Introduction
Carcinogenesis is a multistep process including
genetic alterations that develop over time, and it is associated
with metabolic alterations that may promote neoplastic progression
(1).
Metabolic processes that use folates interfere with
the synthesis, repair and methylation of DNA, as they are involved
in the synthesis of purine and of pyrimidine bases and serve as
methyl donors in the methionine cycle (2).
Folate deficiency encourages the assimilation of
uracil in the DNA, which causes a genomic instability characterized
by the formation of single and double breaks in the DNA filaments,
chromosomal breakages and the formation of micronuclei (2).
It is obvious, therefore, that folate deficiency may
be directly implicated in promoting carcinogenesis (3,4). The
chronological succession of certain types of metaplasia of the
laryngeal epithelium with laryngeal cancer may identify a group of
lesions that are defined as ‘precancerous’ (5).
Several events that take place during the
transformation of precancerous lesions to cancer may be controlled
and even reversed by removing the possible trigger factors (e.g.,
discontinuing smoking and following a balanced diet) and by using
carcinogenesis inhibitors (chemoprevention) (6). Chemoprevention is the use of chemical
or natural substances to reverse, suppress or prevent conversion of
precancerous to invasive lesions (7). At this time, chemoprevention may be
defined as the use of agents to prevent the appearance of
precancerous lesions, or delay or reverse progression from
precancerous to cancerous lesions. The multistep theory of
carcinogenesis (accumulation of genotypic or phenotypic
alterations) has further highlighted the importance of
chemoprevention in arresting these processes, as it may be
sufficient to prevent the development of cancer (8,9).
Folate supplementation, alone or in combination with
other chemopreventive agents, may reduce the risk of progression in
a mucosa that is already genetically altered, particularly in
patients with folate deficiency. This is important, as laryngeal
leukoplakia tends to recur, often with a histological progression
or even transformation (10).
The success of several clinical trials in cancer
prevention in high-risk populations suggests that chemoprevention
is a rational and appealing strategy.
Only few studies have been conducted on laryngeal
precancerous lesions, due to limitations associated with
difficulties in access and monitoring. Instead, premalignant
lesions of the oral cavity represent an ideal model for study, as
ready access allows easy monitoring and serial biopsies, resulting
in a higher likelihood of early intervention and faster data
analysis.
The aim of the present study was to determine the
role of folic acid in the treatment of mild and moderate laryngeal
dysplasia recurring after surgery, and compare the data obtained by
laryngoscopy, measurement of serum folate levels and functional
vocal assessment with the grade, instability, roughness,
breathiness, asthenia and strain (GIRBAS) scale and the voice
handicap index (VHI) questionnaire in patients who received folic
acid with a homogeneous group of patients with dysplastic lesions
who did not receive any therapy.
Patients and methods
Patients
The present study included 24 patients with
persistent glottic leukoplakia, who underwent surgery at the ENT
Division of the Department of Neuroscience, Reproductive and
Odontostomatologic Science (University ‘Federico II’, Naples,
Italy), between 2010 and 2015. The diagnosis was confirmed by
direct microlaryngoscopy with a biopsy for histological assessment.
Leukoplakia was histolocically classified as normal mucosa,
hyperkeratosis without dysplasia, mild dysplasia [laryngeal
intraepithelial neoplasia (LIN) I], moderate dysplasia (LIN II),
severe dysplasia (LIN III), or invasive carcinoma. All the patients
came from a homogeneous geographic area and included 20 men and 4
women. The mean patient age was 65 years.
The patients had been previously treated by
excisional biopsy, namely type I cordotomy/cordectomy, according to
the classification of the Working Committee, European
Laryngological Society (11,12), using ‘cold’ microinstruments and/or
CO2 Acublade 400 Lumenis laser, Sharplan 40C and Zeiss
surgical microscope during microlaryngoscopy.
A total of 18 patients underwent type I cordectomy
and 6 patients underwent type II cordectomy. The histological
findings included mild dysplasia in in 16 cases (66.6%) and
moderate dysplasia in the remaining 8 cases (33.3%).
