Introduction
Sarcomatoid carcinomas are malignant neoplasms that
demonstrate epithelial and mensenchymal differentiation. The tumor
can arise from almost any organ with an epithelial component,
including the breast, larynx, oral cavity, esophagus, female
genital tract and bladder. Sarcomatoid urothelial carcinomas less
commonly arise in urinary tract, and account for ~0.3% of all
urothelial carcinomas (1).
Sarcomatoid carcinoma is a high-grade, biologically aggressive
tumor with a poor prognosis. At the time of diagnosis, nodal and
distant metastases are common and the majority of patients succumb
to the disease within two years (2). Currently, surgical resection remains
the first-line treatment. Sarcomatoid carcinoma of the renal pelvis
is extremely rare (3–9); only ten well-illustrated cases have
been reported since the first true case reported in 1984 (3). The clinical-pathologic characteristics
and potential therapeutic strategies of this tumor are poorly
understood due to the lack of large sample data. In April 2011, the
Urology Department of Beijing Chao-Yang Hospital affiliated with
Capital Medical University (Beijing, China) admitted a patient with
primary sarcomatoid carcinoma of the renal pelvis. In the present
study, the clinicopathological details and the prognosis of this
case are discussed according to the associated literature. Patient
provided written informed consent.
Case report
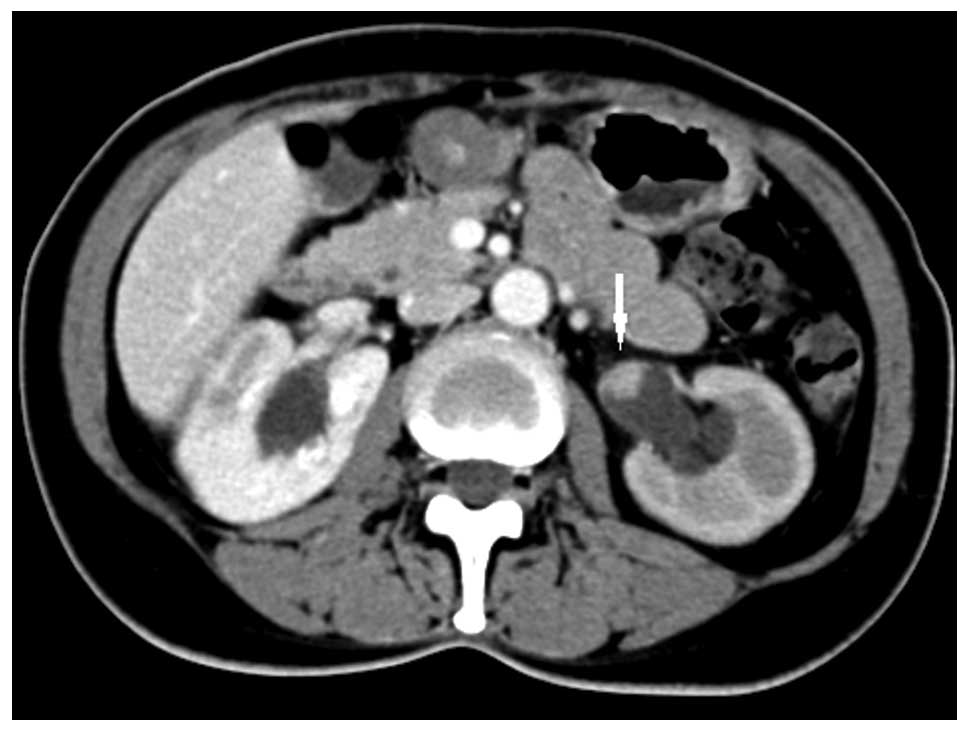
A 49-year-old female patient presented to the
Department of Urology, Beijing Chao-Yang Hospital having
experienced intermittent gross hematuria for the past two weeks.
Physical examination indicated percussion pain in the left kidney
region. An abdominal computed tomography (CT) scan was performed
and revealed a 2 cm in diameter space-occupying lesion in the left
renal pelvis (Fig. 1). Cystoscopic
examination showed intermittent bloody fluid ejection from the left
ureter. Urine cytology did not detect malignant or atypical cells.
