Introduction
The inguinal region is notable for the spectrum of
diseases presenting in that anatomic location. Clinical distinction
between these entities based on history and physical examination
remains challenging. Tumors of the spermatic cord are usually
benign (70–80%), with the majority being simple lipomas. Among
malignant tumors of the spermatic cord, sarcomas are the most
common type. Rhabdomyosarcomas are the most aggressive type and the
predominant type in children. The other histological types of
sarcomas, namely liposarcomas, leiomyosarcomas and fibrosarcomas,
are most frequently encountered in the adult population.
Liposarcomas, derived embryologically from mesodermal tissue, are
the most common type of sarcoma and account for 3–7% of all
spermatic cord tumors (1–3). Liposarcomas are most commonly located
in the lower extremities (41%), retroperitoneum (19%) and inguinal
region (12%) (4). Even within the
inguinal region, liposarcomas of the spermatic cord are quite rare,
with case reports constituting the majority of the published
literature on this topic (5).
Sarcoma of the spermatic cord was first reported by
Lesauvage in 1845 (1). Based on the
case reports since then, it appears that the majority of the
patients with liposarcomas of the spermatic cord present in the
fifth or sixth decade of life with a painless, irregular,
slow-growing inguinal or inguinoscrotal mass clearly distinct from
the testis (3,6,7). As
previously mentioned, diagnosing liposarcomas of the spermatic cord
preoperatively may be challenging, as this clinical presentation
may indicate several more common conditions, including inguinal
hernia, lipoma, hydrocele, epididymal cyst, funicular cyst or
testicular tumors (3–5,8,9).
On ultrasound examination, a liposarcoma of the
spermatic cord usually exhibits heterogeneous echogenicity;
however, these ultrasound findings lack specificity. A CT scan is
suggestive of the diagnosis in approximately half of the cases and
helps to determine the involvement of the anterior abdominal wall
and/or retroperitoneum (1,2,4,10).
We herein report a case of liposarcoma of the
