) time was 12.2
and 5.8 months, respectively (26).
A total of 38 patients with r/r DLBCL were included in the
KEYNOTE-155 study, and the results demonstrated an ORR of 21.1%
following treatment with pembrolizumab plus the CDK9 inhibitor,
dinaciclib. In addition, the median PFS and OS times were 2.1 and
7.9 months, respectively (27). A
total of 32 patients with r/r DLBCL were included in another phase
II clinical trial, and the results demonstrated an ORR of 33%
following treatment with lenalidomide in combination with
rituximab. In addition, the median PFS and OS times were 3.7 and
10.7 months, respectively (28).
However, further clinical trials are required to investigate the
effectiveness and potential side effects of ICIs in the treatment
of DLBCL. In addition, the results of a previous case report
suggested that the combined use of sintilimab and chidamide may
have potential in the treatment of patients with r/r DLBCL,
resulting in a prolonged complete remission. However, during the
combination therapy, the patient experienced adverse events due to
chidamide, including thrombocytopenia and neutropenia (13). Thus, it is necessary for patients to
undergo long-term follow-up, to determine the durability of the
partial remission achieved with sintilimab monotherapy or
combination therapy.
PD-L2 (encoded by PDCD1LG2) is a protein that
regulates the immune response through binding to the PD-1 receptor
on T cells (29). While high levels
of PD-L2 expression have been associated with improved responses to
immunotherapy in certain cancer types, including non-small cell
lung cancer and melanoma (30), the
role of PD-L2 expression in DLBCL is yet to be fully elucidated.
Although KRAS mutations are not commonly observed in
patients with DLBCL, these mutations may be associated with
aggressive disease development and poor clinical outcomes (31). Thus, the identification of
KRAS mutations in patients will aid in determining
appropriate treatment strategies, as these patients may require
more intense or innovative therapies to overcome drug resistance or
immune evasion mediated by abnormal KRAS proteins.
NGS is a powerful tool that provides valuable
insights into the genome of an individual (32). NGS aids in identifying genomic
variations that may be associated with specific diseases or
conditions, promoting earlier diagnoses and the selection of more
effective treatment options (33,34).
Furthermore, blood-based liquid biopsies have the potential to
facilitate the early detection of cancer, thereby improving the
chances of patient recovery (35).
In the present case, NGS was instrumental in the molecular
diagnosis of the patient and provided guidance for the potential
use of sintilimab in patients with r/r DLBCL. Following the use of
conventional treatment modalities for DLBCL, NGS may provide
insight into potential treatment alternatives. In addition, the
results of a previous study revealed that the analysis of
metabolites may assist in revealing the real-time status of
biological systems. For example, metabolomics showed potential in
the early diagnosis, treatment and prognosis prediction of patients
with breast cancer, demonstrating an additional tool for early
screening and diagnosis (36).
The present study exhibited several limitations. For
example, a single patient was included in the present study,
meaning that additional experiments were limited. Further
investigations that examine the effects of the immune
microenvironment or tumor-infiltrating lymphocytes are required.
Further prospective studies are also required to confirm the
efficacy of sintilimab in patients with r/r DLBCL. In addition, the
efficacy of sintilimab monotherapy remains to be fully elucidated.
Thus, further investigations that explore the potential of
sintilimab in combination with other targeted therapies or
immunotherapies are required.
In conclusion, DLBCL is a complex disease with
numerous different subtypes and potential genomic variations.
Understanding the specific molecular mechanisms of DLBCL has
contributed to the development of targeted therapies and
immunotherapies that may improve the survival of patients with this
disease. However, additional investigations are required to further
the current understanding of the disease and determine novel
therapeutic options.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The sequencing results and raw data generated in the
present study may be found in the BioProject database under
accession numbers PRJNA1066705 and PRJNA1086347 or at the following
URLs: https://www.ncbi.nlm.nih.gov/bioproject/PRJNA1066705
and https://www.ncbi.nlm.nih.gov/bioproject/PRJNA1086347.
Authors' contributions
XZ designed this study and collected the data for
this case report. LX conceived the present study. EP analyzed and
interpreted of data. XS acquired the data. XD made substantial
contributions to conception and design. XS and XD confirm the
authenticity of all the raw data. All authors have read and
approved the final version of the manuscript.
Ethics approval and consent to
participate
The clinical trials in which the patient
participated were approved by the Ethics Committee of The Second
Hospital of Dalian Medical University (Dalian, China), including
R-CHOP plus enzastaurin (trial no. CTR20171560) and selinexor
(trial no. ATG-010-DLBCL-001).
Patient consent for publication
Written informed consent to publish the clinical
details and images were obtained from the patient's relative.
Competing interests
EP is employed by Nanjing Geneseeq Technology, Inc.
Nanjing Geneseeq Technology, Inc. is a tumor gene testing company,
and the present study may help to promote the application of NGS
technology, enhance the company's reputation and drive the
company's business. The remaining authors declare that they have no
competing interests.
