Introduction
Multiple myeloma (MM) is a neoplastic disease
characterized by the proliferation and accumulation of B
lymphocytes and plasma cells that synthesize monoclonal
immunoglobulin (M component). Monoclonal plasma cell neoplasms
include MM, solitary plasmacytoma, Waldenström's macroglobulinemia,
and gammapathies associated with lymphoproliferative syndromes.
In 95% of the cases, MM is demonstrable with an
increase of the M component in the serum and/or in the urine
(1,2). The disease may involve the bone marrow
as well as soft tissues; its primary location is usually
represented by a bone marrow hematopoietic content area, with
secondary involvement of an extramedullary site, which is often
represented by the upper aerodigestive tract (3). Primary localization in an
extramedullary site is less frequent, isolated, or associated with
a secondary location in the bone marrow. MM with a laryngeal
localization represents 1% of the malignancies that affect this
organ and predominantly affects men between the sixth and seventh
decades of life, with a male:female ratio of 2:1 (1).
Case report
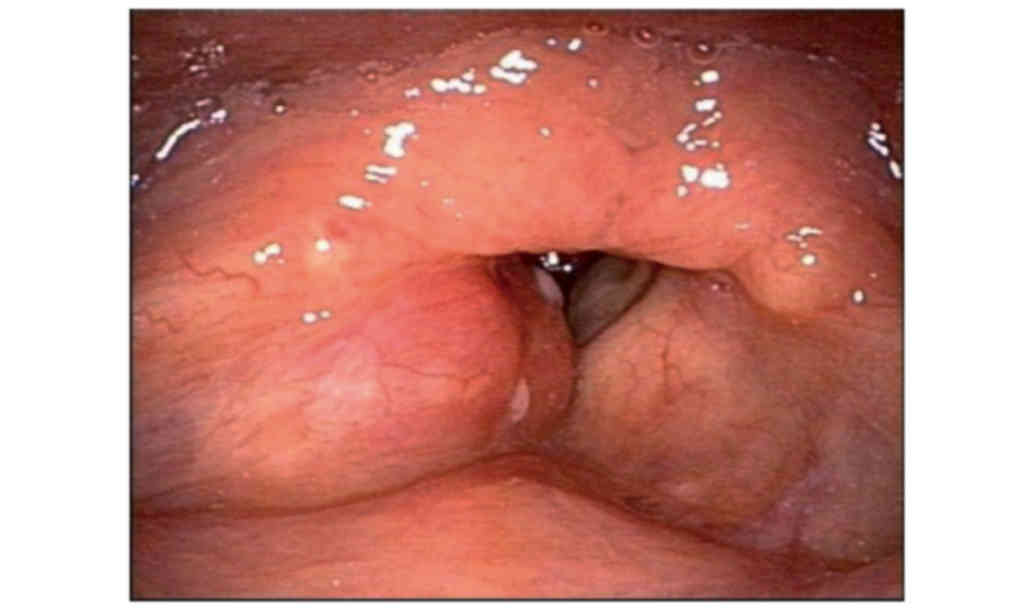
A 68-year-old male non-smoker with a clinical
history of dyspnea, dysphonia and dysphagia, exhibited worsening of
his condition 4 months prior to seeking medical advice.
Laryngoscopic examination revealed a lesion involving the right
glottis and right vestibular (false) vocal fold, with absence of
ipsilateral laryngeal motility and constriction of the airway
(Fig. 1).
