Introduction
Urothelial carcinoma (UC) is a common urological
malignancy, and UC of the urinary bladder is the ninth most common
cancer in the world (1),
furthermore, approximately 5–10% of patients have metastatic
disease at the time of diagnosis (2,3).
Although platinum-based chemotherapy has been performed as standard
first line treatment in patients with metastatic and unresectable
urothelial carcinoma (mUC), the prognosis was poor with a median
overall survival of approximately 15 months (4). Furthermore, no survival-prolonging
subsequent therapy following to the platinum-based chemotherapy was
available for a long period.
In recent years, immune checkpoint inhibitors (ICIs)
have been widely used to treat malignancies. Pembrolizumab
demonstrated survival benefit in patients with mUC who had received
systemic chemotherapy (5) and has
been approved as subsequent treatment following prior chemotherapy
in Japan. Longer survival was observed in patients with mUC treated
in the recent era compared with those treated before pembrolizumab
was approved (6).
Although pembrolizumab can be beneficial for
patients with mUC, only a few patients experienced clinical
responses (5). Additionally, some
patients developed immune-related adverse events (irAEs), which can
be serious. By contrast, a long duration of response was reported
in patients with response (7);
therefore, development of biomarkers that predict pembrolizumab
response is expected.
An exploratory analysis for biomarkers using data
from the randomized phase III KEYNOTE-045 trial revealed that
patients with a higher tumor mutation burden and T-cell-inflamed
gene expression demonstrated better response to pembrolizumab than
those without (8). However, in
clinical practice, these biomarkers cannot be measured easily.
C-reactive protein (CRP) is a representative acute
phase reactant that is widely used to evaluate systemic
inflammation. In addition, continued increasing of CRP levels been
proven to be an indicator of chronic inflammation associated with
many diseases such as obesity (9),
cardiovascular disease (10), and
also malignant tumors (11).
Furthermore, chronic inflammation can contribute to initiation,
promotion, growth, and invasion of tumors (12). Inflammation also affects the
response to therapy, the association between the systemic
inflammation and poor prognosis was reported in many cancers
(13,14). In addition, the relation between
serum CRP levels and oncological outcome has also been investigated
in patients with several malignancies received ICI. Elevated the
pretreatment CRP levels were found to be associated with the poor
outcome in patients with many cancers treated with ICI, including
UC, melanoma, lung cancer, renal cell carcinoma, and other cancers
(15). Moreover, the relationship
between changes in CRP levels with ICI treatment and oncological
outcome have also been studied in patients with renal cell
carcinoma and UC. Among patients with high pretreatment CRP levels,
the patients with decreased CRP levels after initiation of ICI
showed better survival comparing to those without (16,17).
In patients with mUC who were treated with
pembrolizumab, both baseline (BL) CRP levels and post-treatment
changes have been associated with the efficacy of pembrolizumab
(17–19). The association between early CRP
elevation (CRP flare phenomenon) and the efficacy of ICI therapy
was first reported in non-small cell lung cancer (20). Patients with renal cell carcinoma
who demonstrated a decrease in CRP levels below BL following flare
phenomenon (CRP flare-response) showed favorable oncological
outcome (21). We previously
observed that patients with mUC treated with pembrolizumab showed a
favorable outcome after the CRP flare-response (22). However, we could not perform
detailed investigation for clinical significance of the CRP
flare-response because of a small cohort, which included only three
patients with CRP flare. Additionally, only one more study has
investigated the association between CRP flare and oncological
outcome in patients with mUC (23);
thus, data on the clinical significance of CRP flares are limited.
In this study, we used a multicenter cohort to investigate the
impact of CRP flares on clinical outcome in patients with advanced
UC treated with pembrolizumab.
Materials and methods
Study population
The inclusion criteria were patients aged 18 years
or older with histologically confirmed mUC of the urinary tract.
Patients had previously received systemic chemotherapy and
subsequent pembrolizumab between March 2018 and December 2022 at
one academic center (University of Occupational and Environmental
Health) and six general hospitals (Kokura Memorial Hospital,
Munakata Suikokai General Hospital, Shin-kokura Hospital,
Shin-yukuhashi Hospital, Kitakyushu City Yahata Hospital, and Moji
Medical Center). A total of 110 patients were included in this
study and their median age and the range of age were 74 and 40 to
86 years old, respectively. Patients who developed infectious
disease within 3 months of pembrolizumab administration and
patients with insufficient data on CRP were excluded because
evaluation of early CRP kinetics cannot be performed correctly.
This retrospective, multicenter study was approved by the Ethics
Committee of the University of Occupational and Environmental
Health, Japan (UOEHCRB20-180), the ethics committee of Kokura
Memorial Hospital (22092002E), the Ethics Committee of Munakata
Suikokai General Hospital (22003), the Ethics Committee of
Shin-kokura Hospital (2022–002), the Ethics Committee of
Shin-yukuhashi Hospital (R3-35), the Ethics Committee of Kitakyushu
City Yahata Hospital (20220510), and the Ethics Committee of Moji
Medical Center (04–05). This study was conducted in accordance with
the ethical guidelines of the Declaration of Helsinki.
