Introduction
Cholesterol granulomas (ChGs) are chronic
inflammatory lesions that develop due to the body's reaction to
cholesterol crystals. They may be found in any part of the body
where cholesterol crystals can accumulate (1). The ChGs lack an epithelial lining;
for this reason, they are usually known as pseudotumors or not true
tumors. These lesions are most commonly found in the middle ear,
paranasal sinuses, or temporal bones, specifically the petrous
apex. Less common reports of ChGs in the breasts, liver, spleen,
kidney, lymph nodes and peritoneum have also been recorded
(2). Although the etiopathogenesis
of these pseudotumors is unknown, they are considered to be caused
by trauma and inflammation (2).
ChGs in testicular and paratesticular tissues are rare, and pose a
significant challenge in their differentiation from intrascrotal
tumors. This difficulty persists during physical examinations,
ultrasonography and even surgery, as ChGs may mimic the appearance
of intrascrotal tumors (3-5).
The present study describes the second recorded
case, to the best of our knowledge, of a ChG of the testis
mimicking a testicular tumor.
Case report
Patient information
A 62-year-old male presented with a painless right
scrotal mass which had been present for 6 years. There was no
history of trauma to the testis. The patient had a positive medical
history for hypertension, diabetes and two percutaneous coronary
interventions a few years prior. Previous surgical history included
a left-side scrotal exploration for an abscess in 2017 that proved
to be tuberculosis. He received a 6-month course of
anti-tuberculosis medication. Since then, no recurrence has been
detected. He was receiving amlodipine (10 mg, single daily dose),
metformin (500 mg, twice daily), atorvastatin (40 mg, single daily
dose) and aspirin (100 mg, single daily dose).
Clinical findings
A physical examination revealed a hard non-tender
mass at the lower pole of the testis with normal overlying scrotal
skin and transillumination was negative. His vital signs were
normal.
Diagnostic assessment
A complete blood count yielded normal results.
C-reactive protein levels (0.78 mg/l; normal range, <5 mg/l) and
the erythrocyte sedimentation rate (17 mm/h; normal range, 0-20
mm/h for males >50 years old) were both within normal limits.
Lipid profile analysis revealed normal levels of total cholesterol
(138.9 mg/dl; normal range, <200 mg/dl), triglycerides (147.8
mg/dl; normal range, <170 mg/dl), low-density lipoprotein (82.8
mg/dl; normal range, <130 mg/dl) and high-density lipoprotein
(48.5 mg/dl; normal range, 35-55 mg/dl). Other analyses revealed
normal levels of tumor markers [β-human chorionic gonadotropin
(0.03 IU/l; normal range, 0.02-0.8 IU/l), alpha-fetoprotein (8.2
ng/ml; normal range, 0-40 ng/ml) and lactate dehydrogenase (174
IU/l; normal range, 105-233 IU/l)]. A scrotal color Doppler
ultrasound revealed that the right testis was normal in size (39x18
mm), shape and echo texture, apart from a well-defined hypoechoic
13x14 mm lower pole testicular mass with surrounding
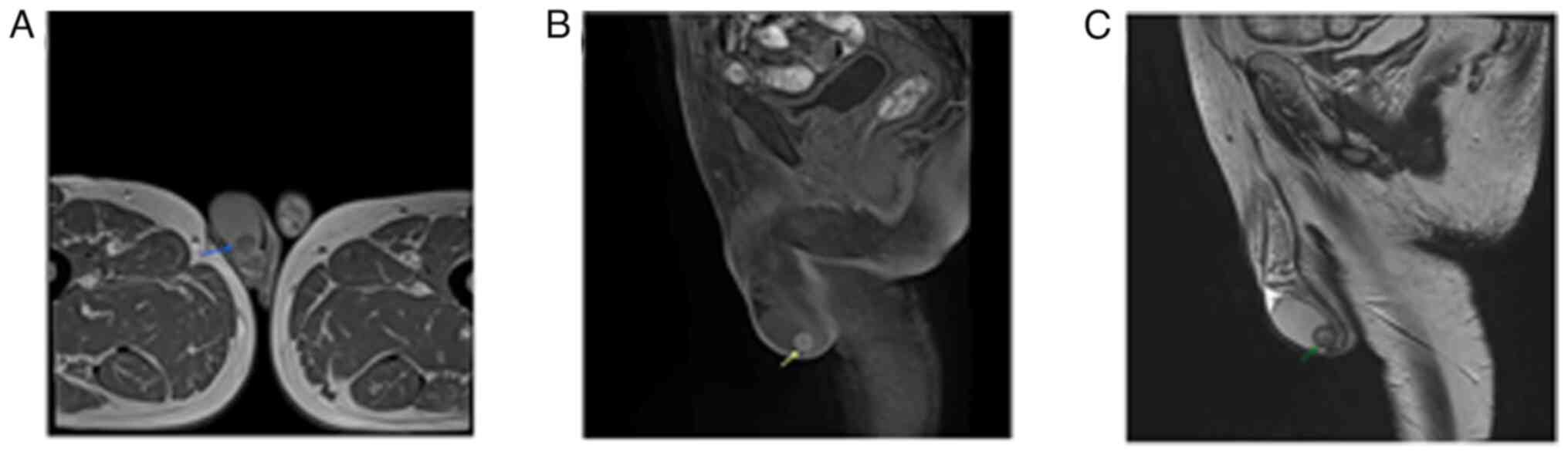
hypervascularity, suggesting a tumor. Scrotal magnetic resonance
imaging revealed a well-defined nodule (13x11x12 mm) (in transverse
x anteroposterior x craniocaudal dimensions) at the lower pole of
the right testis near the epididymis (Fig. 1). The lesion elicited a slightly
hyperintense signal in the T1-weighted image and a heterogenous
hypointense signal in the T2-weighted image. There was no
post-contrast enhancement.
