Introduction
Osteosarcoma is the most common primary malignant
bone tumor of obscure origin, which generally presents in the
second decade of life (1). The
distal radius is a relatively common skeletal site for primary bone
tumors, however, not for osteosarcoma; it was reported that <1%
of osteosarcomas arise in the distal radius (2). En bloc resection of the distal radius
is the mainstream treatment for malignant lesions and aggressive
benign lesions (3). This poses a
dual limitation of skeletal reconstruction and functional
restoration due to the high functional demands of the hand, the
long life expectancy of the patients, particularly for osteosarcoma
treated with neoadjuvant chemotherapy and limb salvage, and the
limited amount of surrounding soft tissue as well as the proximity
of the adjacent nerves and tendons. The various procedures
described include arthrodesis using bulk autograft (4), ulnar translocation (5), reconstruction with non-vascularized or
vascularized fibular grafts (6,7),
osteoarticular allograft (8) and
prosthetic replacement (9). En bloc
resection of the distal radius destroys the structure of distal
radioulnar articulation and radiocarpal joint and results in the
postoperative instability of radiocarpal articulation (10,11).
This report presents a 17-year-old male with an osteosarcoma of the
distal radius, which was treated by en bloc resection and
reconstructed with a fibular shaft, thus preserving the radiocarpal
joint. This technique enables a biological reconstruction with a
precise anatomical fit, and avoids long-term endoprosthetic
complications and the need for maintenance of bone-banking
facilities for allografts. To the best of our knowledge, this
report is the first to describe a case of osteosarcoma of the
distal radius treated with this technique.
Case report
A 17-year-old male complained of mild right wrist
pain for approximately two months. Physical examination at the
Department of Orthopedics, The General Hospital of Jinan Military
Commanding Region (Jinan, China) revealed diffuse swelling, mild
tenderness and local heat at the distal end of the right radius. A
hard mass with an irregular surface (size, 3×2 cm) was palpated in
the dorsal aspect of the distal radius. Wrist motion was slightly
restricted (extension, 55° and flexion, 45°). Radiographs showed
diffuse osteosclerosis and focal osteolysis with periosteal
reaction in the distal radius metaphysis. Magnetic resonance
imaging (MRI) revealed a hypointense lesion on T1-weighted images
and a hyperintense lesion on T2-weighted images with soft tissue
extension. No epiphyseal involvement was identified on the MRI
(Fig. 1). Technetium-99m
scintigraphy showed an increased isotope uptake within the lesion.
A chest computed tomography (CT) scan revealed no abnormalities.
Laboratory data, including blood cell counts, C-reactive protein
levels, erythrocyte sedimentation rate and serum alkaline
phosphatase levels were within reference range. Urinalysis revealed
no abnormalities. A needle aspiration biopsy was performed and
histological examination of the specimen confirmed the diagnosis of
osteosarcoma. Following two cycles, with an interval of three
weeks, of the chemotherapy protocol with cisplatin (120
mg/m2 skin), adriamycin (90 mg/m2 of skin)
and ifosfamide (10 g/m2 of skin), pain diminished, the
local mass decreased and became rigid, and the range of motion of
the affected wrist returned to normal. The sclerotic changes and a
good margin of the lesion were observed on plain radiographs
(Fig. 2), and MRI revealed marked
shrinkage of the tumor as well as diminished marrow edema.
According to the classification of musculoskeletal neoplasms by
Enneking et al (11), the
tumor was at surgical stage IIB.
The patient underwent en bloc resection of the tumor
and reconstruction with a free fibular shaft to preserve the
radiocarpal joint. A longitudinal dorsal incision at the
radiocarpal joint was used to approach the distal radius and an
elliptical excision was made at the needle biopsy site. The
extensor tendons were removed and preserved, and the flexor tendons
were preserved. A 13×3-cm osteotomy was performed proximal to the
radial styloid followed by en bloc resection of the distal radial
osteosarcoma (Fig. 3). The ulna and
distal radioulnar articulation and radiocarpal joint were
preserved, the free fibular shaft was fixed to the host bone with
two plates (Fig. 4) and the wound
was closed. A long arm cast was applied and the wrist was fixed in
a functional position. The incision healed with no complications.
