Introduction
Osteosarcoma is the most common malignant bone tumor
in children, adolescents, and young adults. The occurring rate was
4.0 (3.5–4.6) for 0–14 year-old children per year per million of
people for males and females and from all ethnicities (1). Tumors arise primarily on the metaphysis,
which is near the growth plate and gradually invade the epiphysis
and eventually the whole joint space (2). The distal femur and proximal tibia are
the most common sites for osteosarcomas, and the epiphyses of the
distal femur and proximal tibia contribute ~35 and 30% to the
growth of the lower extremity, respectively (3).
With rising survival rates following chemotherapy,
limb salvage surgery is increasingly becoming the standard of care
for the majority of malignant neoplasms affecting the extremities
(4,5).
Segmental bone loss following tumor resection requires prosthesis
reconstruction in most adult patients, but may be difficult in
skeletally immature patients due to the necessity to preserve the
joint function maximally and maintain good limb function (6). This is a challenging situation for
surgeons treating patients following epiphysis resection and limb
reconstruction with the most suitable procedure in order for the
least length discrepancy compared with the ongoing growth of the
contralateral limb.
The growth plate has a key role in limb growth
(7). Assessment of the relationship
of the growth plate and tumor helps surgeons determine surgical
options based on the involvement of this region and the extent of
the tumor. This will have implications on the clinical result by
potentially affecting limb length and/or the function of the
involved. Therefore, clear images are the first step in treating
tumors in immature patients. In recent years, the extension of
these tumors has been determined through preoperative diagnostic
imaging techniques, primarily via magnetic resonance imaging (MRI)
(8). The extension of the tumor can
be accurately evaluated on T1-weighted, T2-weighted, and
Gd-enhanced T1-weighted MRI images in coronal, sagittal and axial
planes. According to the involved anatomical sites on MRI, Kumta
et al (9) classified the
location and extension of osteosarcoma in bone into five subtypes
as follows: Type 1, the tumor is located >2 cm from the
epiphyseal cartilage; type II, the tumor is located within ≤2 cm of
the epiphyseal cartilage; type III, the tumor extends to or beyond
the epiphyseal cartilage, but >1 cm of epiphyseal tissue is
retained; type IV, the tumor breaches the physes and extends to the
subchondral region but does not breach the articular surface; and
type V, the tumor breaches the articular surface and involves the
adjacent joint.
In the present study, osteosarcoma in immature
patients (open physis and age, <15 years) around the knee joint
was classified into five types according to the classification
system as described by Kumta et al (9) using preoperative MRI, and limb
reconstruction or amputation methods were performed following wide
resection. The goals of the present study were to assess: i)
Characteristics of osteosarcoma in immature patients, ii) different
MRI types with adequate surgical methods, iii) the benefits and
complications of different surgical methods, and iv) overall
survival (OS) rate and factors that affect OS.
Patients and methods
In the present study, the authors performed a
retrospective study of the characteristics and outcomes in immature
patients diagnosed with osteosarcoma around the knee joint treated
at the Henan Cancer Hospital (Zhengzhou, China).
Patients
The cohort consisted of 56 patients (age, <15
years) diagnosed with open physis with osteosarcoma at the distal
femur and proximal tibia between January 2007 and December 2015
that were treated at the Henan Cancer Hospital. Ethical approval
was obtained from the Medical Ethics Committee of the Henan Cancer
Hospital. Written informed consent was obtained from the patients'
legal guardians for publication of the present report and
accompanying images. The following information was collected: i)
Patient demographics including age at diagnosis, sex and date of
diagnosis; ii) tumor characteristics including location, Enneking
stage (10), subtype on MRI and
histology; iii) treatment including response to neoadjuvant
chemotherapy, type of primary surgery, postoperative treatment and
adverse effects; iv) clinical outcomes, including limb discrepancy,
OS, disease-free survival (DFS), event-free survival (EFS) and
predictive factors that are associated with survival.
Treatment
Chemotherapy was utilized in the neoadjuvant and
adjuvant settings. The chemotherapy regimens, specifically dose,
were based on body surface area of the patients. The chemotherapy
included combinations of high doses of methotrexate (Jiangsu
Hengrui Medicine Co., Ltd., Linyungang, China), carboplatin (Corden
Pharma Latina S.P.A., Sermoneta, Italy) (11), doxorubicin/pirarubicin (Shenzhen Main
Luck Pharmaceuticals Inc., Shenzhen, China) (12,13) and
ifosfamide (Jiangsu Hengrui Medicine Co., Ltd.). Each patient was
administered with all the agents. Tumor necrosis percentage (TNP)
was accessed by pathology following operation. The percentage area
of necrosis was calculated in at least 4 continuous slides of each
spice and the sum was used to give a percentage of necrosis of the
whole tumor under a light microscope (magnification, ×100).
Of the 56 patients, 4 abandoned the treatment while
the remaining 52 patients underwent surgery for local control and
had negative surgical margins as confirmed by pathology. The type
of surgery including limb salvage surgeries, such as tumor hinged
prosthesis replacement (TPR, Chun Li Co., Ltd., Beijing, China),
osteoarticular allograft replacement (OAR), inactivated
auto-osteoarticular replacement (IOR), intercalary allograft
replacement (IAR), autogenous bone replacement (ABR), amputation
(AP), rotation-plasty (RP) was based on the extent of disease,
involvement of neurovascular bundle, and appraisal for best limb
functionality following surgical resection. All structural
allograft bones were procured according to the protocol of the
Chinese Association of Tissue Banks (14) and obtained from the bone bank.
