Introduction
Synovial sarcoma is a type of malignant soft-tissue
tumor that usually occurs in 80% of cases and affects knee and
ankle joints in young adults. It also occurs in shoulder, elbow and
hip regions. This neoplasm develops close to the joints, tendon
sheaths and bursae, but it is rare for it to involve the synovial
membrane. For the treatment of these tumors, the mainstay of
curative therapy is the complete surgical resection of such tumor
manifestations with negative histological margins. However, up to
50% of patients will develop distant metastases during the course
of their disease (1). Regional
radiotherapy or adjuvant chemotherapy following surgery is
therefore crucial. In certain cases, surgery is difficult to
perform due to the large volume of the tumor, and then neoadjuvant
chemotherapy is considered. A screening method for the selection of
effective anticancer drugs for individual patients may be useful,
particularly for patients who have large tumors and need
neoadjuvant chemotherapy to decrease the volume of the tumor for
local excision. The collagen gel droplet embedded culutre-drug
sensitivity test (CD-DST) is an anticancer drug sensitivity test
that requires only a small number of cells (3×103 per
droplet) (2–4). The clinical usefulness of CD-DST for
colon (5), breast (6) and gastric (7) cancers and even certain rare cases of
solid tumors, such as ovarian mature cystic teratoma with malignant
transformation to adenocarcinoma (8), have been reported. Yabushita et
al (9) found a strong
correlation between clinical outcome and CD-DST results for
anticancer drugs. This is a study of a case of a large synovial
sarcoma in the right shank, for which neoadjuvant chemotherapy was
investigated using CD-DST.
Materials and methods
Anticancer drugs
Isophosphamide (IFO) (10,11)
and anthracycline anti-tumor drugs (11,12),
including therarubicin (THP), adriamycin (ADM) and epirubicin
(EPI), are the first choice in the chemotherapy of soft tissue
tumors. Cisplatin (CDDP) (13),
vincristine (VCR) (13) and
5-fluorouracil (5-FU) (14,15) have also been reported to be
effective against soft tissue tumors. CDDP, THP, VCR and 5-FU were
examined in CD-DST. IFO has no effect in in vitro tests, and
since it was necessary for IFO to be activated by phosphamidase
in vivo, it was used as a negative control.
Preparation of the tumor cell
suspension
The excisional specimen was minced finely using
scissors, suspended in Hank's balanced saline solution (HBSS,
Gibco), treated with Dispersion Enzyme Cocktail EZ (including 1.0%
collagenase; Nitta Gelatin, Inc., Osaka, Japan) and digested at
37°C for 1 h. The dispersed tumor cells were collected by
centrifugation at 1000 rpm for 3 min, filtered through a 308 nm
nylon mesh, washed in HBSS, suspended in PCM-1 medium (Nitta
Gelatin) and then incubated in a collagen gel-coated flask
(CG-flask, Nitta Gelatin) in a CO2 incubator at 37°C for
24 h. The collagen gel in the CG-flask was dissolved in a cell
dispersion using EZ, and only viable cells that adhered to the
collagen gel were collected and used for the sensitivity test.
Collagen gel droplet embedded
culture-drug sensitivity test
Type I collagen, 10X F-12 medium and reconstitution
buffer (Cellmatrix Type CD, Nitta Gelatin) were combined in an ice
bath at a ratio of 8:1:1. The prepared tumor cell suspension was
added to a collagen solution (1:10, v:v) at a final density of
2×105 cells/ml. A total of three drops of the
collagen-cell mixture (30 μl/drop) were placed in each well of a
6-well multiplate on ice and allowed to gel at 37°C in a
CO2 incubator; the final concentration was
~3×103 cells/droplet. One hour later, each well was
overlaid with 3 ml DMEM/F 12 medium (Gibco) containing 10% fetal
bovine serum (Gibco, Canada), incubated in a CO2
incubator at 37°C overnight. CDDP, THP, VCR and 5-FU were then
added to the final concentrations of 0.2 and 2.0 μg/ml, 0.02 and
0.2 μg/ml, 0.01 and 0.1 μg/ml and 1.0 and 10 μg/ml, respectively,
followed by further incubation for 24 h. IFO (1 or 10 μg/ml) was
added as a negative control.
