Introduction
An accessory spleen is a congenital defect, defined
as ectopic splenic parenchyma separated from the main body of the
spleen. Although the majority are benign and do not usually require
treatment, they may be mistaken for enlarged lymph nodes or
neoplasms. Primary retroperitoneal neoplasms are a group of rare
but diverse neoplasms that arise within the retroperitoneal space,
which account for 0.1–0.2% of all malignancies in the body.
Notably, 80–90% of all primary retroperitoneal tumors are malignant
(1,2).
Primary retroperitoneal neoplasms are classified as solid or cystic
masses. Solid neoplasms are divided into three main categories
according to the tissue of origin: Mesodermal tumors, neurogenic
tumors and extragonadal germ cell tumors (3). Computed tomography (CT) and magnetic
resonance imaging (MRI) are essential for the characterization of
primary retroperitoneal neoplasms, evaluating the extent of local
invasion, identification of metastases, and determination of the
optimal treatment response for such neoplasms (4). Therefore accurate preoperative diagnosis
is important in order to avoid unnecessary surgical intervention.
The current report discusses the case of a patient with a right
retroperitoneal accessory spleen, mimicking a retroperitoneal
neoplasm. Written informed consent was obtained from the patient's
family.
Case report
A 40-year-old woman without any abdominal discomfort
was referred to Zhejiang Hospital (Zhejiang, China) for surgical
excision, following the incidental detection by B ultrasound of a
right retroperitoneal neoplasm at Zhejiang Hospital. Routine
physical examination and laboratory data, including full blood
count, blood glucose, C-reactive protein, tumor markers and liver
function tests, were all unremarkable. Her medical history was
notable for a splenectomy performed in 2002, for splenic rupture as
a result of upper abdominal trauma.