Trans-meta/epiphyseal osteotomy (15)
or physeal distraction (16) was used
to preserve the uninvolved physis (PUP) in certain patients.
Arthrodesis reconstruction was not performed in any of these
patients.
Follow-up
Oncology follow-up was performed at three monthly
intervals for the first two years and six monthly intervals until 5
years. Bone healing and implantation was assessed using
antero-posterior and lateral radiographs. The patients were checked
regularly to detect pulmonary metastases with computed tomography
(CT) scan. Functional results were assessed using the
Musculoskeletal Tumor Society (MSTS) score (17) at the last follow-up visit. Grading of
MSTS score is as follows: ≤23, excellent functional result; 15–22,
good result; 8–14, fair result and <8, poor result. Joint range
of motion, strength, muscular atrophy and lower limb length
discrepancy were also assessed at the follow-up visits. Final
limb-length discrepancy was measured by teleroentgenogram showing
the entire length of the legs on one film. The follow-up was mean
of 21.66 months. At the end of follow-up, the median age of the
patients was 14.31 years (range, 3–23 years), and 18 (32.14%)
patients reached skeletal maturity.
Statistical analysis
The primary focus of the present analysis was OS,
EFS and DFS. OS was calculated from the date of diagnosis to the
date of mortality or most recent follow-up examination. The
survival curves were calculated using the Kaplan-Meier estimate
with 95% confidence interval. The differences of survival curves
were assessed using the log-rank test. Adjusted estimates were
obtained from proportional hazards models with sex, age, clinical
Enneking stage (10), MRI type and
surgical method included as covariates. MSTS scores and differences
in limb length of different surgeries were compared using one-way
analysis of variance with the least significant difference by
comparing means for continuous variables. The associations between
the age at diagnosis and tumor invasion of the physis, response to
treatment and survival were compared using the Mann-Whitney test.
P<0.05 was considered to indicate a statistically significant
difference. SPSS software (version 11.5; SPSS, Inc., Chicago, IL,
USA) was used.
Results
Patient demographics
A total of 56 patients (age, <15 years) with
diagnosis of osteosarcoma around the knee joint were involved in
the present study. The complete demographics and clinical
characteristics are shown in Table I.
The median age, at the time of diagnosis, was 12.14 years (range,
3–15 years). There were 32 male patients (57.1%). Tumor location
was as follows: 41 (82%) at the distal femur and 15 (18%) at the
proximal tibia. High grade, conventional osteosarcoma was diagnosed
in all patients. A total of 49 (87.5%) patients had stage IIB
tumors and 7 (12.5%) had stage III tumors, according to the
Enneking stage classification.
 | Table I.Demographic and clinical
characteristics of 56 patients. |
Table I.
Demographic and clinical
characteristics of 56 patients.
| Patient
demographics | n | Cohort (%) |
|---|
| Age at diagnosis,
years |
|
0–3 | 1 | 1.8 |
|
3–6 | 1 | 1.8 |
|
6–9 | 9 | 16.1 |
|
9–12 | 12 | 21.4 |
|
12–15 | 33 | 58.9 |
| Mean age, years
(range) | 12.14 (3–15) |
|
| Sex |
|
Female | 24 | 42.9 |
|
Male | 32 | 57.1 |
| Tumor site |
| Left
distal femur | 27 | 48.2 |
| Right
distal femur | 14 | 25.0 |
| Left
proximal tibia | 5 | 8.9 |
| Right
proximal tibia | 10 | 17.9 |
| Clinical Enneking
stage |
|
IIB | 49 | 87.5 |
|
III | 7 | 12.5 |
Treatment
Therapy methods are shown in Fig. 1 and were based on MRI findings prior
to operation. There were 45 (80.36%) limb growth plates and
epiphyses closed to or invaded by tumor from MRI type III to V. In
7 patients with stage III, a total of 4 patients (1 with type III
and 2 with type IV) abandoned additional interventions, 3 with lung
metastases (2 with type V and 1 with type IV) underwent debulking
surgery, which comprised amputations (according to the patient's
choice) and 2–6 cycles of chemotherapy. In other patients with
stage IIB, a total of 4 patients (1 with type V, 2 with type IV and
1 with type III) underwent amputations due to massive tumor sizes
and insensitivity to chemotherapy, 3 patients (2 with type III and
1 with type IV) underwent rotation-plasty (Fig. 2A), and the remaining 42 patients
underwent various limb saving surgeries. A patient each with type
III, IV and V was treated by semi femur TPR, to preserve the
adjacent semi joint and growing physis (Fig. 2B). TPR is widely adapted for tumors
growing close to joints (18,19). In the present study, a total of 18
(42.86%) cases (7, 7, 4 with types III, IV, V, respectively)
accepted this method (Fig. 2C). A
total of 21 patients had biological constructions as follows: 4
patients with type 1 underwent resection of the tumor by transverse
osteotomy at the metaphysis with retention of the physeal plate and
a small portion of the adjacent metaphysis. Subsequently, IAR was
used to reconstruct the defect in 1 patient, and inactive
(anhydrous alcohol, 40 min) autogenous bone replacement (ABR) was
performed in 3 patients. A total of 6 patients with type II
preserved PUP by physeal distraction, which was then reconstructed
by IAR (Fig. 2D) in 5 patients and
ABR in 1 patient (Fig. 2E). Due to
the tumor invasion of the physis in types III–V, 4 cases underwent
intraepiphyseal resection and reconstructed by IAR (2 with type III
and IV). A total of 5 patients underwent OAR (3 with type III, 1
with type IV and 1 with type V; Fig.