No distant metastases were detected after the patient underwent a
whole-body CT scan. The patient’s past medical history disclosed
that a laser endoureterotomy procedure had been applied for
treatment of the right ureteral stricture 17 months previously. The
preoperative diagnosis of the patient was left renal pelvic
carcinoma, and a retroperitoneoscopic nephroureterectomy combined
with a bladder cuff excision was performed.
On gross examination, the tumor in the left renal
pelvis was ~2 cm in diameter, the section was gray-white in color
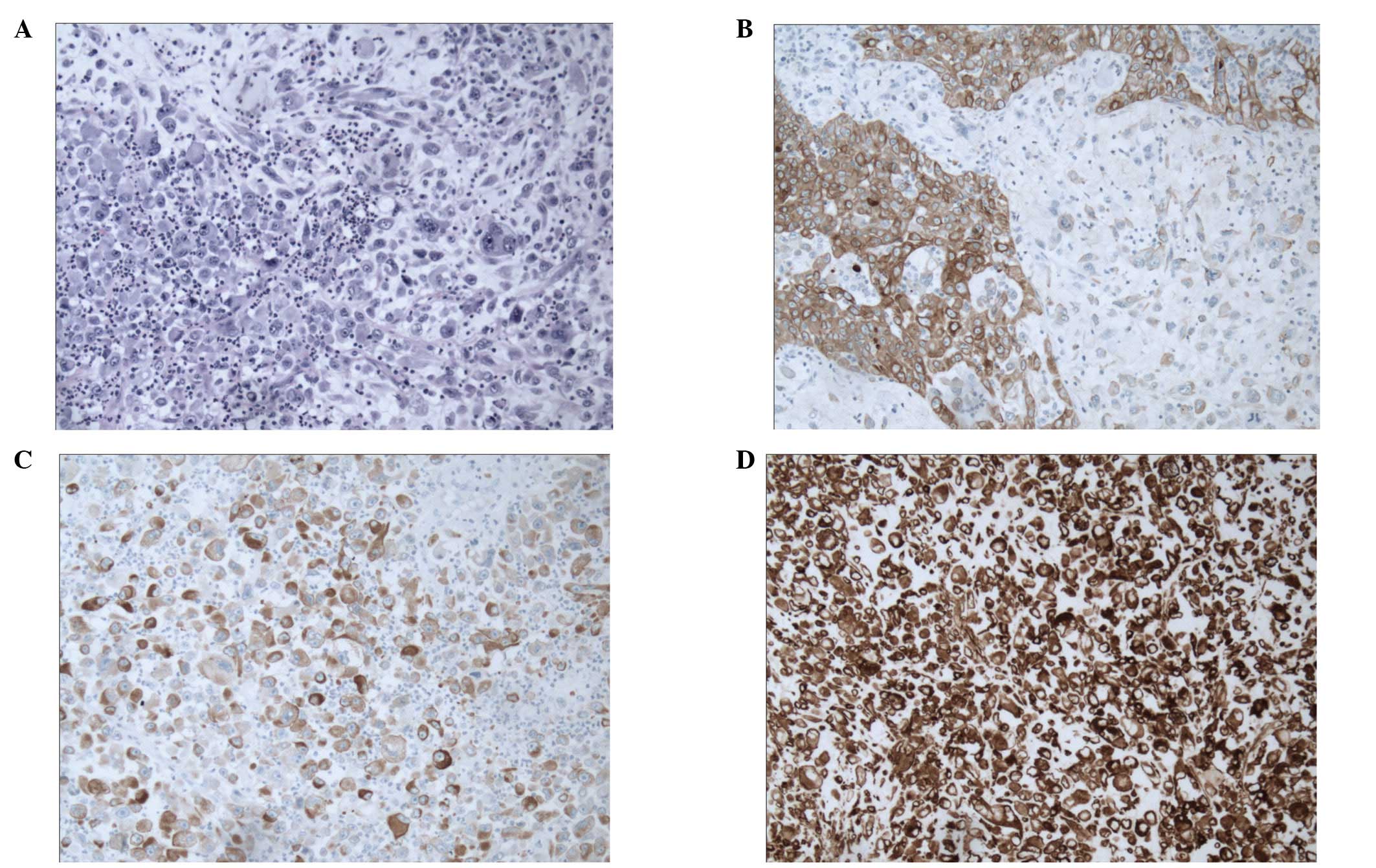
and there was no obvious bleeding or necrosis. Microscopically, the
tumor was composed of high-grade malignant urothelial cells and
sarcomatoid differentiated tumor cells. Numerous pleomorphic, giant
and multinucleated cells with one or more prominent nucleoli were
observed in the sarcomatoid component, and the nuclear chromatin
had a coarse granular shape (Fig.