References
|
1
|
Martelli M, Ferreri AJM, Agostinelli C, Di
Rocco A, Pfreundschuh M and Pileri SA: Diffuse large B-cell
lymphoma. Crit Rev Oncol Hematol. 87:146–171. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wright GW, Huang DW, Phelan JD, Coulibaly
ZA, Roulland S, Young RM, Wang JQ, Schmitz R, Morin RD, Tang J, et
al: A probabilistic classification tool for genetic subtypes of
diffuse large B cell lymphoma with therapeutic implications. Cancer
Cell. 37:551–568.e14. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hertzberg M: R-CHOP in DLBCL: Priming for
success. Blood. 139:1121–1122. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang L and Li LR: R-CHOP resistance in
diffuse large B-cell lymphoma: Biological and molecular mechanisms.
Chin Med J (Engl). 134:253–260. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Goldfinger M and Cooper DL: Refractory
DLBCL: Challenges and treatment. Clin Lymphoma Myeloma Leuk.
22:140–148. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Liu Y and Barta SK: Diffuse large B-cell
lymphoma: 2019 Update on diagnosis, risk stratification, and
treatment. Am J Hematol. 94:604–616. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li T, Yu J, Hou M, Zha S, Cheng Q, Zheng Q
and Li L: Quantitative evaluation of therapy options for
relapsed/refractory diffuse large B-cell lymphoma: A model-based
meta-analysis. Pharmacol Res. 187:1065922023. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
He MY and Kridel R: Treatment resistance
in diffuse large B-cell lymphoma. Leukemia. 35:2151–2165. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hoy SM: Sintilimab: First global approval.
Drugs. 79:341–346. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yi M, Zheng X, Niu M, Zhu S, Ge H and Wu
K: Combination strategies with PD-1/PD-L1 blockade: Current
advances and future directions. Mol Cancer. 21:282022. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liu X and Yi Y: Recent updates on
sintilimab in solid tumor immunotherapy. Biomark Res. 8:692020.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ren Z, Xu J, Bai Y, Xu A, Cang S, Du C, Li
Q, Lu Y, Chen Y, Guo Y, et al: Sintilimab plus a bevacizumab
biosimilar (IBI305) versus sorafenib in unresectable hepatocellular
carcinoma (ORIENT-32): A randomised, open-label, phase 2–3 study.
Lancet Oncol. 22:977–990. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chen C, Zhang W, Zhou D and Zhang Y:
Sintilimab and chidamide for refractory transformed diffuse large B
cell lymphoma: A case report and a literature review. Front Oncol.
11:7574032021. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Roach C, Zhang N, Corigliano E, Jansson M,
Toland G, Ponto G, Dolled-Filhart M, Emancipator K, Stanforth D and
Kulangara K: Development of a companion diagnostic PD-L1
immunohistochemistry assay for pembrolizumab therapy in
non-small-cell lung cancer. Appl Immunohistochem Mol Morphol.
24:392–397. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
National Comprehensive Cancer Network.
NCCN clinical practice guidelines in oncology, . B-cell lymphomas.
Version 4.2019. 2019.Retrieved from. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf
|
|
16
|
Tanimura A, Nakazato A and Tanaka N: MYD88
signals induce tumour-initiating cell generation through the
NF-κB-HIF-1α activation cascade. Sci Rep. 11:39912021. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chapuy B, Stewart C, Dunford AJ, Kim J,
Kamburov A, Redd RA, Lawrence MS, Roemer MGM, Li AJ, Ziepert M, et
al: Molecular subtypes of diffuse large B cell lymphoma are
associated with distinct pathogenic mechanisms and outcomes. Nat
Med. 24:679–690. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cohen JB, Shah NN, Alencar AJ, Gerson JN,
Patel MR, Fakhri B, Jurczak W, Tan XN, Lewis KL, Fenske T, et al:
MCL-133 pirtobrutinib, a highly selective, non-covalent
(reversible) BTK inhibitor in previously treated mantle cell
lymphoma: Updated results from the phase 1/2 BRUIN study. Clin
Lymph Myelom Leuk. 22 (Suppl 2):S394–S395. 2022. View Article : Google Scholar
|
|
19
|
Georgiou K, Chen L, Berglund M, Ren W, de
Miranda NF, Lisboa S, Fangazio M, Zhu S, Hou Y, Wu K, et al:
Genetic basis of PD-L1 overexpression in diffuse large B-cell
lymphomas. Blood. 127:3026–3034. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Green MR, Monti S, Rodig SJ, Juszczynski
P, Currie T, O'Donnell E, Chapuy B, Takeyama K, Neuberg D, Golub
TR, et al: Integrative analysis reveals selective 9p24.1
amplification, increased PD-1 ligand expression, and further
induction via JAK2 in nodular sclerosing Hodgkin lymphoma and
primary mediastinal large B-cell lymphoma. Blood. 116:3268–3277.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Godfrey J, Tumuluru S, Bao R, Leukam M,
Venkataraman G, Phillip J, Fitzpatrick C, McElherne J, MacNabb BW,
Orlowski R, et al: PD-L1 gene alterations identify a subset of
diffuse large B-cell lymphoma harboring a T-cell-inflamed
phenotype. Blood. 133:2279–2290. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ansell SM, Lesokhin AM, Borrello I,
Halwani A, Scott EC, Gutierrez M, Schuster SJ, Millenson MM, Cattry
D, Freeman GJ, et al: PD-1 blockade with nivolumab in relapsed or
refractory Hodgkin's lymphoma. N Engl J Med. 372:311–319. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhang T, Liu H, Jiao L, Zhang Z, He J, Li
L, Qiu L, Qian Z, Zhou S, Gong W, et al: Genetic characteristics
involving the PD-1/PD-L1/L2 and CD73/A2aR axes and the
immunosuppressive microenvironment in DLBCL. J Immunother Cancer.
