Introduction
Lipomas are very common benign lipomatous tumors
that most often grow in the subcutaneous tissue. The majority of
lipomas occur in adults aged >30 years, with an equal gender
incidence. However, ossifying lipomas are rare. They have been
reported at several sites in the body, including the soft tissues
of the head and neck, the oral cavity, and the femur and fibular
regions (1–6). Nitima et al were the first to
report a case of parosteal ossifying lipoma occurring in the fibula
of a 35-year-old female patient (6).
To the best of our knowledge, parosteal ossifying lipomas of the
clavicle have not been reported to date.
Parosteal ossifying lipomas develop over an extended
period of time and present no clinical symptoms, except when they
compress nerves. The clinical symptoms of osteochondromas are
similar to those of parosteal ossifying lipomas, so the two types
of tumors may be easily confused. We herein present our experience
with the diagnosis and management of an ossifying lipoma adjacent
to the periosteum of the clavicle.
Case report
A 40-year-old man was admitted to Beilun People's
Hospital due to a mass on his right clavicle, which had grown
slowly over a period of 20 years. The mass insidiously increased in
size, with no associated pain. The patient did not feel discomfort
when he moved his neck. The patient's general health was good and
there was no other remarkable medical history.
On physical examination, a mass sized ~3×2×2 cm was
palpable beneath the skin of the right shoulder and extending to
the right clavicle. The mass was soft, non-tender and fixed to the
clavicle. No prominent swelling, hyperaemia or ulceration of the
skin were observed. The sensory and motor function of the right
upper limb was normal. Preoperative examination revealed that the
mass was well circumscribed peripherally and not adherent to
adjacent muscles; however, it was fixed to the clavicle.
Radiographic examination revealed that the mass was
located in the middle of clavicle, and its base intensity was
similar to that of the clavicle; thus, the mass was initially
suspected to be an osteochondroma (Fig.
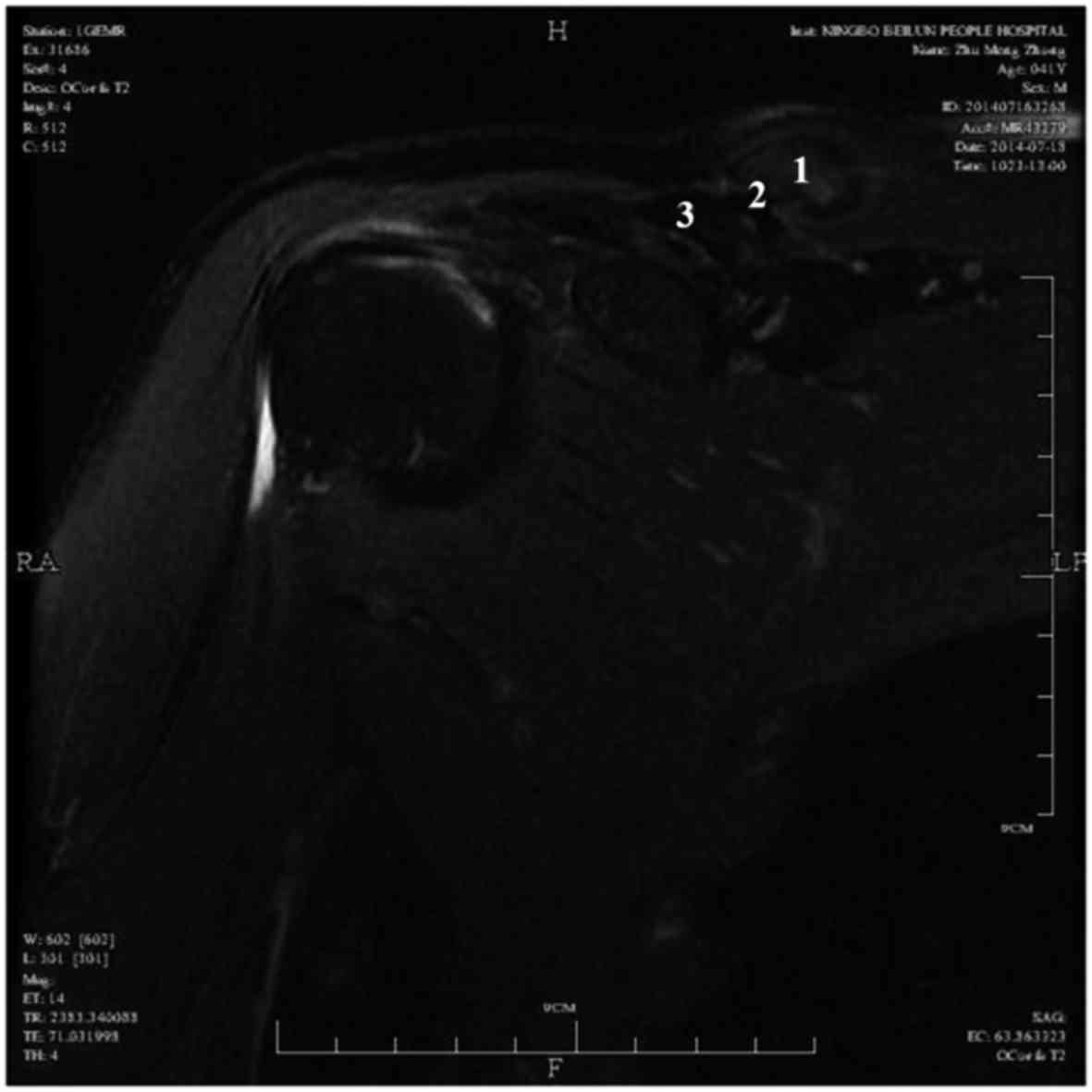
1). On magnetic resonance imaging (MRI), the mass consisted of
3 layers (Fig. 2): The surface was
encased in adipose tissue and the middle layer was osseous tissue;
the base was fixed to the clavicle, but was not associated with
clavicular marrow cavity. On T1- and T2-weighted images, the
surface adipose tissue exhibited a high signal, while the core bone
tissue exhibited a low signal.
Surgical treatment