In vitro chemosensitivity test
After removal of the medium containing the
anticancer drugs, each well was rinsed twice with 3 ml HBSS,
overlaid with 4 ml PCM-2 medium (Serum Free Medium, Nitta Gelatin)
and incubated for an additional 7 days. On the fourth day of
incubation, the medium was changed. At the end of the incubation,
neutral red (Nitta Gelatin) was added to each well at a final
concentration of 50 μg/ml, and cells in the collagen gel droplets
were stained for 2 h. Each collagen droplet was fixed with 10%
neutral formalin buffer, washed in double-distilled water,
air-dried and quantified using image analysis. The in vitro
sensitivity was expressed as the percentage of the T/C ratio, where
T is the total volume in the treated group and C is the total
volume in the control group. When the T/C ratio was ≤50%, the in
vitro drug sensitivity was regarded as effective. A T/C ratio
of >50 and ≤60% was considered borderline, and a T/C ratio of
>60% was considered to indicate a lack of efficacy (2). Clinical responses were assessed
according to World Health Organization criteria, whereby tumors
demonstrating a complete response or partial response are
considered clinically responsive. The results of the CD-DST are
shown in Fig. 4.
Results
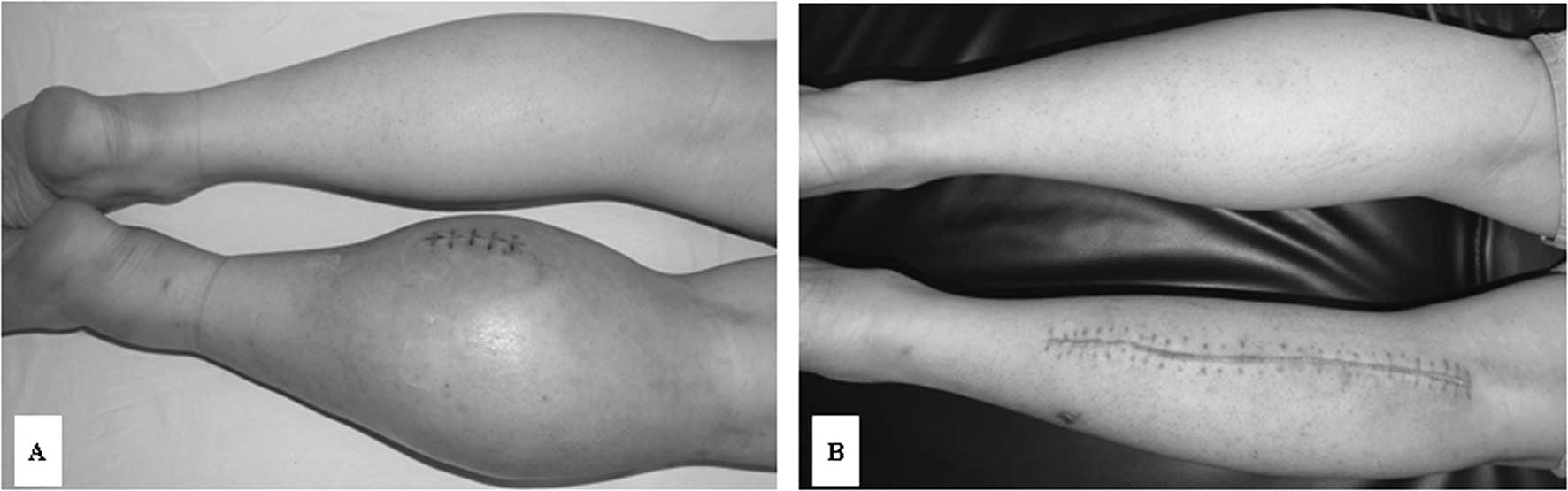
The patient was a 28-year-old male who presented
with a large mass in the right shank. The perimeter of the right
shank was 46.5 cm, while the left side was 37 cm (Fig. 1A). Magnetic resonance imaging (MRI)
revealed a 15×10×9 cm mass in the right shank (Fig. 2A and B), and a B-type Ultrasound
scan showed a 1.0×0.7×0.5 cm intumesce in the right inguinal fold.