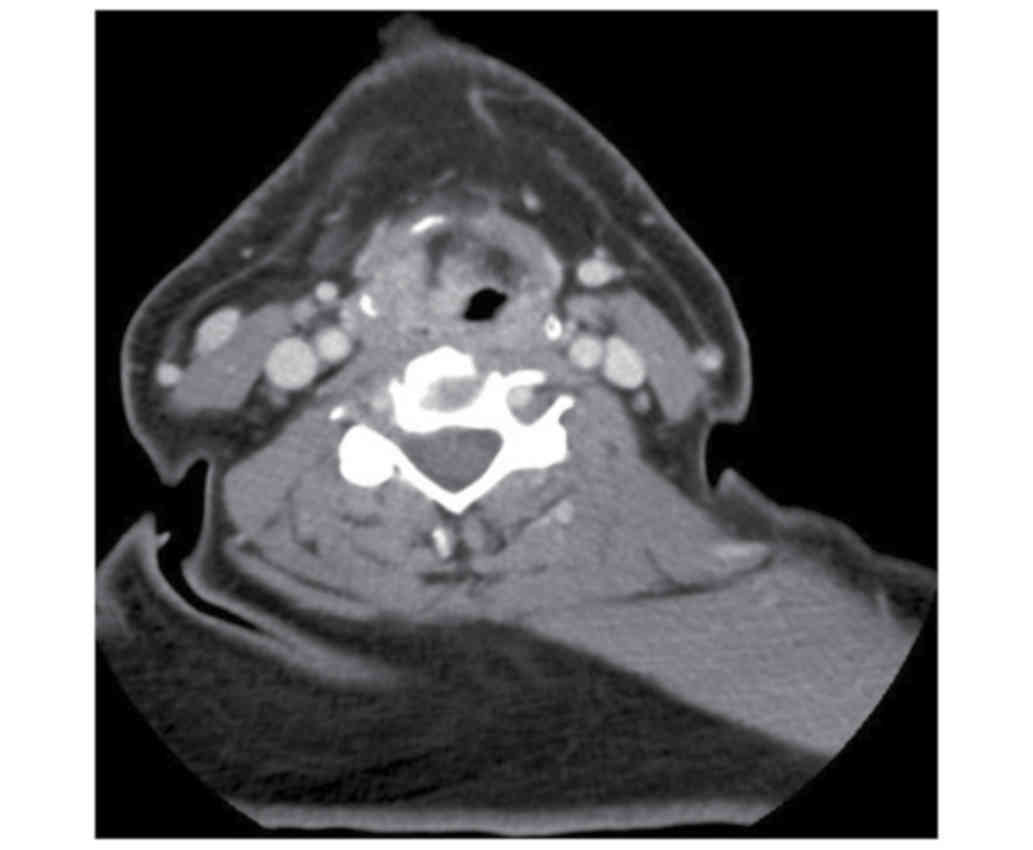
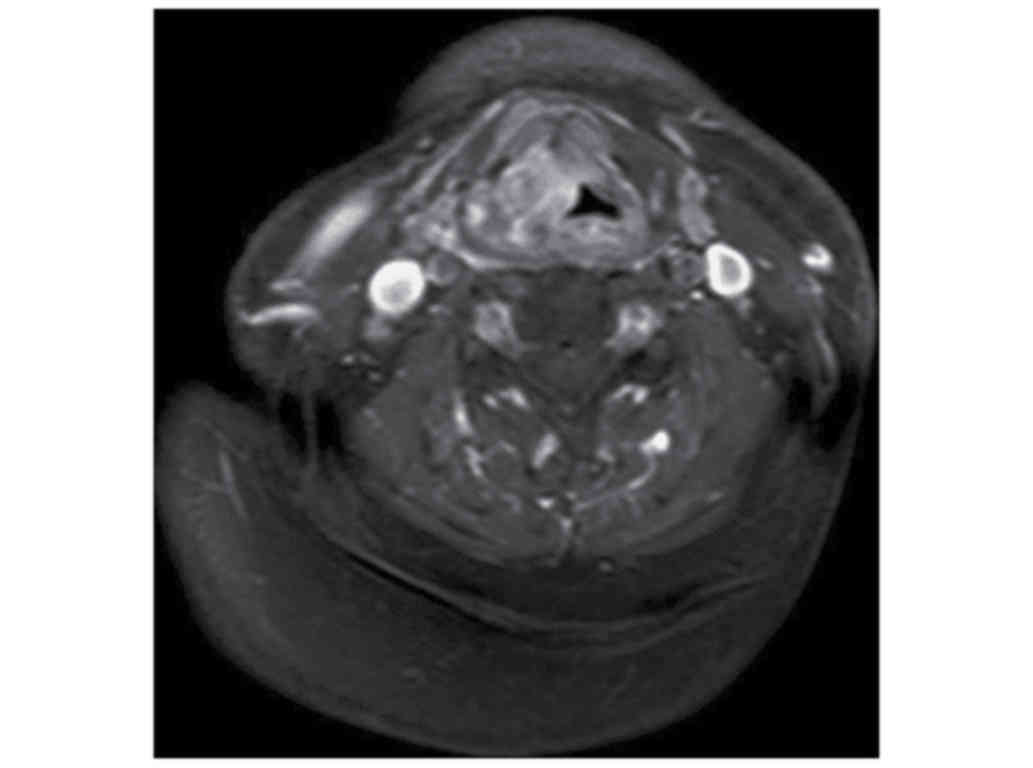
Computed tomography (CT) and magnetic resonance
imaging (MRI) revealed a gross swelling infiltrating the right
glottis and right false vocal fold, sized 33×19×33 mm, with
sub-centimeter laterocervical lymph nodes bilaterally (Figs. 2 and 3). A whole-body CT revealed no pathological
findings. For diagnostic purposes and to resolve the severe
dyspneic symptoms, tracheostomy with targeted biopsies (later found
to be negative for malignancy) was performed in July 2015. Due to
the persistence of the lesion, which was refractory to treatment
with anti-inflammatory drugs and antibiotics, new biopsies were
collected during direct laryngoscopy after 1 month; the subsequent
histological examination revealed a ‘benign laryngeal mucosa,
infiltrated by lymphocytes, plasma cells and granulocytes, a lamina
propria rich in mixed glands (mostly mucous) and excretory ducts,
and striated muscle’. Given the inconclusive diagnosis, further
biochemical, clinical and immunohematological tests were performed
and the results were as follows: Negative for Bence Jones protein;
increased α2 and β1 paraproteins (by 13.90 and 25.50%,
respectively); and decreased albumin, γ-globulin and A/G ratio (by
42.90, 7.60% and 0.75, respectively) on the proteinogram. IgAκ was
