Introduction
Sialolithiasis is the most common disease of the
major salivary glands and accounts for ~30% of all salivary
disorders. Between 0.01 and 1.0% of the world population is
believed to be affected by the disease (1), and the incidence is higher among
males aged between 30 and 60 years. The most common location is the
submandibular gland, the duct being more frequently affected than
the parenchyma (2,3). Sialolithiasis is characterized by
obstruction of the salivary secretion by a calculus. This is
associated with pain and inflammation and in some occasions with an
infection of the affected gland. In a few cases, when the sialolith
is small and located near the orifice of the duct, it may be
removed following a widening of the orifice with a lacrimal probe.
Intraglandular sialoliths require submandibular sialadenectomy or
partial parotidectomy. Clinical, radiographic findings are
important in determination of the precise location and size in
order to indicate the right treatment for the individual
patient.
A case is described here which is of interest
because the large sized salivary stone is rarely located in the
parenchyma of submandibular glands.
Case report
A 45-year-old female who had no significant medical
history was referred to the Department of Oral and Maxillofacial
Surgery (Kyung Hee University Dental Hospital at Gangdong, Seoul,
Korea) with the chief complaints of pain in the right submandibular
region and a dry mouth, which had started one week previously.
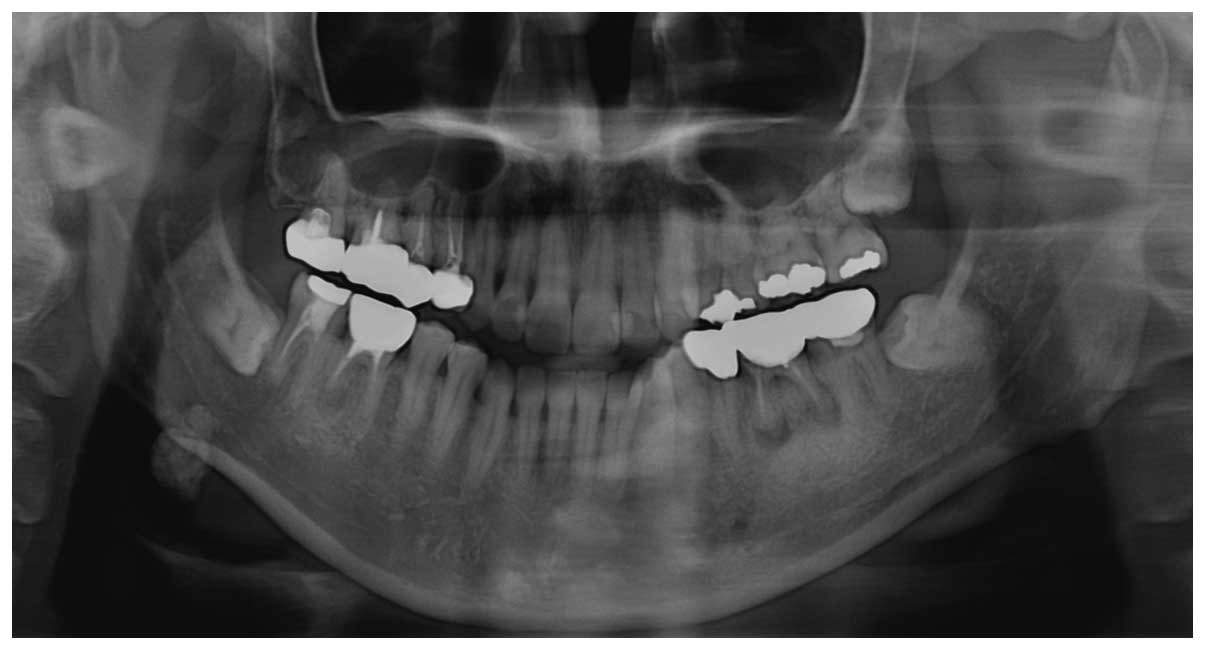
Clinical examination revealed a swelling and tenderness in the
right submandibular region. Panoramic radiography showed a
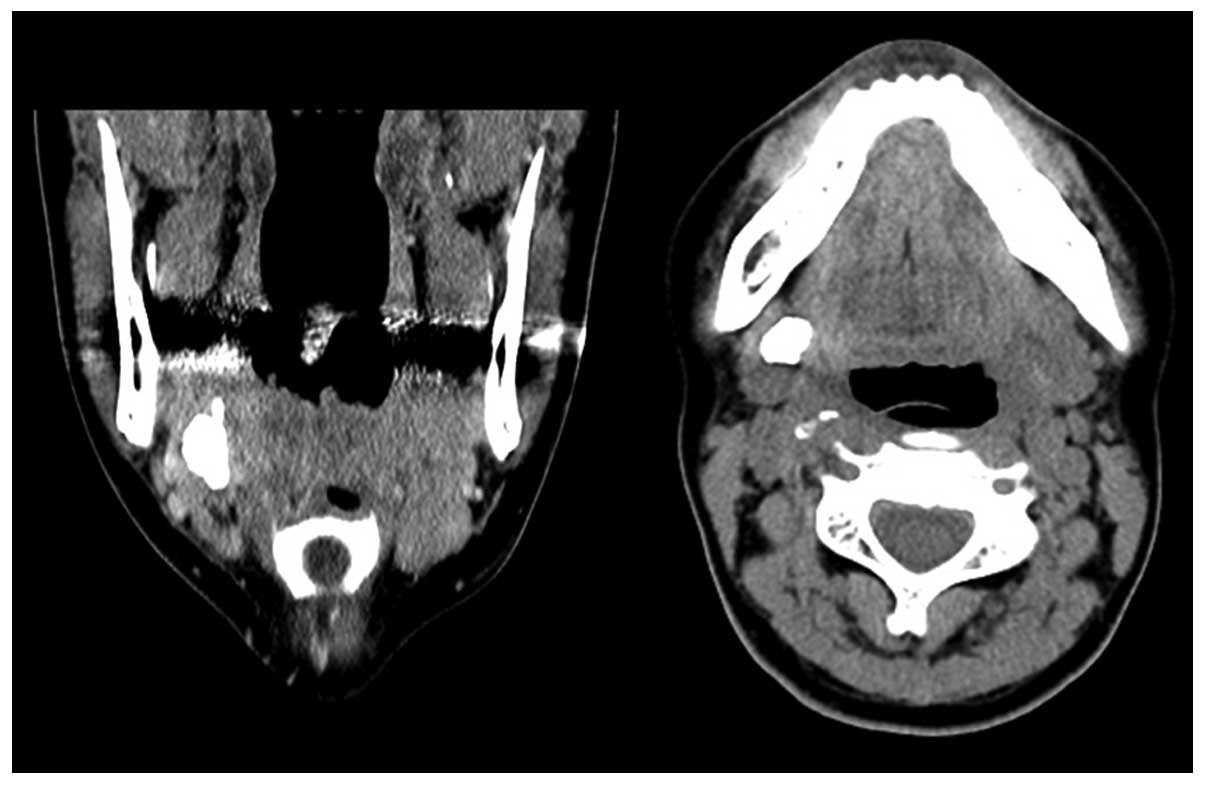
radiopaque mass in the submandibular area (Fig. 1). A few days later, computed
