Introduction
Cancer patients frequently present with metabolic
disorders, including cachexia, with hallmarks of atrophy of fat
(1). Apart from the systemic
stimulatory effects of obesity on tumor growth, adipocytes directly
influence tumor behavior. The omentum is primarily composed of
adipocytes. Of note, intra-abdominal tumors have a predilection for
omentum metastasis (2). Nieman et
al (3) demonstrated that human
omental adipocytes provide energy for rapid tumor growth and
promote homing, migration and invasion of ovarian cancer cells. In
this process, adipokines, including interleukin (IL)-8 serve
important roles. In obese patients, adipose stromal cells (ASCs)
are expanded and subsequently migrate from the endogenous white
adipose tissue to tumors, where they are incorporated into blood
vessels as pericytes (4). Further
evidence has shown that cancer-associated adipocytes modify the
cancer cell phenotype leading to a more aggressive behavior
(5). Of note, lipid oxidative
metabolic programs are essential for regulatory T cells (6) and M2-type macrophages (7), which are classical immune suppressive
subsets facilitating tumor growth. Apolipoprotein E (ApoE),
targeted by a set of microRNAs, has been demonstrated to be an
antiangiogenic and metastasis-suppressive factor in melanoma
(8). ApoA-I binding protein
accelerates cholesterol efflux from endothelial cells and regulates
angiogenesis (9). However, whether
chemotherapy influences lipid levels remains to be fully
elucidated.
Hypertriglyceridemia (HTG) can occur in patients
with cardiovascular diseases, diabetes mellitus, obesity, metabolic
syndrome or chronic renal failure (10). Pregnancy, alcohol abuse and certain
medications have also been reported to increase the TG
concentration (11,12). Elevated plasma levels of TG increase
the risk of cardiovascular diseases, diabetes, obesity and insulin
resistance (13,14). Furthermore, elevated serum TG levels
are associated with hepatosplenomegaly, xanthomas, neuropathy,
lipemia retinalis and even hyperlipemic abdominal crisis (15,16). Of
note, HTG is a well-recognized cause of acute pancreatitis
(17,18), which has a high mortality rate
(19).
At our clinic, numerous patients who experienced
transient HTG after treatment with paclitaxel and cisplatin (TP)
chemotherapy were encountered. The present study reported on three
patients with transient HTG after receiving TP chemotherapy. TG
returned to baseline at chemotherapy intermission. No patients had
any history of HTG or exhibited any evidence of pancreatitis or
other complications of HTG. No regular elevation of any other serum
lipids, including cholesterol, high-density lipoprotein (HDL) and
low-density lipoprotein (LDL), was observed. However, treatment of
mice with TP decreased serum TG and slightly increased cholesterol.
The present study suggested that, to avoid TG-associated
complications, clinicians must monitor TG levels during
chemotherapy.
Methods
Clinical cases
Retrospective data from the electronic medical
records of West China Hospital (Chengdu, China) were collected. All
three patients selected received chemotherapy at the Cancer Center
of West China Hospital.
Animal study
C57BL/6 and BALB/c mice (6–8 weeks old) were
purchased from Beijing HFK Bioscience Co., Ltd. (Beijing, China).
Mice were maintained under pathogen-free conditions with individual
ventilation (temperature: 21–27°C; humidity: 40–60%), with a
light/dark cycle of 12 h, and ad libitum access to food and
water. The study was approved by the ethics committee of Sichuan
University (Chengdu, China). All animal experiments were performed
according to protocols approved by the Institutional Animal Care
and Use Committee of Sichuan University. A total of 10 mg/kg
paclitaxel was administered on day 1, and 5 mg/kg cisplatin was
administered on days 1, 2 and 3. Chemotherapeutic drugs were
administered intravenously to female BALB/c mice (n=3 for each
group) and intraperitoneally to C57BL/6 mice. Mice in the control
group were administered normal saline. At day 4, blood was
collected, the mice were sacrificed and levels of the serum lipids
were examined at Chengdu GLP Center (Chengdu, China). The
chemotherapeutic agents, paclitaxel and cisplatinum, were obtained
from West China Hospital (Chengdu, China).
Statistical analysis
Statistical analysis was performed using Student's
t-test between two groups. P<0.05 was considered to indicate a
statistically significant difference.