10:e0041142022. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhang L, Mai W, Jiang W and Geng Q:
Sintilimab: A promising anti-tumor PD-1 antibody. Front Oncol.
10:5945582020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lesokhin AM, Ansell SM, Armand P, Scott
EC, Halwani A, Gutierrez M, Millenson MM, Cohen AD, Schuster SJ,
Lebovic D, et al: Nivolumab in patients with relapsed or refractory
hematologic malignancy: Preliminary results of a phase Ib study. J
Clin Oncol. 34:2698–2704. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ansell SM, Minnema MC, Johnson P,
Timmerman JM, Armand P, Shipp MA, Rodig SJ, Ligon AH, Roemer MGM,
Reddy N, et al: Nivolumab for relapsed/refractory diffuse large
B-cell lymphoma in patients ineligible for or having failed
autologous transplantation: A single-arm, phase II study. J Clin
Oncol. 37:481–489. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gregory GP, Kumar S, Wang D, Mahadevan D,
Walker P, Wagner-Johnston N, Escobar C, Bannerji R, Bhutani D,
Chang J, et al: Pembrolizumab plus dinaciclib in patients with
hematologic malignancies: The phase 1b KEYNOTE-155 study. Blood
Adv. 6:1232–1242. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang M, Fowler N, Wagner-Bartak N, Feng L,
Romaguera J, Neelapu SS, Hagemeister F, Fanale M, Oki Y, Pro B, et
al: Oral lenalidomide with rituximab in relapsed or refractory
diffuse large cell, follicular and transformed lymphoma: A phase II
clinical trial. Leukemia. 27:1902–1909. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Messal N, Serriari NE, Pastor S, Nunès JA
and Olive D: PD-L2 is expressed on activated human T cells and
regulates their function. Mol Immunol. 48:2214–2219. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Yearley JH, Gibson C, Yu N, Moon C, Murphy
E, Juco J, Lunceford J, Cheng J, Chow LQM, Seiwert TY, et al: PD-L2
expression in human tumors: Relevance to Anti-PD-1 therapy in
cancer. Clin Cancer Res. 23:3158–3167. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lohr JG, Stojanov P, Lawrence MS, Auclair
D, Chapuy B, Sougnez C, Cruz-Gordillo P, Knoechel B, Asmann YW,
Slager SL, et al: Discovery and prioritization of somatic mutations
in diffuse large B-cell lymphoma (DLBCL) by whole-exome sequencing.
Proc Natl Acad Sci USA. 109:3879–3884. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lohmann K and Klein C: Next generation
sequencing and the future of genetic diagnosis. Neurotherapeutics.
11:699–707. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Mosele F, Remon J, Mateo J, Westphalen CB,
Barlesi F, Lolkema MP, Normanno N, Scarpa A, Robson M,
Meric-Bernstam F, et al: Recommendations for the use of
next-generation sequencing (NGS) for patients with metastatic
cancers: A report from the ESMO precision medicine working group.
Ann Oncol. 31:1491–1505. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Hussen BM, Abdullah ST, Salihi A, Sabir
DK, Sidiq KR, Rasul MF, Hidayat HJ, Ghafouri-Fard S, Taheri M and
Jamali E: The emerging roles of NGS in clinical oncology and
personalized medicine. Pathol Res Pract. 230:1537602022. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Adams E, Sepich-Poore GD,
Miller-Montgomery S and Knight R: Using all our genomes:
Blood-based liquid biopsies for the early detection of cancer. View
(Beijing). 3:202001182022.PubMed/NCBI
|
|
36
|
Huang Y, Du S, Liu J, Huang W, Liu W,
Zhang M, Li N, Wang R, Wu J, Chen W, et al: Diagnosis and prognosis
of breast cancer by high-performance serum metabolic fingerprints.
Proc Natl Acad Sci USA. 119:e21222451192022. View Article : Google Scholar : PubMed/NCBI
|