Introduction
Benign osteoblastoma is an osteoid and bone-forming
benign tumor that rarely occurs in the facial bones and was first
described by Jaffe and Mayer in 1932 (1). The current term, benign osteoblastoma
was proposed by Jaffe and Lichtenstein in two different reports in
1956 (2,3). Benign osteoblastoma accounts for 1% of
all bone tumors and 3% of all benign bone tumors, worldwide
(4). Osteoblastoma most frequently
occurs in young adults and primarily involves the vertebral column,
long bones, small bones of the extremities and facial bones,
including the jaw (4–6). The first case of osteoblastoma
described in the jaw bones was reported by Borello and Sedano in
1967 (7). Subsequent data has
revealed that the mandibular bones of the jaw are more commonly
affected by osteoblastoma than the maxillary bones, with the
majority of osteoblastoma affecting the mandibular posterior region
(8). Osteoblastoma can be
classified into two major clinicopathological forms as follows: The
benign form, which has a slow growth rate, a well-defined sclerotic
margin and is moderately well vascularized with a mild inflammatory
response; and the aggressive form, which exhibits locally
aggressive behavior with a tendency to recur, often complicating
its differentiation from low-grade osteosarcoma (9). Osteoblastoma may have a different
clinical prognosis depending on its propensity to recur, its
locally aggressive behavior and, in rare cases, whether malignant
transformation takes place (5).
Morphologically, osteoblastoma is identified by osteoid and woven
bone deposition and enriched osteoblasts, which are frequently in
close association with newly formed bone (4). Therefore, evaluation of clinical,
histological and radiological findings is essential for the
definitive diagnosis and effective treatment of osteoblastoma
(6).
The current study reports a rare case of benign
osteoblastoma in a 12-year-old female patient, involving the right
mandible, which was treated by surgical excision. Written informed
consent was obtained from the patient’s family.
Case report
A 12-year-old female patient, reported to the
Department of Oncology, Tbilisi State Medical University (Tbilisi,
Georgia) in July 2013 with the complaint of intraoral swelling and