spermatic cord and review available data on the pathophysiology,
management and follow-up of patients with this condition.
Case report
A 63-year-old man presented in September, 2006 at
the Hotel Dieu de France University Hospital with a painless,
mobile mass in the right inguinal region. On clinical examination,
the mass was found to descend from the inguinal canal into the
scrotum with the Valsalva maneuver. The patient was diagnosed with
an indirect right inguinal hernia and scheduled for surgical
repair.
Intraoperatively, following dissection of the
spermatic cord, a multi-lobulated, encapsulated, yellow mass was
identified within the cord. The mass appeared to infiltrate
surrounding soft tissue structures, such as muscle and the external
tunica vaginalis. Further dissection and delivery of the right
testis demonstrated an atrophic testis with no evidence of local
invasion. After a thorough on-site evaluation, surgical resection
was delayed to permit better assessment of the disease and to
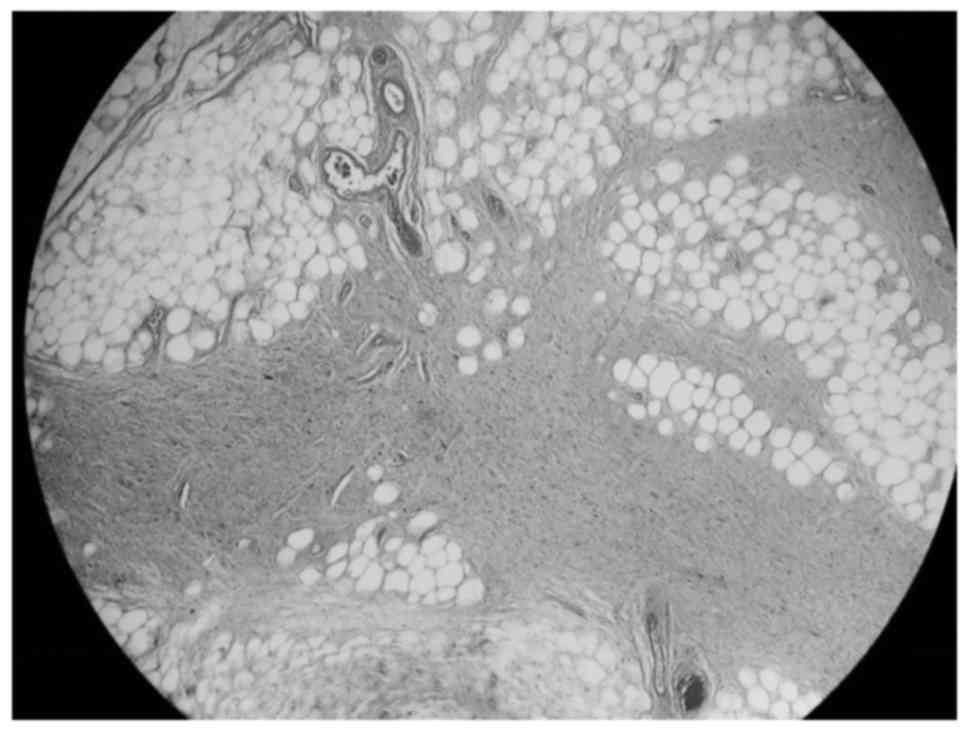
obtain patient consent for possible orchiectomy. An incisional
biopsy of the mass was performed, and pathological analysis
revealed a well-differentiated liposarcoma of the sclerosing type
(Fig. 1).
A computed tomography (CT) scan revealed a 5-cm mass
with heterogeneous enhancement located inside the right inguinal
canal, surrounded by local inflammation. Despite the atrophic
appearance of the ipsilateral testis intraoperatively, on CT scan
it appeared to be enlarged due to the thickening of the overlying
layers (Fig. 2).
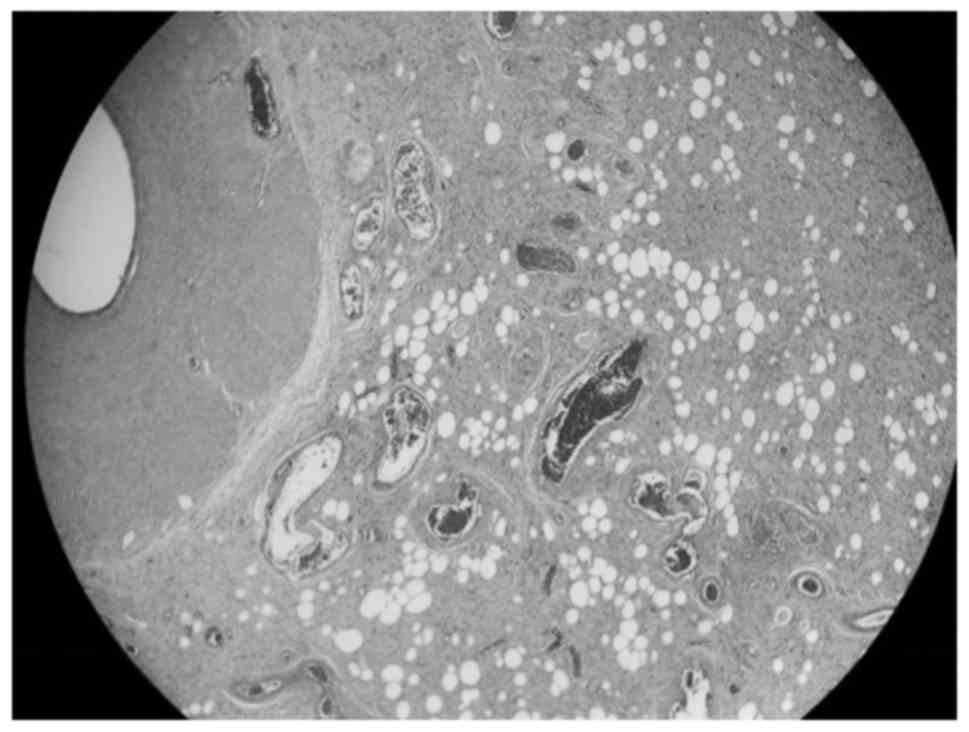
The surgical team decided to proceed with a radical
orchiectomy and an en bloc resection of the mass and associated
cord structures. Final pathology was consistent with a
well-differentiated liposarcoma, sized 7×3 cm, adherent to the
testicle at the level of the tunica albuginea. There was no
invasion of the testicular tissue or the epididymis, but the tumor
extended close to the spermatic cord structures (Fig. 3). All the margins were negative;
thus, no further treatment was recommended.
