Introduction
Patients with lung cancer may develop other
malignancies (1,2), as may those with colon cancer (3). Epidemiologically, it has been suggested
that cigarette smoking is closely associated with an increased risk
of cancer in various organs, including the lung and the colon
(4,5). Lung cancer is primarily known to be
associated with upper aerodigestive tract cancer, but its
association with gastrointestinal cancer should not be overlooked.
In fact, lung cancer appears to be one of the most common second
primary cancers in patients with colon cancer (4). However, there are few reports of the
treatment and outcome of patients with synchronous lung and colon
cancers (6–8). Additionally, the treatments for these
cancer patients and their outcomes are scarcely reported (6–8). To
evaluate the clinical information, we herein review our experience
with lung cancer patients who developed synchronous colon
cancer.
Patients and methods
Patient classification and
staging
The medical records and pathology reports of all
lung cancer patients at the Division of Respiratory Medicine in our
four tertiary hospitals between April 2009 and July 2016 were
reviewed. The collected data included sex, age at diagnosis of
colon and lung cancer, smoking history, comorbid diseases,
histology and clinical stage of lung cancer, type of treatment and
survival from the date of diagnosis of lung cancer. The symptomatic
group of patients were defined as those with symptoms of either or
both lung and colon cancers. In the present study, synchronous
cancers were defined as those diagnosed within 1 month.
The asymptomatic group of patients were defined as
those detected incidentally by mass screening during follow-up
studies for diseases other than these two cancers, and during lung
or colon cancer workup. The diagnoses of colon and lung cancer were
confirmed pathologically in all the patients and the
histopathological cancer types were confirmed by the World Health
Organization classification. Staging was performed according to the
7th edition of the International Union for Cancer Control TNM
classification of malignant tumors (http://www.uicc.org/sites/main/files/private/TNM_Classification_of_Malignant_Tumours_Website_15%20MAy2011.pdf),
using chest computed tomography (CT), brain magnetic resonance
imaging, bone scan, endoscopy and ultrasonography. In a proportion
of the cases, fluorodeoxyglucose (FDG)-positron emission tomography
(PET) was used.
Statistical analysis
The statistical significance of the differences
between the symptomatic and asymptomatic patient groups were
determined using the Mann-Whitney and Chi-squared test. Survival
curves were assessed with the Kaplan-Meier method and the log-rank
test. Survival was defined as the time from the initiation of the
first therapy or supportive care until death or the last follow-up
and was calculated in months. The effects of clinicopathological
factors on survival were analyzed with the Cox proportional hazards
model. Statistical analyses were performed using SPSS 10.1 for
Windows (SPSS Inc., Chicago, IL, USA) and P<0.05 was considered
to indicate statistically significant differences. Access to the
patients' medical records was approved by the Ethics Committee of
Mito Medical Center at the University of Tsukuba Hospital
(NO16-01).
Results
Patient characteristics
During the study period, from April 2009 up to July
2016, 17 (0.54%) of 3,102 patients with primary lung cancer were
diagnosed with synchronous colon cancer. The clinicopathological
characteristics of the 17 patients with synchronous lung and colon
cancers are summarized in Table I.
Of the 17 patients, 13 were male. The median age at diagnosis was
72 years (range, 60–86 years). Of the 17 patients, 13 (76.5%) were
smokers and 11 were >30-pack-year smokers. Only 2 (11.8%) of the
patients were overweight [body mass index (BMI) ≥25.0
kg/m2] at the time of diagnosis of the two cancers. A
total of 13 patients had non-small-cell lung cancer (NSCLS), and 15
(88.2%) had sigmoid colon or rectal cancer.
 | Table I.Characteristics of 17 patients with
synchronous lung and colon cancers. |
Table I.
Characteristics of 17 patients with
synchronous lung and colon cancers.
| Characteristics | No. (%) |
|---|
| Age (years) |
|
| Median,
range | 72, 60–86 |
| Sex |
|
| Male | 13 (76.5) |
|
Female | 4
(23.5) |
| Smoking habit |
|
| Former-
or current smoker | 13 (76.5) |
| Never
smoker | 4
(23.5) |
| Body mass index
(kg/m2) |
|
| ≥20 | 14 (82.4) |
| ≥25 | 2
(11.8) |
| Lung cancer |
|
|
Non-smallcell lung cancer | 13 (76.5) |
| Smallcell
lung cancer | 4
(23.5) |
| Colorectal
cancer |
|
| Sigmoid
colon or rectal cancer | 15 (88.2) |
|
Others | 2
(11.8) |
| Disease
detection |
|
|
Asymptomatica | 276 (86.5) |
|
Symptomatic | 43 (13.5) |
Treatment and outcome
In the 17 patients with synchronous lung and colon
cancers, 9 patients were asymptomatic and the remaining 8 were
symptomatic. The clinical stage and treatment for these two cancers
in the two patient groups are summarized in Table II. Apart from the treatment for
colon cancer, there were no statistically significant differences
between the two groups. The numbers of patients who received
therapy for colon cancer first, those who received therapy for lung
cancer first, and those who received supportive care alone, are
listed in Table III. There was no
statistically significant difference between the two groups of
patients.
