Introduction
According to global cancer statistics for 2022,
Liver cancer is the sixth most commonly diagnosed cancer worldwide
and the third leading cause of cancer-associated mortalities
(1). In 2022, ~860,000 new cases
and 750,000 mortalities were reported globally (1). The prevalence of liver cancer is
higher in regions such as East Asia and South Africa (1). Hepatocellular carcinoma (HCC) accounts
for ~75% of all primary liver cancer cases (2), with 70–80% of patients being diagnosed
at an advanced stage, often with large size tumors and concomitant
poor liver function. Among these cases, the incidence of portal
vein tumor thrombus (PVTT) ranges between 13 and 45% (3,4), and
these patients face the poorest prognosis, often developing severe
complications such as portal hypertension, hepatocellular jaundice
and refractory ascites (5). The
median survival time for patients with HCC and PVTT who receive
only supportive care is 2.7 months (5).
Currently, the optimal treatment strategy for
technically resectable HCC with PVTT remains a subject of debate.
Both the European Association for the Study of the Liver and the
American Association for the Study of Liver Diseases recommend the
Barcelona Clinic Liver Cancer (BCLC) staging system for managing
and prognosticating HCC (6).
According to this system, patients with HCC and PVTT are classified
as advanced (BCLC stage C) and are eligible only for palliative
systemic treatment (6). However,
treatment guidelines have been updated across various regions,
including mainland China (7), Hong
Kong (8) and Japan (9). Portal vein invasion does not preclude
surgical resection, which has been shown to markedly improve the
survival of patients with HCC and PVTT (10). Notably, the surgical mortality rate
for these cases remains <10% (11). A study from Japan have indicated
that the median survival time for patients undergoing surgical
removal of PVTT ranges between 8 and 22 months, with 1-year overall
survival (OS) rates varying between 21.7 and 69.6% (11).
Neoadjuvant therapies, including radiotherapy
(12), chemotherapy (13), immunotherapy (14), targeted therapy (15) and interventional therapy (16), have gained attention for treatment
of HCC. Advocates of neoadjuvant therapy argue that it can help
manage small metastatic lesions, reduce the preoperative tumor
burden, lower recurrence rates and improve OS. Additionally,
neoadjuvant therapies for tumor downstaging are often characterized
by a relatively short treatment duration and high patient
compliance (17). On the other
hand, some experts recommend surgical resection as the preferred
treatment for HCC with isolated PVTT, due to the fact that surgery
typically results in improved preservation of liver function
compared with non-surgical approaches (18). In light of the ongoing debate
surrounding neoadjuvant therapy, the present study aimed to perform
a meta-analysis of the available literature to evaluate the
efficacy and safety of neoadjuvant therapy for the treatment of
resectable HCC with PVTT.
Materials and methods
Search strategy
The present meta-analysis was conducted in
accordance with the Preferred Reporting Items for Systematic
Reviews and Meta-Analyses (PRISMA) guidelines. The present study
was registered with the International Prospective Register of
Systematic Reviews (19) (ID no.
CRD42024539943). A comprehensive literature search was performed
across multiple databases, including PubMed
(pubmed.ncbi.nlm.nih.gov/), Web of Science
(webofscience.clarivate.cn/wos/alldb/basic-search), Embase
(https://www.embase.com/) and the Cochrane Library
(cochranelibrary.com/?contentLanguage=eng), covering studies from
inception to September 2024. Additional relevant studies were
identified through manual searches of reference lists and Google
Scholar (scholar.nq69.top/). The search strategy incorporated a
combination of Medical Subject Headings (MeSH) and free-text terms,
including ‘neoadjuvant chemotherapy’ (MeSH), ‘neoadjuvant
radiation’ (MeSH), ‘neoadjuvant therapies’ (MeSH), ‘neoadjuvant
chemoradiotherapy’ (MeSH), ‘interventional therapy’, ‘targeted
therapy’, ‘immunotherapy’, ‘hepatocellular carcinoma’, ‘HCC’,
‘portal vein thrombosis’ and ‘PVTT’ (Supplementary Search
Strategy).
Inclusion and exclusion criteria
The inclusion criteria for studies were as follows:
i) Patients were diagnosed with HCC and PVTT; ii) neoadjuvant
therapy administered prior to hepatectomy in the experimental
group, while the control group underwent hepatectomy as the initial
intervention; iii) the primary outcomes assessed were OS and
relapse-free survival (RFS); and iv) the study design included
randomized controlled trials (RCTs), cohort studies or case-control
studies. Studies were excluded based on the following criteria: i)
Inability to extract data; ii) unavailability of the full text;
iii) duplication of data from the same cohort; in such cases, the
most comprehensive or recent study was selected (when article is
equally comprehensive and there is no data update and sample size
increases, the latest literature is preferred; iv) non-English
language publications; and v) no interesting outcomes.
Data extraction and quality
evaluation
Data extraction was independently performed by two
authors using a standardized form to collect relevant information,
including basic details (author names, country, year of recruitment
and year of publication) and clinical data (number of patients,
age, sex, neoadjuvant therapy regimen, follow-up duration, PVTT
classification and complications). Any discrepancies between the
authors were resolved through discussion and reevaluation of the
literature. The quality of cohort and case-control studies was
assessed using the Newcastle-Ottawa Scale (NOS) (20). Studies were classified as high
quality (scores 8–9), moderate quality (scores 6–7) or low quality
(scores <6). Only studies with a score of ≥6 were included in
the analysis. For RCTs, the risk of bias was evaluated using the
Cochrane Handbook's criteria (21)
and the Cochrane Collaboration tool (RoB2). Factors such as random
sequence generation, allocation concealment, subject and personnel
blinding, outcome assessment blinding, incomplete outcome data,
selective reporting and other potential bias were assessed.
Statistical analysis
Statistical analyses were conducted using Stata
version 12.0 (StataCorp LLC). The association between neoadjuvant
therapy and long-term prognosis in HCC with PVTT was evaluated
using hazard ratios (HRs) and 95% CIs. A HR <1 indicated a
benefit for the experimental group, while a HR >1 favored the
control group. Postoperative complications were analyzed using odds
ratios (ORs) for dichotomous variables and mean differences (MDs)
in the case of continuous variables, both with corresponding 95%
CIs. Heterogeneity among the studies was assessed using the
χ2 test and expressed as I2. An I2
value >50% was indicative of substantial heterogeneity, whereas
an I2 value of <50% indicated low heterogeneity. A
random-effects model was applied to account for variability in
treatment regimens, inclusion criteria and study designs. If the
number of included articles was insufficient, the test's efficiency
was considered low, in accordance with previous meta-analyses
(22–24). All statistical tests were two-sided.
P<0.05 was considered to indicate a statistically significant
difference.
Results
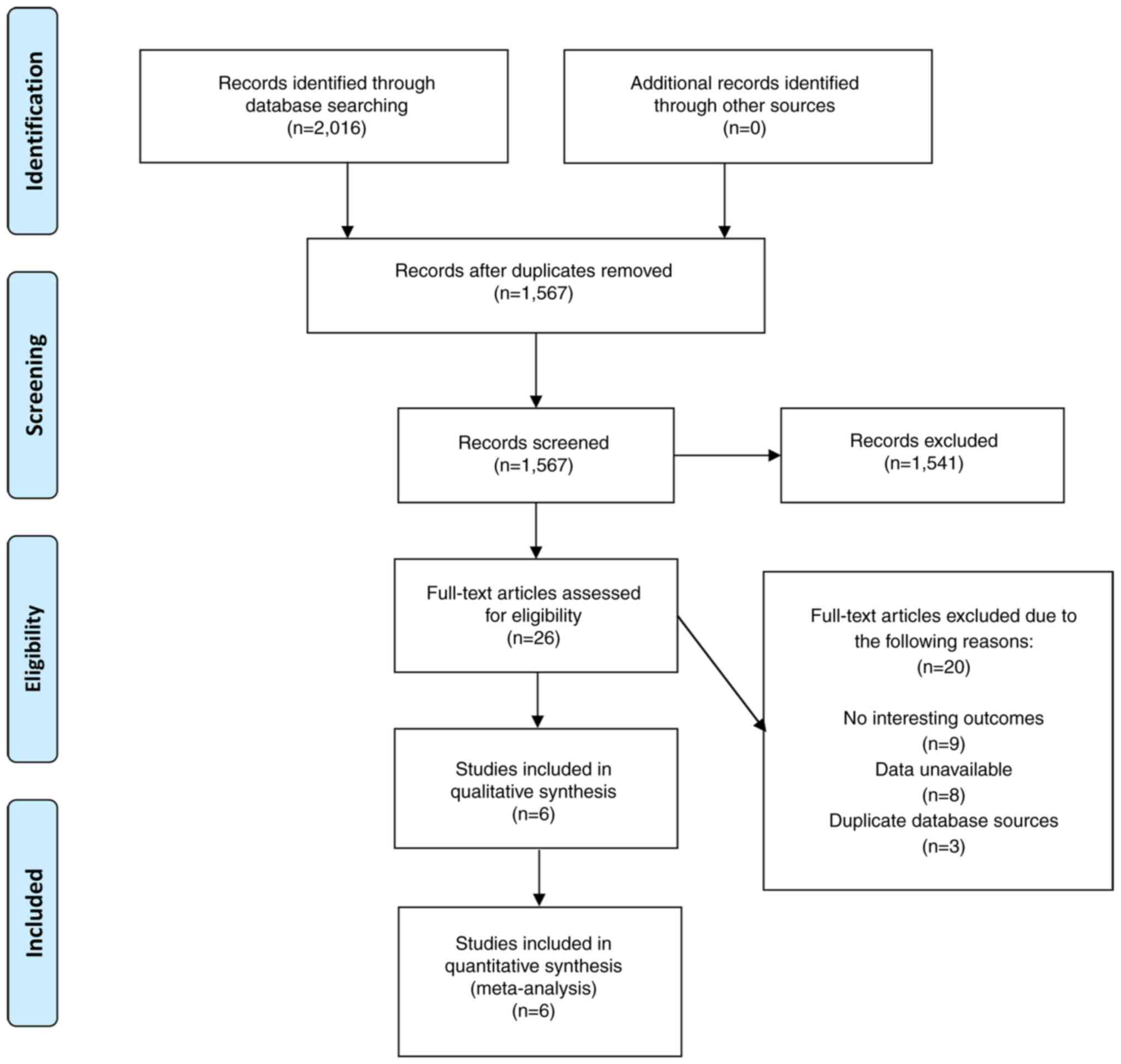
Study selection
A total of 2,016 related literatures were generated
in the initial electronic database and manual retrieval. The titles
and abstracts of 1567 non-duplicate articles were screened, and
1541 records were further excluded. The including 26 articles were
read in full text, and 20 were excluded due to no interesting
outcomes (n=9), unavailability of data (n=8), and data source
duplication (n=3). Ultimately, six studies (25–30)
were selected for inclusion in the meta-analysis. A detailed PRISMA
flowchart illustrating the study selection process is shown in
Fig. 1.