2F). A total of 2 (1 with type III and 1 with type IV)
underwent inactivated auto-osteoarticular replacement (IOR;
inactivation with anhydrous alcohol for 40 min).
 | Figure 1.Treatment methods classified according
to MRI types in 56 patients. AP, amputation; PUP, preserve the
uninvolved physis; ABR, inactive autogenous bone replacement; IAR,
intercalary allograft replacement; OAR, osteoarticular allograft
replacement; IOR, inactivated auto-osteoarticular replacement; TPR,
tumor prosthesis replacement; STPR, semi tumor prosthesis
replacement; RP, rotation-plasty; MRI, magnetic resonance
imaging. |
Follow-up
A total of 21 patients (37.5%) succumbed to disease,
including local recurrence in 4 patients who underwent amputation
at 6–39 months postoperatively. A total of 17 patients succumbed to
pulmonary metastases. A total of 3 patients went through one or
more times of surgical resection of pulmonary recurrence and 1
patient survived for 42 months at the end of follow-up. The mean
time of mortality was 13.14 months following diagnosis (Table II). All patients experienced mild to
severe myelosuppression but without renal or cardiac toxicity.
| Table II.Outcomes and complications of
different operation methods. |
Table II.
Outcomes and complications of
different operation methods.
|
|
|
|
| Complications,
n |
|---|
|
|
|
|
|
|
|---|
| Operation
methods | Cases, n | MSTS 93
scorea | Limb length
discrepancy, cma | Recurrence | Metastasis | Infection | Nonunion | Fracture |
|---|
| TPR | 18 | 24.89±2.65 | 2.64±1.91 | 2 | 5 | 2 | 0 | 0 |
| STPR | 3 | 23.33±2.08 | 2.50±0.71 | 0 | 1 | 0 | 0 | 0 |
| PUP+IAR | 10 | 23.40±6.33 | 2.71±1.25 | 1 | 2 | 1 | 5 | 1 |
| PUP+ABR | 4 | 25.25±3.59 | 3.33±3.21 | 1 | 0 | 0 | 2 | 1 |
| OAR | 5 | 21.40±3.85 | 6.00±1.41 | 0 | 2 | 1 | 3 | 1 |
| IOR | 2 |
12.50±3.54b | 6.00±3.61 | 0 | 1 | 0 | 2 | 0 |
| RP | 3 | 24.67±1.53 |
| 0 | 1 | 0 | 0 | 0 |
| AP | 7 |
14.50±2.65b |
| 0 | 5 | 0 | 0 | 0 |
According to post-operative pathological
examination, the TNP was >90% in 32 (61.54%) patients, 80–90% in
17 cases (32.69%) and <80% in 3 cases (5.77%). There were no
significant differences in age at diagnosis and tumor invasion of
the physis (P=0.705), but differences in response to treatment and
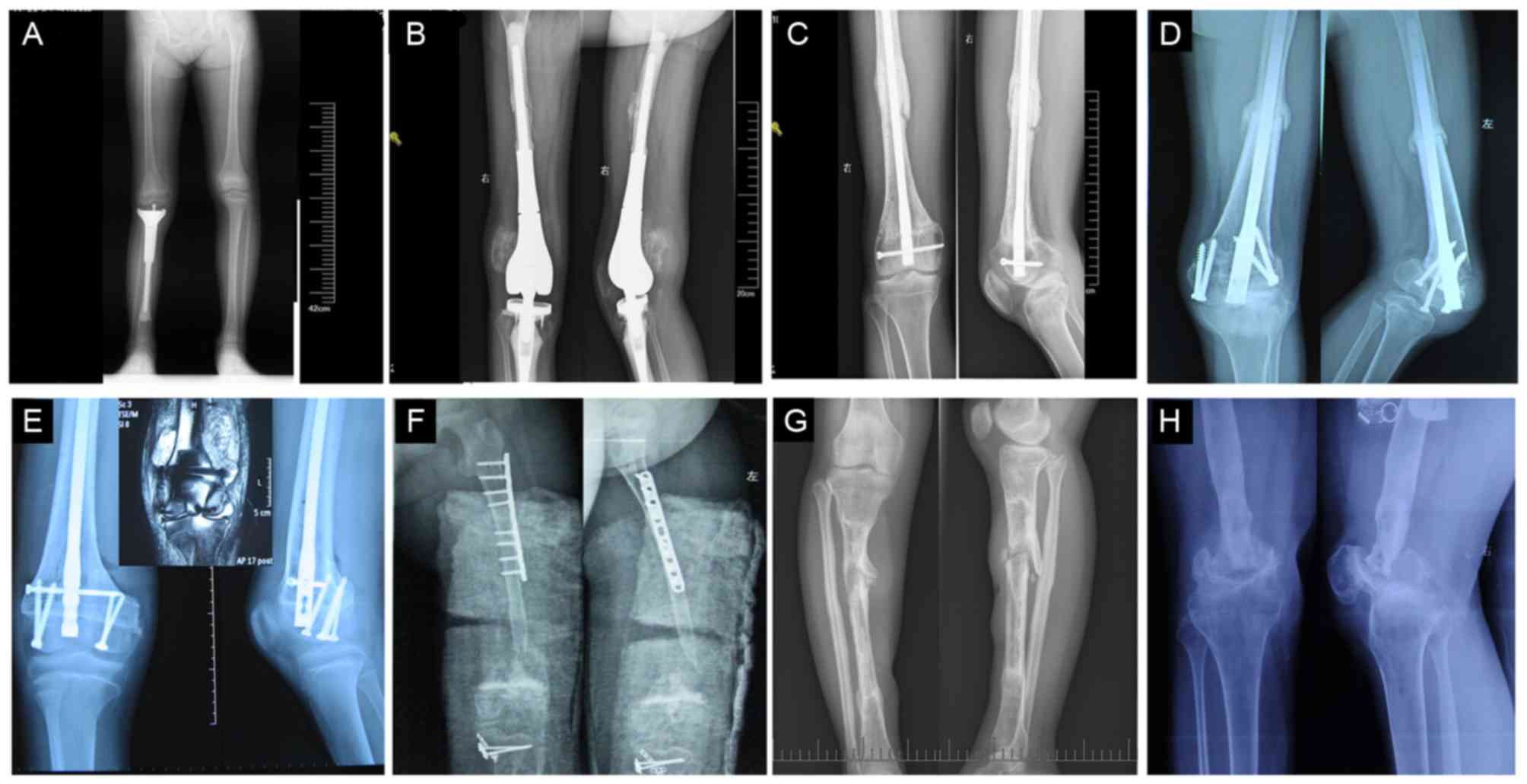
survival were significant (P<0.0001). Fig. 3 depicts follow-up images of
patients.