2A). The tumor was confined to the submucosal area; neither
renal parenchymal invasion nor local lymph node metastasis was
observed. Immunohistochemical studies indicated that the
sarcomatoid components were positive for cytokeratin (Fig. 2B and C) and vimentin (Fig. 2D), and were negative for desmin and
smooth muscle actin. The final pathological diagnosis was
sarcomatoid carcinoma of the renal pelvis (T1N0M0) according to the
Union for International Cancer Control 2009 edition of the Tumor
Node Metastasis Classification (10). The patient did not receive systemic
chemotherapy and radiotherapy due to the organ-confined nature of
the tumor. The postoperative recovery of the patient was good.
Regular clinical follow-up was conducted for 30 months, and the
patient had no evidence of local recurrence or distant
metastasis.
Discussion
The majority of renal pelvic tumors are urothelial
tumors; primary sarcomatoid carcinoma of the renal pelvis is
clinically rare. From the current data, the age of onset for this
disease is usually >50 years and the male-to-female ratio is
2–3:1. Presenting symptoms include gross hematuria, flank pain, an
abdominal mass and hydronephrosis, and are often similar to those
of urothelial tumors. However, sarcomatoid carcinoma is a
higher-grade aggressive epithelial neoplasm compared with
urothelial tumors, which are associated with higher tumor stage,
frequent metastases at presentation and a poor prognosis (2–9).
Commonly, it is almost impossible to establish a correct
histopathological diagnosis preoperatively, due to the lack of
distinctive features. The diagnosis is often made on the basis of
the histological pattern and the immunohistochemical findings,
postoperatively.
The differential diagnosis for this tumor includes a
variety of diseases, such as carcinosarcoma, primary and secondary
spindle cell sarcomas and sarcomatoid renal cell carcinoma.
Sarcomatoid carcinoma is easily confused with carcinosarcomas, due
to the two tumor types having similar histological morphologies.
Immunohistochemical studies are mandatory for the correct
diagnosis. Cytokeratins and other epithelial cell markers are
specific for cells of epithelial origin, and true sarcomatous
components of carcinosarcomas do not stain for epithelial markers.
Immunohistochemical staining may also be of help to distinguish
sarcomatoid carcinomas from mesenchymal malignancy (6–8). It
may be difficult to recognize a sarcomatoid carcinoma as either a
primary renal or urothelial tumor. Identification of improved
differential characteristics of urothelial cell, as well as
demonstration of transitions with in situ urothelial
carcinoma, may aid the diagnosis (11). When the spindle cell component
predominates and there is limited or no morphologic evidence of
epithelial differentiation, the immunohistochemical staining of
PAX8 and the transcription factor GATA3 may be of particular value
(12).
Due to the limited cases reported in the literature,
currently, there is no recommended treatment regimen for
sarcomatoid carcinoma of the upper urinary tract. When the
patient’s condition permits, radical resection is preferred.
However, whether radical surgery can prolong patient survival
awaits further study (13). Other
auxiliary treatments, including systemic chemotherapy and
radiotherapy, are only observed in certain case reports, with
limited clinical experience (9).
More recently, a study showed that the expression of epidermal
growth factor receptor (EGFR) was positive in the majority of
sarcomatoid carcinomas of the upper urinary tract, suggesting that
anti-EGFR molecular targeted therapy may be a promising therapeutic
direction in the future (5).
Sarcomatoid carcinoma of the renal pelvis is a
highly malignant tumor. A poor prognosis has been reported for the
majority of patients and only a few patients have survived for more
than two years following diagnosis (4–8). The
pathological stage may be an important factor for determining
prognosis. Currently, the longest reported survival of an affected
patient is >108 months (14).