Therapeutic intervention and
follow-up
The case was discussed with a multidisciplinary
team, and based on these findings, the surgeon decided to perform
an inguinal orchiectomy. However, the patient gave his consent to a
partial orchiectomy. Under spinal anesthesia, via inguinal
incision, a right partial orchiectomy was performed. A
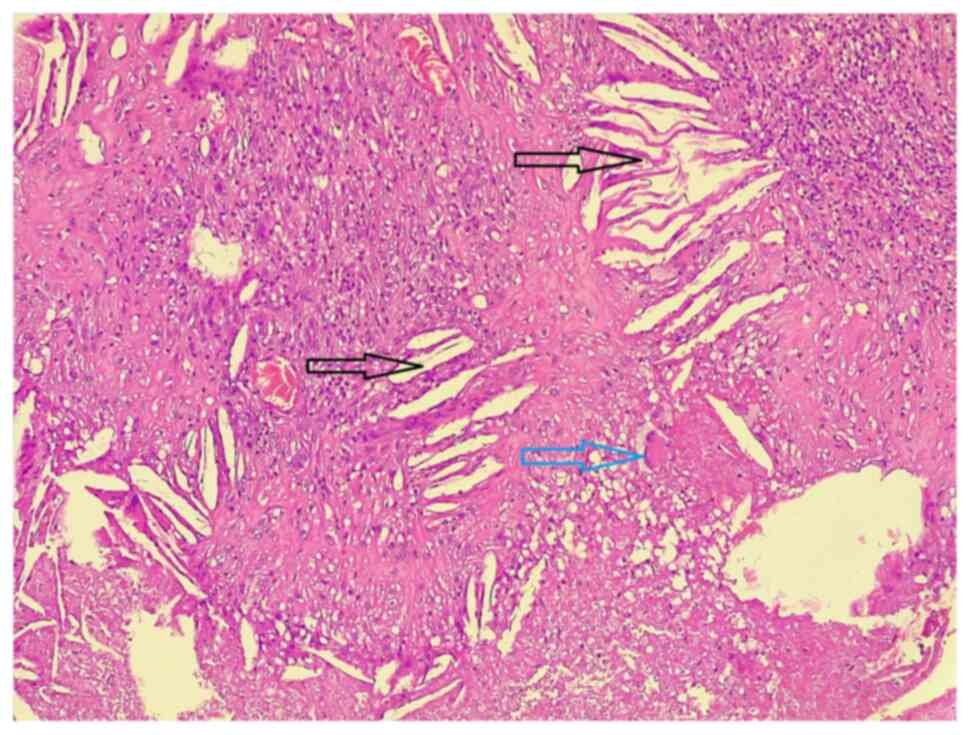
histopathological examination was performed on 5-µm-thick
paraffin-embedded sections. The sections were fixed in 10%
neutral-buffered formalin at room temperature for 24 h and stained
with hematoxylin and eosin (Bio Optica Co.) for 1-2 min at room
temperature. The sections were then examined under a light
microscope (Leica Microsystems GmbH). The results of the
histopathological examination were consistent with testicular ChG
(Fig. 2). The post-operative
period was uneventful.
Discussion
ChGs are benign masses that develop due to the
reaction of a foreign body to cholesterol crystals. They are
characterized by fibrous tissue, granulomatous inflammation and the
accumulation of foreign body giant cells (6,7).