tomography was performed, revealing the stone in the right
submandibular gland (Fig. 2). We
diagnosed this as sialolithiasis on the right submandibular
gland.
Surgery to treat the sialolithiasis was subsequently
completed extraorally under general anesthesia, due to its
location. During surgery, sialoadenectomy was performed around the
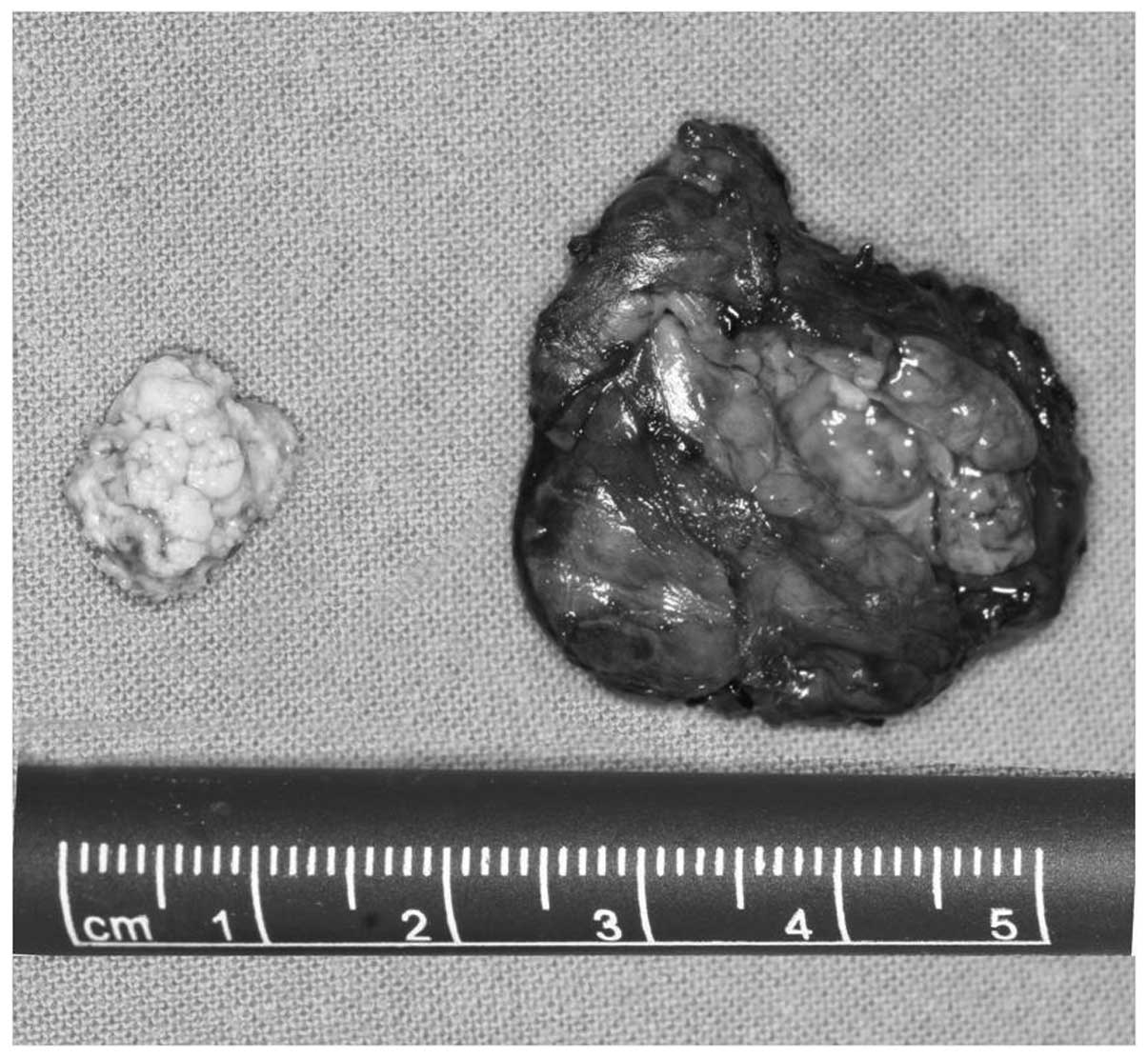
muscle and the branch of the facial nerve. The main specimen
enucleated was an excised submandibular gland, measuring 32×25 mm.
The brownish stone was present in the parenchyma of the
submandibular gland, measuring 14×10 mm (Fig. 3).
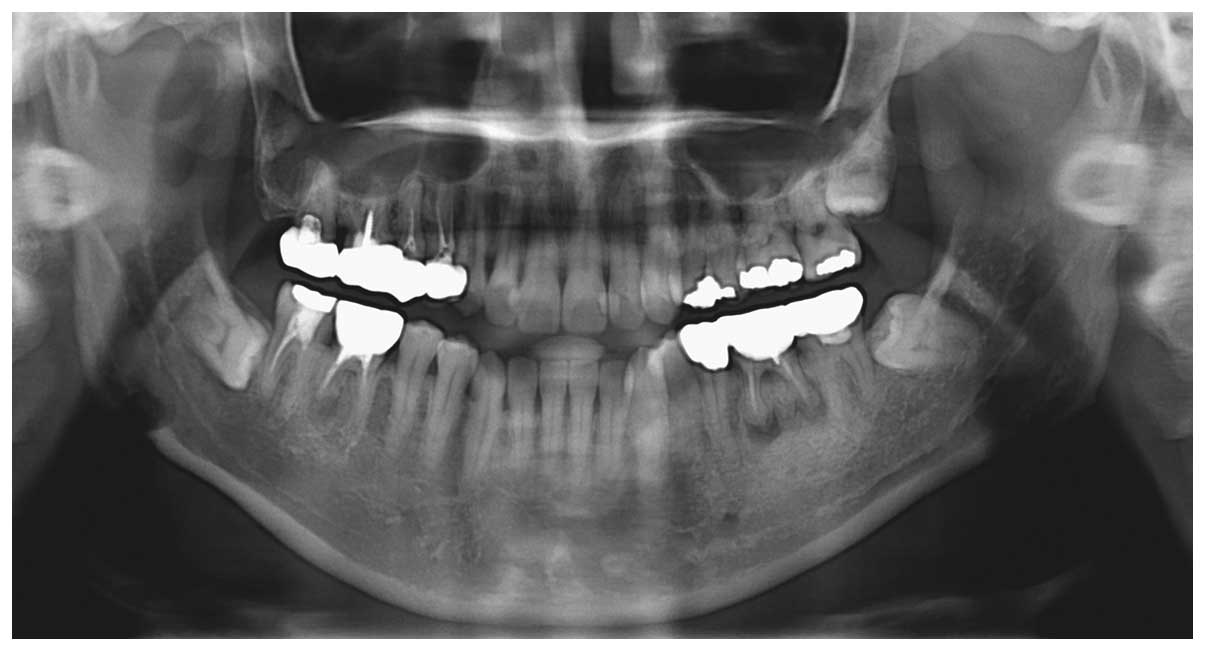
The postoperative follow-up radiograph showed
favorable removal of the salivary stone (Fig. 4). The symptoms and pain of the
patient disappeared following surgery and complete healing of the
surgical site was observed approximately three weeks subsequently.