Results
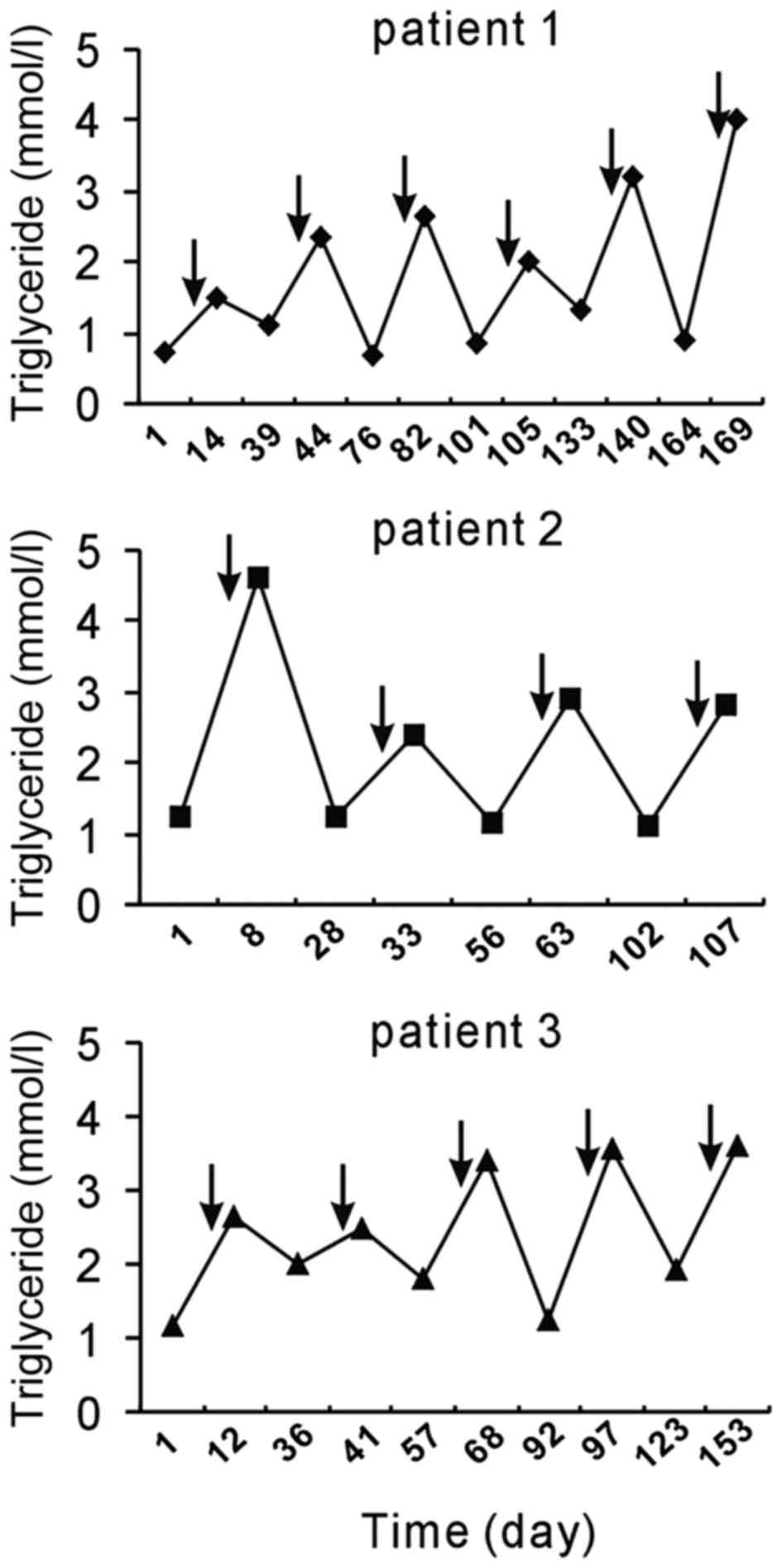
TP chemotherapy induces serum TG
fluctuation in cancer patients
The following three noteworthy cases were
encountered at West China Hospital (Chengdu, China). A 47-year-old
female patient (patient 1) was diagnosed with lung squamous
carcinoma. Since the tumors had invaded the laryngeal recurrent
nerve, surgery was not possible and chemotherapy was applied. TP
was administered six times and the patient received concurrent
radiotherapy. An elevation of serum TG levels was observed each
time following chemotherapy. Of note, the HTG was transient and TG
levels dropped to normal levels prior to the next cycle of
chemotherapy (Fig. 1).