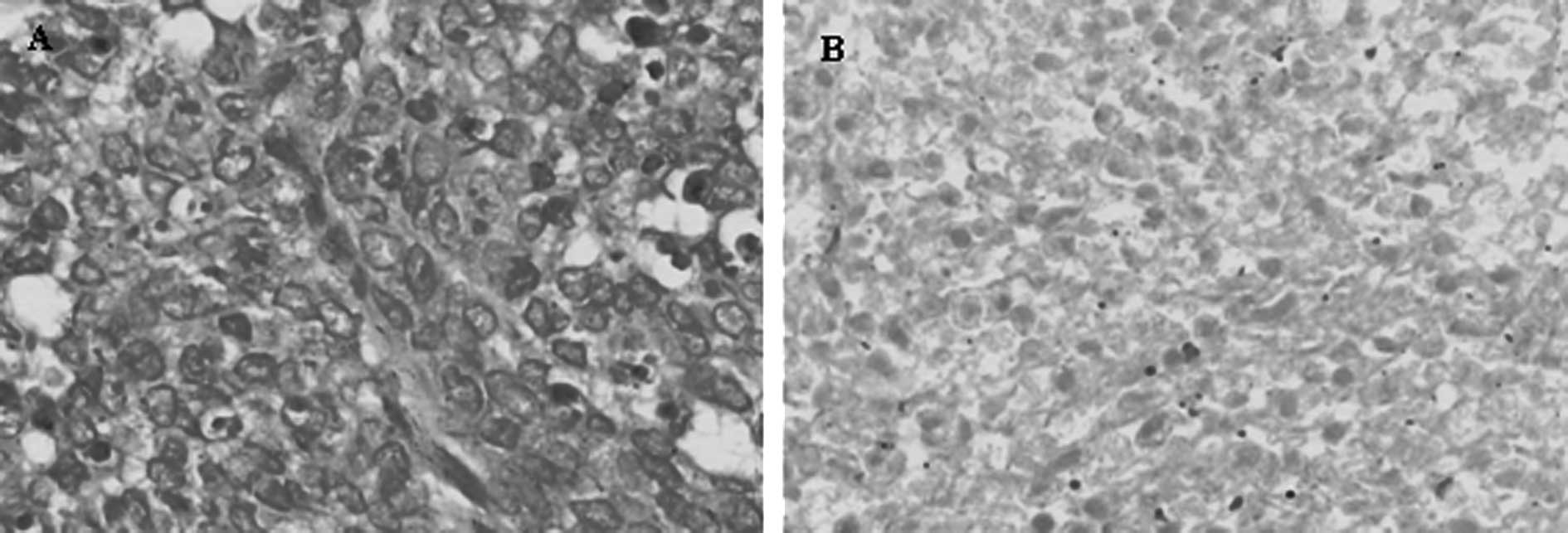
The histopathological diagnosis of excisional biopsy specimens was
synovial sarcoma with low differentiation (Fig. 3A).
Although the tumor was extremely large for local
excision, the patient refused to accept amputation of the right
extremity. Neoadjuvant chemotherapy was considered in order to
decrease the volume of the tumor to allow for a local excision. A
sample of 0.5 g of the excisional specimen was used for the CD-DST
test.
Neoadjuvant THP/CDDP chemotherapy was selected based
on the results of the CD-DST (Fig.