Study characteristics
The six selected studies, published between 2007 and
2023, included one RCT (25), one
case-control study (26) and four
cohort studies (27–30), encompassing a total of 750 patients
with HCC and PVTT. Of these, 312 patients received neoadjuvant
therapy, while 438 patients were included in the control group,
undergoing various treatments such as radiotherapy, chemotherapy
and interventional therapy. The majority of patients (84–100%) had
preserved liver function and were classified as Child-Pugh grade A
(Table SI) (31). Detailed characteristics of the
included studies are presented in Tables I and SI.
 | Table I.Characteristics of all the studies
included in the meta-analysis. |
Table I.
Characteristics of all the studies
included in the meta-analysis.
|
|
|
| Patient
numbers |
|
| Mean follow-up
period, months |
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|---|
| First author/s,
year | Country | Cohort years | EG | CG | Neoadjuvant therapy
regimen | PVTT
classification | EG | CG | Study design | (Refs.) |
|---|
| Kamiyama et
al, 2007 | Japan | 1990-2006 | 15 | 28 | RT | NA | 83 |
| Cohort study | (27) |
| Li et al,
2016 | China | 2010-2013 | 39 | 50 | 3D-CRT | Type III | 8.4 |
| Cohort study | (28) |
| Zhang et al,
2016 | China | 2006-2011 | 85 | 205 | TACE | Mixed-type | NA |
| Cohort study | (29) |
| Chong et al,
2018 | South Korea | 2005-2014 | 26 | 18 | CCRT + HAIC | Type II/type
III | 13 |
| Cohort study | (30) |
| Wei et al,
2019 | China | 2016-2017 | 82 | 82 | RT | Type II/type
III | 15.2 | 10.8 | RCT | (25) |
| Hu et al,
2023 | China | 2017-2021 | 65 | 55 | HAIC | Mixed-type | 33.8 | 38.7 | Case-control
study | (26) |
Methodological quality of the included
studies
The quality of the RCT was evaluated using the
Cochrane Collaboration tool (RoB2) (21), which identified a high risk of bias
due to the absence of blinding, given the nature of the
interventions (Table SII). In
addition, one study (25) also
excluded patients with hepatitis C virus-related HCC, potentially
introducing biases related to differing surgical indications across
centers. The observational studies were assessed using the NOS
(20), with all studies rated as
moderate to high quality, scoring at least 6 out of 9 points.
Propensity score matching (PSM) is applied in a case-control study
(26) to eliminate bias from
gender, age, body mass index. The appropriate design of the
experimental and control groups provides better comparisons.
Scoring of outcomes is according to the sufficient description. For
cohort studies, the differences in sample size, surgeons, and
operative procedures decrease comparability. To address this issue,
some studies have used methods such as using the same surgical
protocol for patients (28).
Absence of a statement describing the follow-up results in a score
of 0 for the section. Further details are provided in Tables SII and SIII.
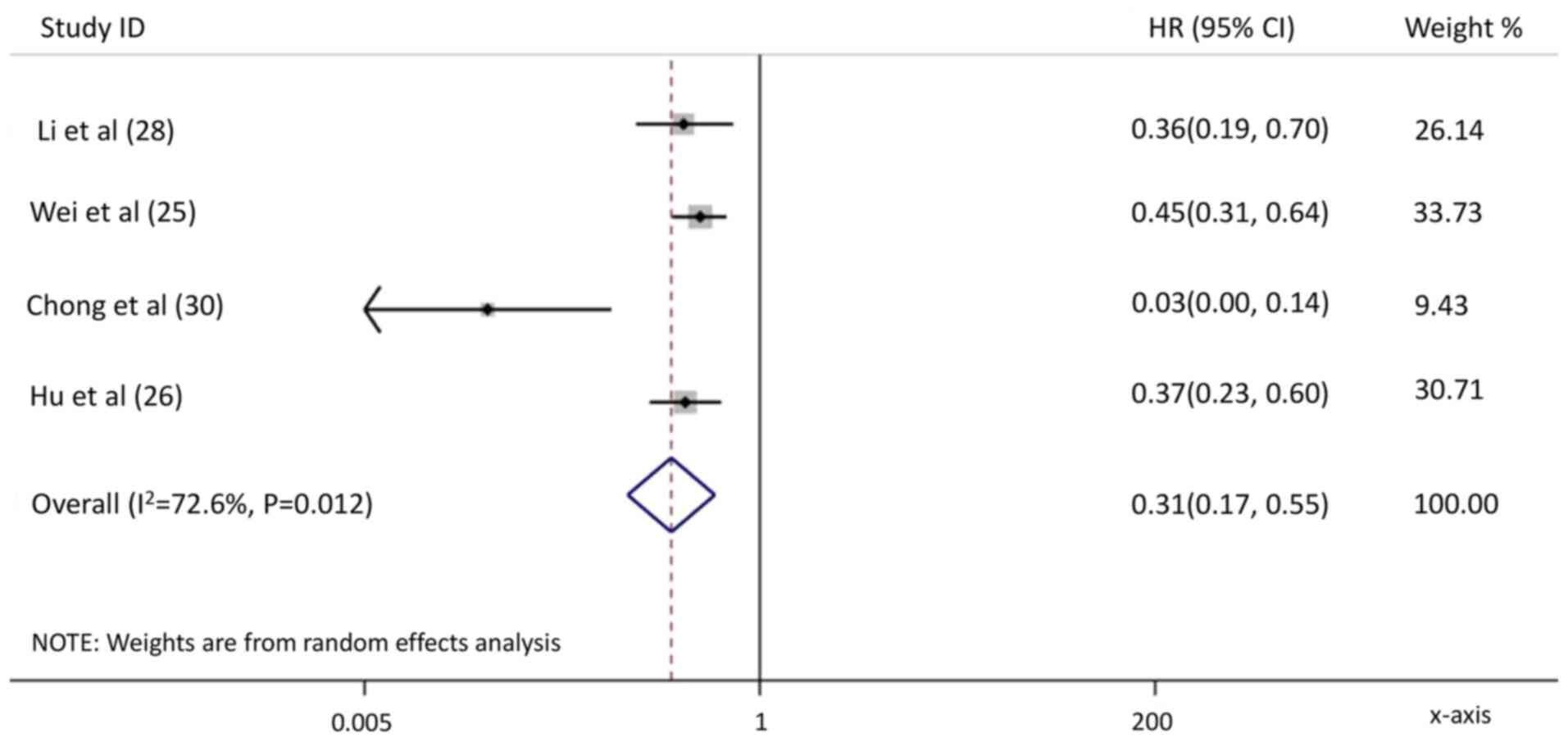
RFS and OS
RFS data were reported in four studies (25,26,28,30),
involving 417 patients. The neoadjuvant therapy group demonstrated
significantly higher RFS compared with the control group (HR, 0.31;
95% CI, 0.17–0.55; P<0.001; Fig.