pain on the right side of the lower jaw. A clinical examination
revealed the presence of a firm, palpable tumor mass, the majority
of which was situated within the body of the right mandible.
Radiological imaging revealed that the lesion consisted of regular
contours and exhibited a marginal amount of calcification (Fig. 1). Due to consideration of the
patient history, clinical examination and the nature of the growth,
a clinical diagnosis of a benign tumor of the bone was determined.
Thus, the patient was subjected to a right lower jaw partial
resection and the lesion was completely surgically removed
(Fig. 2A–C). The jaw defect was
reconstructed using titanium implants and an autologous VI rib
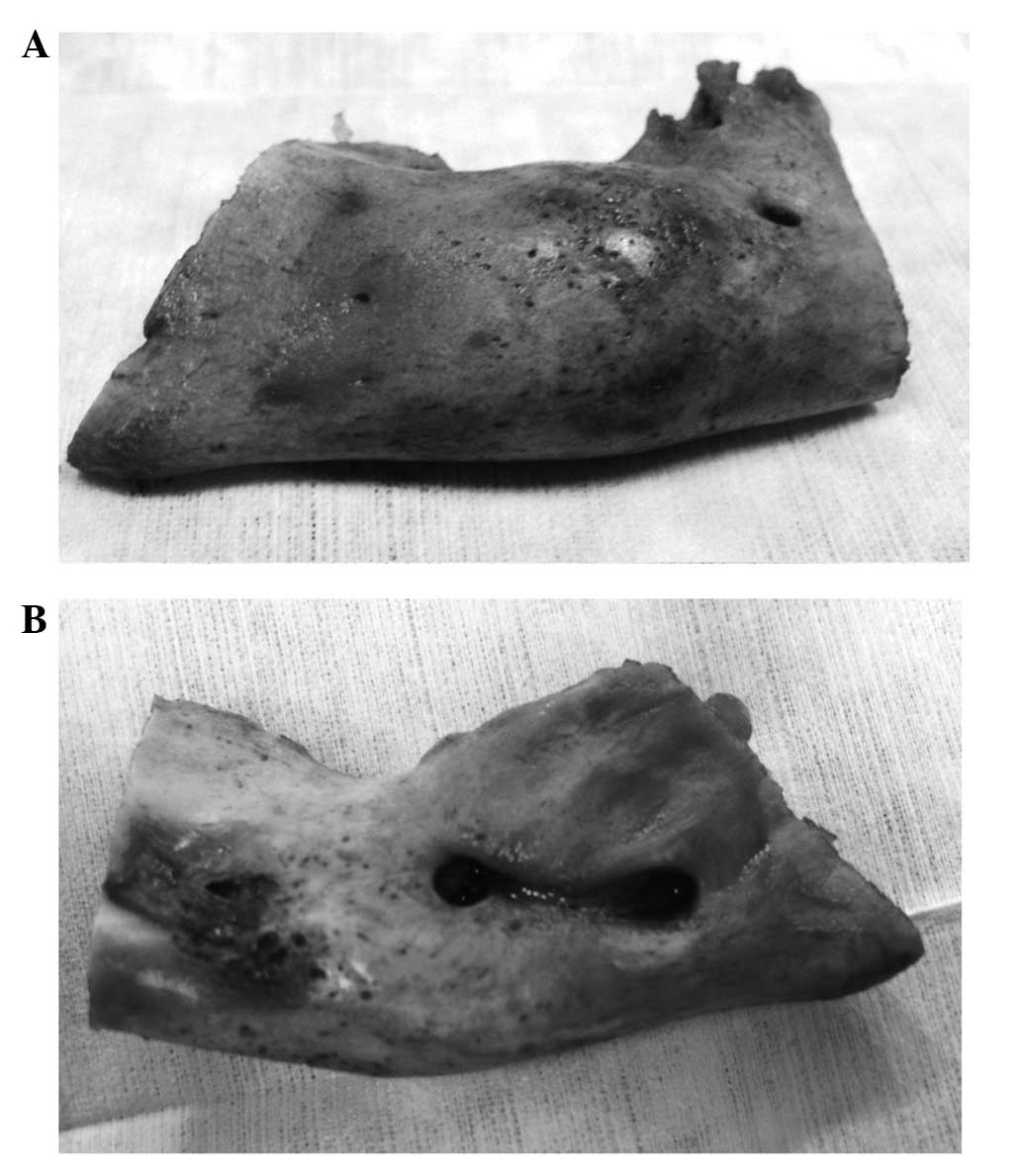
graft (Fig. 3). Upon macroscopic
examination, the excised tumor was observed to be an oval mass
measuring 3.5 cm at its greatest diameter, with a brown, nodular
outer surface (Fig. 4) and
predominantly red cut surface. The tumor had a rough consistency,
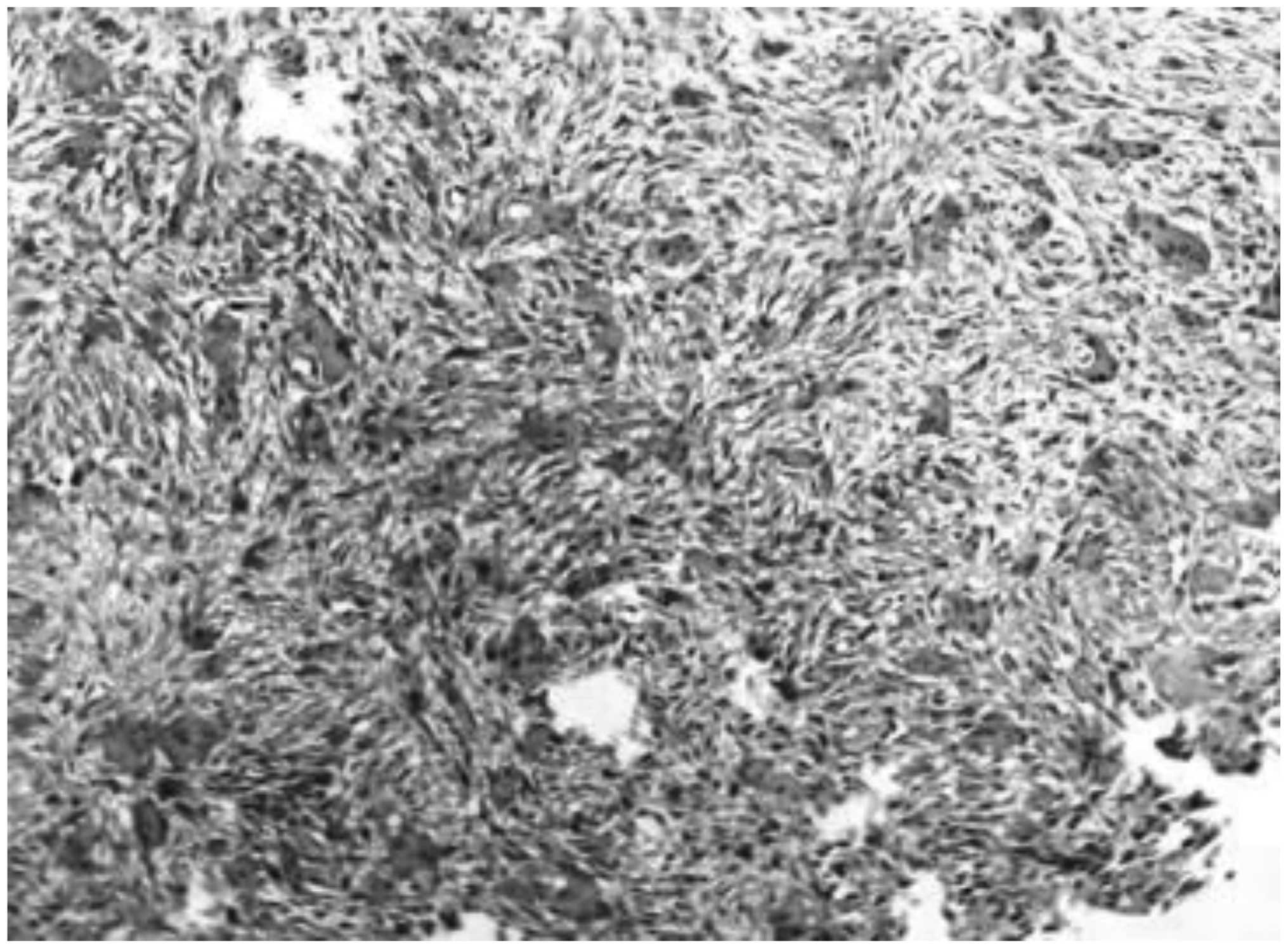
with soft and firm areas of bone tissue. The specimen was sent for
histopathological analysis, which revealed vascularized fibrous
connective tissue with bony trabeculae, which was lined by numerous
osteoblasts and scattered osteoclasts (Fig. 5). Based on the histomorphologic
characteristics of the tumor, clinical observation and radiological
evidence, the diagnosis of a benign osteoblastoma of the mandible
was established. During surgery, it was noted that the lesion had
not extended to the resection margin, indicating the complete
removal of the tumor. This is supported by continued patient
follow-up, with the patient feeling generally healthy and
radiograph images indicating no signs of recurrence or complication
five months subsequent to the surgery (Fig. 6).
Discussion
Osteoblastoma is an osteoid and bone-forming benign
tumor of the bone. Jaffe and Lichtenstein (2,3) were
the first to propose that osteoblastoma is a true neoplasm of
osteoblastic origin, however, other studies hypothesized that
osteoblastoma arise as a result of trauma or inflammation (10). The age range of patients that
present with the disease is 5–78 years, although it typically
occurs in the second and third decades of life (11,12).
Furthermore, the incidence rate is higher in males than in females,