4), and administration of THP (30 mg/m2, d1-d2) and
CDDP (40 mg/m2, d1-d2) was initiated. Upon completion of
three courses of THP/CDDP chemotherapy, the perimeter of the right
shank decreased from 46.5 to 42.5 cm, and its texture became much
more supple. A precontrast CT scan showed that the volume of the
tumor had decreased to 11×8.2 cm, while a contrast scan indicated
tumor necrosis (Fig. 5A and B) and
a B-type Ultrasound scan showed that the intumesce in the right
inguinal fold had disappeared. Since the neoadjuvant THP/CDDP
chemotherapy was successful, a local tumor excision was performed
(Fig. 1B). The pathodiagnosis
indicated fibroblast cell proliferation and tumor cell necrosis as
well as a grade III chemotherapy response (Fig. 3B). Post-operatively, the patient
received further adjuvant chemotherapy of THP/CDDP, and he was
alive and without recurrence at a 16-month follow-up.
Discussion
The first choice for the treatment of synovial
sarcoma is local excision with wide margins of normal tissue,
followed by regional radiotherapy or adjuvant chemotherapy
(16,17). However, in some cases surgery is
difficult to perform due to the large volume of the tumor, thus
neoadjuvant chemotherapy is considered. In the case we reported,
the tumor was extremely large and we were unable to perform a local
excision. The patient involved was young and refused to accept
amputation of the extremity. Neoadjuvant chemotherapy was therefore
considered in order to decrease the volume of the tumor. IFO
(10,11) and anthracycline anti-tumor drugs
(11,12), including THP, ADM and EPI, are the
first choice in the chemotherapy of soft tissue tumors. CDDP
(13), VCR (13) and 5-FU (14,15)
are also reported to be effective against soft tissue tumors. In
this case, we used the system of CD-DST described by Kobayashi
et al (2–4) to check the sensitivity of tumor cells
to THP, VCR, CDDP and 5-FU. Since IFO should be activated by
phosphamidase in vivo, we used it as the negative control.
Based on the results of the CD-DST, THP/CDDP neoadjuvant
chemotherapy was administered. Upon completion of three courses of
THP/CDDP chemotherapy, the perimeter of the right shank decreased
from 46.5 to 42.5 cm, the texture became much more supple, and a CT
scan showed that the volume of the tumor had decreased from 15×10
to 11×8.2 cm and that the tumor necrosis had disappeared. A B-type
Ultrasound scan showed that the intumesce in the right inguinal
fold had also disappeared. The pathodiagnosis of the local excision
specimen indicated fibroblast cell proliferation and tumor cell
necrosis, as well as a grade III chemotherapy response (Fig. 3B). The patient was alive and without
recurrence at a 16-month follow-up evaluation. This clinical course
therefore correlated successfully with the results of the CD-DST.
Our results show that CD-DST can be used to evaluate anticancer
drug sensitivity. Further investigation of CD-DST is required as a
test for the prediction of anticancer drug sensitivity in cancer
patients. CD-DST may therefore be particularly useful for selecting
chemotherapeutic drugs for patients with synovial sarcoma,
particularly for those with large tumors who require neoadjuvant
chemotherapy to decrease the volume of the tumor prior to local
excision surgery.
References
|
1
|
Schmitt T and Kasper B: New medical
treatment options and strategies to assess clinical outcome in
soft-tissue sarcoma. Expert Rev Anticancer Ther. 9:1159–1167. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kobayashi H, Higashiyama M, Minamigawa K,
Tanisaka K, Takano T, Yokouchi H, Kodama K and Hata T: Examination
of in vitro chemosensitivity test using collagen gel droplet
culture method with colorimetric endpoint quantification. Jpn J
Cancer Res. 92:203–210. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kobayashi H: Development of a new in vitro
chemosensitivity test using collagen gel droplet embedded culture
and image analysis for clinical usefulness. Recent Results Cancer
Res. 161:48–61. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kobayashi H: Collagen gel droplet culture
method to examine in vitro chemosensitivity. Methods Mol Med.