2), although the heterogeneity was substantial
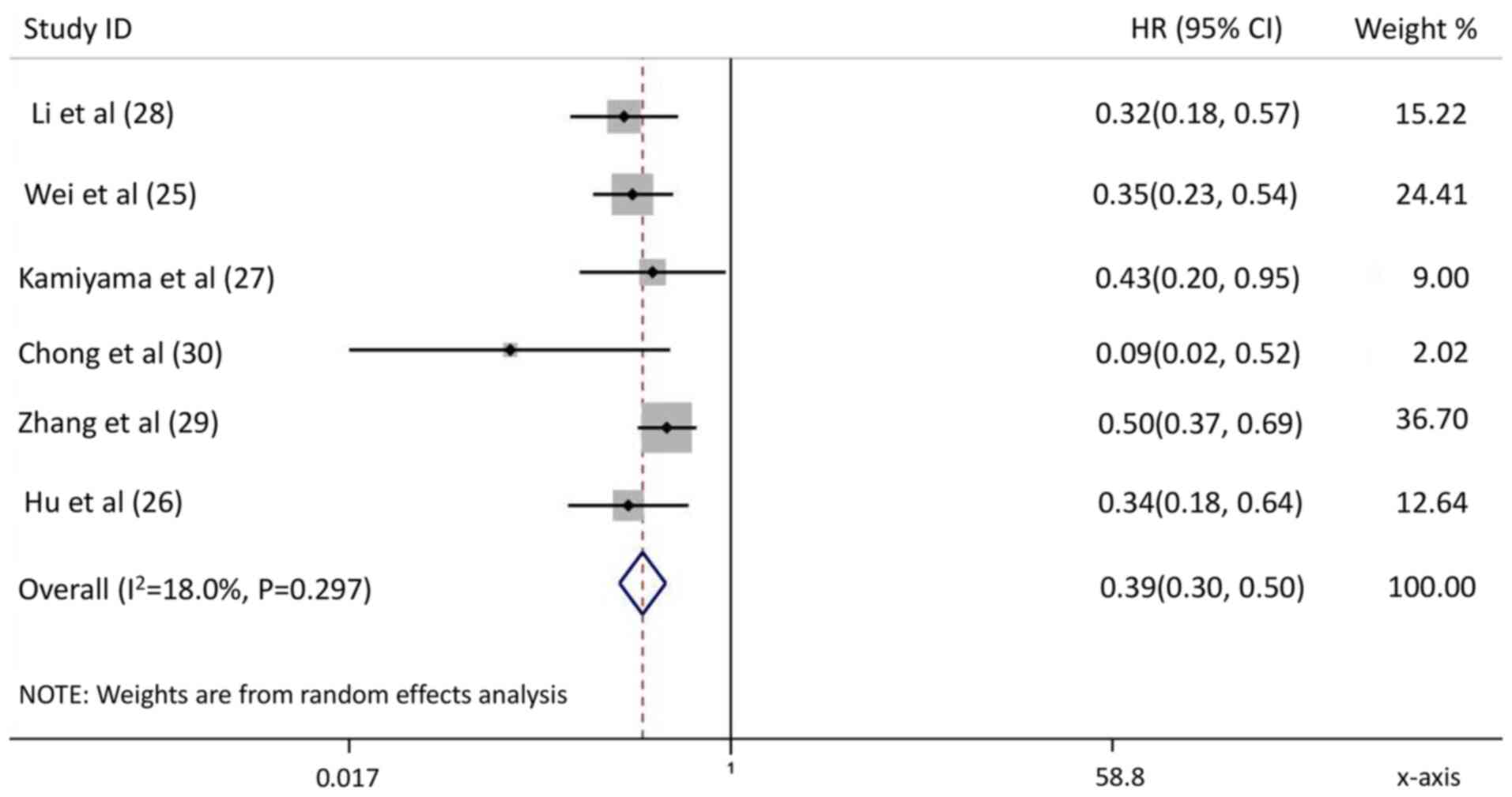
(I2=72.6%). The OS data from six studies (25–30)
indicated that the neoadjuvant therapy group had a markedly
improved OS compared with the control group (HR, 0.39; 95% CI,
0.30–0.50; P<0.001; I2=18.0%; Fig. 3).
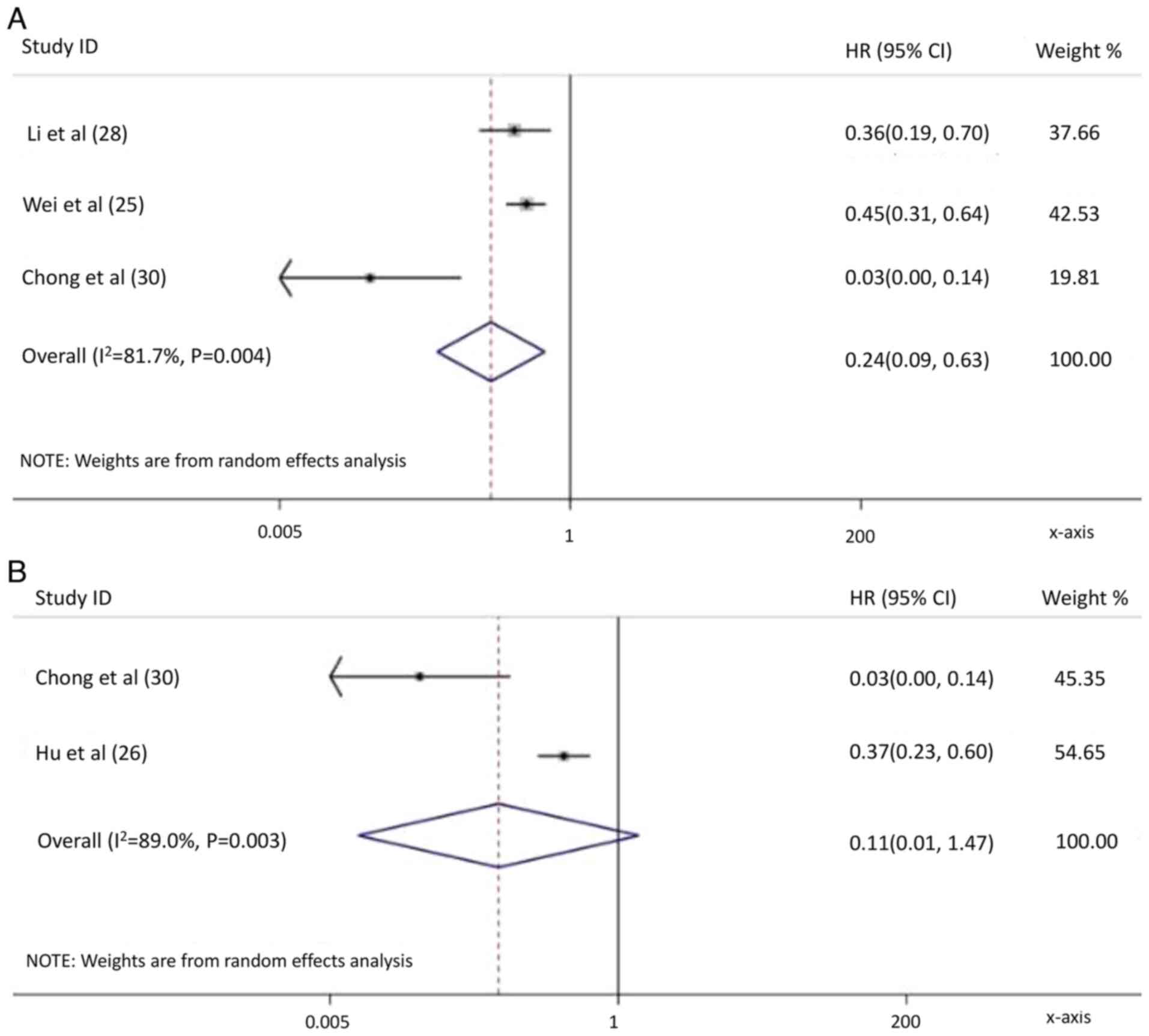
Subgroup analysis
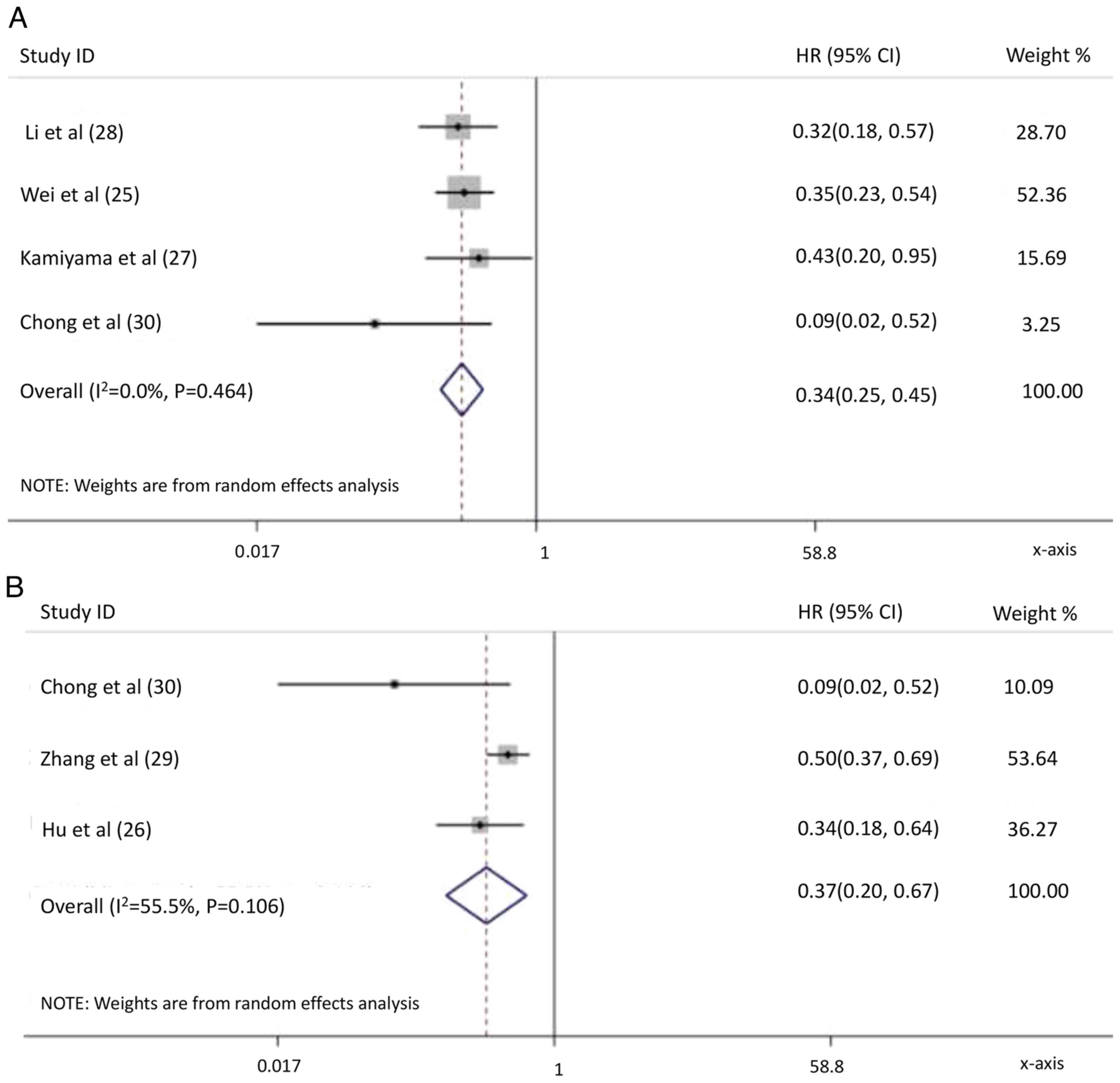
In the subgroup analysis, patients receiving
neoadjuvant radiotherapy exhibited improved RFS compared with