Postoperative histological examination of the specimens revealed no
tumor cells at the edges of the resected segment or in other
regions of the lesion. Two weeks after surgery, chemotherapy with
the same drug and dose as the preoperative protocol was
administered and completed following six courses as the patient
responded well. Progressive passive exercise was initiated once the
affected distal radius and the wrist had been protected (by the
plaster cast) for 12 weeks. Six months after surgery, radiographs
revealed that the grafted fibular bone had healed well with the
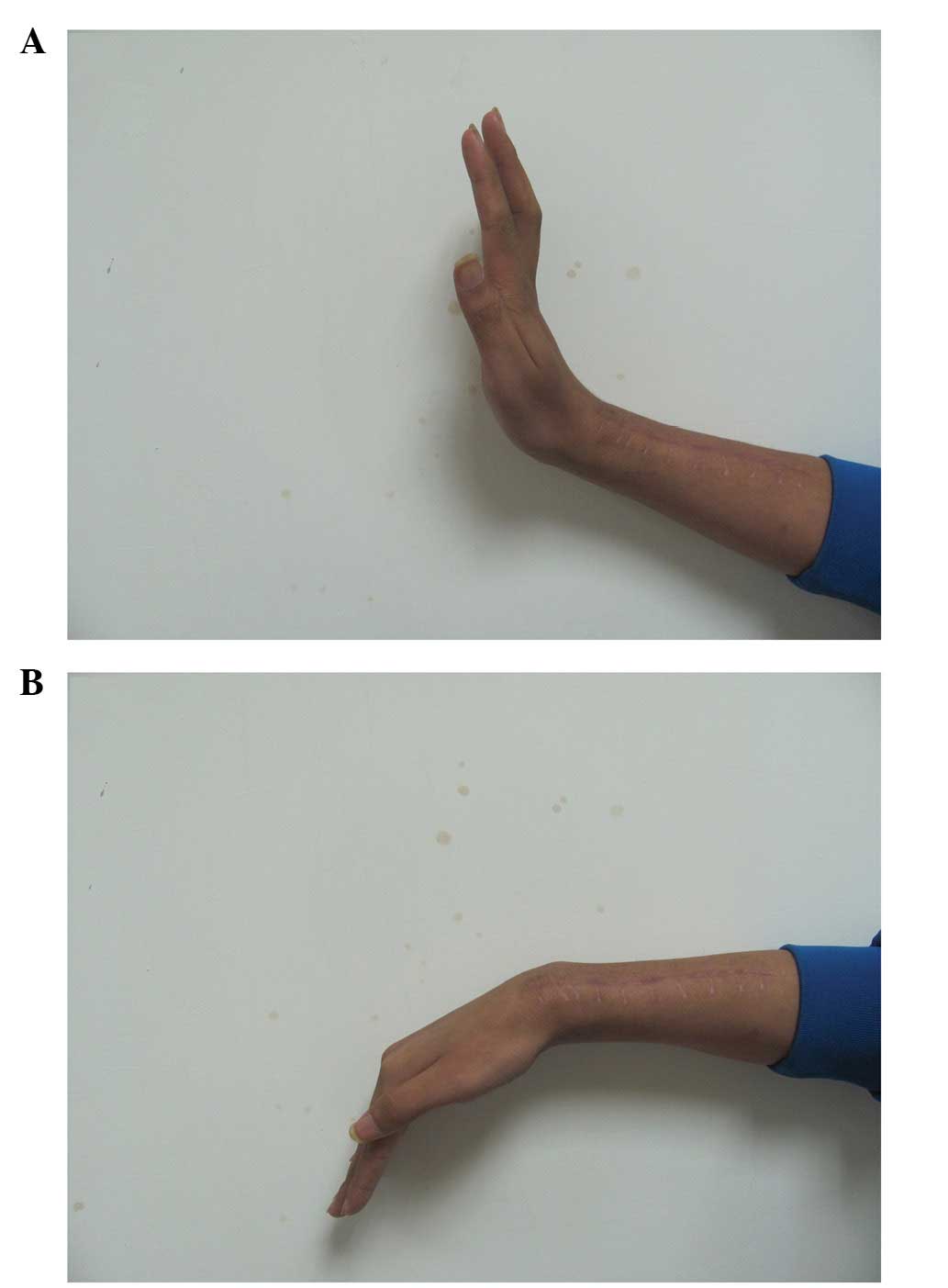
host bone (Fig. 5). Physical
examination showed active dorsiflexion of the affected wrist was to
90° and wrist palmer flexion was to 45° (Fig. 6). One month after surgery, there was
no evidence of wrist deformity, instability, metastasis or local
recurrence. Further follow-up examinations are currently being
conducted. Consent was obtained from both the patient and the
patient’s family.
Discussion
Various reconstructive procedures following the
excision of malignant tumors in long bones have been reported,
including prosthetic replacement, allografts, vascularized fibular
grafts, autoclaved bone grafts and reimplantation of autologous
inactivated bone (4–10). Generally, reconstructive procedures
are selected depending on the site of tumor growth, effectiveness
of preoperative chemotherapy and predicted limb function.
The distal radius is a relatively common skeletal
site for primary bone tumors, however, not for osteosarcomas; it
has been reported that <1% of osteosarcomas arise in the distal
radius (2). Previous studies have
reported en bloc resection of tumors and reconstruction with
prosthesis, and non-vascularized or free proximal fibular grafting
to treat giant cell tumors of the distal radius. Natarajan et
al (9) reported 24 cases of
aggressive benign and malignant tumors of the distal radius treated
by resection and prosthetic replacement. Giant cell tumors were
identified in 16 patients and osteosarcomas in eight. The mean
Musculoskeletal Tumor Society (MSTS) functional score was 75% with
a mean follow-up period of 78 months. The 10-year prosthesis
survival rate was 87.5% and infection was the most common
complication. Saini et al (11) investigated en bloc excision and
reconstruction with ipsilateral non-vascularized fibula to treat
aggressive giant cell tumors of the distal radius. The mean
follow-up period was 5.8 years, the mean time for union at the
fibuloradial junction was 33 weeks (14–69 weeks) and the mean range
of movements were 52° forearm supination, 37° forearm pronation,
42° of wrist palmer flexion and 31° of wrist dorsiflexion. Overall,
the revised MSTS score averaged 91.38% (range, 76.67–93.33%) with
five excellent, four good and three satisfactory results. There
were no cases with graft-related complications or deep infections,
three cases of wrist subluxation, two cases of non-union and one
case of tumor recurrence.