A 66-year-old female patient (patient 2) who had a
3-month history of progressive dysphagia was referred to West China
Hospital and diagnosed with esophageal squamous carcinoma. Upon
admission to the West China Hospital, the patient had normal serum
TG levels. The patient received four cycles of TP chemotherapy and
radiotherapy after the third cycle. The patient had no history of
dyslipidemia; however, she experienced HTG following every
administration of TP (Fig. 1).
A 57-year-old male patient (patient 3) with a
history of synovial carcinoma in the left lower extremity was
admitted to West China Hospital due to the recurrence and lung
metastasis of synovial carcinoma. The patient had undergone
excision of synovial carcinoma 13 years previously and upper left
pulmonary wedge resection 7 months previously. Thereafter, the
patient received 5 cycles of TP chemotherapy. He exhibited HTG
after each treatment with TP chemotherapy, which decreased in the
subsequent interval (Fig. 1).
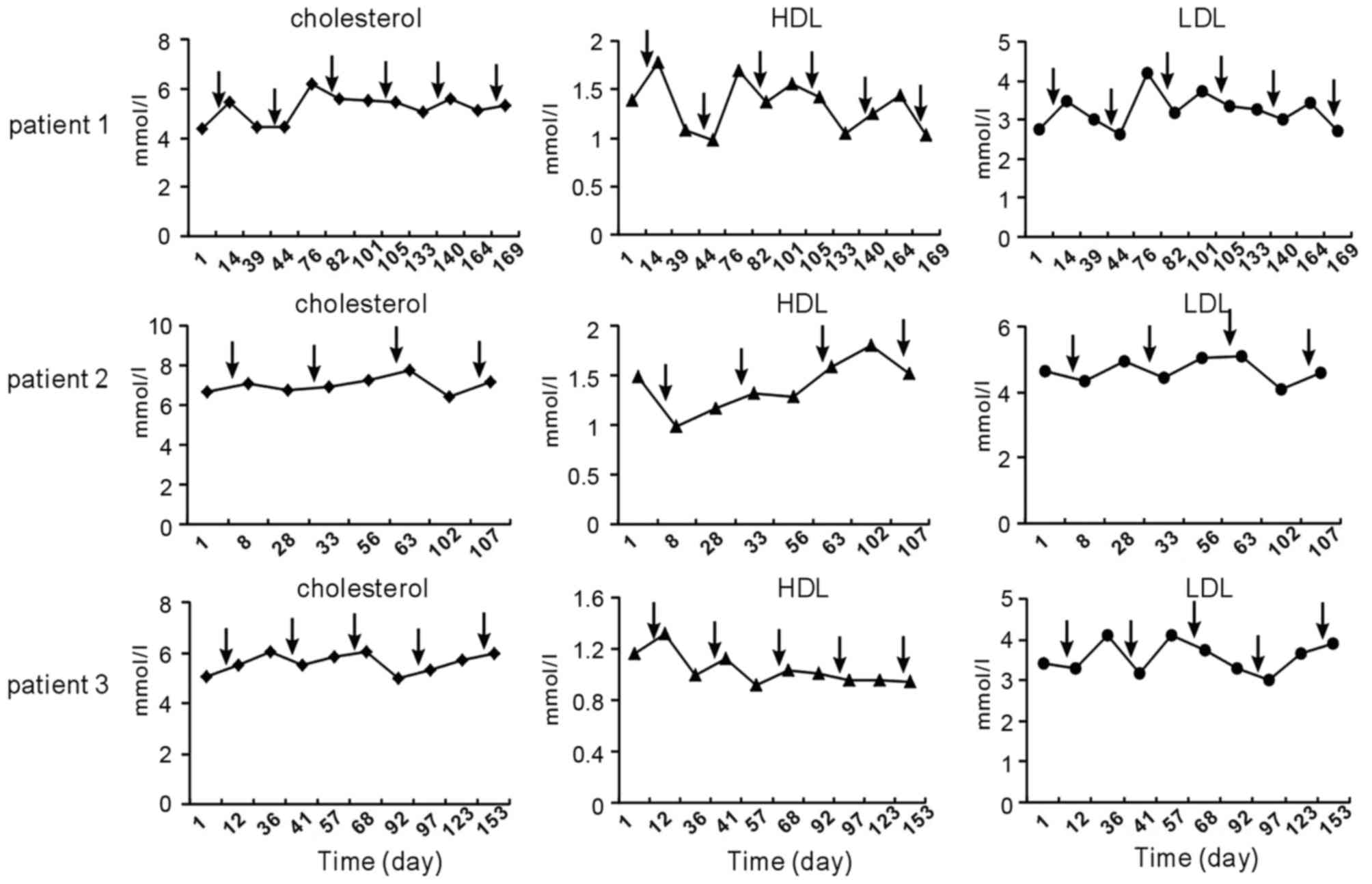
Triglyceride disorders are not
accompanied by any other lipid disorders
Since chemotherapy with TP influenced serum TG
levels, further review of the patients' medical records was
performed to determine whether dyslipidemia was also present for
cholesterol, LDL and HDL. The trend of these lipids observed
following chemotherapy was not similar to that of serum TG
(Fig. 2).