The patient in the present study had a tumor that was confined to
the renal pelvis and has had no signs of metastatic spread;
therefore, we predict that the present patient may have a superior
prognosis. Following radical surgery, at the time of writing, the
patient has survived for 30 months without receiving radiotherapy
and chemotherapy. Radiological examination has not yet detected
either local recurrence or distant metastasis, and regular
follow-ups are ongoing.
In conclusion, the clinicopathological features,
treatment and prognosis of sarcomatoid carcinoma of the upper
urinary tract remains poorly understood and additional data are
required to understand this disease.
References
|
1
|
Zhai QJ, Black J, Ayala AG and Ro JY:
Histologic variants of infiltrating urothelial carcinoma. Arch
Pathol Lab Med. 131:1244–1256. 2007.
|
|
2
|
Wang J, Gillaspiea C, Kunadharajua R,
Talmon GA and Enke C: Sarcomatoid urothelial carcinoma: A single
cancer center experience. World J Oncol. 2:175–180. 2011.
|
|
3
|
Piscioli F, Bondi A, Scappini P and
Luciani L: ‘True’ sarcomatoid carcinoma of the renal pelvis. First
case report with immunocytochemical study. Eur Urol. 10:350–355.
1984.
|
|
4
|
Lopez-Beltran A, Escudero AL, Cavazzana
AO, Spagnoli LG and Vicioso-Recio L: Sarcomatoid transitional cell
carcinoma of the renal pelvis. A report of five cases with
clinical, pathological, immunohistochemical and DNA ploidy
analysis. Pathol Res Pract. 192:1218–1224. 1996.
|
|
5
|
Wang X, MacLennan GT, Zhang S, Montironi
R, Lopez-Beltran A, Tan PH, Foster S, Baldridge LA and Cheng L:
Sarcomatoid carcinoma of the upper urinary tract: clinical outcome
and molecular characterization. Hum Pathol. 40:211–217. 2009.
|
|
6
|
Hisataki T, Takahashi A, Taguchi K,
Shimizu T, Suzuki K, Takatsuka K and Iwaki H: Sarcomatoid
transitional cell carcinoma originating from a duplicated renal
pelvis. Int J Urol. 8:704–706. 2001.
|
|
7
|
Canacci AM and Maclennan GT: Sarcomatoid
urothelial carcinoma of the renal pelvis. J Urol. 175:19062006.
|
|
8
|
Thiel DD, Igel TC and Wu KJ: Sarcomatoid
carcinoma of transitional cell origin confined to renal pelvis.
Urology. 67:622.e9–e11. 2006.
|
|
9
|
Acikalin MF, Kabukcuoglu S and Can C:
Sarcomatoid carcinoma of the renal pelvis with giant cell
tumor-like features: case report with immunohistochemical findings.
Int J Urol. 12:199–203. 2005.
|
|
10
|
Sobin L, Gospodarowicz M and Wittekind C:
Urological tumors Renal Pelvis and Ureter. TNM Classification of
Malignant Tumors. 7th revised edition. Wiley-Blackwell; Hoboken,
NJ: pp. 258–261. 2009
|
|
11
|
Amin MB: Histological variants of
urothelial carcinoma: diagnostic, therapeutic and prognostic
implications. Mod Pathol. 22(Suppl 2): S96–S118. 2009.
|
|
12
|
Chang A, Brimo F, Montgomery EA and
Epstein JI: Use of PAX8 and GATA3 in diagnosing sarcomatoid renal
cell carcinoma and sarcomatoid urothelial carcinoma. Human
Pathology. 44:1563–1568. 2013.
|
|
13
|
Wang J, Wang FW, Lagrange CA, Hemstreet GP
III and Kessinger A: Clinical features of sarcomatoid carcinoma
(carcinosarcoma) of the urinary bladder: analysis of 221 cases.
Sarcoma. 2010:4547922010.
|
|
14
|
Perez-Montiel D, Wakely PE, Hes O, Michal
M and Suster S: High-grade urothelial carcinoma of the renal
pelvis: clinicopathologic study of 108 cases with emphasis on
unusual morphologic variants. Mod Pathol. 19:494–503. 2006.
|