control group (HR, 0.24; P=0.004; Fig.
4A). However, no significant difference in RFS was observed in
the broader neoadjuvant intervention group (HR, 0.11; P=0.095;
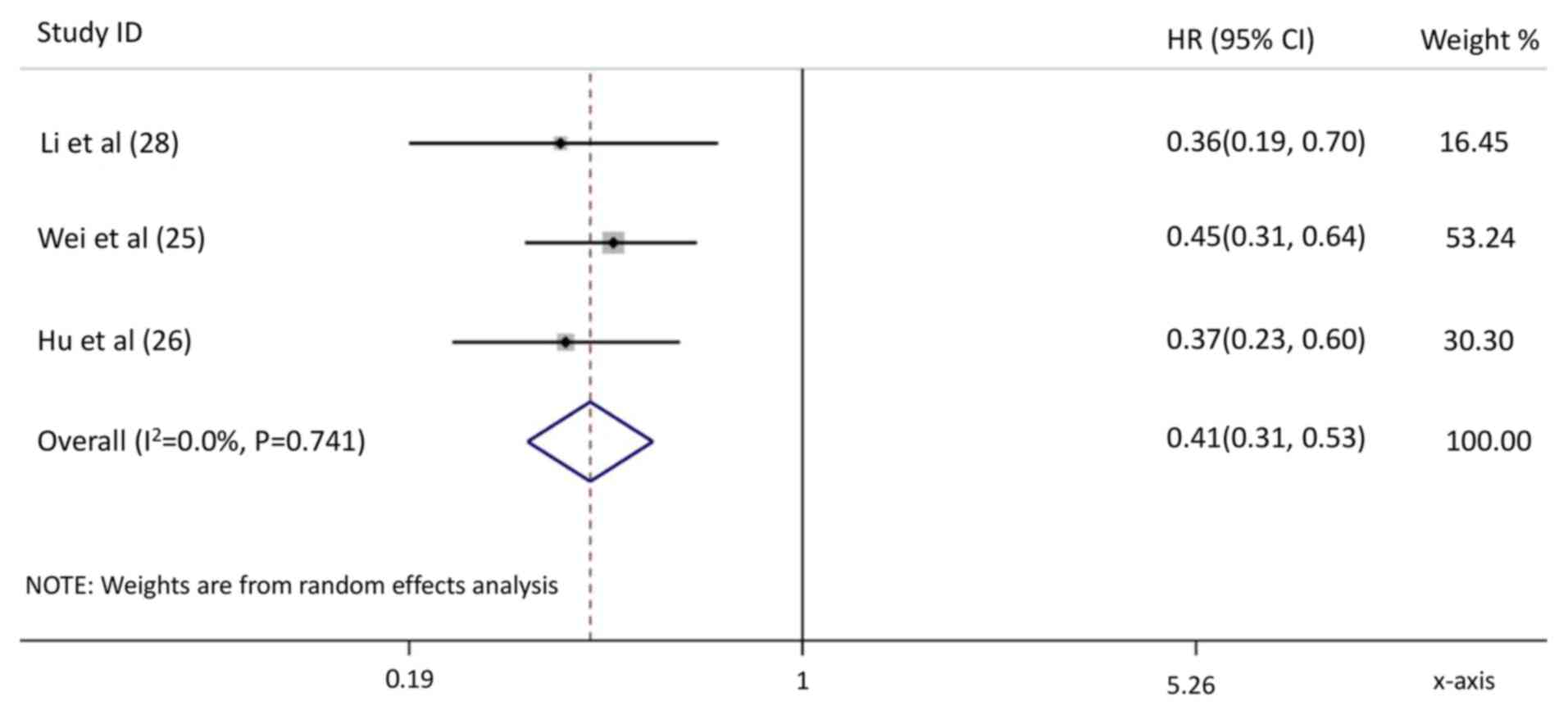
Fig. 4B). In the Chinese subgroup,
neoadjuvant therapy significantly improved RFS (HR, 0.41;
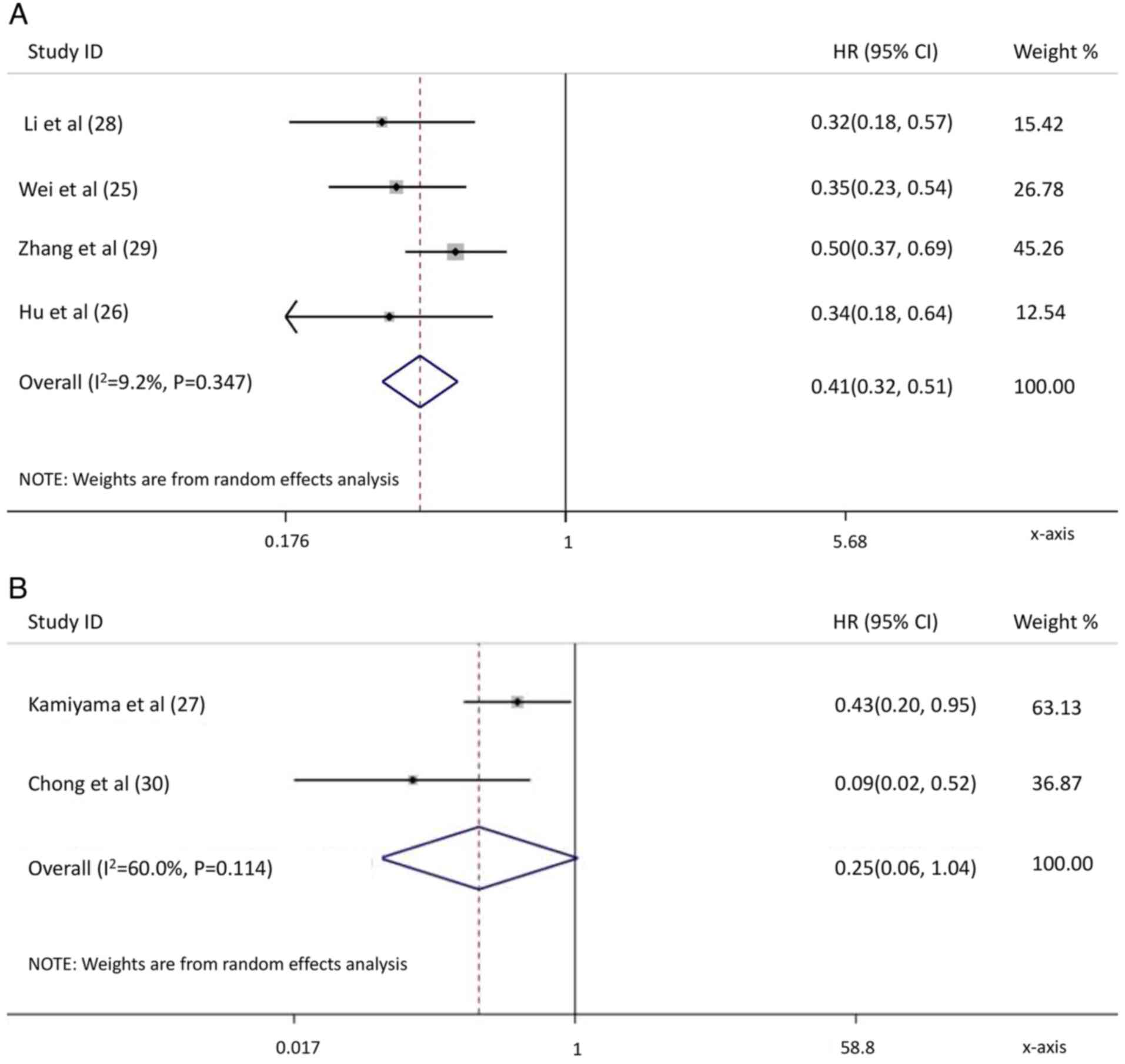
P<0.001; Fig. 5). Regarding OS,
both the neoadjuvant radiotherapy group (HR, 0.34; P<0.001;
Fig. 6A) and the neoadjuvant
intervention group (HR, 0.37; P=0.001; Fig. 6B) outperformed the control group.