Screening CT scans were obtained at 6 months and at
1, 3, 5 and 10 years. The CT scan at 6 months revealed no signs of
tumor recurrence, as well as a net decrease in local inflammation.
The patient remained asymptomatic throughout the follow-up period.
The most recent CT scan, performed in October, 2016 (10 years after
the surgery), revealed no signs of tumor recurrence.
The patient provided consent to the publication of
the case details and associated images.
Discussion
Based on surgeon experience and the limited
available literature, the preferred first-line treatment for
spermatic cord liposarcomas is surgical resection. This is
performed through a wide excision of the mass, including
orchiectomy and high ligation of the spermatic cord to achieve a
negative margin. A number of prospective studies on spermatic cord
sarcomas (including liposarcomas) emphasize the importance of
aggressive surgical management, including wide re-resection of
tumor recurrence, in decreasing local recurrence and improving
disease-free survival (6,11). Rates of positive margins as high as
19% have been reported following initial local excision, which
underscores the challenges associated with surgical resection of
these tumors. Intraoperative assessment of tumor resection margins
is limited by the accuracy of frozen biopsy, making complete
surgical resection difficult.
Tumor staging is based on histological examination
and grading, and the presence of metastases. The World Health
Organization classification of soft tissue tumors classifies
liposarcomas into five categories as follows: Myxoid (most common),
well-differentiated (adipocytic, sclerosing and inflammatory
subtypes), dedifferentiated, round-cell and pleomorphic. Low-grade
subtypes are histologically well-differentiated and have no or
minimal tendency to metastasize, although they may be locally
invasive. High-grade subtypes (round-cell and pleomorphic) are
rarer, but they are associated with a higher rate of recurrence and
hematogenous metastasis to the lungs and bone (1,3,8,9). Neither
low- nor high-grade liposarcomas typically spread via lymphatic
routes, which is consistent with the lack of a survival benefit
from superficial inguinal or retroperitoneal lymphadenectomy
(1,2,4,8). Local recurrence rates for sarcomas,
including liposarcomas of the spermatic cord, have been reported to
be as high as 50%. However, these numbers vary between case
reports. In a recent case series of 42 patients, only 7 (17%)
developed local recurrence (12). In
that study, recurrence developed on average at 40.9 months after
resection; two of the patients had systemic metastases and
succumbed to the disease. This study reported no significant
association between recurrence and margin status, tumor size, or
tumor grade (P>0.05), although it was likely underpowered to
detect these differences.
The use of adjuvant treatment
(chemotherapy/radiotherapy) is controversial, due to the paucity of
data in the literature. Some authors only recommend adjuvant
radiotherapy in cases with multiple local recurrences, positive
margins, and/or poor prognostic factors, such as high-grade tumors.
A study of patients treated for spermatic cord tumors showed
improved locoregional control and disease-free survival in patients
receiving adjuvant radiation; however, the 5-year overall survival
rates did not improve significantly. A more recent study confirmed
that adjuvant radiation therapy improved local control in patients
at high risk for local failure, but did not assess its effect on
long-term survival (13). Based on
this limited literature, there is no definitive role for
chemotherapy in the management of localized liposarcoma of the
spermatic cord (1,2,5,8,9,14,15).
As the surgical margins were negative in our case
and the efficiency of adjunctive therapies in such cases is
uncertain, it was decided that radiotherapy and chemotherapy were
not indicated for our patient. A similar strategy was undertaken by
Malizia et al, who reported two cases of well-differentiated
liposaromas treated by wide excision, high ligation and ipsilateral
radical orchiectomy, without any adjuvant therapy. No recurrence or
distant metastases were observed after 8 years in the first case or
after 20 months in the second case (2). Ikinger et al also reported one
case of a combination mixoid liposarcoma and angiolipoma of the
spermatic cord, which was treated surgically and had no
demonstrable recurrences or metastases during the 30 months of
follow-up (7).