Study design
Patients received intravenous infusion of
pembrolizumab once every 3 (200 mg) or 6 (400 mg) weeks and
continued use until disease progression or unacceptable adverse
events (AEs) were observed. Blood parameters, including CRP levels,
were tested at BL and at least every 3 weeks within 3 months after
starting pembrolizumab therapy. Chest and abdominal computed
tomography scans were performed before initiation of pembrolizumab
therapy and repeated every 8–12 weeks at the physician's
discretion. Best overall response (BOR), progression-free survival
(PFS), overall survival (OS), and incidence of irAEs were compared
between the groups divided based on early CRP kinetics. BOR was
defined as the best tumor response achieved during pembrolizumab
treatment and assessed according to the Response Evaluation
Criteria in Solid Tumor version 1.1. Objective response rate (ORR)
was shown as the sum of complete and partial response rate. AEs
were evaluated based on the Common Terminology Criteria for Adverse
Events version 5.0. In addition, factors associated with PFS were
investigated.
Definition of early CRP kinetics
According to the definition of CRP kinetics
(21), patients were grouped as
follows: i) Flare-responders, in which CRP levels increased to at
least double from BL within the first month after initiation of
pembrolizumab (CRP flare) and then decreased below BL within 3
months; ii) responders, in which CRP levels decreased by ≥30% from
BL within 3 months without CRP flare; and iii) non-responders,
which included the remaining patients.
Furthermore, CRP flare-responders were divided into
two groups according to the median BL CRP value before
pembrolizumab administration. Because several cutoff values of
pretreatment CRP predicting the prognosis in patients with mUC who
received pembrolizumab were reported and no established reference
value was available (18,19,24–26),
the median value was used.
Statistical analysis
Fisher's exact test was used for comparing BOR and
incidence of irAEs among groups. OS and PFS were calculated from
the first initiation of pembrolizumab until the last follow-up or
death from any cause and disease progression, respectively.
Survival analysis was performed using the Kaplan-Meier method and
log-rank test. Multivariate analysis was performed using the Cox
proportional hazards regression model to identify PFS-associated
factors. P<0.05 was considered to indicate a statistically
significant difference. Statistical analyses were performed using
EZR (Saitama Medical Center, Jichi Medical University, Saitama,
Japan), which is a graphical user interface for R (The R Foundation
for Statistical Computing, Vienna, Austria) (27).
Results
During the study, 110 patients with mUC received
pembrolizumab as subsequent therapy following chemotherapy. One
patient who had acute pyelonephritis 5 d after starting
pembrolizumab treatment and a patient who had insufficient CRP data
was excluded from the study cohort. Thus, 108 eligible patients
were included in this study and 17 (16%), 27 (25%), and 64 (59%)
patients were grouped as CRP flare-responders, CRP responders, and
CRP non-responders, respectively. In CRP non-responders, more
patients had histologic subtypes or divergent differentiation
comparing to CRP flare-responders and CRP responders. No remarkable