| Table II.Differences between SCLC patients with
and without ILD. |
Table II.
Differences between SCLC patients with
and without ILD.
| Variables | Patients with
ILD | Patients without
ILD | P-value |
|---|
| Age |
|
| 0.489 |
| Median,
range (years) | 68, 5880 | 70, 27–86 |
|
| Sex |
|
| 0.999 |
| Male | 14 | 280 |
|
|
Female | 1 | 37 |
|
| Performance
status |
|
| 0.999 |
| 0–1 | 13 | 265 |
|
| 2–4 | 2 | 52 |
|
| Clinical stage |
|
| 0.999 |
|
Early | 7 | 152 |
|
|
Advanced | 8 | 165 |
|
| Treatment |
|
| 0.079 |
|
Chemotherapy | 13 | 263 |
|
| Surgery +
chemotherapy | 2 | 24 |
|
| Chest
irradiation | 0 | 25 |
|
|
Supportive care | 0 | 5 |
|
| Table III.Sequence of treatments among patients
with synchronous lung and colon cancer. |
Table III.
Sequence of treatments among patients
with synchronous lung and colon cancer.
|
| Number of
patients |
|
|---|
|
|
|
|
|---|
| Treatment
sequence | Asymptomatic
group | Symptomatic
group | P-value |
|---|
| Treatment for colon
cancer first | 5 | 2 | 0.117 |
| Treatment for lung
cancer first | 4 | 3 |
|
| Supportive care
alone | 0 | 3 |
|
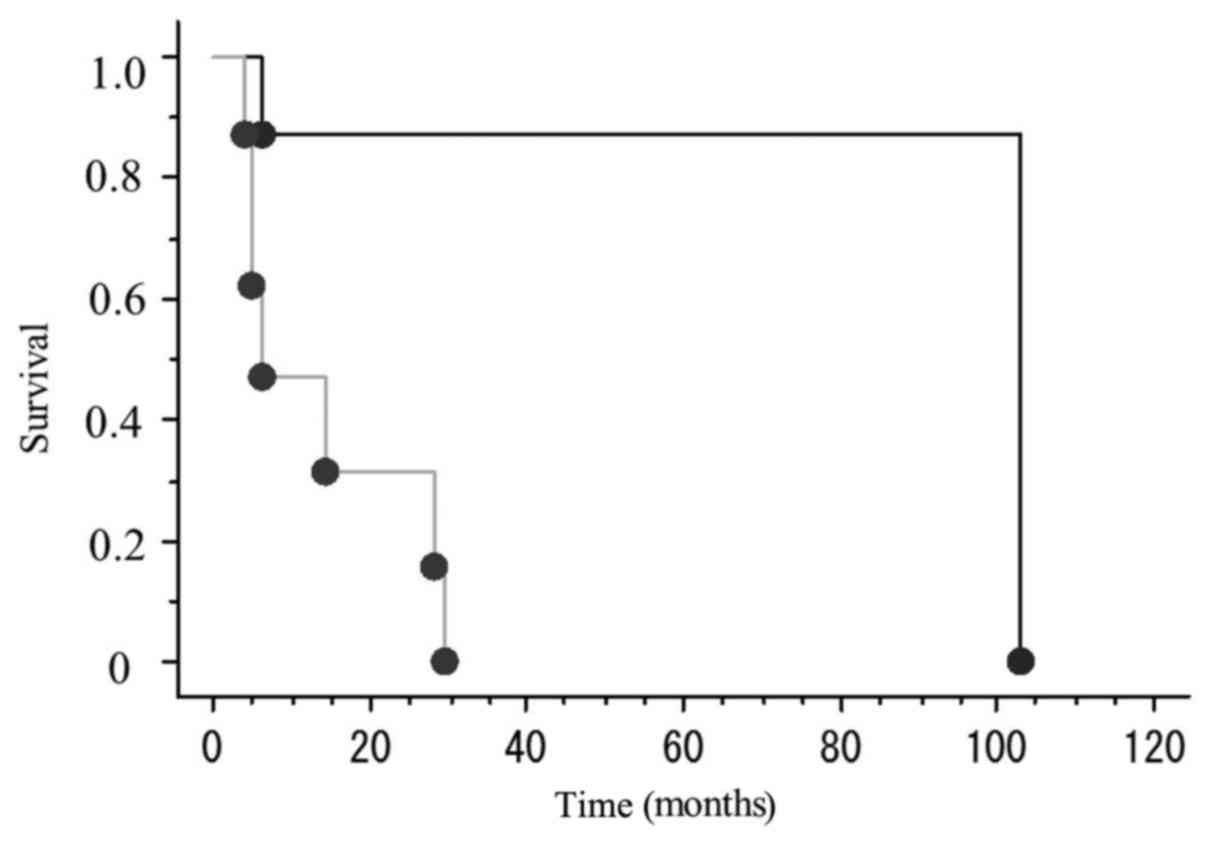
During the study period, 9 patients succumbed to
their disease. The cause of death in all 9 patients was directly
associated with lung cancer. The median survival in the
asymptomatic group of patients was 80 months and that in the
symptomatic group of patients 23.2 months. The difference in
survival between the two groups of patients was statistically
significant (P=0.007; Fig. 1).