with a ratio of 3-2:1 (5,11,13).
Osteoblastoma can arise in any bone in the body, however, it rarely
involves the maxilla and mandible. The mandible is affected more
commonly than the maxilla, with the majority of lesions occurring
in the mandible body (14). In
addition to being characterized as benign or aggressive,
osteoblastoma growth can be classified as cortical, medullary, or
periosteal. Whilst cortical growth commonly occurs in extragnathic
craniofacial bones, it does not occur in the jaw (9). Clinically, osteoblastoma may be
associated with painful or painless characteristics.
Due to the rarity and non-specific manifestation of
osteoblastoma, diagnosis can be challenging. Radiological imaging
may vary depending on the size of the tumor and the intensity of
the calcification, although osteoblastomas commonly form
well-circumscribed, fully radiolucent or calcified lesions ≤12 cm
in diameter (15). Osteoblastoma
must be differentiated from other bone-producing lesions, such as
osteoid osteoma, osteosarcoma, cementoblastoma and ossifying
fibroma as this may lead to improved treatment and prognosis
(16). However, the differential
diagnosis may be complicated due to the tumor’s rarity, ambiguous
clinicoradiological presentation, and histopathologic features,
which occasionally resemble osteosarcoma in particular.
Histological analysis of osteosarcoma reveals pleomorphic
osteoblasts and osteocytes, and malignant stromal cells. In benign
osteoblastoma, stromal connective tissue cells do not demonstrate
sarcomatous growth, and mitoses and sarcoma giant cells are absent.
Furthermore, the cells that are enmeshed in the osteoid matrix are
relatively small and homogeneous (8,17).
Conventional osteoblastomas are biologically benign
with limited growth potential, typically ≤4 cm in diameter.
However, a small subgroup of osteoblastomas possess a locally
aggressive growth pattern and are usually >4 cm in diameter.
These tumors are distinct from conventional osteoblastoma and are
classified as osteoblastoma-like osteosarcomas, malignant
osteoblastomas or aggressive osteoblastomas (18). It is hypothesized that, when
compared with benign osteoblastoma, aggressive osteoblastomas occur
in older patients and demonstrate clinically aggressive behavior.