In the present study, excellent functional result
according to MSTS score was achieved in the TPR, PUP plus ABR and
PR groups. Good result was achieved in the semi tumor prosthesis
replacement (STPR, Fig. 3A), PUP plus
IAR and OAR groups. Fair result was achieved in the AP and IOR
groups. In the IOR group, two 6-year-old patients without suitable
osteoarticular allograft had restrictions in recreational
activities for 6–12 months due to absorption and nonunion of
inactivated osteoarticular. This caused the low MSTS score and
dysfunction of the knee joint (Table
II).
Recurrence (2 cases, 16.67%) and infection (2 cases,
16.67%) were the main complications in the TPR group (Table. II and Fig.
3B). Patients with local tumor recurrence underwent
amputations. Prosthesis was removed in one patient who developed
deep infection, a temporary cement spacer was implanted and
antibiotics of Cefotiam were administered. After 6 months of
treatment and observation, another prosthesis was replaced. The
other patient with delayed infected prostheses (occurred at 24
months following surgery) underwent immediate amputation. During
the follow-up, loosening or fractures of prostheses were not seen
in these patients. In patients of biological reconstructions, the
main complications were delayed union (12 cases, 57.14%) and
fracture (3 cases, 14.29%). Delayed union occurred at the
diaphyseal in 7, at metaphyseal in 3 case and at both places in 2
cases (Fig. 3C and D). The delayed
union was treated by autologous iliac bone replantation and/or
replacement of internal fixation, which eventually resulted in
union in 10 cases (90.48%) at the host donor junction. All the
fractures occurred when the internal fixation had been taken out
48–72 months following tumor resection (Fig. 3G). Patients refused additional
operation without pain of the involved limb.
Limb-length discrepancies (0–3 cm) were observed in
four patients in MRI type I with both physes preserved caused by
the growth plate partly injured by internal fixations. In the
remaining 38 limb-saving patients, limb-length discrepancy
developed as a result of loss of one or two physes (Fig. 3A). At final follow-up, the mean
shortage was 3.32 cm (range, 1–10 cm). There was no asociation
between surgical methods, age at the time of diagnosis with limb
discrepancies (P>0.05). A total of 18 patients had no
discernible limp, 20 cases had a minor cosmetic limp and 4 cases
had a major cosmetic limp.
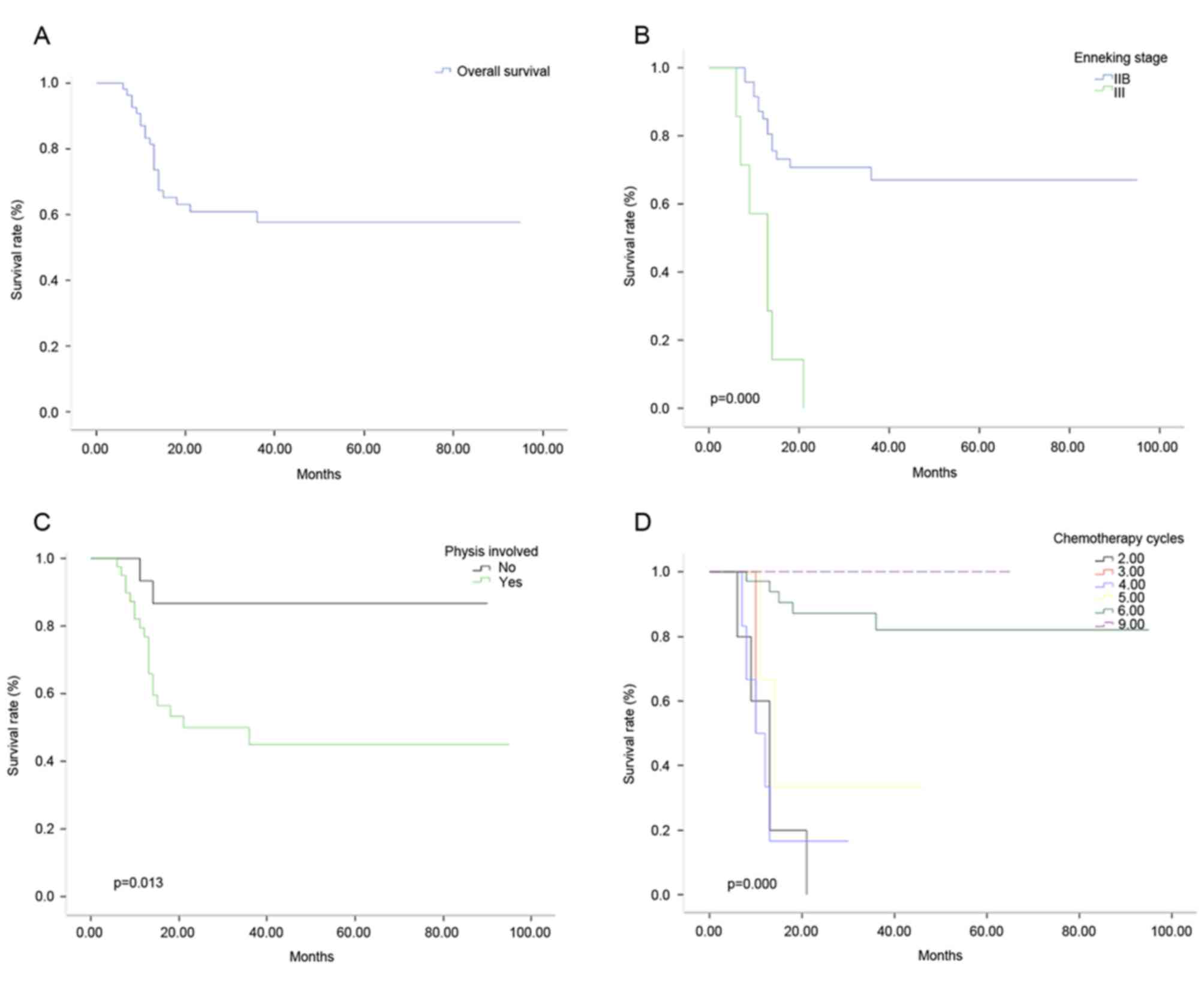
Survival
The OS rate was 57.66% in 56 patients (Fig. 4A), the 2 and 5 year DFS was 48.21 and
10.71% respectively. The EFS of 1, 2 and 3 years was 85.02, 60.27
and 57.80%, respectively. The OS rates were 67.01 and 0% for
patients at Enneking stages IIB and III (Fig. 4B), respectively, and 86.67 and 44.97%
for patients with and without physis (Fig. 4C), respectively. In patients with 6
and 5 cycles of chemotherapy, the OS rates were 82.17 and 33.33%,
respectively (Fig. 4D; P<0.05).
There were no statistically significant differences in sex, age,
surgical method and tumor location in relation to OS.
Discussion
In mature patients, prosthesis replacement is the
main method for limb salvage surgery of malignant bone tumor
(20). However, it is a controversial