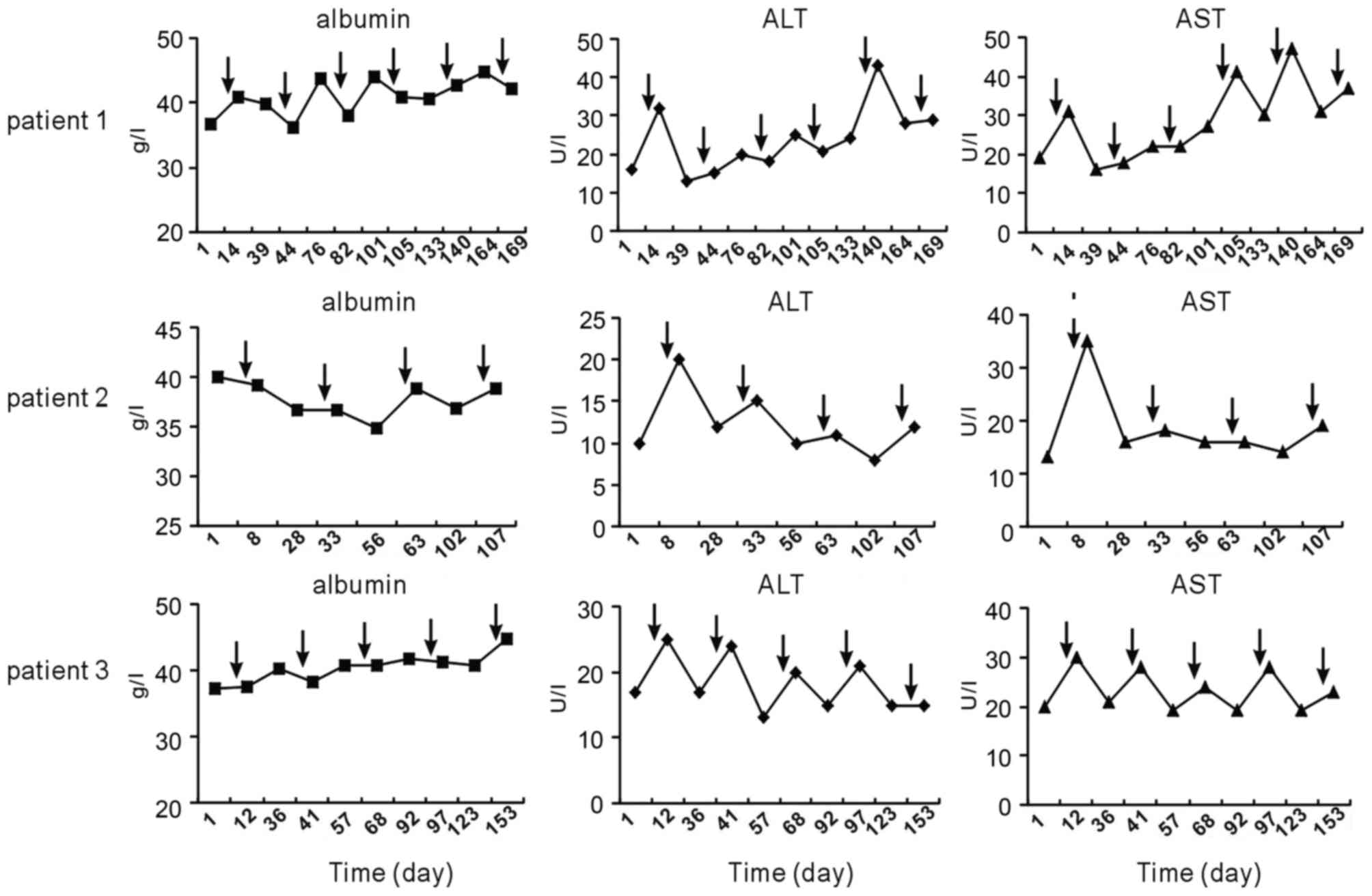
Influence of TP chemotherapy on liver
and kidney function
Furthermore, serum levels of albumin, ALT and AST
after chemotherapy were compared at various time-points. It was
revealed that chemotherapy induced a slight elevation of ALT and/or