Neoadjuvant therapy in the Chinese subgroup also showed a
significant OS advantage compared with the control group (HR, 0.41;
P<0.001; Fig. 7A). In other
regions such as Japan and South Korea, there was no significant
difference in OS between the neoadjuvant group and the control
group (HR, 0.25; P=0.057; Fig.
7B).
Analysis of postoperative
complications
A comparative analysis of perioperative
complications, including intraoperative blood transfusion, blood
loss, operative time, bile leakage, ascites, peritoneal infection,
postoperative hemorrhage, complications and mortality, revealed no
significant differences between the neoadjuvant therapy and control
groups (all P>0.05; Table
II).
| Table II.Subgroup analysis of postoperative
complications. |
Table II.
Subgroup analysis of postoperative
complications.
| Complication | No. of studies | OR/MD (95% CI) | P-value | I2,
% |
|---|
| No. of blood
transfusions | 4 | 1.44 (0.85,
2.43)a | 0.18 | 28 |
| Operative blood
loss, ml | 4 | 83.60 (−149.43,
316.62)b | 0.48 | 53 |
| Operation time,
min | 3 | 14.76 (−7.14,
36.66)b | 0.19 | 82 |
| Bile leakage | 2 | 1.11 (0.27,
4.48)a | 0.89 | 0 |
| Ascites pleural
effusion | 2 | 0.91 (0.19,
4.35)a | 0.91 | 50 |
| Intra-abdominal
infection | 2 | 0.43 (0.12,
1.60)a | 0.21 | 0 |
| Postoperative
hemorrhage | 2 | 1.90 (0.64,
5.64)a | 0.25 | 0 |
| Postoperative
complications | 4 | 1.72 (0.90,
3.28)a | 0.10 | 55 |
| Mortality | 3 | 0.74 (0.20,
2.82)a | 0.66 | 0 |
Sensitivity analysis and publication
bias
Sensitivity analysis and Begg's weighted regression
test for detecting potential publication bias are typically
suitable for meta-analyses including >10 studies (23). Given the limited number of studies
in the present analysis, these tests were not performed.
Discussion
HCC is classified using various staging systems,
with the BCLC staging system (32)
being the most widely adopted. Under this system, patients with HCC
and PVTT are categorized as stage C (33). In a number of Western medical
systems, including the United States, any degree of vascular
invasion has traditionally been considered a contraindication for
surgical intervention (34).
However, the 2022 updated BCLC guidelines recommend
atezolizumab-bevacizumab as the first-line treatment for these
patients (35).
In contrast to Western practices, vascular invasion,
whether in the portal vein, hepatic vein or with extrahepatic
metastasis, does not universally preclude surgical resection in HCC
management (36). Several surgical
centers in Asia have reported favorable clinical outcomes for
patients with technically resectable BCLC stage C HCC (36,37).
For instance, a national multicenter study in Japan conducted by
Kokudo et al (38) revealed
that hepatectomy in patients with PVTT confined to the primary or
peripheral branches markedly extended the median survival by 1.77
years compared with non-surgical management. These findings suggest
that hepatectomy may be a viable option for treating HCC with PVTT
in carefully selected cases.
While surgical resection offers a potentially
curative approach for HCC with PVTT, its effectiveness is limited
by several critical factors. Surgical resection is primarily
feasible for patients with type I/II PVTT, where prognosis is
comparatively more favorable, with 5-year OS rates ranging between
10 and 59% (39). By contrast, for
patients with type III/IV PVTT, the prognosis is worse, with
survival rates dropping to 0–26% (39). Additionally, hepatic resection is
only possible under specific conditions, such as a performance
status grade of 0–2, Child-Pugh grade A or sufficient liver
reserve, which restricts the number of eligible patients (40,41).
Furthermore, hepatectomy is associated with considerable trauma and
carries the risk of severe complications, particularly in cases of
advanced HCC with metastasis. In such cases, resecting the primary
tumor often does little to improve survival due to the high
likelihood of recurrence (42). A
clinical trial involving 47 patients with advanced HCC underscored
this issue, reporting 40 fatalities, 37 of which were due to tumor
recurrence (43). Furthermore, when
PVTT extends to the main, left or right branches of the portal
vein, the complexity of the surgery increases substantially,
leading to worse postoperative survival outcomes (44).
Due to these limitations, there is a growing
emphasis on multimodal combination therapies to improve long-term
survival in these patients, including
neoadjuvant/adjuvant/downstaging therapy for surgery and the
combined modality of non-operative therapies (45). The present literature analysis aimed
to evaluate whether combining neoadjuvant therapy with hepatectomy
is associated with improved prognostic outcomes compared with
priority surgery. Data from Eastern countries indicated that
integrating neoadjuvant therapy with surgery offers a survival
advantage over prioritizing surgery as the sole treatment.
Neoadjuvant therapy, including radiotherapy and
interventional therapy, improves the prognosis of patients with HCC
and PVTT when combined with hepatectomy. Neoadjuvant radiotherapy
can effectively downstage PVTT, expanding the pool of patients
eligible for surgical intervention and increasing the success rate
of surgeries (25–30). A pivotal study (46) reported a 5-year survival rate of 57%
for patients who underwent salvage surgery following the
downstaging of initially unresectable HCC, which compares favorably
to that in patients who underwent liver resection when they first
presented with resectable tumors, demonstrating notable improvement
in long-term outcomes.
By alleviating the adverse effects of PVTT on the
blood supply of the hepatic portal vein, which is crucial for
maintaining liver function, neoadjuvant radiotherapy prevents tumor
cell dissemination into surrounding liver tissues, thereby reducing
the risk of intrahepatic and extrahepatic metastases (47–51).
This approach utilizes a targeted radiation dose that is markedly
lower than that used in adjuvant therapies, minimizing damage to
the liver while focusing primarily on the tumor thrombus (52). Furthermore, the use of low-dose
radiation, critical for ensuring both surgical safety and efficacy,
is effective in lowering HCC-related mortality and recurrence
rates, while concurrently preserving liver function and capacity
(25).
By reducing the size and extent of PVTT, neoadjuvant
therapy decreases the risk of tumor dissemination during
hepatectomy (25). This is
especially crucial when the thrombus extends into major portal
branches, facilitating a more comprehensive resection of cancerous
tissue and lowering the risk of postoperative recurrence (12). Neoadjuvant radiotherapy can markedly
increase surgical margins. For instance, one study demonstrated
that the median surgical margin increased from 0 to 1 cm, with the
addition of neoadjuvant intensity modulated radiation therapy
(IMRT), making nearly half of previously unresectable lesions
suitable for surgery (53). This
suggests neoadjuvant IMRT may be associated with improved OS by
increasing the R0 resection rate. This improvement not only
enhances the likelihood of achieving a complete resection but also
reduces the incidence of positive surgical margins, thereby
improving OS outcomes for patients (12).