issue in patients with an immature skeletal age. At present, a
variety of procedures have been used in these young patients,
including prostheses, biological reconstruction, arthrodesis,
rotation-plasty (21–23) and amputations. Children who undergo
limb-sparing surgery of the lower limbs will face various problems
postoperatively as they grow. In particular, limb-length
discrepancies and loosening involving the prosthesis can cause
serious limb dysfunction (24,25).
Ablative surgery (amputation or rotation-plasty) was
performed in patients with Enneking stage III disease (with lung
metastasis and debulking surgery), local recurrence, extensive
sarcoma and in those who were unresponsive to chemotherapy or were
young (<9 years old). Amputation can leave cosmetic, emotional
and functional defects. In the present study, amputation was
performed in 7 patients. Rotation-plasty permits the concurrent
correction of limb-length discrepancies (26). Limb reconstruction is a good
alternative to prosthetic limb with excellent function in young
patients with a short recovery time, normal knee movement and no
adverse events during follow-up, however for many patients there
might be emotional and cosmetic concerns (27). In the present study, only three
patients accepted rotation-plasty.
Hinged tumor prosthesis was used in immature
patients (18 cases) in limb sparing surgery, because it fills the
defect and immediately restores knee joint function and limb
biomechanical stability. In the present cohort, 45 limb growth
plates and epiphyses were invaded by tumor, and resection of tumor
resulted in the loss of a significant portion of the joint
surface.
Tumor prosthesis may be considered as one of the
most convenient reconstructive options (20,21). At
present, epiphysis non-invasive expandable prosthesis is not
commonly used in China due to high price, scarce lengthening
equipment and high rate of complications, including distracted
neurovascular injuries, deep infection and aseptic loosening of
implantation (25,28). Meanwhile, reconstruction with
prosthesis compromises the growing physis. The growth physis of the
segment is compromised by the tumor, and the physis of the opposite
side of the joint may be physiologically altered in its growing
potential by the intra-medullary stem perforation (29). This may cause inevitable limb
discrepancy particularly in young children (age, <9 years).
Therefore, a remodeled prosthesis with a smaller diameter (<10
mm) for intra-medullary stem was used in the present study, and the
healthy part of the epiphysis was preserved (Fig. 2C). The involved limb with semi tibia
prosthesis was also reconstructed (hemiarthroplasty) in 3 cases
(Fig. 2B), as only the growth physis
of the segment compromised by the tumor was sacrificed and the
unaffected opposing joint cartilage was retained. Hemiarthroplasty
resulted in multi-directional instability and limited the movement
of knee joint during the follow-up. The limb length discrepancy
ranged from 1 to 6 cm (average, 2.60 cm) in TPR and STPR groups. In
the two recurrences in the TPR group, huge tumor size (diameter,
>10 cm), reduced sensitivity to chemotherapy (tumor necrosis
rate <90%) and an inadequate resection margin were the main
reasons of relapse.