The pathophysiology of ChG development remains
unknown and the suggested cause of development may differ depending
on the location. Hemorrhage, drainage obstruction and the
disruption of ventilation are factors that may be associated with
the development of the condition (8). Trauma leading to inflammation and
ischemia results in the extravasation of blood containing
cholesterol, fibrin and hemosiderin. The extravasated cholesterol
evokes a foreign body reaction, causing the formation of a
fibrogranulomatous lesion, which is the ChG (1). Although rare, there are reported
cases of ChGs in the kidneys (9),
mediastinum (10), breast
(11) and femur (12) in the literature. In the breasts,
duct ectasia leads to cholesterol crystal formation, and the
leakage of these crystals through the ducts then initiates an
inflammatory response (11).
Testicular ChGs are very rare and there has been
only one other recorded case in the literature to date, at least to
the best of our knowledge (4).
Cases of ChGs in the tunica vaginalis (13,14),
hydrocele sac (2,14), epididymis (6,15)
and tunica albuginea (5,16) have also been recorded in the
literature.
Lowenthal et al (13) reported a case of a 52-year-old male
patient with a left testicular mass that caused testis enlargement
for >25 years due to a trauma that was found to be ChG of the
tunica vaginalis. Another study reported a case of a 38-year-old
male who presented with a right scrotal mass for 7 years, without
having infections, such as tuberculosis or any history of trauma
(6). In that study, the results of
the histopathological analysis revealed a paratesticular ChG, and
they suggested that the condition should be a differential
diagnosis in cases with large and non-tender scrotal masses
(6). Gupta et al (2) also reported a case of ChG of the left
hydrocele sac presenting as a testicular tumor. ChG mimicking the
clinical signs of an acute scrotum has also been reported (15). Doi et al (16) reported the first case of ChG
associated with hematoma of the tunica albuginea. The case
described in the present study, unlike that in the study by
Lowenthal et al (13), did
not have any history of trauma and had no infectious diseases in
the same testis as the other mentioned studies (2,6,15,16).
ChG of the testes and paratesticular tissue most
commonly occurs after the age of 30, while Saeki et al
(5) recorded a case of ChG of the
tunica albuginea in a child aged 6 years. The only other recorded
case of ChG of the testis was that of a 76-year-old male (4), further supporting that ChGs of the
testes and paratesticular tissue occur in older age groups.
The case report of testicular ChG by Lin et
al (4) described a patient who
was admitted to the hospital for fever and shortness of breath. He
had a history of squamous cell carcinoma of the tongue and
radiation therapy. The condition of the patient deteriorated and
the patient passed away on the 12th day of hospitalization. A
genitourinary examination revealed a firm enlargement in the right
testis. Initially, it presented as a caseating tuberculous
granuloma, and a microscopic examination was necessary to establish
the diagnosis of ChG (4). The
patient described herein was vitally stable and had no history of
cancer or radiation therapy.
The clinical presentation of testicular and
paratesticular ChG is variable and may be encountered incidentally
during a physical examination or may present as mild scrotal
discomfort and a painless lump (6,13).
The case of testicular ChG recorded in the study by Lin et
al (4) presented for reasons
other than the scrotal swelling and the swelling was noted during a
physical examination.
Although patients reported with testicular and
paratesticular ChG did not have hypercholesterolemia (15), Albakheet et al (17) suggested an association between
familial hypercholesterolemia and ChG. The patient in the present
study had a normal lipid profile, but was on atorvastatin. Unal
et al (6) reported a case
with a mild elevation in serum cholesterol levels, but did not
assume this to be a direct cause of the ChG.
The diagnosis of testicular ChG can be challenging
without a histopathological examination (2,5). In
the present study, the pre-operative investigations of the patient
suggested a testicular tumor and the diagnosis of ChG was confirmed
by a histopathological examination.
The treatment of choice for the patient described
herein was inguinal orchiectomy; however, he only gave consent to a
partial orchiectomy. A right partial orchiectomy was performed via
an inguinal incision. In their report of testicular ChG, Lin et
al (4) performed an autopsy.
In the study by Unal et al (6), a radical inguinal orchiectomy was
performed for their case of ChG of the paratesticular tissue. Saeki
et al (5) performed a
surgical enucleation via a scrotal approach for their case of
paratesticular ChG, and were able to preserve the testis and
epididymis. All the cited references in the present case report
have been confirmed to be reliable (18).