Informed consent was obtained from the patient and the pateint’s
family.
Discussion
Sialolithiasis is a frequently occurring disease of
the salivary glands that is characterized by the obstruction of
salivary secretion by a calculus. This is associated with pain and
inflammation and, in certain cases, infection of the affected gland
may also be present (4). Swelling
is the most common symptom, followed by pain, fever and pus
secretion (5).
The size of salivary calculi varies from small
particles, described as salivary sand, to large concrement
formations. The average size of the salivary calculi lies between
3.3 and 17.9 mm (6). According to
Lutsmann et al (7),
sialoliths measuring <10 mm account for 78.8% of cases, while
those measuring 10–15 and >15 mm account for 13.6 and 7.65% of
cases, respectively. In the present study, the sialolith measured
14×10 mm in size. Salivary calculi are usually located in the ducts
of glands and in the hilus, whereas sialoliths on the parenchyma
occur in 9–17% of all cases, as stated in previous studies
(1,7,8).
The treatment of choice for sialolithiasis is the
removal of the obstructing stone by an intraoral approach. In
certain instances this method may also be applied for sialoliths
located in the hilus of the submandibular gland. In a few cases,
when the sialolith is small and located near the orifice of the
duct, the sialolith may be removed following a widening of the
orifice with a lacrimal probe. Intraglandular sialoliths require
submandibular sialoadenectomy or partial parotidectomy (7,9). In
the present case, submandibular sialoadenectomy was performed, as
the sialolith was large and located in the parenchyma of the
gland.
The patient in the present case presented with
typical symptoms, and the findings of clinical and radiographic
examination were also typical. The diagnosis was made by clinical
and radiographic examination, and sialoadenectomy was selected as
the treatment method due to the location of the stone. The
presented case illustrates the requirement for proper diagnosis and
treatment of choice in cases of salivary gland disease.
Postoperative follow-up is essential to ensure the patient is
symptom- and stone-free in the long-term.
In conclusion, clinical and radiographic findings
are important in determining the precise location and size of the
sialolith in order to indicate the right treatment for the
individual patient.
References
|
1
|
Andretta M, Tregnaghi A, Prosenikliev V
and Staffieri A: Current opinions in sialolithiasis diagnosis and
treatment. Acta Otorhinolaryngol Ital. 25:145–149. 2005.PubMed/NCBI
|
|
2
|
Grases F, Santiago C, Simonet BM and
Costa-Bauzá A: Sialolithiasis: mechanism of calculi formation and
etiologic factors. Clin Chim Acta. 334:131–136. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Austin T, Davis J and Chan T:
Sialolithiasis of submandibular gland. J Emerg Med. 26:221–223.
2004. View Article : Google Scholar
|
|
4
|
Antoniadis D, Mendonidou L, Papanayotou P
and Trigonidis G: Clinical study of sialolithiasis. Findings from
100 cases. Hell Stomatol Chron. 33:245–251. 1989.(In Greek).
|
|
5
|
Levy DM, Remine WH and Devine KD: Salivary
gland calculi. Pain, swelling associated with eating. JAMA.
181:1115–1119. 1962. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Anneroth G, Eneroth CM and Isacsson G:
Morphology of salivary calculi. The distribution of the inorganic
component. J Oral Pathol. 4:257–265. 1975. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lustmann J, Regev E and Melamed Y:
Sialolithiasis. A survey on 245 patients and a review of the
literature. Int J Oral Maxillofac Surg. 19:135–138. 1990.PubMed/NCBI
|
|
8
|
Zenk J, Koch M, Klintworth N, König B,
Konz K, Gillespie MB and Iro H: Sialendoscopy in the diagnosis and
treatment of sialolithiasis: a study on more than 1000 patients.
Otolaryngol Head Neck Surg. 147:858–863. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yoshimura Y, Morishita T and Sugihara T:
Salivary gland function after sialolithiasis: scintigraphic
examination of submandibular glands with 99mTc-pertechnetate. J
Oral Maxillofac Surg. 47:704–711. 1989. View Article : Google Scholar
|