In the long run, prosthesis may result in high rates
of mechanical complications and limited articular function. In
addition, as surviving patients have long life expectancy, it is
very difficult for any prosthetic reconstruction to achieve
durability during this time (30).
Compared with prosthesis replacement, biologic
reconstructions require graft material to incorporate within the
host. Once the graft bone has been substituted by autologous bone,
a lower complication rate than prosthesis over time follows
(31). Therefore, massive bone graft
is commonly used in growing patients with long life expectations.
Therefore, different resection and reconstruction methods were
adopted according to the MRI image classification obtained prior to
the operation (9).
In the present study, when a safe margin was present
between the tumor and the growth plate and epiphysis, transverse
osteotomy at the metaphysis was performed in patients with MRI type
I as described by Kumta et al (9). Physeal distraction was performed in
patients with MRI type II to preserve the joint surface and
maintain joint function as described by Cañadell et al
(16). Once safe margins were
confirmed during operation by histological examination, replacement
was applied by inactive autogenous bone or intercalary allograft.
In cases with MRI type III, as the tumors are intact with the
growth plate, intra-epiphyseal resection or osteoarticular
replacement is used as an alternative to endoprosthetic
reconstruction (16). However, care
must be taken when determining surgical margins, and the tumor
should not cross the growth plate for intra-epiphyseal resection
(32). In the present study, although
safe epiphyseal resection margins have been confirmed by pathology,
2 cases in the cohort relapsed within 6–12 months during follow-up
(Fig. 3E, Table II). In cases with MRI type IV and V,
osteoarticular allograft replacement was the preferred choice of
treatment due to the invasion of growth plate and epiphysis by
tumor cells as previously described by Kumta et al (9). In osteoarticular reconstructions in our
study, the remaining ligaments were reattached to the corresponding
allograft or inactive tissues by a direct lateral-lateral interval
suture to improve stability. The host meniscus was reattached to
the osteoarticular allograft, and both horn insertions and the
articular capsule were sutured. The cruciate ligament of allograft
or inactive tissues were inserted and fixed to host bone (33).
In the present study, the results indicated that
preservation of the PUP with adequate margins and biological
reconstruction in MRI types I, II and III may be an alternative to
endoprosthetic reconstruction. The clinical results from PUP and
endoprosthetic reconstruction indicated equal MSTS scores and knee
joint function. As the patients' own joint cartilage and
stabilizing structures, and the potential for continued axial
growth can be retained, permanent curative effect can be acquired
(34). The limb length discrepancy
was 1–10 cm (average, 2.83 cm) in the PUP plus IAR and PUP plus ABR
groups in the present study. Discrepancy in the current cohort was
not treated, as the normal life of the patients was not seriously
affected.
In the present study, a better functional result was
observed for endoprosthetic replacement than osteoarticular
reconstruction in patients with MRI types IV and V. Due to the
corrosion of joint fluid and long time restriction of movement,
evident bone absorption and knee joint stiffness can be observed in
the majority of osteoarticular replacement patients in the present
study. Joint instability, degeneration of cartilage and metaphyseal
fractures were observed in the patients in the present study
(Fig. 3F and H), consistent with the
findings of DeGroot et al (33). Joint instability, degeneration of
cartilage and metaphyseal fractures caused lower MSTS scores and
reduced knee joint function compared with prosthesis replacement.
The limb length discrepancy ranged from 4–9 cm (average, 6.17 cm)
in the OAR and IOR groups.
In the present study, the results indicated that
infections, particularly deep infections, which is a serious
impediment and may require an amputation, are the main
complications in prosthetic reconstruction. However, delayed or
nonunion and fractures are the primary complications in biological
constructions. The delayed union can be identified by progressive,
massive absorption of the graft at the bone-graft junction, as the
replaced allograft or inactive autologous bone lacks adequate blood
supply. The treatment involves additional surgery with new
autograft and changed fixation. To accelerate bone healing, a part
of the intramedullary locked screws is usually removed 12 months
following surgery to obtain a dynamic compressive force on the
fracture surface, which can result in bony union in some cases
(35).
The ultimate non-union rate in the present study was
9.52%, which is similar to the rate reported in other studies
(36,37). In osteoarticular reconstructions,
progressive articular degeneration was observed in the majority of
patients as early as 3–5 years following implantation, resulting in
narrow joint space and pain, decreased function of involved joint
(Fig. 3H).
A number of factors have been reported to affect the
clinical effect and patient survival rate of osteosarcoma. Faisham
et al (38) analyzed 163
patients with osteosarcoma with an average age of 19 years (range,
6–59 years). It was reported that the OS rate in patients who
completed chemotherapy and surgery (n=117) was 72% at 2 years and
44% at 5 years post-treatment. The factors that affected survival
rate were surgery methods (limb salvage prior to amputation) and
the presence of lung metastasis. Ayerza et al (39) retrospectively reviewed 251 patients
with high-grade osteosarcoma from 1980 to 1989 and reported higher
rates of limb salvage treatment and survival, with a lower
incidence of secondary amputation occurring with the use of
chemotherapy. In the present study, the factors affecting overall
survival rate included clinical Enneking stage, involvement of the
growth plate, and cycles of chemotherapy.