For tumors located in the metaphysis or in contact
with the epiphyseal line, limb salvage surgery, to preserve
epiphysis or the native joint, is required (13). When joint preservation is possible,
the final affected limb functional evaluation shows the most
satisfactory results. However, the joint surface preserving method
may be performed only in a limited number of patients who
adequately respond to chemotherapy and have a tumor in areas
allowing joint surface preservation. This report presents a
17-year-old male patient with osteosarcoma of the distal radius
treated at the General Hospital of Jinan Military Commanding Region
(Jinan, China) with en bloc resection of the tumor and
reconstruction with a free fibular shaft to preserve the
radiocarpal joint. This technique was performed as the patient
exhibited a marked response to preoperative chemotherapy and showed
no evidence of epiphyseal invasion on the MRI scan. No local
recurrence or metastasis was observed 14 months after surgery. In
the final follow-up the movement ranges were wrist palmer flexion
of 45° and wrist dorsiflexion of 90°.
In conclusion, the present report demonstrated that
en bloc resection of a tumor and reconstruction with a free fibular
shaft to preserve the radiocarpal articulation appears to be a
promising procedure to treat osteosarcoma of the distal radius,
with no evidence of epiphyseal invasion following effective
preoperative chemotherapy. This technique preserved the important
structures and joint surfaces to maintain wrist stability and
effective function. However, the long-term outcomes of this
technique require further investigation.
References
|
1
|
Messerschmitt PJ, Garcia RM, Abdul-karim
FW, Greenfield EM and Getty PJ: Osteosarcoma. J Am Acad Orthop
Surg. 17:515–527. 2009.
|
|
2
|
Unni KK: Dahlin’s Bone Tumors: General
Aspects and Data on 11,087 Cases. 5th edition. Lippincott-Raven;
Philadelphia, PA: pp. 143–183. 1996
|
|
3
|
Eckardt JJ and Grogan TJ: Giant cell tumor
of bone. Clin Orthop Relat Res. 204:45–58. 1986.PubMed/NCBI
|
|
4
|
Leung PC and Chan KT: Giant cell tumor of
the distal end of the radius treated by the resection and free
vascularized iliac crest graft. Clin Orthop Relat Res. 202:232–236.
1986.
|
|
5
|
Seradge H: Distal ulnar translocation in
the treatment of giant-cell tumors of the distal end of the radius.
J Bone Joint Surg Am. 64:67–73. 1982.PubMed/NCBI
|
|
6
|
Lackman RD, McDonald DJ, Beckenbaugh RD
and Sim FH: Fibular reconstruction for giant cell tumor of the
distal radius. Clin Orthop Relat Res. 218:232–238. 1987.PubMed/NCBI
|
|
7
|
Pho RW: Malignant giant-cell tumor of the
distal end of the radius treated by a free vascularized fibular
transplant. J Bone Joint Surg Am. 63:877–884. 1981.PubMed/NCBI
|
|
8
|
Kocher MS, Gebhardt MC and Mankin HJ:
Reconstruction of the distal aspect of the radius with use of an
osteoarticular allograft after excision of a skeletal tumor. J Bone
Joint Surg Am. 80:407–419. 1998.PubMed/NCBI
|
|
9
|
Natarajan MV, Bose JC, Viswanath J,
Balasubramanian N and Sameer M: Custom prosthetic replacement for
distal radial tumours. Int Orthop. 33:1081–1084. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yamamoto T, Akisue T, Marui T, Nagira K
and Kurosaka M: Osteosarcoma of distal radius treated by
intraoperative extracorporeal irradiation. J Hand Surg. 27:160–164.
2002. View Article : Google Scholar
|
|
11
|
Saini R, Bali K, Bachhal V, Mootha AK,
Dhillon MS and Gill SS: En bloc excision and autogenous fibular
reconstruction for aggressive giant cell tumor of distal radius: a
report of 12 cases and review of literature. J Orthop Surg Res.
6:142011. View Article : Google Scholar
|
|
12
|
Enneking WF, Spanier SS and Goodman MA: A
system for the surgical staging of musculoskeletal sarcoma. Clin
Orthop. 153:106–120. 1980.
|
|
13
|
Yoshida Y, Osaka S and Tokuhashi Y:
Analysis of limb function after various reconstruction methods
according to tumor location following resection of pediatric
malignant bone tumors. World J Surg Oncol. 8:392010. View Article : Google Scholar
|