En bloc resection of the mass together with the
osseous protuberance of the right clavicle was performed. The mass
was well circumscribed and was easily dissected from the adjacent
soft tissue. The base of the tumour adhered strongly to the
clavicle. The mass measured 3×2×2 cm, with a smooth surface. The
cut surface of the specimen was yellowish, with a mostly
homogeneous appearance. The hard bony protuberance was chiselled
from the clavicle; the mass was not continuous with the marrow
cavity of the clavicle.
Histological examination
Microscopically, the mass was mostly composed of
mature adipocytes, whereas mature chondrocytes were identified in
the basal layer adherent to the clavicle (Fig. 3A). This mass consisted of three
layers, namely an ossification center, bone tissue and adipose
tissue. The ossification center resembled bone marrow, consisting
of numerous osteogenic cells. The bone tissue included osteoblasts
and chondrocytes surrounded by cartilage matrix. The adipose tissue
was composed of mature adipose cells and fibrous tissue. None of
the major components exhibited any nuclear pleomorphism or
immaturity (Fig. 3B). Thus the
diagnosis of ossifying parosteal lipoma was confirmed.
Discussion
Lipomas are the most common benign soft tissue
neoplasms, accounting for ~50% of all soft tissue neoplasms.
Parosteal lipomas may be considered as a separate group of rare
benign lipomas affecting the bones, performing either in mandible,
cervical vertebra or fibula (7,8).
Parosteal lipomas are exceedingly rare benign lipomatous neoplasms
located adjacent to the periosteum of bones. Parosteal lipomas have
been reported at several sites in the body, including the soft
tissues of the head and neck, the oral cavity, and the femur and
fibular regions (1–5,9). The
most common site of parosteal lipomas is in the thigh, contiguous
with the femur (6). To the best of
our knowledge, parosteal lipomas in the clavicle have not been
reported to date.
Patients with parosteal lipomas are generally aged
40–60 years and they usually present with a slowly growing,
painless mass fixed to the bone. Neurological deficits have
occasionally been reported, most commonly associated with forearm
lesions adjacent to the radius, resulting in posterior interosseous
nerve palsy (10,11). In the present case, the patient did
not present with nerve palsy, paresthesia, or pain and the serum
tumor marker levels were not elevated. This parosteal lipoma had
been growing slowly over a period of 20 years and the patient
wished to have the mass removed for aesthetic reasons alone.