found in the subsequent immunofixation, also confirmed by
immunohistochemistry of a bioptic specimen that was positive for
CD138 (Fig. 4).
The bone marrow contained 40% plasma cells, which
were also positive for CD138. Staging by positron emission
tomography/CT imaging, performed 1 month after whole-body CT,
revealed localization of the disease in the V right rib. At the end
of the diagnostic process (September 2015) the patient underwent 6
cycles of chemotherapy with bortezomib (Velcade), thalidomide and
dexamethasone (VTD scheme), achieving partial remission of the
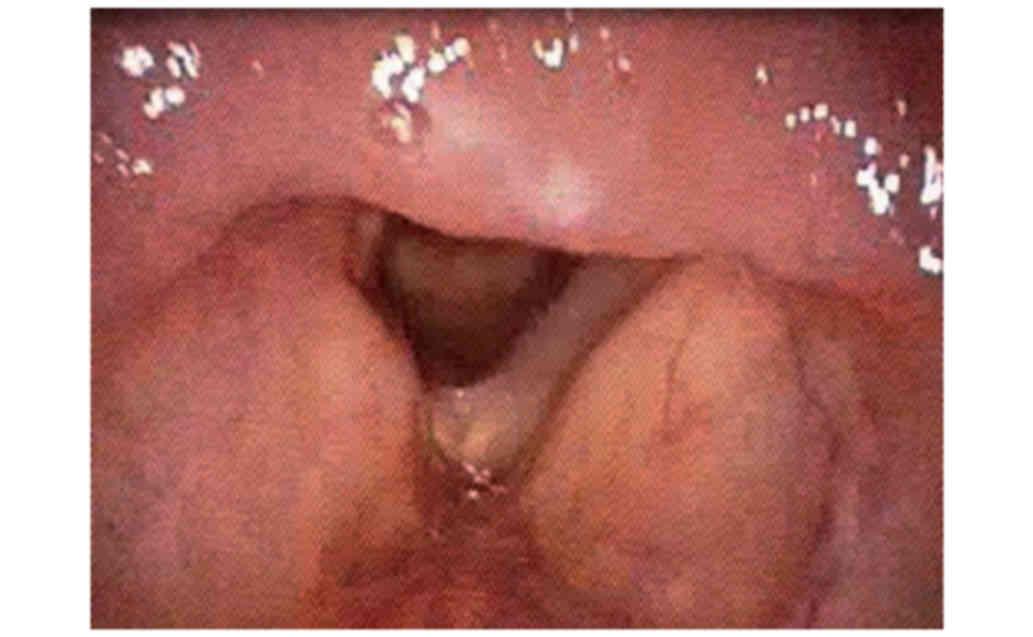
disease. At the end of the chemotherapy (March 2016), an endoscopic
examination (Fig. 5) and MRI control
showed a reduction in the dimensions of the pathological tissue
(20×10×12 mm), which infiltrated the right false vocal fold and
glottis and extended to the anterior commissure, with right
persistent disease in the right paraglottic space and signal
alteration of the thyroid cartilage. The relief of the airway
constriction allowed for decannulation of the patient in April
2016, after a median follow-up of 6 months. The patient is
currently on maintenance treatment with interferon and steroids and
the next laryngoscopic control is scheduled for January 2017.