Upon joining the study, the patients were adequately
informed regarding the risks of the disease and its possible
progression to malignancy, as well as the high tendency of
recurrence, and they all signed a consent form for the therapy. The
Institutional Review Board of the University ‘Federico II’ approved
the study protocol. Patients who were smokers or habitual alcohol
consumers were excluded from the study. All patients denied using
narcotics, receiving gastroesophageal reflux therapy, having any
dietary deficiencies or being exposed to toxic substances by
inhalation. All patients underwent the following
examinations/tests: i) Ear, nose and throat examination upon
enlisting, at 3 months, and at 6 months from agreeing to
participate in the study. ii) Fibrolaryngoscopy with optical fibers
of the airways-digestive system with the aid of video recording
upon joining, at 3 months and at 6 months. The response was then
classified as stable disease, when the dimensions and the
appearance of the lesion remained virtually unchanged compared with
the start of the study, as partial response when a reduction in the
size of the lesions was observed, or as complete response when
there was no evidence of residual leukoplakia. Should any lesion
exhibit malignant transformation during treatment, surgical
resection would have been performed; however, there were no such
cases in the present study. If the lesion persisted after 6 months,
the patients underwent endoscopic resection followed by a further
histological assessment of the residual leukoplakia. iii) Serum
folate levels upon enlisting (baseline), at 3 months and at 6
months. iv) Functional assessment of vocal emission using the
GIRBAS scale and VHI questionnaire upon enrolling, at 3 months and
at 6 months.
During follow-up, all the patients exhibited a
tendency to relapse, with the appearance of low-degree
hyperkeratosis.
The patients were randomly divided into two
homogeneous groups by sex and age (groups A and B), each group
including 12 patients (10 male and 2 female). In group A, 8
patients exhibited mild dysplasia and 4 had moderate dysplasia; 9
of the patients underwent type I and 3 underwent type II cordectomy
with CO2 laser. The lesion was bilateral in 10 patients
(83%). In group B, 7 patients exhibited mild dysplasia and 5 had
moderate dysplasia; 9 of the patients underwent type I and 3
underwent type II cordectomy with CO2 laser. The lesion
was bilateral in 9 patients (75%).
All 12 patients in group A were treated with folic
acid (Folina; Schwarz Pharma, Monheim am Rhein, Germany)
administered orally (15 mg every 8 h) for 6 months. The 12 patients
in group B received no chemoprevention treatment, but served as the
control group. Prior to treatment initiation, assessment of serum
folate levels was performed.
Statistical analysis
Statistical analysis was performed using the MedCalc
statistical software, version 9.3.7.0 (MedCalc Software, Ostend,