However, individualized surgical procedures were
performed on a limited number of 56 patients, and it would
therefore be difficult to compare substantially different
techniques with the same surgeon. Another limitation is a
relatively short follow-up period (range, 2–95 months; average,
21.66 months) and that only some of the patients (18 cases, 32.14%)
reached their skeletal maturity at the last follow-up. Therefore,
it was not possible to establish any final limb-length discrepancy.
A longer follow-up is necessary to establish long-term survival of
the different reconstructions and final limb-length
discrepancies.
Different limb surgeries, including epiphysis/physis
preservation with biological construction in MRI types I to III,
endoprosthetic/osteoarticular reconstruction in MRI types IV and V,
are useful in the management of osteosarcoma in growing young
patients with proper surgery indications, and maintains knee joint
function with acceptable complications including limb discrepancy,
delayed union, infection, recurrence and fracture.
References
|
1
|
Ottaviani G and Jaffe N: The epidemiology
of osteosarcoma. Cancer Treat Res. 152:3–13. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen Y, Yu XC, Xu SF, Xu M and Song RX:
Impacts of tumor location, nature and bone destruction of extremity
osteosarcoma on selection of limb salvage operative procedure.
Orthop Surg. 8:139–149. 2016. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Haynes K, Tyner C and Williams PD:
Repiphysis prosthesis for limb preservation in pediatric patients
with bone cancer: A literature review. Orthop Nurs. 32:81–86. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kudawara I, Aoki Y, Ueda T, Araki N, Naka
N, Nakanishi H, Matsumine A, Ieguchi M, Mori S, Myoui A, et al:
Neoadjuvant and adjuvant chemotherapy with high-dose ifosfamide,
doxorubicin, cisplatin and high-dose methotrexate in non-metastatic
osteosarcoma of the extremities: A phase II trial in Japan. J
Chemother. 25:41–48. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hegyi M, Semsei AF, Jakab Z, Antal I, Kiss
J, Szendroi M, Csoka M and Kovacs G: Good prognosis of localized
osteosarcoma in young patients treated with limb-salvage surgery
and chemotherapy. Pediatr Blood Cancer. 57:415–422. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Eleutério SJ, Senerchia AA, Almeida MT, Da
Costa CM, Lustosa D, Calheiros LM, Barreto JH, Brunetto AL, Macedo
CR and Petrilli AS: Osteosarcoma in patients younger than 12 years
old without metastases have similar prognosis as adolescent and
young adults. Pediatr Blood Cancer. 62:1209–1213. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ruzbarsky JJ, Goodbody C and Dodwell E:
Closing the growth plate: A review of indications and surgical
options. Curr Opin Pediatr. 29:80–86. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hao YK, Zhang YK, Yang ZP, Li X, Yang Q
and Li JM: The accuracy of magnetic resonance imaging in
determining the osteotomy plane in osteosarcoma. Orthopedics.
31:5442008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kumta SM, Chow TC, Griffith J, Li CK, Kew
J and Leung PC: Classifying the location of osteosarcoma with
reference to the epiphyseal plate helps determine the optimal
skeletal resection in limb salvage procedures. Arch Orthop Trauma
Surg. 119:327–331. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Enneking WF, Springfield D and Gross M:
The surgical treatment of parosteal osteosarcoma in long bones. J
Bone Joint Surg Am. 67:125–135. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Skorupski KA, Uhl JM, Szivek A, Frazier
Allstadt SD, Rebhun RB and Rodriguez CO Jr: Carboplatin versus
alternating carboplatin and doxorubicin for the adjuvant treatment
of canine appendicular osteosarcoma: A randomized, phase III trial.
Vet Comp Oncol. 14:81–87. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schwartz CL, Wexler LH, Krailo MD, Teot
LA, Devidas M, Steinherz LJ, Goorin AM, Gebhardt MC, Healey JH,
Sato JK, et al: Intensified chemotherapy with dexrazoxane
cardioprotection in newly diagnosed nonmetastatic osteosarcoma: A
report from the children's oncology group. Pediatr Blood Cancer.
63:54–61. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yu W, Tang L, Lin F, Yao Y and Shen Z:
Pirarubicin versus doxorubicin in neoadjuvant/adjuvant chemotherapy
for stage IIB limb high-grade osteosarcoma: Does the analog matter?
Med Oncol. 32:3072015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
American Association of Tissue Banks:
American Association of Tissue Banks provisional guidelines for
cell, tissue and organ preservation: Reproductive council
guidelines. Newsl Am Assoc Tissue Banks. 4 Suppl:S37–S40. 1980.
|
|
15
|
Tsuchiya H, Abdel-Wanis ME, Sakurakichi K,
Yamashiro T and Tomita K: Osteosarcoma around the knee.
Intraepiphyseal excision and biological reconstruction with
distraction osteogenesis. J Bone Joint Surg Br. 84:1162–1166. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cañadell J, Forriol F and Cara JA: Removal
of metaphyseal bone tumours with preservation of the epiphysis.
Physeal distraction before excision. J Bone Joint Surg Br.
76:127–132. 1994.PubMed/NCBI
|
|
17
|
Enneking WF, Dunham W, Gebhardt MC,
Malawar M and Pritchard DJ: A system for the functional evaluation
of reconstructive procedures after surgical treatment of tumors of
the musculoskeletal system. Clin Orthop Relat Res. 286:241–246.
1993.
|
|
18
|
Tan PX, Yong BC, Wang J, Huang G, Yin JQ,
Zou CY, Xie XB, Tang QL and Shen JN: Analysis of the efficacy and
prognosis of limb-salvage surgery for osteosarcoma around the knee.