difference was shown in the other patient characteristics among the
three groups (Table I).
 | Table I.Patients characteristics stratified
by early CRP kinetics. |
Table I.
Patients characteristics stratified
by early CRP kinetics.
| Characteristic | Non-responder | Responder |
Flare-responder |
|---|
| Number of
patients | 64 | 27 | 17 |
| Median age, years
(IQR) | 73 (67–78) | 75 (49–81) | 75 (66–79) |
| Sex, n (%) |
|
|
|
|
Male | 50 (78) | 20 (74) | 11 (65) |
|
Female | 14 (22) | 7 (26) | 6 (35) |
| Median BMI,
kg/m2 (IQR) | 23.3
(20.3–25.2) | 22.8
(20.4–25.5) | 20.6
(20.0–23.3) |
| ECOG-PS, n (%) |
|
|
|
| 0 | 40 (63) | 19 (70) | 10 (59) |
| ≥1 | 24 (37) | 8 (30) | 7 (41) |
| Primary lesion, n
(%) |
|
|
|
| Upper
tract | 32 (50) | 16 (59) | 9 (53) |
|
Bladder | 28 (44) | 10 (37) | 7 (41) |
|
Both | 4 (6.2) | 1 (3.7) | 1 (5.9) |
| Histological grade,
n (%) |
|
|
|
| High
grade | 64 (100) | 27 (100) | 17 (100) |
| G2 | 10 (16) | 3 (11) | 3 (18) |
|
G2>G3 | 6 (9.4) | 4 (15) | 1 (5.9) |
|
G3>G2 | 8 (13) | 2 (7.4) | 2 (12) |
| G3 | 40 (63) | 18 (67) | 11 (65) |
| Histologic type
(%) |
|
|
|
| Pure
UC | 44 (69) | 23 (85) | 14 (82) |
|
Squamous differentiation | 15 (23) | 3 (11) | 1 (5.9) |
|
Glandular differentiation | 1 (1.6) | 0 (0) | 1 (5.9) |
| Clear
cell subtype | 1 (1.6) | 0 (0) | 0 (0) |
|
Sarcomatoid subtype | 1 (1.6) | 1 (3.7) | 0 (0) |
| Giant
cell subtype | 1 (1.6) | 0 (0) | 0 (0) |
| Nested
subtype | 1 (1.6) | 0 (0) | 0 (0) |
|
Plasmacytoid subtype | 0 (0) | 0 (0) | 1 (5.9) |
| Hemoglobin, n
(%) |
|
|
|
| ≥10
g/dl | 36 (56) | 15 (56) | 10 (59) |
| <10
g/dl | 28 (44) | 12 (44) | 7 (41) |
| Liver metastasis, n
(%) |
|
|
|
|
Absence | 48 (75) | 23 (85) | 15 (88) |
|
Presence | 16 (25) | 4 (15) | 2 (12) |
| Prior treatment
line, n (%) |
|
|
|
| 1 | 54 (84) | 24 (89) | 16 (94) |
| ≥2 | 10 (16) | 3 (11) | 1 (5.9) |
| Radical surgery, n
(%) |
|
|
|
|
Absence | 28 (44) | 14 (52) | 7 (41) |
|
Presence | 36 (56) | 13 (48) | 10 (59) |
| Time from prior
chemotherapy, n (%) |
|
|
|
| ≥3
months | 22 (34) | 12 (44) | 8 (47) |
| <3
months | 42 (66) | 15 (56) | 9 (53) |
| Median baseline
CRP, g/dl (IQR) | 0.80
(0.19–4.05) | 1.18
(0.35–3.08) | 0.32
(0.20–1.97) |
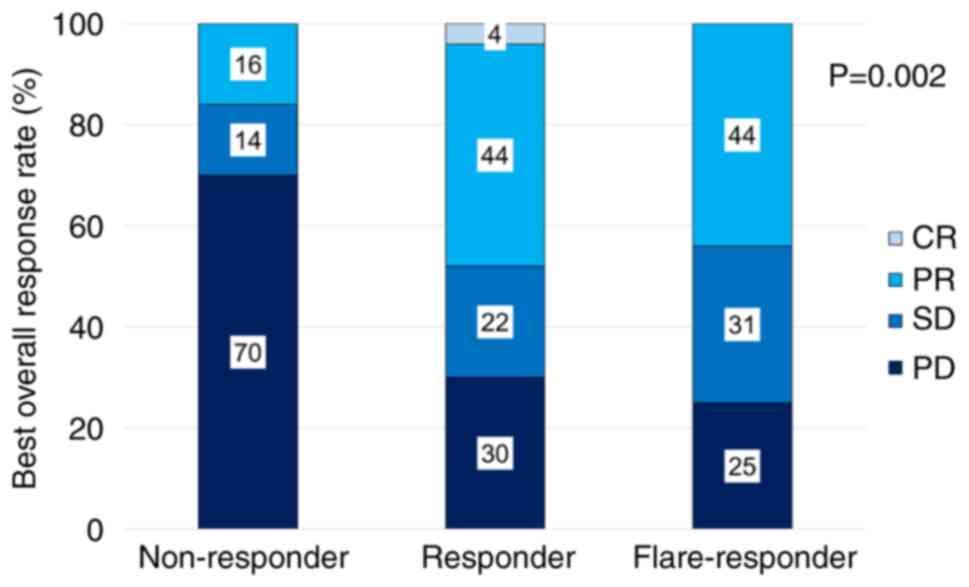
In BOR, ORR was 44, 48, and 16% in CRP
flare-responders, CRP responders, and CRP non-responders,
respectively (Fig. 1). The median
follow-up was 8.6 months, 90 patients developed progression and 81
died during the study. Forty patients received subsequent therapy:
10, 2, and 28 patients received platinum-based chemotherapy,
paclitaxel and gemcitabine therapy, and enfortumab vedotin,
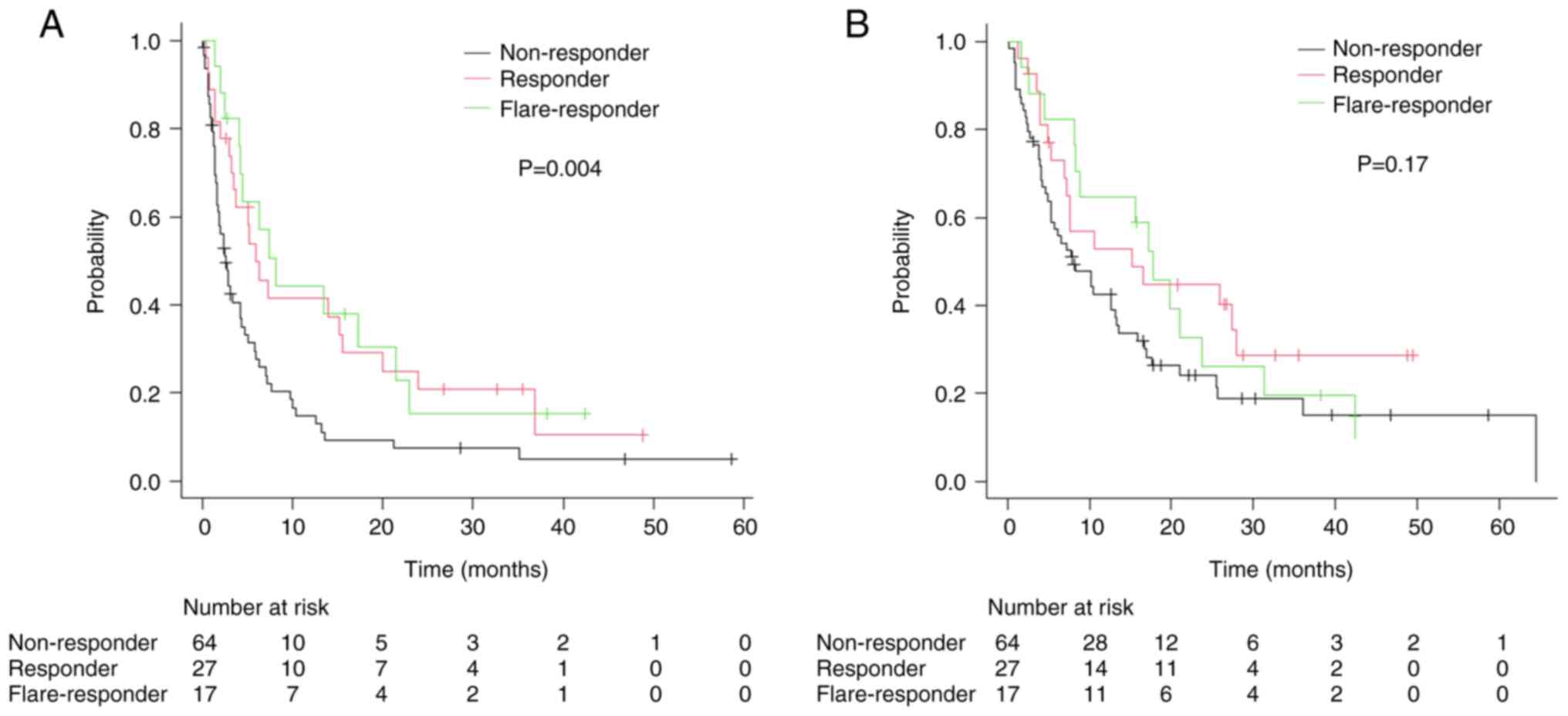
respectively, following pembrolizumab. In survival analysis, median
PFS was 8.1 [95% confidence interval (CI) 4.1–21.5] months for CRP
flare-responders, 5.9 (95% CI: 3.3–15.6) months for CRP responders,
and 2.6 (95% CI: 1.7–4.2) months for CRP non-responders, with
significant differences between the groups (Fig. 2A). Median OS for CRP
flare-responders, CRP responders, and CRP non-responders was 17.8
(95% CI: 8.2–23.7) months, 15.2 (95% CI: 7.0–27.9) months, and 7.9
(95% CI: 5.3–13.2) months, respectively (Fig. 2B). Between the groups, difference in
the incidence of irAEs, including severe cases (≥grade 3) was
insignificant (Table II).