Belgium). Groups A and B were compared using the t-test for
quantitative variables and the Wilcoxon/Mann-Whitney U test for
non-parametric variables. A P-value of <0.005 was considered to
indicate statistically significant differences.
Results
Response to treatment
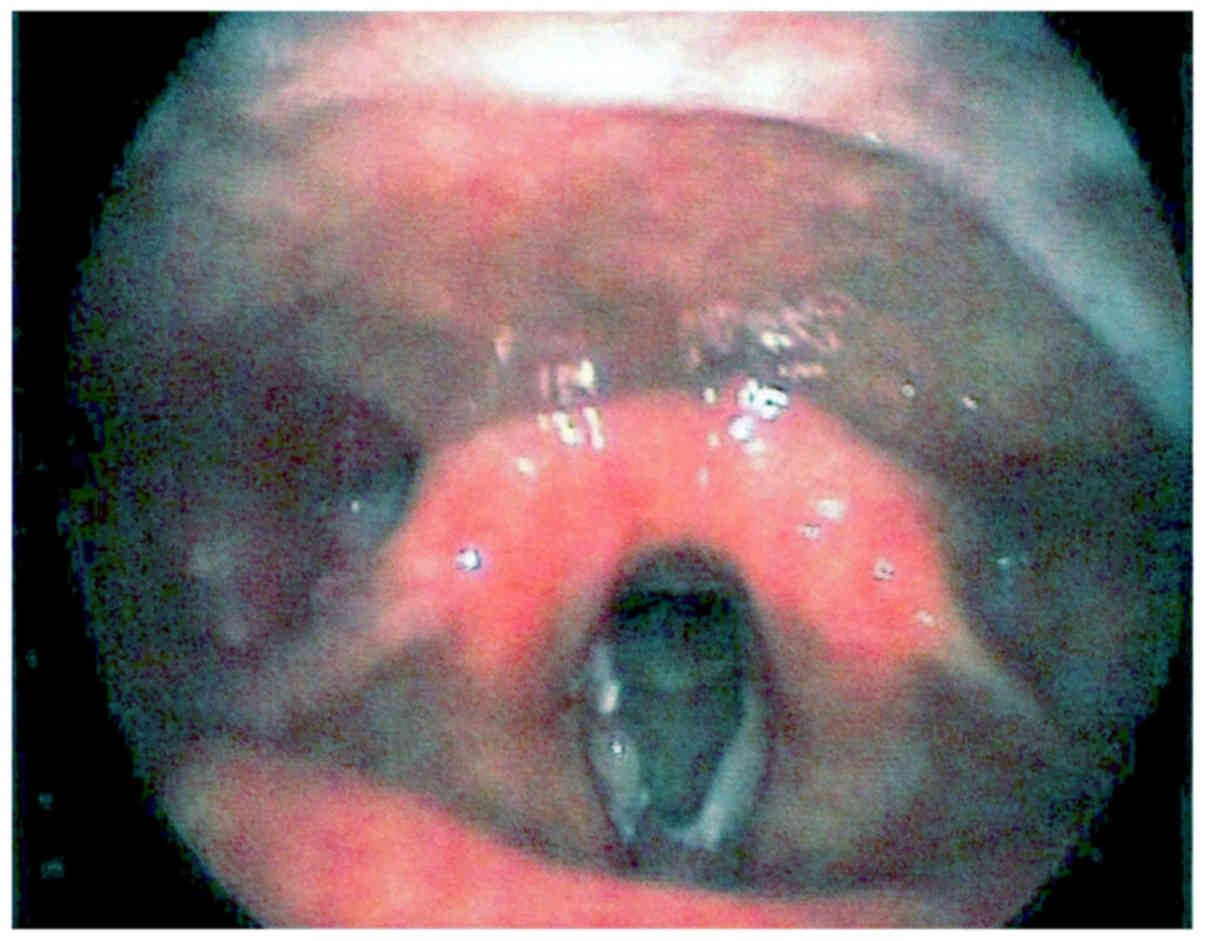
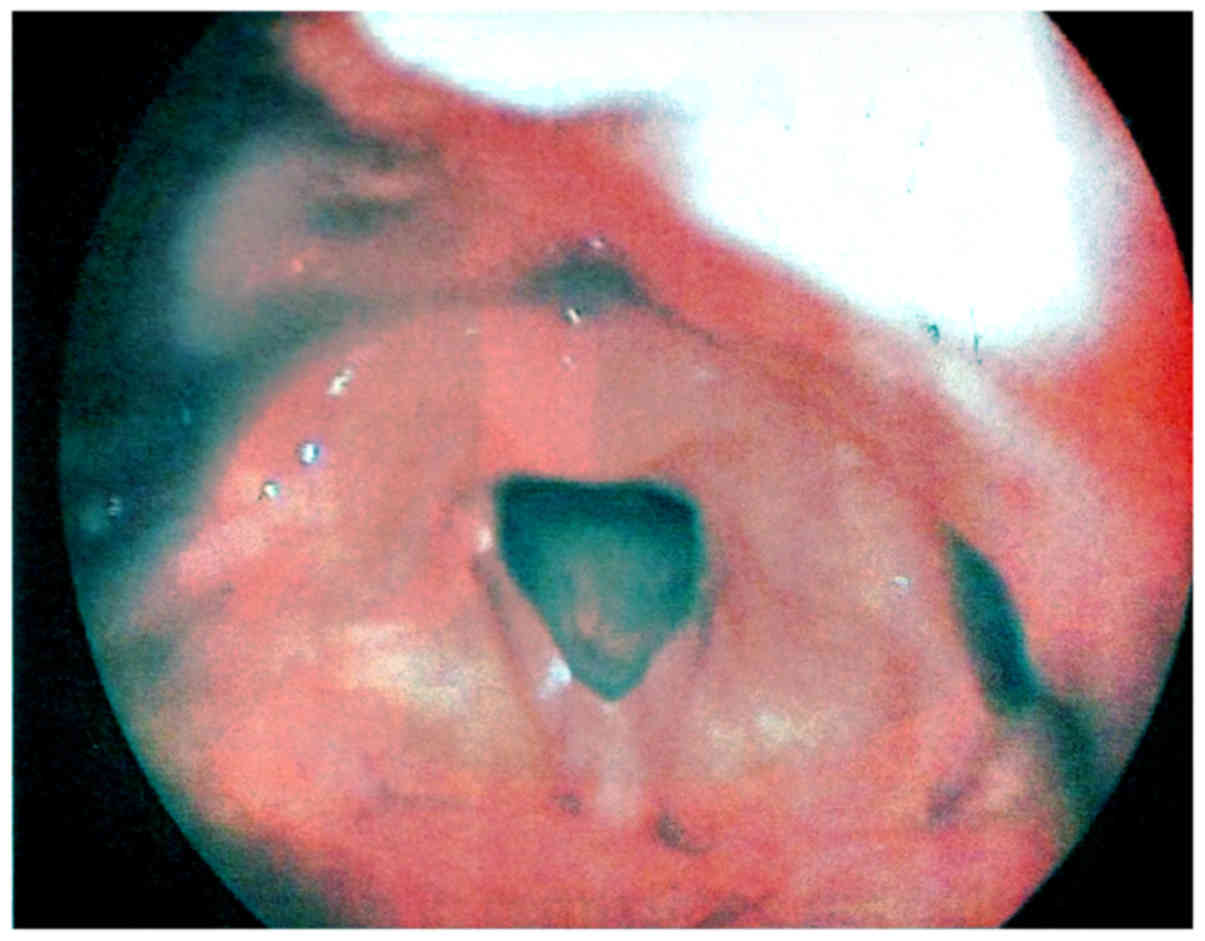
In group A, upon laryngoscopic examination there was
a clinical improvement of up to 80% at 6 months. Specifically, 7
patients (58%) had a complete response, with clinically evident
regression of the leukoplakia, 3 (25%) displayed a partial decrease
in the lesions with reduced volume of the area involved, whereas 2
patients exhibited no change. As regards patients in control group
B, 8 (67%) exhibited no change, in 1 case there was spontaneous
regression, and in 3 (25%) there was histological progression with
suspected malignant transformation that led to repeat surgery
(Figs. 1 and 2). As regards smoking and drinking habits,
none of the patients reported any change.
Restoration of serum folate
levels
The serum folate levels at baseline (t0) were low in
all patients from both groups compared with normal values (range,
2.7–34 ng/ml). However, after 6 months of treatment, the difference
between the two groups was statistically significant (P<0.0001;
Table I).
 | Table I.Comparison of folate serum levels
between patients in groups A and B. |
Table I.
Comparison of folate serum levels
between patients in groups A and B.