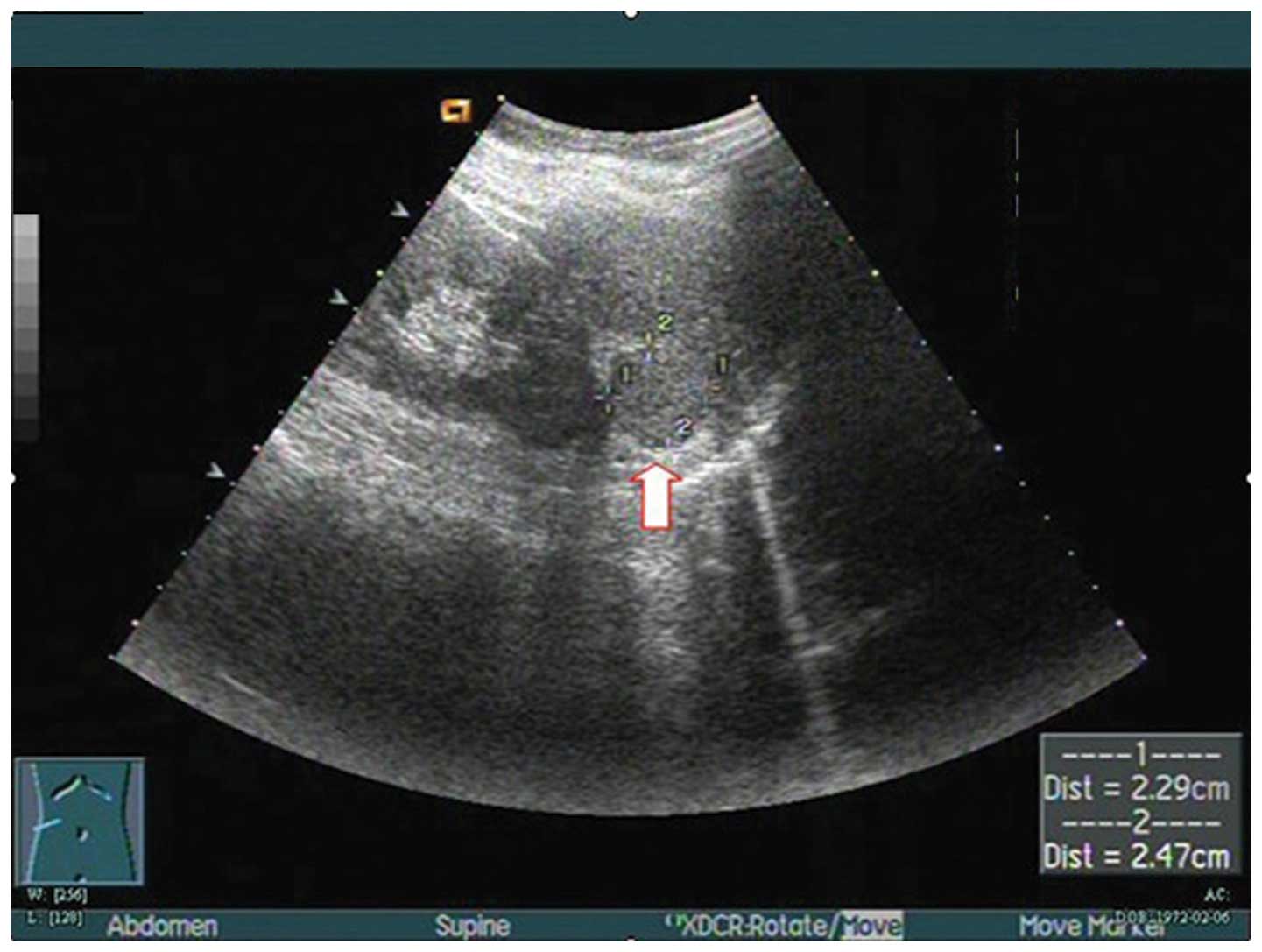
Ultrasonography demonstrated a space-occupying
neoplasm, with a less abundant vascular supply than the surrounding
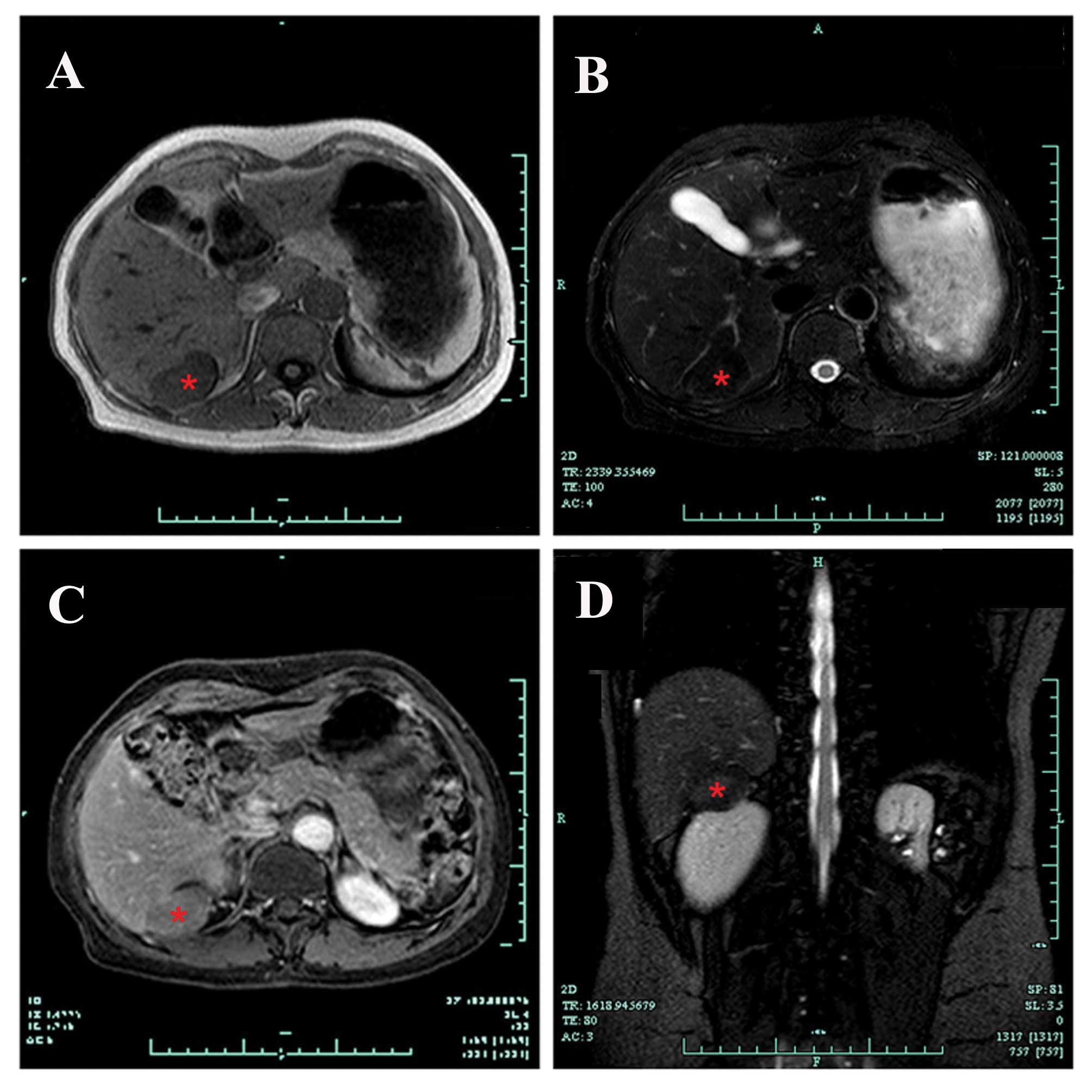
normal tissue, located in the right retroperitoneal space (Fig. 1). CT imaging revealed a
well-marginated ovoid neoplasm, of ~38.0×25.0 mm, in the right
retroperitoneal space. An MRI scan further confirmed the presence
of a neoplasm, with low signal intensity on T1-weighted images,
high signal intensity on T2-weighted images and slightly enhanced
signal intensity on the contrast-enhanced phases of dynamic MRI
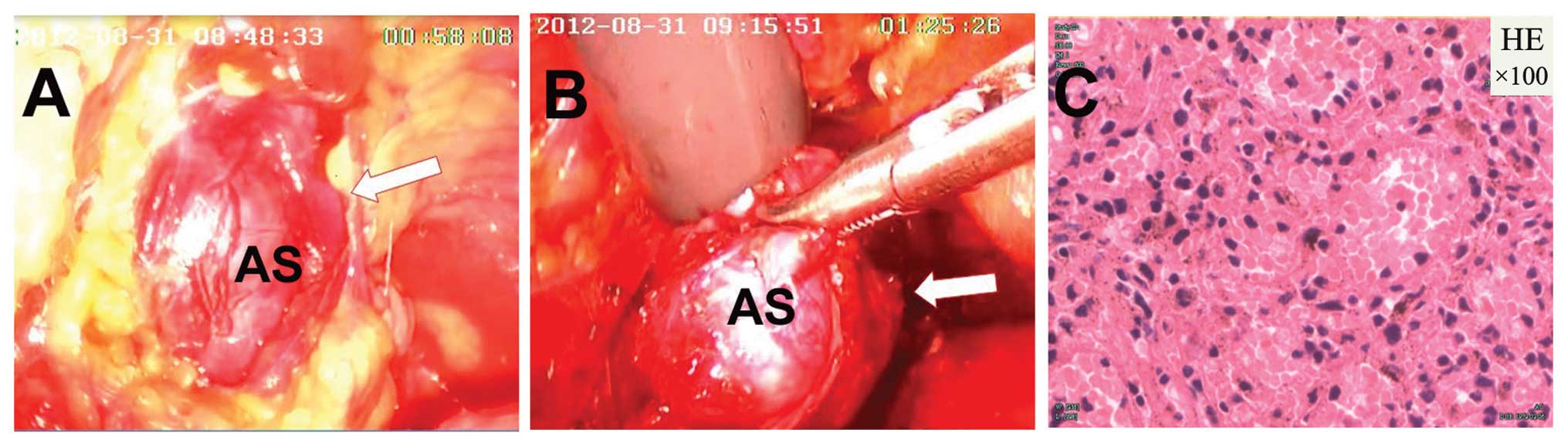
(Fig. 2). As a retroperitoneal
neoplasm of unknown origin had been identified, a
retroperitoneoscopic excision was conducted in order to remove the
neoplasm with minimal invasiveness. Pathological examination of the
resected specimen demonstrated splenic tissue (Fig. 3). The patient recovered well
post-operatively.