| Table II.Immune-related adverse events in each
group according to early C-reactive protein kinetics. |
Table II.
Immune-related adverse events in each
group according to early C-reactive protein kinetics.
| Grade of adverse
events | Non-responder | Responder |
Flare-responder | P-value |
|---|
| Any grade (%) | 15 (23) | 8 (29) | 5 (29) | 0.78 |
| ≥Grade 3 (%) | 7 (11) | 0 (0) | 2 (12) | 0.16 |
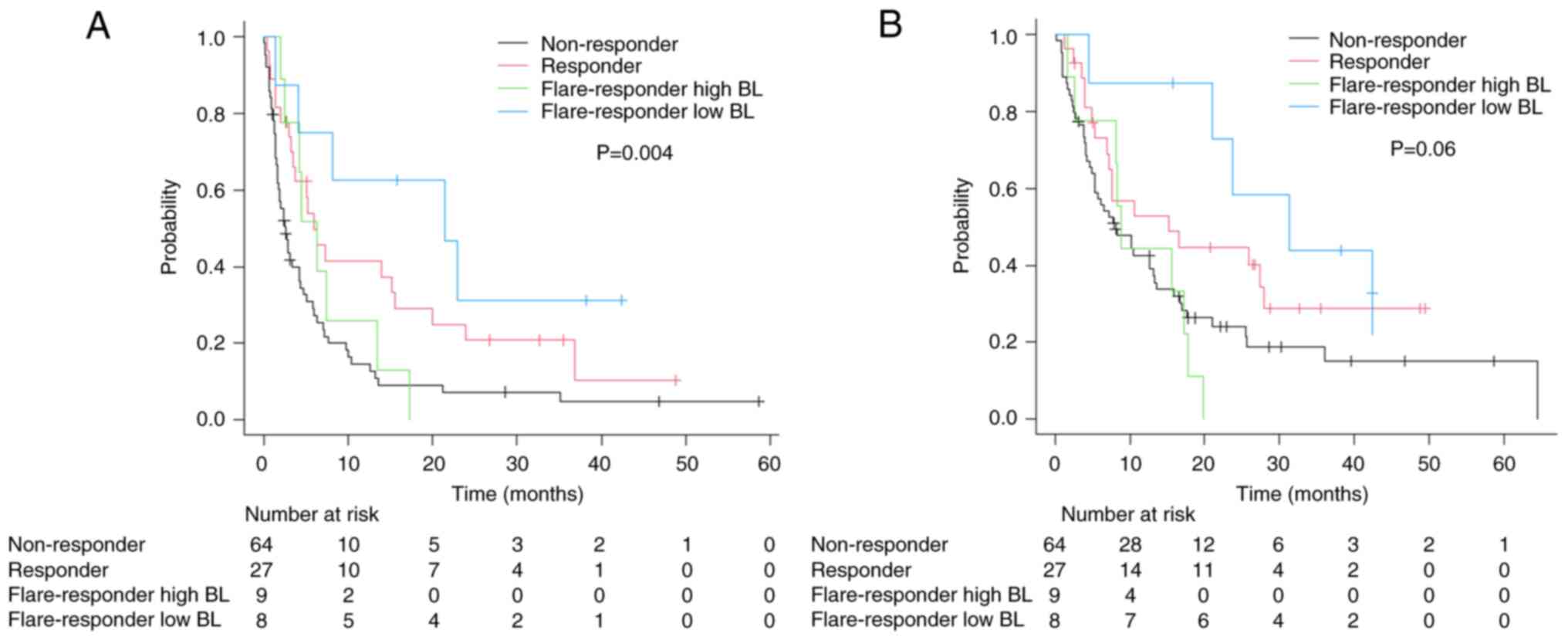
CRP flare-responders were further divided into two
groups based on median BL (before initiation of pembrolizumab) CRP
value (0.32 g/dl): CRP flare-responders low BL and CRP
flare-responders high BL. In total, 8 and 9 patients were
categorized as CRP flare-responders low and high BL, respectively.