Aggressive osteoblastomas invade adjacent tissues and recur in
10–21% of patients, however, do not metastasize. Certain authors
advocate that lesions described as aggressive osteoblastoma are
actually well-differentiated osteosarcomas resembling
osteoblastomas. Therefore, the diagnostic evaluation is based on
the histologic features and the clinical behavior of the lesion
(11).
Additionally, in view of the supposed benign nature
of osteoblastoma tumors, surgical excision is the treatment of
choice. Since recurrence is a rare event and usually attributable
to an incomplete excision, the overall prognosis for osteoblastoma
patients is considered to be good (4).
In conclusion, in the case of the present study, the
clinical presentation of the disease was rare, however, the
histopathologic findings were in accordance with those reported in
previous literature. Correct diagnosis and complete surgical
excision of the tumor is essential to minimize the risk of
recurrence and the potential malignization of a benign
osteoblastoma.
References
|
1
|
Jaffe HL and Mayer L: An osteoblastic
osteoid tissue-forming tumor of a metacarpal bone. Arch Surg.
24:550–564. 1932.
|
|
2
|
Jaffe HL: Benign osteoblastoma. Bull Hosp
Joint Dis. 17:141–151. 1956.
|
|
3
|
Lichtenstein L: Benign osteoblastoma; a
category of osteoid-and bone-forming tumors other than classical
osteoid osteoma, which may be mistaken for giant-cell tumor or
osteogenic sarcoma. Cancer. 9:1044–1052. 1956.
|
|
4
|
Madalli V, Basavaraddi SM, Naikmasur V, et
al: Osteoblastoma of Mandible: A Rare Clinical Presentation. Head
Neck. 27:616–621. 2005.
|
|
5
|
Alvares Capelozza AL, Gião Dezotti MS,
Casati Alvares L, Negrão Fleury R and Sant’Ana E: Osteoblastoma of
the mandible: systematic review of the literature and report of a
case. Dentomaxillofac Radiol. 34:1–8. 2005.
|
|
6
|
Bokhari K, Hameed MS, Ajmal M and Togoo
RA: Benign osteoblastoma involving maxilla: a case report and
review of the literature. Case Rep Dent. 2012:3512412012.
|
|
7
|
Borello ED and Sedano HO: Giant osteoid
osteoma of the maxilla. Report of a case. Oral Surg Oral Med Oral
Pathol. 23:563–566. 1967.
|
|
8
|
Madalli V, Basavaraddi SM, Naikmasur V,
Burde K and Horatti P: Osteoblastoma of mandible: A rare clinical
presentation. Iran J Pathol. 9:79–80. 2014.
|
|
9
|
Manjunatha BS, Sunit P, Amit M and Sanjiv
S: Osteoblastoma of the jaws: report of a case and review of
literature. Clin Pract. 1:e1182011.
|
|
10
|
Miller AS, Rambo HM, Bowser MW and Gross
M: Benign osteoblastoma of the jaws: report of three cases. J Oral
Surg. 38:694–697. 1980.
|
|
11
|
Ivkovic T, Vuèkovic N, Gajanin R, et al:
Benign osteoblastoma of the mandible. Arch Oncol. 8:73–74.
2000.
|
|
12
|
Utumi E, Sales M, Yamamoto F and
Cavalcanti M: Difficulty in diagnosing atypical osteoblastoma of
the face: Case report. Intl Arch Otorhinolaryngol. 14:131–135.
2010.
|
|
13
|
Lichtenstein L and Sawyer WR: Benign
osteoblastoma. Further observations and report of twenty additional
cases. J Bone Joint Surg Am. 46:755–765. 1964.
|
|
14
|
Weinberg S, Katsikeris N and Pharoah M:
Osteoblastoma of the mandibular condyle: review of the literature
and report of a case. J Oral Maxillofac Surg. 45:350–355. 1987.
|
|
15
|
Alawi F: Benign fibro-osseous diseases of
the maxillofacial bones. A review and differential diagnosis. Am J
Clin Pathol. 118:S50–S70. 2002.
|
|
16
|
Peters TE, Oliver DR and McDonald JS:
Benign osteoblastoma of the mandible: report of a case. J Oral
Maxillofac Surg. 53:1347–1349. 1995.
|
|
17
|
Haug RH, Hauer C, De Camillo AJ and
Araneta M: Benign osteoblastoma of the mandible: report of a case.
J Oral Maxillofac Surg. 48:743–748. 1990.
|
|
18
|
Angiero F, Mellone P, Baldi A and Stefani
M: Osteoblastoma of the jaw: report of two cases and review of the
literature. In Vivo. 20:665–670. 2006.
|