Discussion
Lung cancer and colon cancer are two of the most
common malignancies and among the leading causes of cancer-related
mortality (9). Particularly in
developed countries, these cancers are a major public health burden
(9). There is a possibility that
this combination may be more common than initially considered, if
endoscopically treatable early colon cancer is taken into
consideration. It is generally accepted that cigarette smoking
plays an important role in lung carcinogenesis (4). In addition, epidemiological data
suggested that obesity is associated with an increased risk of
colon cancer (10). Diabetes and
high dietary meat intake are also associated with an increased risk
of colon cancer (11). In the
present study, there were 4 notable findings: First, we identified
that 17 (0.54%) of 3,102 patients with lung cancer had synchronous
colon cancer. In the present study, 13 (76.5%) of the 17 patients
were smokers, 11 of whom were >30-pack-year smokers. However,
only 5 (29.4%) had one of two smoking-related histological types of
lung cancer, namely squamous cell carcinoma and small-cell lung
carcinoma (SCLC). In addition, only 2 (11.8%) patients were
overweight (BMI ≥25.0 kg/m2) at the time of diagnosis.
These results suggested that several known and unknown factors may
exhibit a complex association with the synchronous development of
these two common cancers. Second, 15 (88.2%) of the 17 patients had
colon cancer at the lower part of the large intestine, namely
rectal cancer (n=8) and sigmoid cancer (n=7). Metastases from lung
cancer to the descending colon and rectum are extremely rare,
although there have been some case reports (12,13).
However, it is generally accepted that these lower parts of the
large intestine are the most common sites where primary colon
cancer develops (14). Third, the
cause of death of the 9 patients who succumbed to the disease
during the study period were directly associated with primary lung
cancer (7 NSCLCs and 2 SCLCs). Excluding 3 patients who were lost
to follow-up, 4 of the 5 patients who remain alive underwent
surgical resection of lung cancer. Our results suggested that lung
cancer is more likely to be the primary prognostic cancer rather
than colon cancer. However, appropriate evaluation of the clinical
stage is crucial for determining the optimal therapeutic strategy
and predicting the patients' prognosis. It has not been fully
elucidated why the prognosis of symptomatic patients was poorer
compared with that of asymptomatic patients. It was hypothesized
that the lung cancers in the latter group were more slow-growing.
The limited number of patients and the short period of follow-up
may have affected the results. Fourth, among the 17 patients, two
colon cancers (1 rectal and one sigmoid colon cancer), were
detected by PET/CT during the workup of primary lung cancer.
Pezzuto et al also reported a case exhibiting FDG uptake on
PET/CT (15). New diagnostic
modalities, such as PET/CT, may provide important clinical
information for patients with this rare condition (16,17).
There were certain limitations to the present study:
The study was conducted only on a database of lung cancer patients,
whereas it should also be conducted on a database of colon cancer
patients. In addition, the retrospective design limits the
generalization of the results. In light of our experience, it is
appropriate to consider heightened surveillance of patients with
synchronous lung and colon cancers, as early diagnosis and standard
therapy are the only chance for long-term survival and cure. Swift
evaluation of signs or symptoms that are suggestive not only of
lung cancer but also of colon cancer is recommended. Although the
incidence of synchronous lung and colon cancers may be low, future
genetic and epidemiological studies are required to elucidate the
potential connection between these two types of cancer.