CRP flare-responders low BL included fewer patients with recent
(<3 months) chemotherapy and low (<10 g/dl) hemoglobin
compared with CRP flare-responders high BL (Table SI). Comparison between the groups
revealed higher ORR in the CRP flare-responders low BL group than
the CRP flare-responders high BL group (63% vs. 25%). Although CRP
flare-responders low BL demonstrated the longest PFS (median 21.5
months, 95% CI: 1.3-not estimable), CRP flare-responders high BL
showed a similar PFS (median 6.3 months, 95% CI: 2.1–13.4) as CRP
responders (Fig. 3A). CRP
flare-responders low BL demonstrated longer OS (median 31.4 months,
95% CI: 4.7-not estimable) compared with other groups, whereas CRP
flare-responders high BL had similar OS (median 8.9 months, 95% CI:
1.7–17.8) as CRP non-responders (Fig.
3B). In multivariate analysis to predict PFS, CRP
flare-responders low BL was a significant factor with lowest hazard
ratio (Table III). Although
severe (≥grade 3) irAEs were frequently observed in CRP
flare-responders low BL compared with CRP flare-responders high BL
(25% vs. 0%), the occurrence of all irAEs was similar between the
groups (25% vs. 33%).
| Table III.Multivariate analysis to predict
progression-free survival in patients with metastatic and
unresectable urothelial carcinoma who received pembrolizumab. |
Table III.
Multivariate analysis to predict
progression-free survival in patients with metastatic and
unresectable urothelial carcinoma who received pembrolizumab.
| Factor | Hazard ratio | P-value |
|---|
| Age
(continuous) | 1.00
(0.98–1.03) | 0.72 |
| Sex (female) | 1.81
(1.07–3.05) | 0.03 |
| Hemoglobin (<10
g/dl) | 1.33
(0.83–2.14) | 0.24 |
| ECOG-PS (≥1) | 1.25
(0.78–2.00) | 0.35 |
| Time from prior
chemotherapy (<3 months) | 1.61
(1.00–2.60) | 0.05 |
| Liver metastasis
(presence) | 1.54
(0.89–2.67) | 0.13 |
| CRP responder | 0.46
(0.26–0.79) | 0.01 |
| CRP flare-responder
high BL | 0.46
(0.21–1.04) | 0.06 |
| CRP flare-responder
low BL | 0.31
(0.12–0.80) | 0.02 |
Discussion
In this study, we demonstrated that 16% of the
patients with mUC treated with pembrolizumab showed the CRP
flare-response. A favorable tumor response and survival were
observed in CRP flare-responders and responders compared with CRP
non-responders. In CRP flare-responders, patients with low BL CRP
demonstrated better tumor response and survival than those with
high BL CRP. The CRP flare-response with low BL CRP levels was a
significant favorable factor predicting PFS. Although no difference
was shown in the occurrence of any grade of irAE, severe irAEs were
most commonly observed in CRP flare-responders low BL.
The association between the CRP flare-response and
oncological outcomes was reported in patients with several
malignancies, such as renal cell carcinoma (21,28),
non-small cell lung cancer (29,30),
hepatocellular carcinoma (31),
head and neck cancer (32), and
urothelial carcinoma (22,23), treated with ICI. In patients who
received ICI, the CRP flare-response was observed in approximately
10–25% of the patients. Consistent with our data, 17% of the
patients with UC showed the CRP flare-response (23).
In the studies investigated the CRP flare-response,
whereas the better tumor response and survival in patients with the
CRP flare-response compared with those of the CRP responders and
non-responders was reported (21,29,31),
several studies showed that there was not much difference in
oncological outcomes between CRP flare-responders and responders as
well as our results (23,28,30,32).
Interestingly, in this study, tumor response and survival were
greatly different between the groups depending on BL CRP among CRP
flare-responders. Although favorable oncological outcomes were
observed in CRP flare-responders low BL, tumor response and
survival in CRP flare-responders high BL, as well as
non-responders, was low. In patient characteristics of CRP
flare-responders, CRP flare-responders high BL had several poor
prognostic factors; however, CRP flare-response with low BL was a
significantly independent predictive factor associated with
favorable PFS. These results suggest that patients with the CRP
flare-response were an immunologically heterogeneous population. In
patients with mUC who were categorized as CRP flare-responders, the
duration to decrease below BL CRP levels was the predicting factor
associated with efficacy of pembrolizumab (23). CRP BL levels were one of the
biomarkers to classify CRP flare-responders according to ICI
efficacy. In the tumor microenvironment, elevated BL CRP levels
indicated chronic inflammation that causes or contributes to
immunosuppression (33). High CRP
levels induced an immunosuppressive microenvironment (34). Differences in the condition of the
tumor microenvironment might have affected the oncological outcomes
between CRP flare-responders low and high BL.
In this study, no significant association was
observed between the incidence of irAE and the groups stratified by
early CRP kinetics. The relationship between the CRP flare-response
and development of AE has not been fully investigated; only one
study reported no relation between them (23). The association between irAE
development during ICI and favorable oncological outcomes was
reported (35). Additionally,
elevated levels of serum CRP during ICI were associated with the
development of irAEs (36).
Although the number of patients was small in our study, CRP
flare-responders low BL most frequently showed severe irAEs.
Therefore, careful observation performing blood tests or imaging
might be important regarding the occurrence of irAE when patients
with low BL CRP levels showed the CRP flare-response.