AST in each of the three patients; however, levels almost remained
in the normal range. Unlike ALT and AST, albumin levels did not
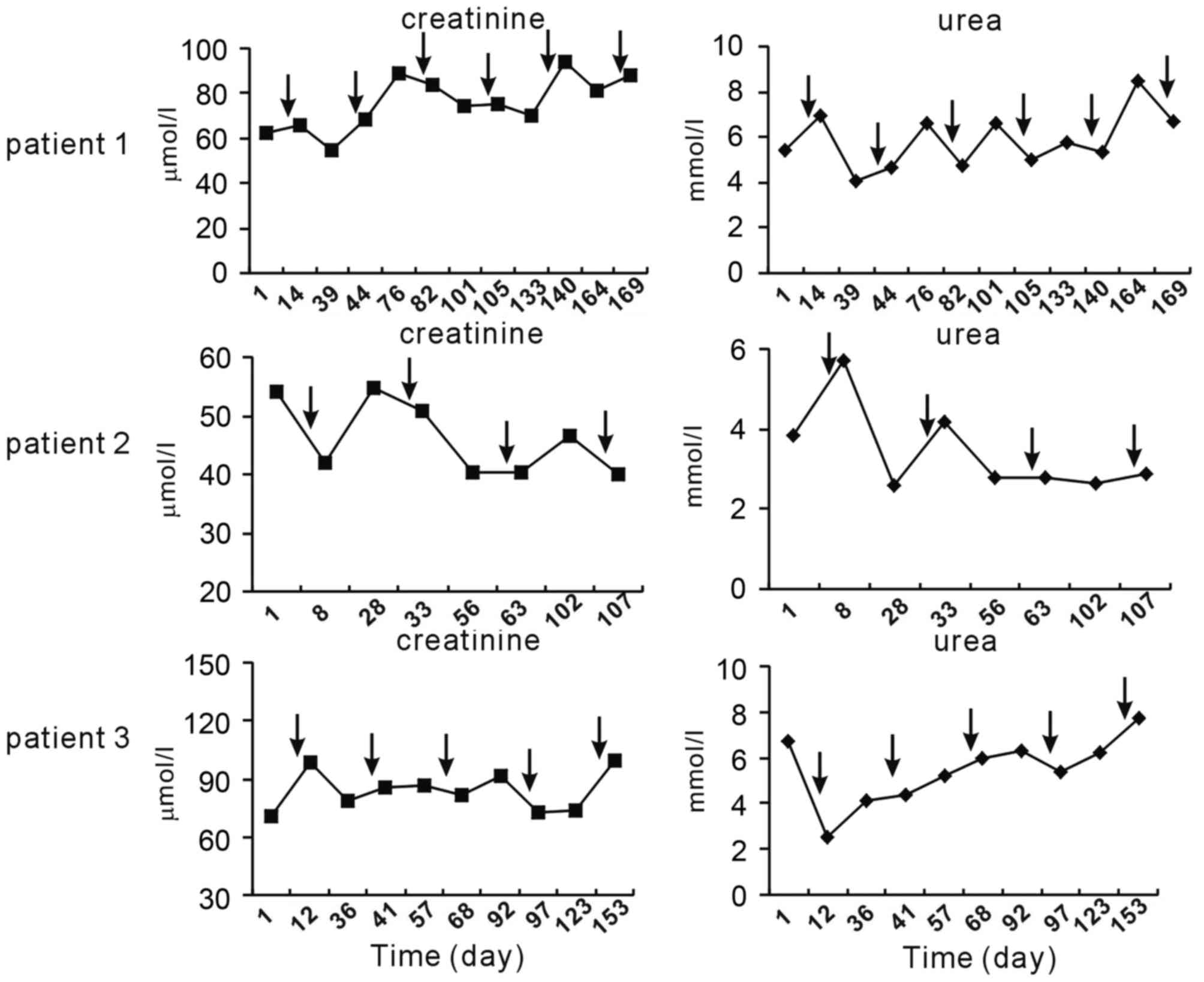
fluctuate following chemotherapy (Fig.
3). In addition, no regular elevation of creatinine and urea
was observed following TP chemotherapy (Fig. 4).