In conclusion, ChG of the testis is an extremely
rare condition. Upon presentation, ChGs may be non-tender and may
only cause mild discomfort. Differentiating between the condition
and testicular tumors prior to surgery can be relatively
challenging and should be regarded as a differential diagnosis in
cases of testicular masses.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
RB was a major contributor to the conception of the
study, as well as to the literature search for related studies. NHH
and FHK were involved in the design of the study, in the literature
review and in the writing of the manuscript. JIH, AMA, BAA and IA
were involved in the literature review, in the design of the study,
in the critical revision of the manuscript and the processing of
the figures. AMA was the pathologist who performed the
histopathological diagnosis. SHT and AAMA were the radiologists who
performed the radiological assessments of the case. FHK and RB
confirm the authenticity of all the raw data. All authors have read
and approved the final manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from the
patient for this participation in the present study.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the present case report and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Nikolaidis V, Malliari H, Psifidis D and
Metaxas S: Cholesterol granuloma presenting as a mass obstructing
the external ear canal. BMC Ear Nose Throat Disord.
10(4)2010.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Gupta SC, Kumar V and Gupta NN:
Cholesterol granuloma of left-sided hydrocele sac mimicking
testicular tumor. RUHS J Health Sci. 4:163–165. 2019.
|
|
3
|
Mahmood ZH, Mohemed FM, Fatih BN, Qadir AA
and Abdalla SH: Cancer publications in one year (2022); a
cross-sectional study. Barw Med J. 1:2023.
|
|
4
|
Lin JI, Tseng CH, Marsidi PJ and Bais VC:
Cholesterol granuloma of right testis. Urology. 14:522–523.
1979.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Saeki I, Kurihara S, Kojima M, Imaji R and
Hiyama E: Paratesticular cholesterol granuloma. J Pediatric Sur
Case Rep. 61(101630)2020.
|
|
6
|
Unal D, Kilic M, Oner S, Erkinuresin T,
Demirbas M, Coban S and Aydos MM: Cholesterol granuloma of the
paratesticular tissue: A case report. Can Urol Assoc J.
9:E390–E392. 2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Nager GT and Vanderveen TS: Cholesterol
granuloma involving the temporal bone. Ann Otol Rhinol Laryngol.
85:204–209. 1976.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Ahmetgjekaj I, Harizi E, Rahman A, Hyseni
F, Nasir F, Decka A, Rahman M, Shemsi K, Saliaj K, Akram S, et al:
Giant cholesterol granuloma of petrous apex. Radiol Case Rep.
17:1220–1224. 2022.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Okamoto K, Hatori M, Tomita K, Yokoyama Y,
Makino T, Hirono M, Muramatsu K, Arai S, Morikawa Y, Miyakubo M, et
al: Cholesterol granuloma of the kidney: A case report. Nihon
Hinyokika Gakkai Zasshi. 102:586–590. 2011.PubMed/NCBI View Article : Google Scholar : (In Japanese).
|
|
10
|
Luckraz H, Coulston J and Azzu A:
Cholesterol granuloma of the superior mediastinum. Ann Thorac Surg.
81:1509–1510. 2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Letter H, Komforti M, Maxwell R and
Maimone S: Cholesterol granuloma of the breast: A case report.
Radiol Case Rep. 18:3009–3013. 2023.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Hao S, Dong S, Li H, Liu S, Chen H and
Zhang Z: Case report: Cholesterol granuloma of femur. Front Surg.
9(944499)2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Lowenthal SB, Goldstein AM and Terry R:
Cholesterol granuloma of tunica vaginalis simulating testicular
tumor. Urology. 18:89–90. 1981.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Farina Perez LA, Menendez P and Macho V:
Hydrocele and cholesterol granuloma of the tunica vaginalis
simulating a tumor in echography. Actas Urol Esp. 22:70–73.
1998.PubMed/NCBI(In Spanish).
|
|
15
|
Spajic B, Cupic H, Stimac G, Brigic I,
Kruslin B and Kraus O: Cholesterol granuloma of the right
epididymis mimicking an acute scrotum. Asian J Androl. 8:749–750.
2006.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Doi H, Naka Y, Matsuda T, Harada T and
Komatz Y: A case of cholesterol granuloma with hematoma of tunica
albuginea. Hinyokika Kiyo. 39:193–195. 1993.PubMed/NCBI(In Japanese).
|
|
17
|
Albakheet N, Al-Shawi Y, Bafaqeeh M,
Fatani H, Orz Y and Shami I: Familial hypercholesterolemia with
bilateral cholesterol granuloma: A case series. Int J Surg Case
Rep. 62:135–159. 2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Muhialdeen AS, Ahmed JO, Baba HO, Abdullah
IY, Hassan HA, Najar KA, Mikael TM, Mustafa MQ, Mohammed DA, Omer
DA, et al: Kscien's List; A New Strategy to Discourage Predatory
Journals and Publishers (Second Version). Barw Med J. 1:24–26.
2023.
|