Furthermore, 0.32 g/dl was used as the cutoff of CRP
value to further divide CRP flare-responders into two groups in
this study. Several studies reported the usefulness of baseline CRP
value as a biomarker predicting the prognosis in patients with mUC
treated with pembrolizumab, however, various cutoff values were
reported and optimal cutoff value has not been established
(18,19,24–26).
Although we used median as the cutoff value, approximately 0.5 g/dl
was often used and not different from our cutoff value (18,19,24).
Therefore, we believe our cutoff value was acceptable.
This study has several limitations. First, this
study was retrospective; therefore, unavoidable selection biases
and confounders may be included in the results. In fact, the
histologic subtypes or divergent differentiation were more commonly
observed in CRP non-responders comparing to CRP flare-responders
and CRP responders. There are few studies have investigated the
outcomes of systemic therapy for mUC with subtype of UC (SUC),
defined here as UC with any histologic subtype or divergent
differentiation. In patients with mUC treated with systemic
chemotherapy, poor survival was observed in patient with SUC
compared to those with pure UC (37,38).
In contrast, studies investigated in patients with mUC treated with
pembrolizumab reported that the tumor response and survival between
patients with pure UC and patients with SUC were comparable
(39,40). Although the impact on response to
systemic therapies in patients with SUC remains unclear, the
difference of histologic features among the groups may affect the
results in our study. Moreover, we excluded patients who developed
infectious disease within 3 months of pembrolizumab administration
and patients with insufficient data on CRP. However, we believe
there was little impact on the results because only two patients
were excluded in our cohort. Additionally, molecular testing data,
such as expression of programmed cell death ligand 1, and tumor
mutation burden were not investigated. Although these data were
important for investigating factors predicting oncological outcomes
in patients treated with ICI, we could not collect the data because
these immunohistochemical analyses are not covered by national
insurance and cannot be routinely performed in daily practice in
Japan.
In conclusion, patients with mUC who showed the CRP
flare-response demonstrated favorable oncological outcomes,
comparable with CRP responders. Furthermore, CRP levels before
initiation of pembrolizumab could predict oncological outcomes in
CRP flare-responders. Better tumor response and survival were
expected in CRP flare-responders with low BL CRP levels than those
with high BL CRP levels. However, careful follow-ups might be
necessary to detect severe irAEs as early as possible for CRP
flare-responders with low BL CRP levels.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
IT was responsible for conceptualization, data
curation, formal analysis, investigation, methodology, project
administration and writing the original draft. SS, MT, RH, SH, HM
and SA contributed to the study conception and design. MH, SS, MT,
RH, SH, HM, SA, YN and AM were responsible for reviewing the
manuscript and acquisition of data on patient backgrounds, clinical
tests, including CRP levels, AEs and treatment efficacy at each
participating institution. MH, YN and AM were responsible for
interpretation of data and edited the manuscript. KH was
responsible for analysis and interpretation of data, wrote and
edited the manuscript. NF was responsible for analysis and
interpretation of data, supervised the study, and wrote and edited
the manuscript. IT and NF confirm the authenticity of all the raw
data. All authors read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
the University of Occupational and Environmental Health, Japan
(approval no. UOEHCRB20-180), the Ethics Committee of Kokura
Memorial Hospital (approval no. 22092002E), the Ethics Committee of
Munakata Suikokai General Hospital (approval no. 22003), the Ethics
Committee of Shin-kokura Hospital (approval no. 2022-002), the
Ethics Committee of Shin-yukuhashi Hospital (approval no. R3-35),
the Ethics Committee of Kitakyushu City Yahata Hospital (approval
no. 20220510) and the Ethics Committee of Moji Medical Center
(approval no. 04-05). An opt-out approach was used to obtain
informed consent from the patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
AE
|
adverse event
|
|
BL
|
baseline
|
|
BOR
|
best overall response
|
|
CRP
|
C-reactive protein
|
|
ICI
|
immune checkpoint inhibitor
|
|
mUC
|
metastatic and unresectable urothelial
carcinoma
|
|
ORR
|
objective response rate
|
|
OS
|
overall survival
|
|
SUC
|
subtype of urothelial carcinoma
|
|
UC
|
urothelial carcinoma
|
|
PFS
|
progression-free survival
|
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Flaig TW, Spiess PE, Abern M, Agarwal N,
Bangs R, Buyyounouski MK, Chan K, Chang SS, Chang P, Friedlander T,
et al: NCCN guidelines® insights: Bladder cancer,
version 3.2024. J Natl Compr Canc Netw. 22:216–225. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jones RJ, Crabb SJ, Linch M, Birtle AJ,
McGrane J, Enting D, Stevenson R, Liu K, Kularatne B and Hussain
SA: Systemic anticancer therapy for urothelial carcinoma: UK
oncologists' perspective. Br J Cancer. 130:897–907. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
von der Maase H, Sengelov L, Roberts JT,
Ricci S, Dogliotti L, Oliver T, Moore MJ, Zimmermann A and Arning
M: Long-term survival results of a randomized trial comparing
gemcitabine plus cisplatin, with methotrexate, vinblastine,
doxorubicin, plus cisplatin in patients with bladder cancer. J Clin
Oncol. 23:4602–4608. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bellmunt J, de Wit R, Vaughn DJ, Fradet Y,
Lee JL, Fong L, Vogelzang NJ, Climent MA, Petrylak DP, Choueiri TK,
et al: Pembrolizumab as second-line therapy for advanced urothelial
carcinoma. N Engl J Med. 376:1015–1026. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Taguchi S, Kawai T, Nakagawa T, Miyakawa
J, Kishitani K, Sugimoto K, Nakamura Y, Kamei J, Obinata D,
Yamaguchi K, et al: Improved survival in real-world patients with
advanced urothelial carcinoma: A multicenter propensity
score-matched cohort study comparing a period before the
introduction of pembrolizumab (2003-2011) and a more recent period
(2016-2020). Int J Urol. 29:1462–1469. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Balar AV, Castellano DE, Grivas P, Vaughn
DJ, Powles T, Vuky J, Fradet Y, Lee JL, Fong L, Vogelzang NJ, et
al: Efficacy and safety of pembrolizumab in metastatic urothelial
carcinoma: Results from KEYNOTE-045 and KEYNOTE-052 after up to 5
years of follow-up. Ann Oncol. 34:289–299. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bellmunt J, de Wit R, Fradet Y, Climent
MA, Petrylak DP, Lee JL, Fong L, Necchi A, Sternberg CN, O'Donnell
PH, et al: Putative biomarkers of clinical benefit with
pembrolizumab in advanced urothelial cancer: Results from the
KEYNOTE-045 and KEYNOTE-052 landmark trials. Clin Cancer Res.
