Introduction
The function of vitamin D {25-hydroxyvitamin D
[25(OH)D]} in regulating calcium homeostasis and bone metabolism
was first identified in 1930 and has since become well established
(1). Over recent decades, increasing
data has implicated vitamin D to be a type of endocrine substance
that serves an important role in many biological activities,
including the immune response and cell differentiation,
proliferation and apoptosis (2).
Abnormal vitamin D level may be a risk factor for a range of acute
and chronic illnesses, including cancer, diabetes and
cardiovascular diseases (3,4).
Previous epidemiological studies have indicated an
association between vitamin D deficiency and risk of type 2
diabetes mellitus (T2DM) (5,6). Animal studies have also demonstrated
that vitamin D may serve a role in insulin secretion (2,7). These
findings suggested that vitamin D deficiency probably has a causal
relationship with T2DM. Therefore, randomized clinical trials
(RCTs) were needed to observe the effect of vitamin D
supplementation on prevention of T2DM, decreasing fasting plasma
glucose (FPG) and/or improvement of insulin resistance, to confirm
the association between vitamin D and T2DM.
Numerous RCTs of vitamin D supplementation have been
performed in the past decade. The results regarding control of FPG
level, improving insulin resistance and preventing T2DM were
inconsistent. A number of RCTs suggested that supplementation of
vitamin D could improve insulin resistance and FPG (8–11).
However, certain studies obtained contrary results (12) or identified no beneficial effect
(13–16). Dutta et al revealed that
vitamin D supplementation could significantly lower the progression
of diabetes (17); while reports from
others indicated that supplementation with vitamin D had no effect
on T2DM prevention (13,18,19). Thus,
a meta-analysis is required to validate the effect of vitamin D
supplementation on diabetes development.
A number of meta-analyses on the effect of vitamin D
supplementation on FPG control have been conducted. These mainly
focused on glycemic control in T2DM patients (20,21),
glucose metabolism in gestational diabetes patients (22), and glycemic control and insulin
resistance in non-T2DM individuals (23). However, these analyses did not
consider the preventative effect of vitamin D on T2DM. Furthermore,
the impacts from individual variation and intervention strategy
were not considered. Previous studies have suggested that there is
individual variation for vitamin D sensitivity, with different
individuals exhibiting different responses to the same vitamin D
supplementation (24,25). Considering the aforementioned reasons,
the present aim was to conduct a systematic update meta-analysis,
in order to obtain an objective and more definitive conclusion on
the effect of vitamin D supplementation on FPG, insulin resistance
and prevention of T2DM for non-T2DM people. This should provide
insight on the relationship between vitamin D deficiency and risk
of T2DM, as well as how vitamin D serves a role in T2DM
development.
Materials and methods
Literature retrieval
RCT literature on the effects of vitamin D
supplementation on FPG, insulin resistance and risk of T2DM in
non-diabetic individuals published from January 2000 to February
2017 was retrieved from PubMed (https://www.ncbi.nlm.nih.gov/pubmed/) and two Chinese
academic databases, CNKI (http://www.cnki.net) and Wanfang (http://www.wanfangdata.com.cn/index.html). The
language of the literature was restricted to English and Chinese.
The key words used to search relevant articles were ‘vitamin D’,
‘vitamin D2’, ‘vitamin D3’, ‘ergocalciferol’,
‘cholecalciferol’, ‘calciferol’, ‘vitamin D analogs’, ‘25-(OH)D’,
‘1,25-(OH)2D’, ‘diabetes mellitus’, ‘type 2 diabetes
mellitus’, ‘hyperglycemia’, ‘impaired glucose tolerance’, ‘insulin
resistance’ and ‘insulin sensitivity’.
Literature screening
The inclusion criteria were as follows: i) Study
subjects were non-diabetic individuals, including those with normal
blood glucose (<6.1 mmol/l) and prediabetes (6.1–7.0 mmol/l)
(26); ii) RCTs that focused on the
influence of vitamin D deficiency on the indices related to blood
glucose through vitamin D supplementation; iii) the intervention
group vs. control group should be vitamin D vs. placebo, vitamin D
+ calcium vs. placebo + calcium or vitamin D + calcium vs. placebo;
and iv) study outcome indicators included at least one of the
following: Incidence rate or the number of participants who
developed T2D, FPG measurements and/or homeostasis model insulin
resistance index (HOMA-IR) data, with the value for FPG and HOMA-IR
prior to and following supplementation expressed as the mean ±
standard deviation (SD).