In addition to neoadjuvant radiotherapy,
interventional therapies such as transcatheter arterial
chemoembolization (TACE) serve a pivotal role in the management of
liver cancer, particularly in intermediate to advanced stages of
HCC (54). TACE, including its
variants conventional TACE and drug-eluting beads TACE, targets the
hepatic artery, the primary vascular supply for both HCC and
PVTT.TACE refers to injection of selective vascular embolization
with chemotherapy drugs into the tumor-feeding arteries to prevent
its nutrition and blood supplying, thereby leading to ischemic
necrosis of the targeted tumor (55). TACE improves survival rates in
patients with all types of PVTT compared with those of patients
receiving conservative treatment (56).
Another advanced interventional option, hepatic
arterial infusion chemotherapy (HAIC), offers a more consistent and
targeted delivery of chemotherapeutic agents directly to the tumor.
HAIC is particularly beneficial for patients with significant
arterial-portal shunts or complete portal vein obstruction,
maximizing therapeutic efficacy while minimizing systemic side
effects (57). A study performed by
Hatooka et al (58)
demonstrated that HAIC achieved notable disease control and
objective response rates of 79.9 and 25.4%, respectively. These
interventional strategies underscore the evolving landscape of
neoadjuvant therapies, affirming their role in improving the
long-term prognosis of patients with advanced HCC.
In the present study, compared with the control
group (priority hepatectomy group), neoadjuvant therapy was
associated with a survival advantage across the Chinese, Japanese
and Korean subgroups; however, the survival benefits did not reach
statistical significance in the Japanese and Korean groups. The
pronounced effects observed in the Chinese subgroup can be
attributed to the substantial representation of Chinese cases,
reflecting the broader epidemiological reality, as China accounts
for ~50% of the global HCC incidence (59), with PVTT prevalence rates between 44
and 62% (5). Since 1995, Chinese
medical institutions have increasingly adopted the associating
liver partition and portal vein ligation for staged hepatectomy
procedure for managing large HCCs, leading to improvements in 1-,
3- and 5-year OS rates compared with earlier decades (60). This surgical approach has
transitioned numerous patients from being considered inoperable to
operable, enhancing treatment outcomes beyond palliative care
(46,60). Additionally, experienced surgical
teams in China have managed to reduce 30-day mortality rates to
2.7%, notably below the global average of 5–10% (61), highlighting the critical role of
surgical expertise in improving these outcomes. In the present
study, the efficacy of interventional therapies, particularly
regarding RFS, remains inconclusive, potentially due to the limited
sample size.
Another concern is the impact of neoadjuvant therapy
on liver function and the associated risks. Preoperative
interventions, including TACE, have been scrutinized for potential
adverse effects, including hepatic artery injury, on-target
embolization, fever and decreased immune function, all of which
could compromise postoperative recovery (62). For example, an RCT by Zhou et
al (63) indicated that while
preoperative TACE did not improve mortality or tumor recurrence
rates, it increased the complexity and duration of surgical
procedures and elevated the risk of postoperative liver failure.
Similarly, another study highlighted that preoperative targeted
immunotherapy raised the risk of severe biliary complications
(64). However, data from other
studies, including those by Hu et al (26) and Zhang et al (29), suggest that neoadjuvant TACE did not
exacerbate postoperative complications, affirming its safety when
performed in experienced clinical settings. The present
comprehensive statistical analysis supports these findings, showing
no significant increase in complications such as bile leakage or
ascites, thereby confirming the overall safety profile of
neoadjuvant therapy in the surgical management of HCC with
PVTT.
The present meta-analysis systematically and
comprehensively evaluated the efficacy and safety of neoadjuvant
therapy in patients with HCC complicated by PVTT, suggesting that
neoadjuvant therapy represents a viable alternative treatment
modality. A total of four previous meta-analyses (65–68)
have assessed the efficacy of adjuvant therapies (in single or
combined modalities) in patients with HCC and PVTT. A key
distinction between these studies and the present study lies in the
inclusion criteria. In three network meta-analyses (65–67),
the experimental groups consisted of patients receiving adjuvant
therapy (single or combined), and these studies comprehensively
compared the benefits and safety of various treatment methods for
patients with HCC and PVTT. In another study (68), only seven of the included articles
focused on comparative studies of adjuvant therapy, which was
administered either before or after surgery.
By contrast, the present study strictly limited the
experimental and control groups to neoadjuvant therapy plus surgery
vs. priority surgery, providing novel insights into the comparative
prognosis and safety of these two approaches, an aspect not
addressed in previous studies. For patients with HCC and PVTT, only
a select few undergo radical surgery; however, the findings of the
present study suggested that surgery following neoadjuvant therapy
yielded superior outcomes compared with priority surgery. This
expands the candidate pool for radical surgery, representing a
significant and core contribution of the present research.
Neoadjuvant therapy combined with surgery not only improved patient
survival rates and reduced recurrence but was also safe.
Additionally, the present study conducted a subgroup analysis based
on the type of neoadjuvant therapy, which has not been performed in
similar studies.
The classification of PVTT influences the outcomes
of neoadjuvant therapy (69), and
future studies should take this into consideration. However,
several limitations of the present study warrant emphasis. Firstly,
the number of included studies was limited, which may affect the
robustness of the conclusions and precluded the use of a suitable
network meta-analysis. Secondly, while the classification of PVTT
is crucial in determining treatment strategies and outcomes, the
lack of original data hindered the ability to perform subgroup
analyses based on PVTT classifications. Thirdly, most of the
included studies were observational, and there were substantial
differences in treatment methods, contributing to the heterogeneity
in statistical results and potentially weakening the reliability of
the findings. Beyond treatment heterogeneity, variations in patient
populations also introduce unavoidable heterogeneity. The disease
characteristics of HCC differ between patients in Asia and Western
regions (70), and since the
present study population predominantly comprised East Asian
individuals, the generalizability of these findings to a global
context is limited. The development of neoadjuvant therapies in HCC
is progressing rapidly, and the present study will be updated as
new relevant literature is published.
The present meta-analysis evaluated the long-term
prognosis and safety of neoadjuvant therapy in patients with HCC
complicated by PVTT. The findings suggested that neoadjuvant
therapy not only offered superior efficacy compared with priority
surgery, but also demonstrated a favorable safety profile. However,
these preliminary conclusions require further validation through
larger, multicenter RCTs to improve their reliability and
generalizability across diverse patient populations.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was supported by the Medical Scientific
Research Foundation of Zhejiang Province, China (grant no.
2021KY1018) and the HwaMei Research Foundation of Ningbo No. 2
Hospital (grant no. 2024HMKYA55).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
WX, XiaZ, YF, YZ, ZX, YY, QW and XinZ contributed to
the conception and development of the paper. WX and XiaZ confirm
the authenticity of all the raw data. WX and XiaZ designed the
research process. YF and YZ conducted the database search and
extracted relevant data from the articles. ZX and YY performed the
statistical analysis. QW and XinZ drafted the meta-analysis. All
authors read and approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
HCC
|
hepatocellular carcinoma
|
|
PVTT
|
portal vein tumor thrombus
|
|
OS
|
overall survival
|
|
RFS
|
relapse-free survival
|
|
HR
|
hazard ratio
|
|
BCLC
|
Barcelona Clinic Liver Cancer
|
|
PRISMA
|
Preferred Reporting Items for
Systematic Reviews and Meta-Analyses
|
|
MeSH
|
Medical Subject Headings
|
|
RCT
|
randomized controlled trial
|
|
NOS
|
Newcastle-Ottawa scale
|
|
TACE
|
transcatheter arterial
chemoembolization
|
|
HAIC
|
hepatic arterial infusion
chemotherapy
|
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dasgupta P, Henshaw C, Youlden DR, Clark
PJ, Aitken JF and Baade PD: Global trends in incidence rates of
primary adult liver cancers: A systematic review and meta-analysis.