28:2050–2060. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Park HS, Park JY and Yu R: Relationship of
obesity and visceral adiposity with serum concentrations of CRP,
TNF-alpha and IL-6. Diabetes Res Clin Pract. 69:29–35. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Burger PM, Koudstaal S, Mosterd A, Fiolet
ATL, Teraa M, van der Meer MG, Cramer MJ, Visseren FLJ, Ridker PM
and Dorresteijn JAN; UCC-SMART study group, : C-reactive protein
and risk of incident heart failure in patients with cardiovascular
disease. J Am Coll Cardiol. 82:414–426. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhu M, Ma Z, Zhang X, Hang D, Yin R, Feng
J, Xu L and Shen H: C-reactive protein and cancer risk: A
pan-cancer study of prospective cohort and Mendelian randomization
analysis. BMC Med. 20:3012022. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fernandes JV, Cobucci RN, Jatobá CA,
Fernandes TA, de Azevedo JW and de Araújo JM: The role of the
mediators of inflammation in cancer development. Pathol Oncol Res.
21:527–534. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mosca M, Nigro MC, Pagani R, De Giglio A
and Di Federico A: Neutrophil-to-lymphocyte ratio (NLR) in NSCLC,
gastrointestinal, and other solid tumors: Immunotherapy and beyond.
Biomolecules. 13:18032023. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Proctor MJ, Morrison DS, Talwar D, Balmer
SM, Fletcher CD, O'Reilly DSJ, Foulis AK, Horgan PG and McMillan
DC: A comparison of inflammation-based prognostic scores in
patients with cancer. A glasgow inflammation outcome study. Eur J
Cancer. 47:2633–2641. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Han CL, Meng GX, Ding ZN, Dong ZR, Chen
ZQ, Hong JG, Yan LJ, Liu H, Tian BW, Yang LS, et al: The predictive
potential of the baseline C-reactive protein levels for the
efficiency of immune checkpoint inhibitors in cancer patients: A
systematic review and meta-analysis. Front Immunol. 13:8277882022.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ishihara H, Takagi T, Kondo T, Fukuda H,
Tachibana H, Yoshida K, Iizuka J, Okumi M, Ishida H and Tanabe K:
Predictive impact of an early change in serum C-reactive protein
levels in nivolumab therapy for metastatic renal cell carcinoma.
Urol Oncol. 38:526–532. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kijima T, Yamamoto H, Saito K, Kusuhara S,
Yoshida S, Yokoyama M, Matsuoka Y, Numao N, Sakai Y, Matsubara N,
et al: Early C-reactive protein kinetics predict survival of
patients with advanced urothelial cancer treated with
pembrolizumab. Cancer Immunol Immunother. 70:657–665. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fujiwara M, Yuasa T, Urasaki T, Komai Y,
Fujiwara R, Numao N, Yamamoto S and Yonese J: Effectiveness and
safety profile of pembrolizumab for metastatic urothelial cancer: A
retrospective single-center analysis in Japan. Cancer Rep 4. Cancer
Rep (Hoboken). 4:e13982021. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yamamoto Y, Yatsuda J, Shimokawa M, Fuji
N, Aoki A, Sakano S, Yamamoto M, Suga A, Tei Y, Yoshihiro S, et al:
Prognostic value of pre-treatment risk stratification and
post-treatment neutrophil/lymphocyte ratio change for pembrolizumab
in patients with advanced urothelial carcinoma. Int J Clin Oncol.
26:169–177. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ozawa Y, Amano Y, Kanata K, Hasegwa H,
Matsui T, Kakutani T, Koyauchi T, Tanahashi M, Niwa H, Yokomura K
and Suda T: Impact of early inflammatory cytokine elevation after
commencement of PD-1 inhibitors to predict efficacy in patients
with non-small cell lung cancer. Med Oncol. 36:332019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Fukuda S, Saito K, Yasuda Y, Kijima T,
Yoshida S, Yokoyama M, Ishioka J, Matsuoka Y, Kageyama Y and Fujii
Y: Impact of C-reactive protein flare-response on oncological
outcomes in patients with metastatic renal cell carcinoma treated
with nivolumab. J Immunother Cancer. 9:e0015642021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tomisaki I, Harada M, Tokutsu K, Minato A,
Nagata Y, Kimuro R, Matsumoto M and Fujimoto N: Impact of
C-reactive protein flare response in patients with advanced
urothelial carcinoma who received pembrolizumab. In Vivo.