References
|
1
|
Kurishima K, Satoh H, Kagohashi K, Homma
S, Nakayama H, Ohara G, Ishikawa H and Hizawa N: Patients with lung
cancer with metachronous or synchronous gastric cancer. Clin Lung
Cancer. 10:422–425. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ghosh SK, Roland NJ, Kumar A, Tandon S,
Lancaster JL, Jackson SR, Jones A, Jones H Lewis, Hanlon R and
Jones TM: Detection of synchronous lung tumors in patients
presenting with squamous cell carcinoma of the head and neck. Head
Neck. 31:1563–1570. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kato T, Suzuki K, Muto Y, Sasaki J,
Tsujinaka S, Kawamura YJ, Noda H, Horie H, Konishi F and Rikiyama
T: Multiple primary malignancies involving primary sporadic
colorectal cancer in Japan: Incidence of gastric cancer with
colorectal cancer patients may be higher than previously
recognized. World J Surg Oncol. 13:232015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Malhotra J, Malvezzi M, Negri E, La
Vecchia C and Boffetta P: Risk factors for lung cancer worldwide.
Eur Respir J. 48:889–902. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ezuka A, Sakai E, Kawana K, Nagase H,
Kakuta Y, Uchiyama S, Ohkubo H, Higurashi T, Nonaka T, Endo H, et
al: Association between factors associated with colorectal cancer
and rectal aberrant crypt foci in humans. Oncol Lett. 10:3689–3695.
2015.PubMed/NCBI
|
|
6
|
Yamanaka S, Sakamoto A and Tomoyasu H:
Synchronous multiple primary lung and colon cancers. Kyobu Geka.
66:882–885. 2013.(In Japanese). PubMed/NCBI
|
|
7
|
Nosaka S, Yamauchi N, Sasaki T, Hanada T
and Tamura K: Clinical study of synchronous double cancers of the
lung and digestive tract. Kyobu Geka. 51:400–402. 1998.(In
Japanese). PubMed/NCBI
|
|
8
|
Imataka A, Satoh H, Yamashita YT, Kamma H,
Ohtsuka M and Sekizawa K: Synchronous presentation of
adenocarcinoma in lung and colon. Australas J Cancer. 1:78–80.
2000.
|
|
9
|
Allemani C, Weir HK, Carreira H, Harewood
R, Spika D, Wang XS, Bannon F, Ahn JV, Johnson CJ, Bonaventure A,
et al: Global surveillance of cancer survival 1995–2009: Analysis
of individual data for 25,676,887 patients from 279
population-based registries in 67 countries (CONCORD-2). Lancet.
385:977–1010. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bardou M, Barkun AN and Martel M: Obesity
and colorectal cancer. Gut. 62:933–947. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Aykan NF: Red Meat and colorectal cancer.
Oncol Rev. 9:2882015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yamagishi H, Sakamoto T, Matsuda T,
Nakajima T and Saito Y: Solitary metastatic colon cancer showing a
small depressed configuration. Intern Med. 51:2321–2324. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Miyazu K and Kobayashi K: Rectal
metastasis from lung cancer; report of a case. Kyobu Geka.
65:165–167. 2012.(In Japanese). PubMed/NCBI
|
|
14
|
Dinning JP, Hixson LJ and Clark LC:
Prevalence of distal colonic neoplasia associated with proximal
colon cancers. Arch Intern Med. 154:853–856. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pezzuto A, Mariotta S, Fioretti F and
Uccini S: Metastasis to the colon from lung cancer presenting with
severe hyponatremia and dyspnea in a young male: A case report and
review of the literature. Oncol Lett. 5:1477–1480. 2013.PubMed/NCBI
|
|
16
|
Chen SH, Chan SC, Chao YK and Yen TC:
Detection of synchronous cancers by fluorodeoxyglucose positron
emission tomography/computed tomography during primary staging
workup for esophageal squamous cell carcinoma in Taiwan. PLoS One.
8:e828122013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Caballero Gullón L, Dorado I Borrego and
Vázquez Albertino R: A colon adenocarcinoma and a pharyngeal
carcinoma incidentally detected by means of (18)F-FDG PET in a
patient diagnosed of lung cancer. Rev Esp Med Nucl Nucl in a
patient diagnosed of lung cancer. Rev Esp Med Nucl. 29:29–31.
2010.(In Spanish). PubMed/NCBI
|