Front Oncol. 10:1712020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gavriilidis P, Pawlik TM and Azoulay D:
Comprehensive review of hepatocellular carcinoma with portal vein
tumor thrombus: State of art and future perspectives. Hepatobiliary
Pancreat Dis Int. 23:221–227. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Deng ZJ, Li L, Teng YX, Zhang YQ, Zhang
YX, Liu HT, Huang JL, Liu ZX, Ma L and Zhong JH: Treatments of
hepatocellular carcinoma with portal vein tumor thrombus: Current
status and controversy. J Clin Transl Hepatol. 10:147–158. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sun J, Guo R, Bi X, Wu M, Tang Z, Lau WY,
Zheng S, Wang X, Yu J, Chen X, et al: Guidelines for diagnosis and
treatment of hepatocellular carcinoma with portal vein tumor
thrombus in China (2021 edition). Liver Cancer. 11:315–328. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Khan AR, Wei X and Xu X: Portal vein tumor
thrombosis and hepatocellular carcinoma-the changing tides. J
Hepatocell Carcinoma. 8:1089–1115. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cheng S, Chen M and Cai J; National
Research Cooperative Group for Diagnosis and Treatment of
Hepatocellular Carcinoma with Tumor Thrombus, : Chinese expert
consensus on multidisciplinary diagnosis and treatment of
hepatocellular carcinoma with portal vein tumor thrombus: 2016
Edition. Oncotarget. 8:8867–8876. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yau T, Tang VYF, Yao TJ, Fan ST, Lo CM and
Poon RTP: Development of Hong Kong liver cancer staging system with
treatment stratification for patients with hepatocellular
carcinoma. Gastroenterology. 146:1691–1700.e3. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kudo M, Matsui O, Izumi N, Iijima H,
Kadoya M, Imai Y, Okusaka T, Miyayama S, Tsuchiya K, Ueshima K, et
al: JSH consensus-based clinical practice guidelines for the
management of hepatocellular carcinoma: 2014 Update by the liver
cancer study group of Japan. Liver Cancer. 3:458–468. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ye JZ, Wang YY, Bai T, Chen J, Xiang BD,
Wu FX and Li LQ: Surgical resection for hepatocellular carcinoma
with portal vein tumor thrombus in the Asia-Pacific region beyond
the Barcelona clinic liver cancer treatment algorithms: A review
and update. Oncotarget. 8:93258–93278. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sakamoto K and Nagano H: Surgical
treatment for advanced hepatocellular carcinoma with portal vein
tumor thrombus. Hepatol Res. 47:957–962. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wei Z, Zhao J, Bi X, Zhang Y, Zhou J, Li
Z, Huang Z, Zhao H and Cai J: Neoadjuvant radiotherapy for
resectable hepatocellular carcinoma with portal vein tumor
thrombus: A systematic review. Hepatobiliary Surg Nutr. 11:709–717.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Anand AC and Acharya SK: New developments
in the treatment of hepatocellular carcinoma: The concept of
adjuvant and neoadjuvant chemotherapy. J Clin Exp Hepatol.
11:284–287. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Seckler F, Doussot A, Colpart P, Turco C,
Calame P, Aubin F, Algros MP, Borg C, Nardin C and Heyd B:
Preoperative immunotherapy for resectable hepatocellular carcinoma:
Toward a paradigm shift? J Hepatol. 73:1588–1590. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Huang A, Yang XR, Chung WY, Dennison AR
and Zhou J: Targeted therapy for hepatocellular carcinoma. Signal
Transduct Target Ther. 5:1462020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lee M and Shin HP: Efficacy of
transarterial chemoembolization (TACE) for early-stage
hepatocellular carcinoma. Medicina (Kaunas). 59:21742023.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xu L, Chen L and Zhang W: Neoadjuvant
treatment strategies for hepatocellular carcinoma. World J
Gastrointest Surg. 13:1550–1566. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yang J, Kim JM, Rhu J, Choi GS, David Kwon
CH and Joh JW: Surgical resection is preferred in selected solitary
hepatocellular carcinoma with portal vein tumor thrombosis. Dig
Surg. 39:42–50. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Page MJ, McKenzie JE, Bossuyt PM, Boutron
I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan
SE, et al: The PRISMA 2020 statement: An updated guideline for
reporting systematic reviews. BMJ. 372:n712021. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zeng X, Zhang Y, Kwong JS, Zhang C, Li S,
Sun F, Niu Y and Du L: The methodological quality assessment tools
for preclinical and clinical studies, systematic review and
meta-analysis, and clinical practice guideline: A systematic
review. J Evid Based Med. 8:2–10. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Higgins JP, Altman DG, Gøtzsche PC, Jüni
P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA, et
al: The cochrane collaboration's tool for assessing risk of bias in
randomised trials. BMJ. 343:d59282011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gao B, Shentu H, Sha S, Wang D, Chen X,
Huang Z, Dong N, Lai H, Xu J and Zhou X: Efficacy of IL-23
inhibitors and IL-12/23 inhibitors in the induction treatment of
Crohn's disease: A meta-analysis based on randomized controlled
trials. Cent Eur J Immunol. 48:301–310. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhou Y, Dai M, Huang T, Chen B, Xiang Z,
Tang J, Zheng M and Guo L: Association between BMI and efficacy of
SGLT2 inhibitors in patients with heart failure or at risk of heart
failure: A meta-analysis based on randomized controlled trials.
Cardiology. 149:104–116. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yin J, Wang D, He Y, Sha H, Zhang W and
Huang W: The safety of not implementing endoscopic nasobiliary
drainage after elective clearance of choledocholithiasis: A
systematic review and meta-analysis. BMC Surg. 24:2392024.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wei X, Jiang Y, Zhang X, Feng S, Zhou B,
Ye X, Xing H, Xu Y, Shi J, Guo W, et al: Neoadjuvant
three-dimensional conformal radiotherapy for resectable
hepatocellular carcinoma with portal vein tumor thrombus: A
randomized, open-label, multicenter controlled study. J Clin Oncol.
37:2141–2151. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hu Z, Yang Z, Wang J, Fu Y, Hu Z, Zhou Z,
Chen M and Zhang Y: Survival benefit of neoadjuvant hepatic
arterial infusion chemotherapy followed by hepatectomy for
hepatocellular carcinoma with portal vein tumor thrombus. Front
Pharmacol. 14:12236322023. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kamiyama T, Nakanishi K, Yokoo H, Tahara
M, Nakagawa T, Kamachi H, Taguchi H, Shirato H, Matsushita M and
Todo S: Efficacy of preoperative radiotherapy to portal vein tumor
thrombus in the main trunk or first branch in patients with
hepatocellular carcinoma. Int J Clin Oncol. 12:363–368. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Li N, Feng S, Xue J, Wei XB, Shi J, Guo
WX, Lau WY, Wu MC, Cheng SQ and Meng Y: Hepatocellular carcinoma
with main portal vein tumor thrombus: A comparative study comparing
hepatectomy with or without neoadjuvant radiotherapy. HPB (Oxford).
18:549–556. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zhang YF, Guo RP, Zou RH, Shen JX, Wei W,
Li SH, OuYang HY, Zhu HB, Xu L, Lao XM and Shi M: Efficacy and
safety of preoperative chemoembolization for resectable
hepatocellular carcinoma with portal vein invasion: A prospective
comparative study. Eur Radiol. 26:2078–2088. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chong JU, Choi GH, Han DH, Kim KS, Seong
J, Han KH and Choi JS: Downstaging with localized concurrent
chemoradiotherapy can identify optimal surgical candidates in
hepatocellular carcinoma with portal vein tumor thrombus. Ann Surg
Oncol. 25:3308–3315. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Durand F and Valla D: Assessment of the
prognosis of cirrhosis: Child-Pugh versus MELD. J Hepatol. 42
(Suppl):S100–S107. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Trevisani F, Vitale A, Kudo M, Kulik L,
Park JW, Pinato DJ and Cillo U: Merits and boundaries of the BCLC
staging and treatment algorithm: Learning from the past to improve
the future with a novel proposal. J Hepatol. 80:661–669. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yau T, Yao TJ, Chan P, Ng K, Fan ST and
Poon RTP: A new prognostic score system in patients with advanced
hepatocellular carcinoma not amendable to locoregional therapy:
Implication for patient selection in systemic therapy trials.
Cancer. 113:2742–2751. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Govalan R, Lauzon M, Luu M, Ahn JC, Kosari
K, Todo T, Kim IK, Noureddin M, Kuo A, Walid AS, et al: Comparison
of surgical resection and systemic treatment for hepatocellular
carcinoma with vascular invasion: National cancer database
analysis. Liver Cancer. 10:407–418. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Reig M, Forner A, Rimola J, Ferrer-Fàbrega
J, Burrel M, Garcia-Criado Á, Kelley RK, Galle PR, Mazzaferro V,
Salem R, et al: BCLC strategy for prognosis prediction and
treatment recommendation: The 2022 update. J Hepatol. 76:681–693.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Ho MC, Hasegawa K, Chen XP, Nagano H, Lee
YJ, Chau GY, Zhou J, Wang CC, Choi YR, Poon RT and Kokudo N:
Surgery for intermediate and advanced hepatocellular carcinoma: A
consensus report from the 5th Asia-Pacific primary liver cancer
expert meeting (APPLE 2014). Liver Cancer. 5:245–256. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Torzilli G, Belghiti J, Kokudo N, Takayama
T, Capussotti L, Nuzzo G, Vauthey JN, Choti MA, De Santibanes E,
Donadon M, et al: A snapshot of the effective indications and
results of surgery for hepatocellular carcinoma in tertiary
referral centers: Is it adherent to the EASL/AASLD
recommendations?: An observational study of the HCC East-West study
group. Ann Surg. 257:929–937. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Kokudo T, Hasegawa K, Matsuyama Y,
Takayama T, Izumi N, Kadoya M, Kudo M, Ku Y, Sakamoto M, Nakashima
O, et al: Survival benefit of liver resection for hepatocellular
carcinoma associated with portal vein invasion. J Hepatol.