35:3563–3568. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Klümper N, Sikic D, Saal J, Büttner T,
Goldschmidt F, Jarczyk J, Becker P, Zeuschner P, Weinke M,
Kalogirou C, et al: C-reactive protein flare predicts response to
anti-PD-(L)1 immune checkpoint blockade in metastatic urothelial
carcinoma. Eur J Cancer. 167:13–22. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yasuoka S, Yuasa T, Nishimura N, Ogawa M,
Komai Y, Numao N, Yamamoto S, Kondo Y and Yonese J: Initial
experience of pembrolizumab therapy in japanese patients with
metastatic urothelial cancer. Anticancer Res. 39:3887–3892. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nagasaka H, Yamamoto S, Suzuki A, Usui K,
Terao H, Nakaigawa N and Kishida T: C-reactive protein is a
prognostic factor for survival in metastatic upper tract urothelial
carcinoma patients receiving pembrolizumab. In Vivo. 38:1823–1828.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tamura D, Jinnouchi N, Abe M, Ikarashi D,
Matsuura T, Kato R, Maekawa S, Kato Y, Kanehira M, Trakata R and
Obara W: Prognostic outcomes and safety in patients treated with
pembrolizumab for advanced urothelial carcinoma: Experience in
real-world clinical practice. Int J Clin Oncol. 25:899–905. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kanda Y: Investigation of the freely
available easy-to-use software ‘EZR’ for medical statistics. Bone
Marrow Transplant. 48:452–458. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hoeh B, Garcia CC, Banek S, Klümper N, Cox
A, Ellinger J, Schmucker P, Hahn O, Mattigk A, Zengerling F, et al:
Early CRP kinetics to predict long-term efficacy of first-line
immune-checkpoint inhibition combination therapies in metastatic
renal cell carcinoma: An updated multicentre real-world experience
applying different CRP kinetics definitions. Clin Transl
Immunology. 12:e14712023. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Klümper N, Saal J, Berner F,
Lichtensteiger C, Wyss N, Heine A, Bauernfeind FG, Ellinger J,
Brossart P, Diem S, et al: C reactive protein flare predicts
response to checkpoint inhibitor treatment in non-small cell lung
cancer. J Immunother Cancer. 10:e0040242022. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Saal J, Bald T, Eckstein M, Ritter M,
Brossart P, Ellinger J, Hölzel M and Klümper N: Early C-reactive
protein kinetics predicts immunotherapy response in non-small cell
lung cancer in the phase III OAK trial. JNCI Cancer Spectr.
7:pkad0272023. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Qin Q, Kou X, Zheng Y, Zhou F, Zhang X and
Liu H: Early C-reactive protein kinetics predict response to immune
checkpoint blockade in unresectable hepatocellular carcinoma. J
Hepatocell Carcinoma. 10:2009–2019. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Haas M, Lein A, Fuereder T, Schnoell J,
Brkic FF, Liu DT, Kadletz-Wanke L, Heiduschka G and Jank BJ: Early
on-treatment C-reactive protein and its kinetics predict survival
and response in recurrent and/or metastatic head and neck cancer
patients receiving first-line pembrolizumab. Invest New Drugs.
41:727–736. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Nakayama T, Saito K, Kumagai J, Nakajima
Y, Kijima T, Yoshida S, Kihara K and Fujii Y: Higher serum
C-reactive protein level represents the immunosuppressive tumor
microenvironment in patients with clear cell renal cell carcinoma.
Clin Genitourin Cancer. 16:e1151–e1158. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Yoshida T, Ichikawa J, Giuroiu I, Laino
AS, Hao Y, Krogsgaard M, Vassallo M, Woods DM, Stephen Hodi F and
Weber J: C reactive protein impairs adaptive immunity in immune
cells of patients with melanoma. J Immunother Cancer.
8:e0002342020. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Hussaini S, Chehade R, Boldt RG, Raphael
J, Blanchette P, Maleki Vareki S and Fernandes R: Association
between immune-related side effects and efficacy and benefit of
immune checkpoint inhibitors-a systematic review and meta-analysis.
Cancer Treat Rev. 92:1021342021. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Abolhassani AR, Schuler G, Kirchberger MC
and Heinzerling L: C-reactive protein as an early marker of
immune-related adverse events. J Cancer Res Clin Oncol.
145:2625–2631. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Hsieh MC, Sung MT, Chiang PH, Huang CH,
Tang Y and Su YL: The prognostic impact of histopathological
variants in patients with advanced urothelial carcinoma. PLoS One.
10:e01292682015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Minato A, Murooka K, Okumura Y, Takaba T,
Higashijima K, Nagata Y, Tomisaki I, Harada K and Fujimoto N:
Efficacy of platinum-based chemotherapy in patients with metastatic
urothelial carcinoma with variant histology. In Vivo. 38:873–880.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Kobayashi M, Narita S, Matsui Y, Kanda S,
Hidaka Y, Abe H, Tsuzuki T, Ito K, Kojima T, Kato M, et al: Impact
of histological variants on outcomes in patients with urothelial
carcinoma treated with pembrolizumab: A propensity score matching
analysis. BJU Int. 130:226–234. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Minato A, Furubayashi N, Harada M, Negishi
T, Sakamoto N, Song Y, Hori Y, Tomoda T, Tamura S, Kuroiwa K, et
al: Efficacy of pembrolizumab in patients with variant urothelial
carcinoma: A multicenter retrospective study. Clin Genitourin
Cancer. 20:499.e1–499.e8. 2022. View Article : Google Scholar : PubMed/NCBI
|