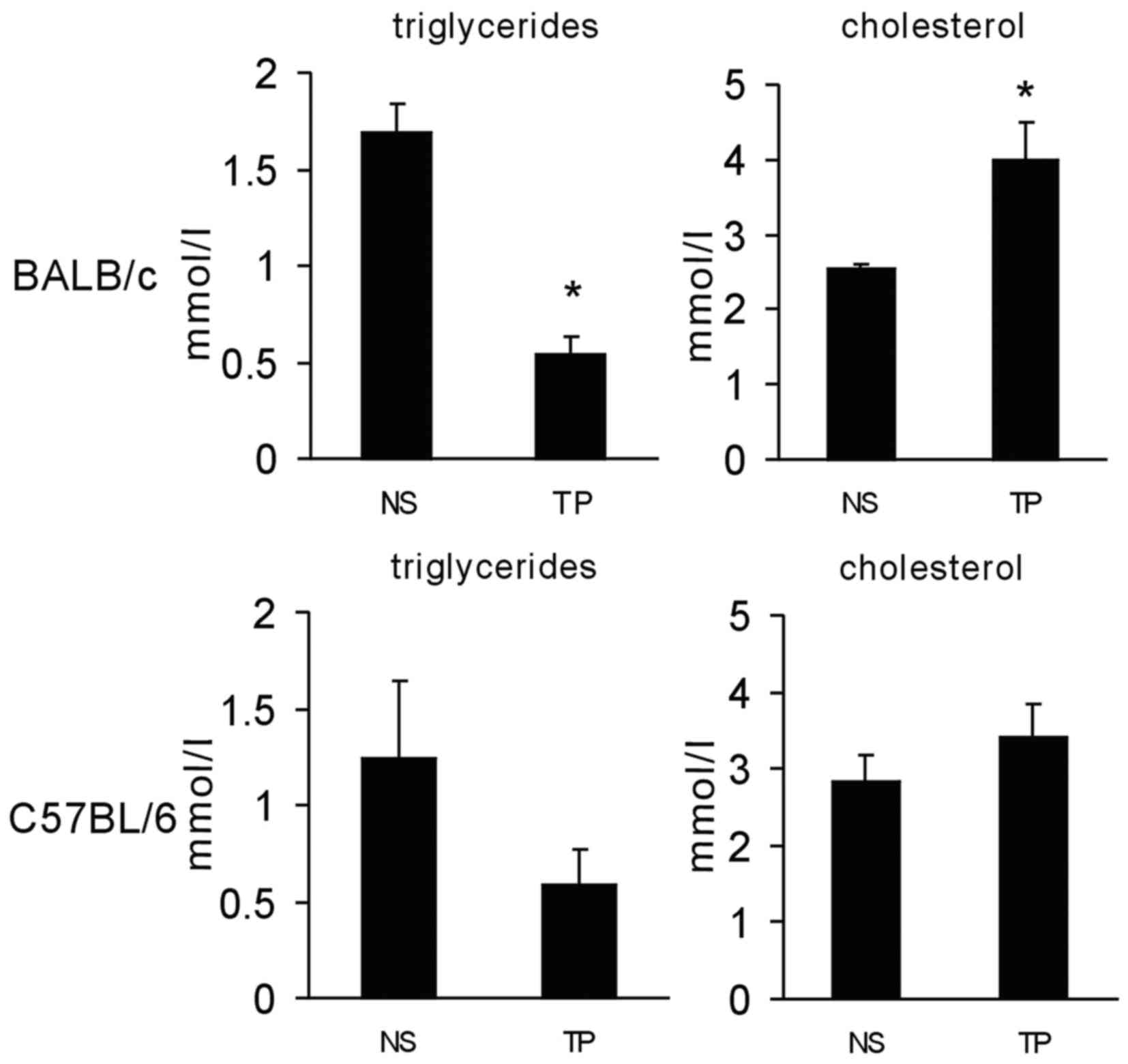
Animal model of TP
chemotherapy-induced lipid disorder
To investigate whether TP chemotherapy causes a
lipid disorder in experimental animals, BALB/c mice were
administered intravenously with chemotherapeutic drugs. To mimic
the clinical settings, the animals were administered paclitaxel (10
mg/kg body weight) at day 1 and cisplatin (5 mg/kg body weight) at
days 1, 2 and 3. At day 4, serum from the mice was obtained to
evaluate the TG and cholesterol levels. TG was revealed to be
significantly decreased and cholesterol levels were increased
(Fig. 5). Furthermore, the same
experiment was performed on C57BL/6 mice with intraperitoneal
injection of the drugs. In C57BL/6 mice, the same trend was
observed as in BALB/c mice, while not reaching statistical
significance (Fig. 5). These results
suggested that TP chemotherapy caused lipid disorders in mice,
while they were not consistent with those in human subjects.