Discussion
Laryngeal localization of MM is extremely rare as a
primary or secondary site to a primary marrow localization, which
is a more frequent occurrence. The etiology is not known. Point
mutations of the N-ras and K-ras genes, as well as mutations or
deletions of the tumor suppressor genes p53 and Rb-1, are delayed
molecular events that may play a role in the onset and progression
of this disease (1). In decreasing
order of frequency, the most commonly affected laryngeal areas are
the epiglottis, glottis, false vocal folds, aryepiglottic folds and
thyroid cartilage (3). The disease
rarely presents with a sudden onset. Dyspnea, dysphonia and
dysphagia are correlated with disease localization (2,4). The
lesion may present as a polypoid mass or swelling involving the
entire organ, with a smooth, benign mucosal surface. The
differential histological diagnosis may be challenging, as plasma
cell infiltrates may also be encountered in various benign
conditions, such as chronic inflammatory diseases, inflammatory
polyps and amyloid deposits (5,6).
Therefore, histological diagnosis should be supported by
hematological and radiological examination. The blood count in MM
patients may reveal anemia and/or leukopenia and/or
thrombocytopenia. In 95% of the MM cases, electrophoresis and
immunofixation indicate the presence of an M component. A urine
test is only useful for detecting light chains (Bence Jones
protein). Bone marrow biopsy shows an excess of plasma cells
(>10% of the total nucleated cell population), which may extend
to total replacement of the normal myeloid parenchyma.
Immunohistochemistry is crucial for determining positivity of B
lymphocytes and plasma cells for the CD138 marker in the bone
marrow as well as in extramedullary sites (3,5). For
prognostic purposes, the determination of the serum concentration
of b2-microglobulin is relevant (1).
The overall clinical assessment of the patient applies diagnostic
imaging (chest X-ray and whole-body CT and MRI), which is useful in
determining the possible presence of the disease in other locations
and in evaluating lymph node stations. The therapy mainly includes
radiation and/or chemotherapy, with subsequent transplantation of
autologous or allogeneic stem cells (1,7).
Despite its low incidence, primary laryngeal
localization of MM should always be considered in the presence of a
laryngeal mass of undetermined clinical nature.
References
|
1
|
McKenna RW, Kyle RA, Kuehl WM, Grogan TM,
Harris NL and Coupland RW: Plasma cell neoplasmsWHO Classification
of Tumours of Haematopoietic and Lymphoid Tissues. Swerdlow SH,
Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J and
Vardiman JW: 2. IARC; Lyon: pp. 200–213. 2008
|
|
2
|
Nofsinger YC, Mirza N, Rowan PT, Lanza D
and Weinstein G: Head and neck manifestations of plasma cell
neoplasms. Laryngoscope. 107:741–746. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mitchell HK, Garas G, Mazarakis N and
McGlashan J: Extramedullary relapse of multiple myeloma in the
thyroid cartilage. BMJ Case Rep 2013. pii.bcr2013200689. 2013.
|
|
4
|
Nampoothiri MP, Kumar KP and Sajina VK:
Multiple myeloma presenting as stridor: A case report. Indian J
Otolaryngol Head Neck Surg. 58:111–112. 2006.PubMed/NCBI
|
|
5
|
Grobman AB, Vivero RJ, Campuzano-Zuluaga
G, Ganjei-Azar P and Rosow DE: Laryngeal involvement of multiple
myeloma. Case Rep Oncol Med. 2012:2578142012.PubMed/NCBI
|
|
6
|
Aslan I, Yenice H and Baserer N: An
indolent course of multiple myeloma mimicking a solitary thyroid
cartilage plasmacytoma. Eur Arch Otorhinolaryngol. 259:84–86. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Michalaki VJ, Hall J, Henk JM, Nutting CM
and Harrington KJ: Definitive radiotherapy for extramedullary
plasmacytomas of the head and neck. Br J Of Radiology. 76:738–741.
2003. View Article : Google Scholar
|