Parosteal lipoma may occasionally be misdiagnosed as
osteochondroma, when there is association with the underlying bone
(12). In this case, the X-ray
examination raised the suspicion of osteochondroma. On MRI, the
mass was characterized by high signal intensity on T1-weighted
images, with low signal of the bone layer. The mass exhibited low
signal intensity on T2-weighted images (Fig. 2).
Intraoperatively, the mass was found to be wrapped
with a pseudomembrane, had a large base and was fixed to the right
clavicle. The surface of the mass was covered with a cap that was
initially considered to be a cartilaginous cap. From the
radiographic, MRI and macroscopic findings, the mass was highly
suspected to be an osteochondroma; however, the pathological
examination revealed that it was a parosteal ossifying lipoma
(Fig. 3B). The mass did not have a
cartilaginous cap, but consisted of an ossification center, bone
tissue and adipose tissue. The cap covering the mass was composed
of adipose tissue. The absence of a cartilaginous cap is a
distinguishing characteristic between osteochondromas and ossifying
lipomas.
The treatment of parosteal ossifying lipomas of the
clavicle is complete surgical resection. Local recurrence is rare
and malignant changes have not been documented to date. In this
case, the periosteal lipoma was surgically removed by simple
excision and there has been no evidence of recurrence.
To the best of our knowledge, this is the first
reported case of parosteal ossifying lipoma of clavicle. The lesion
was initially mistaken for osteochondroma. However, the
cytohistomorphology of this case and the radiological
characteristics supported the diagnosis of parosteal ossifying
lipoma.
In conclusion, the clinical presentation of
parosteal ossifying lipoma is similar to that of osteochondroma.
The treatment in this case was complete surgical resection and the
patient has experienced no recurrence, malignant transformation or
metastasis.
References
|
1
|
Bognár L, Bálint K and Bárdóczy Z:
Symptomatic osteolipoma of the tuber cinereum. Case report. J
Neurosurg. 96:361–363. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mackenzie IR, Girvin JP and Lee D:
Symptomatic osteolipoma of the tuber cinereum. Clin Neuropathol.
15:60–62. 1996.PubMed/NCBI
|
|
3
|
Moschopulos M, Becheanu G and Stamm B:
Hypothalamic osteolipoma of the tuber cinereum. J Cell Mol Med.
10:240–242. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hashmi AA, Malik B, Edhi MM, Faridi N and
Ashraful M: A large parosteal ossifying lipoma of lower limb
encircling the femur. Int Arch Med. 7:52014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Diom ES, Ndiaye IC, Ndiaye M, Thiam A,
Tall A, Nao EE, Diallo BK, Diouf R and Diop EM: Osteolipoma: An
unusual tumor of the parotid region. Eur Ann Otorhinolaryngol Head
Neck Dis. 128:34–36. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Saksobhavivat N, Jaovisidha S,
Sirikulchayanonta V and Nartthanarung A: Parosteal ossifying lipoma
of the fibula: A case report with contrast-enhanced MR study and a
review of the literature. Singapore Med J. 53:e172–e175.
2012.PubMed/NCBI
|
|
7
|
Ramos A, Castello J, Sartoris DJ, Greenway
GD, Resnick D and Haghighi P: Osseous lipoma: CT appearance.
Radiology. 157:615–619. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Demiralp B, Alderete JF, Kose O, Ozcan A,
Cicek I and Basbozkurt M: Osteolipoma independent of bone tissue: A
case report. Cases J. 2:87112009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sun Z, Sun L, Zhang Z and Ma X: Ossifying
parosteal lipoma of the mandible: A case report and review of the
literature. Dentomaxillofac Radiol. 42:578520732013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Murphey MD, Carroll JF, Flemming DJ, Pope
TL, Gannon FH and Kransdorf MJ: From the archives of the AFIP:
Benign musculoskeletal lipomatous lesions. Radiographics.
24:1433–1466. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kawashima A, Magid D, Fishman EK, Hruban
RH and Ney DR: Parosteal ossifying lipoma: CT and MR findings. J
Comput Assist Tomogr. 17:147–150. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Brones A, Mengshol S and Wilkinson CC:
Ossifying lipoma of the cervical spine. J Neurosurg Pediatr.
5:283–284. 2010. View Article : Google Scholar : PubMed/NCBI
|