Discussion
The present study reported on three patients with
cancer who developed HTG following TP chemotherapy. No patient had
any history of or any pre-existing lipid abnormalities, and
exhibited no other predisposing factors, including chronic
alcoholism, diabetes mellitus or hypothyroidism. Typically, HTG
occurs in conjunction with low HDL levels and atherogenic small
dense LDL particles (20). However,
the present study found that the levels of physiologically
important plasma cholesterol, LDL and HDL were normal or only
minimally changed. The reason for the observed TG elevation remains
elusive. In the three patients, it was observed that ALT and/or AST
were transiently elevated after TP chemotherapy and showed a
similar trend to serum TG, while remaining in the normal range.
Therefore, the fluctuation of TG may have resulted from impaired
hepatic cellular function.
The significance of HTG in patients undergoing
chemotherapy has remained elusive. In a clinical trial reported by
Blumenschein et al (21) HTG
had a prognostic value for bexarotene-treated patients with
non-small cell lung cancer. Furthermore, the occurrence of
high-grade HTG was highly correlated with increased survival
(21). Of note, a marked elevation
of TG appeared to be causally linked to acute pancreatitis. Acute
pancreatitis induced by HTG usually occurs when serum TG levels
exceed 20 mmol/l (16,22). A TG serum level of >1,000 mg/dl
can be used to determine the required therapy (23). Failure to consider lipid levels as
the cause of disease can lead to clinical deterioration (24). In the present study, the serum TG
levels in most patients who received chemotherapy was <5 mmol/l.
However, there is evidence that serum TG levels as low as 343 mg/dl
(3.9 mmol/l) were able to trigger pancreatitis (25). Therefore, clinicians must be vigilant
of acute pancreatitis in all patients who receive TP therapy. As
HTG can impair the function of endothelial cells, it is necessary
to protect the endothelium when it is encountered during treatment
with TP chemotherapy.
Notably, the present study observed an elevation of
TG in patients following TP chemotherapy, whereas the opposite
phenomenon was observed in mice. To mimic the clinical settings,
mice were administered paclitaxel at day 1 and cisplatin at days 1,
2 and 3. On day 4, serum TG were reduced in the mice, while
cholesterol was increased. This difference from the observations in
human patients may have resulted from different species or
different dosage of chemotherapeutic agents.
In conclusion, the present study highlighted the
requirement for clinicians to consider severe dyslipidemia as a
possible side effect prior to initiating TP chemotherapy, which may
result in complications.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (no. 81501609), the National
Natural Science Foundation of China (no. 81301980), and the Chinese
Postdoctoral Science Foundation (no. 2015M582553).
References
|
1
|
Fearon KC, Glass DJ and Guttridge DC:
Cancer cachexia: Mediators, signaling, and metabolic pathways. Cell
Metab. 16:153–166. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Landen CN Jr, Birrer MJ and Sood AK: Early
events in the pathogenesis of epithelial ovarian cancer. J Clin
Oncol. 26:995–1005. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nieman KM, Kenny HA, Penicka CV, Ladanyi
A, Buell-Gutbrod R, Zillhardt MR, Romero IL, Carey MS, Mills GB,
Hotamisligil GS, et al: Adipocytes promote ovarian cancer
metastasis and provide energy for rapid tumor growth. Nat Med.
17:1498–1503. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang Y, Daquinag AC, Amaya-Manzanares F,
Sirin O, Tseng C and Kolonin MG: Stromal progenitor cells from
endogenous adipose tissue contribute to pericytes and adipocytes
that populate the tumor microenvironment. Cancer Res. 72:5198–5208.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dirat B, Bochet L, Dabek M, Daviaud D,
Dauvillier S, Majed B, Wang YY, Meulle A, Salles B, Le Gonidec S,
et al: Cancer-associated adipocytes exhibit an activated phenotype
and contribute to breast cancer invasion. Cancer Res. 71:2455–2465.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Michalek RD, Gerriets VA, Jacobs SR,
Macintyre AN, MacIver NJ, Mason EF, Sullivan SA, Nichols AG and
Rathmell JC: Cutting edge: Distinct glycolytic and lipid oxidative
metabolic programs are essential for effector and regulatory CD4+ T
cell subsets. J Immunol. 186:3299–3303. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Huang SC, Everts B, Ivanova Y, O'Sullivan
D, Nascimento M, Smith AM, Beatty W, Love-Gregory L, Lam WY,
O'Neill CM, et al: Cell-intrinsic lysosomal lipolysis is essential
for alternative activation of macrophages. Nat Immunol. 15:846–855.