65:938–943. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Cheng S, Yang J, Shen F, Zhou W, Wang Y,
Cong W, Yang GS, Cheng H, Hu H, Gao C, et al: Multidisciplinary
management of hepatocellular carcinoma with portal vein tumor
thrombus-Eastern hepatobiliary surgical hospital consensus
statement. Oncotarget. 7:40816–40829. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Václav T: Surgical treatment of
hepatocellular carcinoma. Klin Onkol. 33 (Suppl 3):S30–S33.
2020.
|
|
41
|
Tsoulfas G, Agorastou P, Tooulias A and
Marakis GN: Current and future challenges in the surgical treatment
of hepatocellular carcinoma: A review. Int Surg. 99:779–786. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Delis SG and Dervenis C: Selection
criteria for liver resection in patients with hepatocellular
carcinoma and chronic liver disease. World J Gastroenterol.
14:3452–3460. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Ohkubo T, Yamamoto J, Sugawara Y, Shimada
K, Yamasaki S, Makuuchi M and Kosuge T: Surgical results for
hepatocellular carcinoma with macroscopic portal vein tumor
thrombosis. J Am Coll Surg. 191:657–660. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Jiao T, Tang H, Zhang W, Hu B, Wan T, Cao
Y, Zhang Z, Wang Y, Cao J, Cui M and Lu S: Long-term survival and
portal vein patency with novel PVTT surgery approach in advanced
HCC patients with Vp3/4 PVTT following combination therapy of TKIs
and PD-1 inhibitors. BMC Surg. 23:3842023. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Yang J, Yan L and Wang W: Current status
of multimodal & combination therapy for hepatocellular
carcinoma. Indian J Med Res. 136:391–403. 2012.PubMed/NCBI
|
|
46
|
Lau WY, Ho SKW, Yu SC, Lai ECH, Liew CT
and Leung TWT: Salvage surgery following downstaging of
unresectable hepatocellular carcinoma. Ann Surg. 240:299–305. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Fimognari FL and Violi F: Portal vein
thrombosis in liver cirrhosis. Intern Emerg Med. 3:213–218. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Yu JI and Park HC: Radiotherapy as valid
modality for hepatocellular carcinoma with portal vein tumor
thrombosis. World J Gastroenterol. 22:6851–6863. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Yoon HI, Song KJ, Lee IJ, Kim DY, Han KH
and Seong J: Clinical benefit of hepatic arterial infusion
concurrent chemoradiotherapy in locally advanced hepatocellular
carcinoma: A propensity score matching analysis. Cancer Res Treat.
48:190–197. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Nakazawa T, Hidaka H, Shibuya A, Okuwaki
Y, Tanaka Y, Takada J, Minamino T, Watanabe M, Kokubu S and Koizumi
W: Overall survival in response to sorafenib versus radiotherapy in
unresectable hepatocellular carcinoma with major portal vein tumor
thrombosis: Propensity score analysis. BMC Gastroenterol.
14:842014. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Shiozawa K, Watanabe M, Ikehara T,
Matsukiyo Y, Kogame M, Kishimoto Y, Okubo Y, Makino H, Tsukamoto N,
Igarashi Y and Sumino Y: Comparison of percutaneous radiofrequency
ablation and CyberKnife(®) for initial solitary
hepatocellular carcinoma: A pilot study. World J Gastroenterol.
21:13490–13499. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Hamaoka M, Kobayashi T, Kuroda S, Iwako H,
Okimoto S, Kimura T, Aikata H, Nagata Y, Chayama K and Ohdan H:
Hepatectomy after down-staging of hepatocellular carcinoma with
portal vein tumor thrombus using chemoradiotherapy: A retrospective
cohort study. Int J Surg. 44:223–228. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Wu F, Chen B, Dong D, Rong W, Wang H, Wang
L, Wang S, Jin J, Song Y, Liu Y, et al: Phase 2 evaluation of
neoadjuvant intensity-modulated radiotherapy in centrally located
hepatocellular carcinoma: A nonrandomized controlled trial. JAMA
Surg. 157:1089–1096. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Chang Y, Jeong SW, Young Jang J and Jae
Kim Y: Recent updates of transarterial chemoembolilzation in
hepatocellular carcinoma. Int J Mol Sci. 21:81652020. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Chen C, Qiu H, Yao Y, Zhang Z, Ma C, Ma Y,
Zhao C, Xiang H, Zhao H, Zheng C, et al: Comprehensive predictive
factors for CalliSpheres® microspheres (CSM)
drug-eluting bead-transarterial chemoembolization and conventional
transarterial chemoembolization on treatment response and survival
in hepatocellular carcinoma patients. Clin Res Hepatol
Gastroenterol. 45:1014602021. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Niu ZJ, Ma YL, Kang P, Ou SQ, Meng ZB, Li
ZK, Qi F and Zhao C: Transarterial chemoembolization compared with
conservative treatment for advanced hepatocellular carcinoma with
portal vein tumor thrombus: Using a new classification. Med Oncol.
29:2992–2997. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Iwamoto H, Shimose S, Shirono T, Niizeki T
and Kawaguchi T: Hepatic arterial infusion chemotherapy for
advanced hepatocellular carcinoma in the era of chemo-diversity.
Clin Mol Hepatol. 29:593–604. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Hatooka M, Kawaoka T, Aikata H, Inagaki Y,
Morio K, Nakahara T, Murakami E, Tsuge M, Hiramatsu A, Imamura M,
et al: Hepatic arterial infusion chemotherapy followed by sorafenib
in patients with advanced hepatocellular carcinoma (HICS 55): An
open label, non-comparative, phase II trial. BMC Cancer.
18:6332018. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Chen XP and Huang ZY: Surgical treatment
of hepatocellular carcinoma in China: Surgical techniques,
indications, and outcomes. Langenbecks Arch Surg. 390:259–265.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Chen XP, Qiu FZ, Wu ZD and Zhang BX:
Chinese experience with hepatectomy for huge hepatocellular
carcinoma. Br J Surg. 91:322–326. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Clark TWI: Complications of hepatic
chemoembolization. Semin Intervent Radiol. 23:119–125. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Zhou WP, Lai ECH, Li AJ, Fu SY, Zhou JP,
Pan ZY and Lau WYand Wu MC: A prospective, randomized, controlled
trial of preoperative transarterial chemoembolization for
resectable large hepatocellular carcinoma. Ann Surg. 249:195–202.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Wu X, Wang Y, Wang S, Chen Y, Han J, Wang
C, Zhang M, Hu X, Song B, Wan X, et al: Neoadjuvant targeted
immunotherapy followed by surgical resection versus upfront surgery
for hepatocellular carcinoma with macrovascular invasion: A
multicenter study. J Cancer. 15:3024–3033. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Wu QQ, Chen YX, Zheng TT, Dai MT, Ye T, Xu
YH, Hu Y, Du SS and Zeng ZC: Which is the best combination of
surgery for hepatocellular carcinoma with hepatic/portal vein
thrombosis in China: A network meta-analysis of randomized
controlled trials. J BUON. 26:889–896. 2021.PubMed/NCBI
|
|
66
|
Wu QQ, Gao H, Du SS, Chen YX, Hu Y, Yang
P, Hou JZ and Zeng ZC: Comparing the efficacy and safety of
local-regional treatments for hepatocellular carcinoma with
portal/hepatic vein tumor thrombosis in China: A network
meta-analysis of randomized controlled trials. J BUON.
26:1950–1957. 2021.PubMed/NCBI
|
|
67
|
Leung JH, Wang SY, Leung HWC and Chan ALF:
Comparative efficacy and safety of multimodality treatment for
advanced hepatocellular carcinoma with portal vein tumor thrombus:
Patient-level network meta-analysis. Front Oncol. 14:13447982024.
View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Lee HA, Seo YS, Shin IS, Yoon WS, Lee HY
and Rim CH: Efficacy and feasibility of surgery and external
radiotherapy for hepatocellular carcinoma with portal invasion: A
meta-analysis. Int J Surg. 104:1067532022. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Chan SL, Chong CCN, Chan AWH, Poon DMC and
Chok KSH: Management of hepatocellular carcinoma with portal vein
tumor thrombosis: Review and update at 2016. World J Gastroenterol.
22:7289–7300. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Lu J, Zhang XP, Zhong BY, Lau WY, Madoff
DC, Davidson JC, Qi X, Cheng SQ and Teng GJ: Management of patients
with hepatocellular carcinoma and portal vein tumour thrombosis:
Comparing east and west. Lancet Gastroenterol Hepatol. 4:721–730.
2019. View Article : Google Scholar : PubMed/NCBI
|