|
| Folate serum levels,
ng/ml |
|
|---|
|
|
|
|
|---|
| Time point,
months | Group A | Group B | P-value |
|---|
| 0 | 4.5±1.8 |
4.6±1.7 | 0.5 |
| 3 | 6.5±2.0 | 4.75±2.1 |
0.0001 |
| 6 | 6.9±1.9 |
4.9±1.8 | <0.0001 |
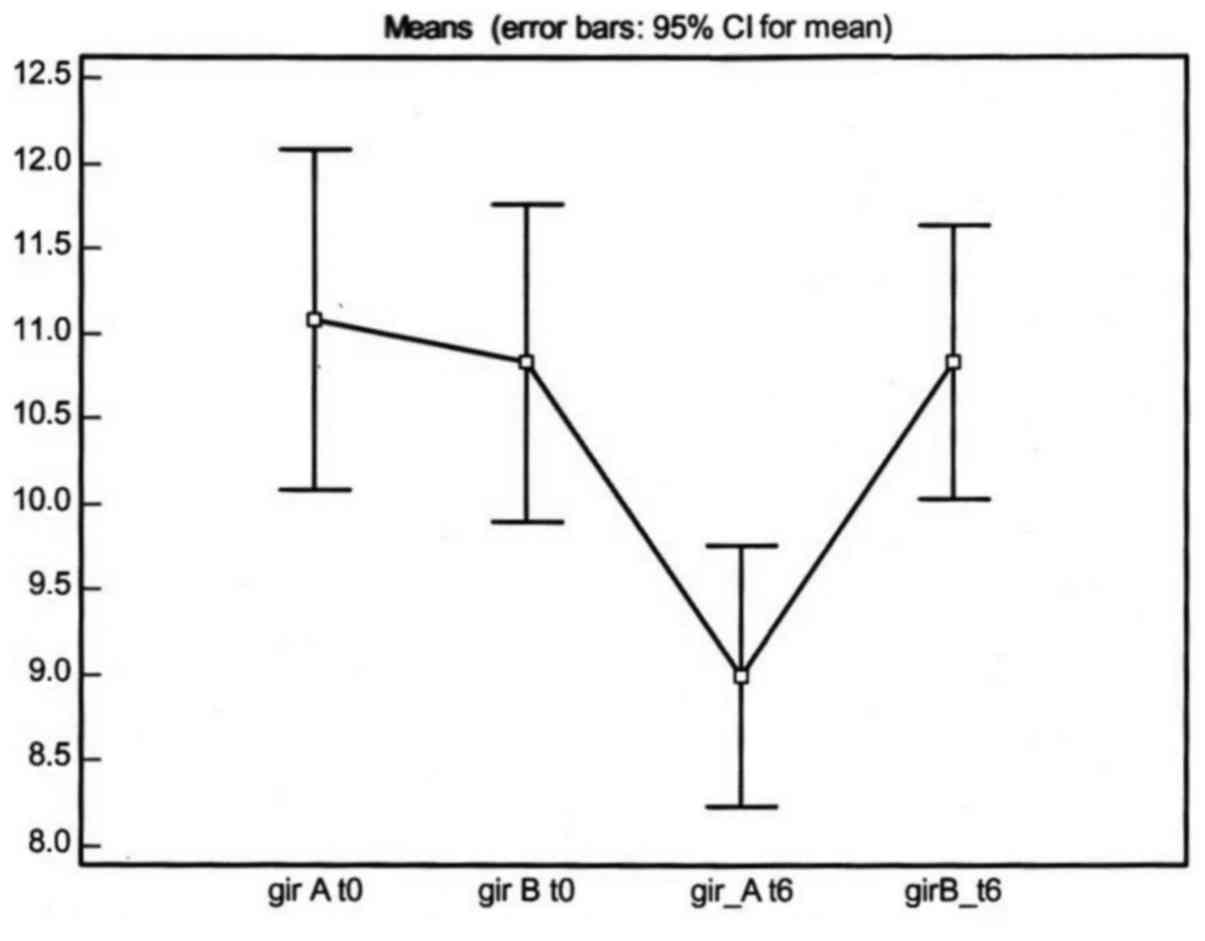
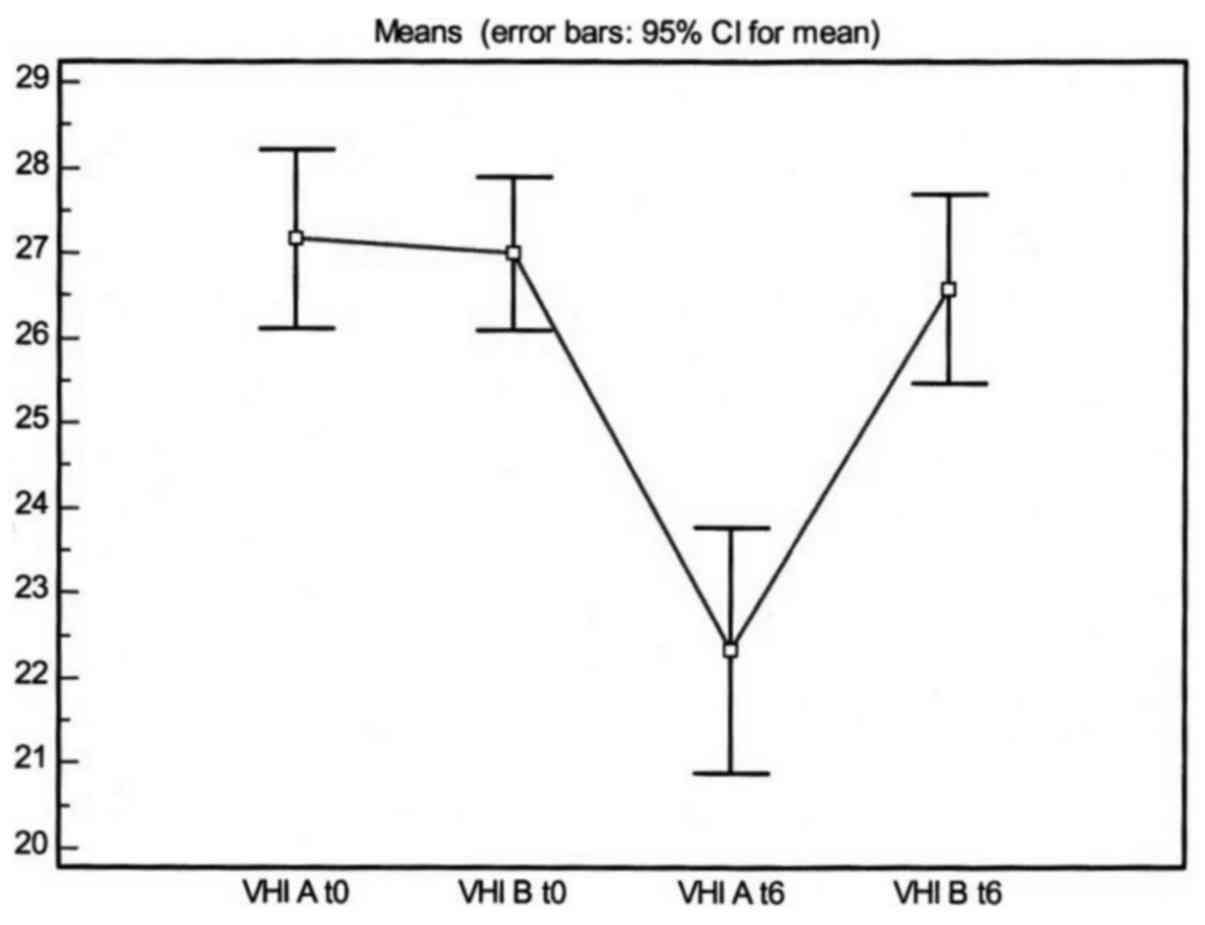
Functional improvement
To assess treatment efficacy, the GIRBAS scale and
VHI questionnaire were used. Vocal discomfort values tended to
return to normal in group A, while they remained virtually
unchanged in group B, with statistically significant differences as
determined with the Wilcoxon/Mann-Whitney U test (P=0.004 and
P=0.001 respectively; Figs. 3 and
4).
Discussion
A standard treatment for leukoplakia and other
dysplastic lesions has not been established and the proposed
approaches range from observation to endoscopic surgery (12–14).
However, none of these options currently appears to effectively
prevent recurrence or malignant transformation (10). Thus, the larynx is a good model for
the development of chemoprevention therapy. Cancer chemoprevention
is the use of natural, synthetic or biological chemical agents to
reverse, suppress or prevent carcinogenesis progression. The
success of several clinical trials in cancer prevention in
high-risk populations suggests that chemoprevention is a rational
strategy. Chemoprevention may be categorized as either primary or
secondary. Primary chemoprevention is directed at patients with
premalignant lesions, whereas secondary chemoprevention is targeted
at cancer patients who, in order to prevent disease recurrence or
to prevent metachronous primary diseases, have undergone
potentially curative therapy.
Folic acid plays an essential role in the stability
and in the methylation and repair of chromatin. Alterations in the
folate cycle were observed in patients with leukoplakia and tumors
of the larynx. A decrease in the serum folate levels have been
reported in subjects with dysplasia (10).
The administration of folates is associated with
decreased risk of tumor of the oral cavity (4).
Various studies are evaluating the effects of folic
acid on the progression of laryngeal leukoplakia; however, it has
already been demonstrated that there is a folic acid deficiency in
laryngeal neoplasia.
The majority of spontaneous clinical regressions of
glottic leukoplakia occur in the first month after diagnosis
(10).
In our chemoprevention protocol, the patients who
suffered from recurring leukoplakia of the larynx had low serum
folate levels. Folate is characterized by a low grade of toxicity
and our results are encouraging, as a complete response rate of 58%
was obtained in Group A patients, who were treated with folic acid
and the low serum folate levels were partially corrected after 3
months and further increased after 6 months of therapy. The
laryngoscopic appearance improved by 80% in the treated patients,
as did vocal discomfort, which tended to resolve.