Discussion
Primary retroperitoneal neoplasms are relatively
rare. Malignant primary retroperitoneal neoplasms, which are more
common than benign neoplasms in the retroperitoneal neoplasm,
account for ~0.1% of all malignancies (5). When a retroperitoneal neoplasm of
unknown origin is detected, surgical removal may be conducted and a
definitive diagnosis may be made following pathological examination
of the surgical specimen (2).
An accessory spleen is a common congenital defect
that affects 10–30% of the population (6). They are generally small (15.0–20.0 mm)
and are primarily located in the splenic hilum (75%) or in the tail
of the pancreas (20%) (7).
Occasionally they may be located in the splenorenal ligament,
greater omentum, mesentery, presacral area, adnexal region,
scrotum, pelvic cavity, liver or the thorax (8–12).
Although an accessory spleen usually presents as an isolated
asymptomatic abnormality, it may have clinical significance as it
may be mistaken for an enlarged lymph node or a neoplasm.
Therefore, the accurate preoperative diagnosis of an accessory
spleen is important in order to avoid unnecessary surgery. CT/MRI
and scintigraphy with Tc-99 m are helpful in marking the diagnosis
of an accessory spleen (4).
In conclusion, the presence of an accessory spleen
in the right retroperitoneal space is extremely rare (2). When a retroperitoneal neoplasm is
detected, surgeons should be aware of the possibility of an
accessory spleen in this location, in order to make precise
preoperative diagnoses.
References
|
1
|
Osman S, Lehnert BE, Elojeimy S, Cruite I,
Mannelli L, Bhargava P and Moshiri M: A comprehensive review of the
retroperitoneal anatomy, neoplasms, and pattern of disease spread.
Curr Probl Diagn Radiol. 42:191–208. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tambo M, Fujimoto K, Miyake M, Hoshiyama
F, Matsushita C and Hirao Y: Clinicopathological review of 46
primary retroperitoneal tumors. Int J Urol. 14:785–788. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shah JD, Kirshenbaum M and Shah KD: CT
characteristics of primary retroperitoneal tumors and the
importance of differentiation from secondary retroperitoneal
tumors. Contemp Diagn Radiol. 31:1–5. 2008. View Article : Google Scholar
|
|
4
|
Zhang C and Zhang XF: Accessory spleen in
the greater omentum. Am J Surg. 202:e28–e30. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kim MK, Im CM, Oh SH, Kwon DD, Park K and
Ryu SB: Unusual presentation of right-side accessory spleen
mimicking a retroperitoneal tumor. Int J Urol. 15:739–740. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gardikis S, Pitiakoudis M, Sigalas I,
Theocharous E and Simopoulos C: Infarction of an accessory spleen
presenting as acute abdomen in a neonate. Eur J Pediatr Surg.
15:203–205. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang KR and Jia HM: Symptomatic accessory
spleen. Surgery. 144:476–477. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cowles RA and Lazar EL: Symptomatic pelvic
accessory spleen. Am J Surg. 194:225–226. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lee HJ, Kim YT, Kang CH and Kim JH: An
accessory spleen misrecognized as an intrathoracic mass. Eur J
Cardiothorac Surg. 28:6402005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lhuaire M, Sommacale D, Piardi T, Grenier
P, Diebold MD, Avisse C and Kianmanesh R: A rare cause of chronic
abdominal pain: Recurrent sub-torsions of an accessory spleen. J
Gastrointest Surg. 17:1893–1896. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rodriguez E, Netto G and Li QK:
Intrapancreatic accessory spleen: A case report and review of
literature. Diagn Cytopathol. 41:466–469. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Izzo L, Caputo M and Galati G:
Intrahepatic accessory spleen: Imaging features. Liver Int.
24:216–217. 2004. View Article : Google Scholar : PubMed/NCBI
|