In summary, liposarcomas of the spermatic cord are
challenging to diagnose clinically. Suspicion of the possible
diagnosis when evaluating an inguinal hernia should prompt imaging
studies. As there is no gold standard treatment, the management of
these tumors relies on the guidance of case reports in the
literature. These reports suggest that a wide and complete
resection with clear microscopic margins is key to the management
of spermatic cord liposarcomas. If the margins are positive,
re-resection should be performed (1,5,6,10,13,16).
Adjuvant radiation therapy should be considered in cases at high
risk for local recurrence. However, a relatively conservative
approach may reduce morbidity in patients with localized disease.
The indications for retroperitoneal lymph node dissection remain
very limited. For patient follow-up, the consensus is to perform
close and regular follow-up with imaging at 3, 6, 12 and 24 months;
the benefit of longer follow-up has not been determined. As the
literature on this subject grows, guidelines for treatment should
be developed.
References
|
1
|
Chintamani Tandon M, Khandelwal R, Jain S,
Narayan N, Kumar Y and Saxena S: Liposarcoma of the spermatic cord:
A diagnostic dilemma. JRSM Short Rep. 1:492010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Malizia MBE, Bertaccini A, Palmieri F,
Vitullo G and Martorana G: Liposarcoma of the spermatic-cord:
Description of two clinical cases and review of the literature.
Arch Ital Urol Androl. 77:115–117. 2005.PubMed/NCBI
|
|
3
|
Papageorgiou MS, Dadakas G and Donev K:
Liposarcoma of the spermatic cord: A case report. Case Rep Med.
2011:1975842011.PubMed/NCBI
|
|
4
|
Vázquez-Lavista GL, Pérez-Pruna C,
Flores-Balcázar HC, Guzmán-Valdivia G, Romero-Arredondo E and
Ortiz-López BJ: Spermatic cord liposarcoma: A diagnostic challenge.
Hernia. 10:195–197. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bestman TJ, Populaire J, Lauwers K and
Molderez C: Liposarcoma of the spermatic cord: Report of 2 cases.
Acta Chir Belg. 107:58–59. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ballo MT, Zagars G, Pisters PW, Feig BW,
Patel SR and von Eschenbach AC: Spermatic cord sarcoma: Outcome,
patterns of failure and management. J Urol. 166:1306–1310. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ilkinger U, Westrich M, Pietz B,
Mechtersheimer G and Schmidt C: Combined myxoid liposarcoma and
angiolipoma of the spermatic cord. Urology. 49:635–637. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bouropoulos C, Skopelitou A, Vaggos G and
Papamichael C: Liposarcoma of the spermatic cord. Int Urol Nephrol.
33:397–398. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Domşa I, Olinici CD and Crişan D:
Spermatic cord mixed liposarcoma. Case report and review of the
literature. Rom J Morphol Embryol. 49:105–109. 2008.PubMed/NCBI
|
|
10
|
Hsu YF, Chou YY and Cheng YH: Spermatic
cord myxoid liposarcoma presenting as an incarcerated inguinal
hernia: Report of a case and review of literatures. Hernia.
16:719–722. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fagundes MAZA, Althausen AF, Coen JJ and
Shipley WU: The management of spermatic cord sarcoma. Cancer.
77:1873–1876. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kryvenko ON, Rosenberg AE, Jorda M and
Epstein JI: Dedifferentiated liposarcoma of the spermatic cord: A
series of 42 cases. Am J Surg Pathol. 39:1219–1225. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Coleman J, Brennan M, Alektiar K and Russo
P: Adult spermatic cord sarcomas: Management and results. Ann Surg
Oncol. 10:669–675. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Johnson DE, Harris J and Ayala AG:
Liposarcoma of the spermatic cord. Urology. 11:190–192. 1978.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhao H, Zhou L, Chen X and Liu Y:
Liposarcoma of the spermatic cord: A case report. Urologe A.
50:600–602. 2011.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ugidos L, Suárez A, Cubillo A and Durán I:
Mixed paratesticular liposarcoma with osteosarcoma elements. Clin
Transl Oncol. 12:148–149. 2010. View Article : Google Scholar : PubMed/NCBI
|