The management of head and neck cancer and laryngeal
leukoplakia has become multidisciplinary. The inclusion of
effective chemotherapeutic agents in the initial curative therapy
of head and neck cancer has the potential to prolong survival and
preserve organ function. Through well-designed and well-executed
clinical trials, coupled with basic research on the biology of
upper aerodigestive tract tumors, further advances in the
management and prevention of these cancers may be achieved. Folate
deficiency may be considered to be a factor predisposing to
precancerous lesions. Dietary supplementation may prevent and
inhibit the events occurring during the multistep process of
carcinogenesis or the reversal of a premalignant condition
(15).
References
|
1
|
Almadori G, Bussu F, Galli J, Cadoni G,
Zappacosta B, Persichilli S, Minucci A and Giardina B: Serum folate
and homocysteine levels in head and neck squamous cell carcinoma.
Cancer. 94:1006–1011. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Blount BC and Ames BN: DNA damage in
folate deficiency. Bailleres Clin Haematol. 8:461–478. 1995.
View Article : Google Scholar
|
|
3
|
Eto I and Krumdieck CL: Role of vitamin
B12 and folate deficiencies in carcinogenesis. Adv Exp Med Biol.
206:313–330. 1986.PubMed/NCBI
|
|
4
|
Weinstein SJ, Gridley G, Harty LC, Diehl
SR, Brown LM, Winn DM, Bravo-Otero E and Hayes RB: Folate intake,
serum homocysteine and methylenetetrahydrofolate reductase (MTHFR)
C677T genotype are not associated with oral cancer risk in Puerto
Rico. J Nutr. 132:762–767. 2002.PubMed/NCBI
|
|
5
|
Dobrossy L: Epidemiology of head and neck
cancer: Magnitude of the problem. Cancer and Metastis Rew. 24:9–17.
2005. View Article : Google Scholar
|
|
6
|
Brugere J, Guenel P, Leclere A and
Rodriguez J: Differential effects of tobacco and alcohol in cancer
of the larynx, pharynx, and mouth. Cancer. 57:391–395. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hail N Jr, Cortes M, Drake EN and
Spallholz JE: Cancer chemoprevention: A radical perspective. Free
Radic Biol Med. 45:97–110. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Xiangwei, Wu Sherri, Patterson Ernest and
Hawk MDMPH: Chemoprevention-history and general principles. Best
Pract Res Clin Gastroenterol. 25:445–459. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rhee JC, Khuri FR and Shin DM: Advances in
chemioprevention of head and neck cancer. Oncologist. 9:302–311.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Almadori G, Bussu F, Galli J, Cadoni G,
Zappacosta B, Persichilli S, Minucci A, Giardina B and Maurizi M:
Serum levels of folate, homocysteine and vitamin B12 in head and
neck squamous cell carcinoma and in laryngeal leukoplakia. Cancer.
103:284–292. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Remacle M, Eckel HE, Antonelli A, Brasnu
D, Chevalier D, Friedrich G, Olofsson J, Rudert HH, Thumfart W, de
Vincentiis M and Wustrow TP: Endoscopic cordectomy. A proposal for
a classification by the Working Committee, European Laryngological
Society. Eur Arch Otorhinolaryngol. 257:227–231. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Remacle M, Van Haverbeke C, Eckel H,
Bradley P, Chevalier D, Djukic V, de Vicentiis M, Friedrich G,
Olofsson J, Peretti G, et al: Proposal for revision of the European
Laryngological Society classification of endoscopic cordectomies.
Eur Arch Otorhinolaryngol. 264:499–504. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mesolella M, Iorio B, Misso G, Luce A,
Cimmino M, Iengo M, Landi M, Sperlongano P, Caraglia M and
Ricciardiello F: Role of perineural invasion as a prognostic factor
in laryngeal cancer. Oncol Lett. 11:2595–2598. 2016.PubMed/NCBI
|
|
14
|
Motta S, Cesari U, Mesolella M and Motta
G: Functional vocal result after CO2 laser endoscopic
surgery for glottic tumors. J Laryngol Otol. 122:948–951. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mesolella M, Iorio B, Landi M, Cimmino M,
Ilardi G, Iengo M and Mascolo M: Overexpression of chromatin
assembly factor-1/p-60 predicts biological behaviour of laryngeal
carcinomas. Acta Otorhinolaryngol Ital. 37:17–24. 2017.PubMed/NCBI
|