Eur J Surg Oncol. 38:1171–1177. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bi W, Wang W, Han G, Jia J and Xu M:
Osteosarcoma around the knee treated with neoadjuvant chemotherapy
and a custom-designed prosthesis. Orthopedics. 36:e444–e450. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Houdek MT, Watts CD, Wyles CC, Rose PS,
Taunton MJ and Sim FH: Functional and oncologic outcome of cemented
endoprosthesis for malignant proximal femoral tumors. J Surg Oncol.
114:501–506. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ieguchi M, Hoshi M, Aono M, Takada J,
Ohebisu N, Kudawara I and Nakamura H: Knee reconstruction with
endoprosthesis after extra-articular and intra-articular resection
of osteosarcoma. Jpn J Clin Oncol. 44:812–817. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hahn SB, Park HJ, Kim HS, Kim SH and Shin
KH: Surgical treatment of malignant and aggressive bone tumors
around the knee by segmental resection and rotationplasty. Yonsei
Med J. 44:485–492. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Campanacci L, Alì N, Casanova JM, Kreshak
J and Manfrini M: Resurfaced allograft-prosthetic composite for
proximal tibial reconstruction in children: Intermediate-term
results of an original technique. J Bone Joint Surg Am. 97:241–250.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Abdel-Ghani H, Ebeid W and El-Barbary H:
Management of combined nonunion and limb-length discrepancy after
vascularised fibular grafting. J Bone Joint Surg Br. 92:267–272.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cipriano CA, Gruzinova IS, Frank RM,
Gitelis S and Virkus WW: Frequent complications and severe bone
loss associated with the repiphysis expandable distal femoral
prosthesis. Clin Orthop Relat Res. 473:831–838. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sawamura C, Matsumoto S, Shimoji T, Ae K,
Tanizawa T, Gokita T, Koyanagi H and Okawa A: Indications for and
surgical complications of rotationplasty. J Orthop Sci. 17:775–781.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Forni C, Gaudenzi N, Zoli M, Manfrini M,
Benedetti MG, Pignotti E and Chiari P: Living with
rotationplasty-quality of life in rotationplasty patients from
childhood to adulthood. J Surg Oncol. 105:331–336. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Dotan A, Dadia S, Bickels J, Nirkin A,
Flusser G, Issakov J, Neumann Y, Cohen I, Ben-Arush M, Kollender Y
and Meller I: Expandable endoprosthesis for limb-sparing surgery in
children: Long-term results. J Child Orthop. 4:391–400. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Arteau A, Lewis VO, Moon BS, Satcher RL,
Bird JE and Lin PP: Tibial growth disturbance following distal
femoral resection and expandable endoprosthetic reconstruction. J
Bone Joint Surg Am. 97:e722015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Abed YY, Beltrami G, Campanacci DA,
Innocenti M, Scoccianti G and Capanna R: Biological reconstruction
after resection of bone tumours around the knee: Long-term
follow-up. J Bone Jt Surg Br. 91:1366–1372. 2009. View Article : Google Scholar
|
|
31
|
Bus MP, Dijkstra PD, van de Sande MA,
Taminiau AH, Schreuder HW, Jutte PC, van der Geest IC, Schaap GR
and Bramer JA: Intercalary allograft reconstructions following
resection of primary bone tumors: A nationwide multicenter study. J
Bone Joint Surg Am. 96:e262014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Aponte-Tinao L, Ayerza MA, Muscolo DL and
Farfalli GL: Survival, recurrence and function after epiphyseal
preservation and allograft reconstruction in osteosarcoma of the
knee. Clin Orthop Relat Res. 473:1789–1796. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
DeGroot H III and Mankin H: Total knee
arthroplasty in patients who have massive osteoarticular
allografts. Clin Orthop Relat Res. 373:62–72. 2000. View Article : Google Scholar
|
|
34
|
Muscolo DL, Ayerza MA, Aponte-Tinao LA and
Ranalletta M: Partial epiphyseal preservation and intercalary
allograft reconstruction in high-grade metaphyseal osteosarcoma of
the knee. J Bone Joint Surg Am. 86:2686–2693. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Karakaşli A, Satoğlu İS and Havitçioğlu H:
A new intramedullary sustained dynamic compression nail for the
treatment of long bone fractures: A biomechanical study. Eklem
Hastalik Cerrahisi. 26:64–71. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Bus MP, Dijkstra PD, van de Sande MA,
Taminiau AH, Schreuder HW, Jutte PC, vander Geest IC, Schaap GR and
Bramer JA: Intercalary allograft reconstructions following
resection of primary bone tumors: A nationwide multicenter study. J
Bone Joint Surg Am. 96:e262014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Hornicek FJ, Gebhardt MC, Tomford WW,
Sorger JI, Zavatta M, Menzner JP and Mankin HJ: Factors affecting
nonunion of the allograft-host junction. Clin Orthop Relat Res.
382:87–98. 2001. View Article : Google Scholar
|
|
38
|
Faisham WI, Saad Mat AZ, Alsaigh LN, Azman
Nor MZ, Imran Kamarul M, Biswal BM, Bhavaraju VM, Salzihan MS,
Hasnan J, Ezane AM, et al: Prognostic factors and survival rate of
osteosarcoma: A single-institution study. Asia Pac J Clin Oncol.
13:e104–e110. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ayerza MA, Farfalli GL, Aponte-Tinao L and
Muscolo DL: Does increased rate of limb-sparing surgery affect
survival in osteosarcoma? Clin Orthop Relat Res. 468:2854–2859.
2010. View Article : Google Scholar : PubMed/NCBI
|