110:59–67. 2005.PubMed/NCBI
|
|
5
|
Araki Y, Isomoto H, Matsumoto A, Kaibara
A, Yasunaga M, Hayashi K, Yatsugi H and Yamauchi K: An in vitro
chemosensitivity test for colorectal cancer using collagen-gel
droplet embedded cultures. Kurume Med J. 46:163–166. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tamura Y, Kobayashi H, Taguchi T, Motoyama
K, Inaji H and Noguchi S: Prediction of chemotherapeutic response
by collagen gel droplet embedded culture-drug sensitivity test in
human breast cancers. Int J Cancer. 98:450–455. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hanatani Y, Kobayashi H, Kodaira S, Takami
H, Asagoe T and Kaneshiro E: An in vitro chemosensitivity
test for gastric cancer using collagen gel droplet embedded
culture. Oncol Rep. 7:1027–1033. 2000.
|
|
8
|
Yamagami W, Banno K, Kawaguchi M, Yanokura
M, Kuwabara Y, Hirao N, Susumu N, Tsukazaki K and Aoki D: Use of
the collagen gel droplet embedded drug sensitivity test to
determine drug sensitivity against ovarian mature cystic teratoma
with malignant transformation to adenocarcinoma: a case report.
Chemotherapy. 53:137–141. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yabushita H, Ohnishi M, Komiyama M, Mori T
and Noguchi M, Kishida T, Noguchi Y, Sawaguchi K and Noguchi M:
Usefulness of collagen gel droplet embedded culture drug
sensitivity testing in ovarian cancer. Oncol Rep. 12:307–311.
2004.PubMed/NCBI
|
|
10
|
Macdermed DM, Miller LL, Peabody TD, Simon
MA, Luu HH, Haydon RC, Montag AG, Undevia SD and Connell PP:
Primary tumor necrosis predicts distant control in locally advanced
soft-tissue sarcomas after preoperative concurrent
chemoradiotherapy. Int J Radiat Oncol Biol Phys. 15:1147–1153.
2010. View Article : Google Scholar
|
|
11
|
Kopp HG, Patel S, Brücher B and Hartmann
JT: Potential combination chemotherapy approaches for advanced
adult-type soft-tissue sarcoma. Am J Clin Dermatol. 9:207–217.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Patel S, Keohan ML, Saif MW, Rushing D,
Baez L, Feit K, DeJager R and Anderson S: Phase II study of
intravenous TZT-1027 in patients with advanced or metastatic
soft-tissue sarcomas with prior exposure to anthracycline-based
chemotherapy. Cancer. 107:2881–2887. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Goto T, Kosaku H, Kobayashi H, Hozumi T
and Kondo T: Soft tissue sarcoma: postoperative chemotherapy. (In
Japanese). Gan To Kagaku Ryoho. 31:1324–1330. 2004.PubMed/NCBI
|
|
14
|
Wada Y, Hirayama Y, Seki R, Konuma Y,
Kohda K, Yoshida M, Nakamura Y, Obata M and Ando M: Long-term
remission survival with a case of rectal carcinoid tumor with
metastasis in the soft tissue effectively treated with the
combination therapy of irinotecan/5-fluorouracil/levofolinate
followed by resection. (In Japanese). Nippon Naika Gakkai Zasshi.
96:2513–2515. 2007. View Article : Google Scholar
|
|
15
|
Marchal JA, Boulaiz H, Rodríguez-Serrano
F, Peran M, Carrillo E, Vélez C, Domínguez J, Gómez-Vidal JA,
Campos J, Gallo MA, Espinosa A and Aránega A: 5-Fluorouracil
derivatives induce differentiation mediated by tubulin and HLA
class I modulation. Med Chem. 3:233–239. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kopp HG, Patel S, Brucher B and Hartmann
JT: Potential combination chemotherapy approaches for advanced
adult-type soft-tissue sarcoma. Am J Clin Dermatol. 9:207–217.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pervaiz N, Colterjohn N, Farrokhyar F,
Tozer R, Figueredo A and Ghert M: A systematic meta-analysis of
randomized controlled trails of adjuvant chemotherapy for localized
resectable soft-tissue sarcoma. Cancer. 113:573–581. 2008.
View Article : Google Scholar : PubMed/NCBI
|