2014. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pencheva N, Tran H, Buss C, Huh D,
Drobnjak M, Busam K and Tavazoie SF: Convergent multi-miRNA
targeting of ApoE drives LRP1/LRP8-dependent melanoma metastasis
and angiogenesis. Cell. 151:1068–1082. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fang L, Choi SH, Baek JS, Liu C, Almazan
F, Ulrich F, Wiesner P, Taleb A, Deer E, Pattison J, et al: Control
of angiogenesis by AIBP-mediated cholesterol efflux. Nature.
498:118–122. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ito Y, Azrolan N, O'Connell A, Walsh A and
Breslow JL: Hypertriglyceridemia as a result of human apo CIII gene
expression in transgenic mice. Science. 249:790–793. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hsia SH, Connelly PW and Hegele RA:
Successful outcome in severe pregnancy-associated hyperlipemia: A
case report and literature review. Am J Med Sci. 309:213–218. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Calza L, Manfredi R and Chiodo F:
Dyslipidaemia associated with antiretroviral therapy in
HIV-infected patients. J Antimicrob Chemother. 53:10–14. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Austin MA: Plasma triglyceride and
coronary heart disease. Arterioscler Thromb. 11:2–14. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Reaven GM: Banting lecture 1988. Role of
insulin resistance in human disease. Diabetes. 37:1595–1607. 1988.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Maher NG and Ramaswamykanive H: Use of
plasmapheresis in managing the diagnostic dilemma of symptomatic
hypertriglyceridemia. Case Rep Gastrointest Med.
2012:5013732012.PubMed/NCBI
|
|
16
|
Kyriakidis AV, Raitsiou B, Sakagianni A,
Harisopoulou V, Pyrgioti M, Panagopoulou A, Vasilakis N and
Lambropoulos S: Management of acute severe hyperlipidemic
pancreatitis. Digestion. 73:259–264. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Athyros VG, Giouleme OI, Nikolaidis NL,
Vasiliadis TV, Bouloukos VI, Kontopoulos AG and Eugenidis NP:
Long-term follow-up of patients with acute
hypertriglyceridemia-induced pancreatitis. J Clin Gastroenterol.
34:472–475. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yadav D and Pitchumoni CS: Issues in
hyperlipidemic pancreatitis. J Clin Gastroenterol. 36:54–62. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bollen TL, van Santvoort HC, Besselink MG,
van Leeuwen MS, Horvath KD, Freeny PC and Gooszen HG: Dutch Acute
Pancreatitis Study Group: The Atlanta Classification of acute
pancreatitis revisited. Br J Surg. 95:6–21. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Subramanian S and Chait A:
Hypertriglyceridemia secondary to obesity and diabetes. Biochim
Biophys Acta. 1821:819–825. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Blumenschein GR Jr, Khuri FR, von Pawel J,
Gatzemeier U, Miller WH Jr, Jotte RM, Le Treut J, Sun SL, Zhang JK,
Dziewanowska ZE and Negro-Vilar A: Phase III trial comparing
carboplatin, paclitaxel, and bexarotene with carboplatin and
paclitaxel in chemotherapy-naive patients with advanced or
metastatic non-small-cell lung cancer: SPIRIT II. J Clin Oncol.
26:1879–1885. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gan SI, Edwards AL, Symonds CJ and Beck
PL: Hypertriglyceridemia-induced pancreatitis. A case-based review.
World J Gastroenterol. 12:7197–7202. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jain P, Rai RR, Udawat H, Nijhawan S and
Mathur A: Insulin and heparin in treatment of
hypertriglyceridemia-induced pancreatitis. World J Gastroenterol.
13:2642–2643. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Markota A, Knehtl M, Sinkovic A, Ekart R,
Hojs R and Bevc S: Plasma exchange treatment for acute
hyperlipidemic pancreatitis with falsely low levels of serum
triglycerides- a case report. Transfus Apher Sci. 51:178–180. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Monib SM and El-Barbary HM: Acute
relapsing pancreatitis with pseudocyst formation due to sporadic
hypertriglyceridemic pancreatitis: A case report. Indian J Surg.
75:(Suppl 1). S340–S344. 2013. View Article : Google Scholar
|