The exclusion criteria were as follows: i) Animal
experiments; ii) non-RCTs; iii) incomplete information on the
outcome indicators, such as only reporting the mean and not
providing SD; iv) outcome variables were expressed as the median
(four interquartile range) or interquartile range, and outcome
measurements that did not meet the inclusion requirements; v)
articles that were reviews, systematic reviews or meta-analyses;
and vi) the subjects were children, pregnant women or lactating
women, or suffering from any diseases.
Data extraction
Literature screening and data extraction were
performed by two reviewers. The quality and bias risk of the
included studies were evaluated. Disputes or differences in the
process of document selection or data extraction were settled by a
third reviewer. The extracted data included: i) Title, first author
and year of publication; ii) geographic location, sample size,
blood glucose status, age, body mass index (BMI), baseline 25(OH)D
concentration, female proportion and follow-up time; iii) dose and
methods of vitamin D supplementation; iv) the related data of
outcome variables; and v) the information needed for bias risk
assessment and Jadad scoring.
Bias risk and quality evaluation of
included studies
The bias risk assessment tool recommended by the
Cochrane Handbook for Systematic Reviews of Interventions, version
5.1.0 (27) and the Jadad scoring
scale (28) were used to assess the
methodological quality of the included RCTs. The evaluation
criteria in the bias risk assessment include: i) Randomization
methods; ii) allocation concealment; iii) whether the researchers,
participants and observers remained blinded; iv) the integrity of
data; v) whether there was selective reporting bias; and vi) other
sources of bias. In the Jadad scoring scale, there are three levels
for the randomization method, allocation concealment and blinding
method, namely appropriate (2 points), unclear (1 point) and
inappropriate (0 point). In addition, the scale accounts for when
reasons for withdrawal of subjects are reported (1 point) or
unspecified (0 points). Studies that scored ≤4 points were
considered to be of high quality.
Data synthesis
When the literature provided the mean ± SD of FPG
and/or HOMA-IR at baseline and at the end of the study, mean ± SD
changes in corresponding outcome variable were converted by the
following formula: MDΔ = Mean1 -
Mean0; and SDΔ = (SD12
+ SD02 -
2×0.5×SD1xSD0)1/2, where
Mean1, mean of outcome variable after intervention;
SD0, SD of outcome variable after intervention;
Mean0, mean of outcome variable at baseline;
SD0, SD of outcome variable at baseline (29). The standard error with 95% confidence
intervals (95% CIs) of the change in the corresponding outcome
variable was converted by the following formula: SEΔ =
(ULΔ - LLΔ)/3.92, where SEΔ, the
standard error of the change in the corresponding outcome variable;
ULΔ, the upper limit of the 95% CI; LLΔ, the
lower limit of the 95% CI. The results expressed as standard error
were then transformed into SD by the following formula: SD = √n ×
σ, where n, sample size; σ, standard error. The unified units of
FPG, baseline 25(OH)D concentration and vitamin D intervention dose
were mg/dl, ng/ml and IU, respectively (with 1 mg/dl=18 mmol/l, 1
ng/ml=2.5 nmol/l and 1 µg=40 IU). The association between vitamin D
supplementation and T2DM was expressed by relative risk (RR =
incidence of supplementation group/incidence of control group), and
the effect on FPG was represented by mean difference (MD = glucose
level pre-supplementation - glucose level following
supplementation). The effect on insulin resistance (HOMA-IR) was
represented by standardized mean difference (SMD = difference of
HOMA-IR/SD of HOMA-IR) as the measurement method, or when units
were inconsistent. Subgroup analysis was performed in view of the
differences of research aims and interventions among studies.
Subgroups were stratified on the following bases: i) Glucose status
of subjects: Normal glucose tolerance or prediabetes; ii) the age
of subjects: Age <45 years, 45≤ age <60 years, age ≥60 years;
iii) the body weight index of subjects: Normal (BMI <25),
overweight (25≤ BMI <30) and obese (BMI ≥30) (30); iv) the baseline 25(OH)D concentration
of subjects: Deficient [25(OH)D <20 ng/ml], insufficient [20≤
25(OH)D <30 ng/ml] and sufficient [25(OH)D ≥30 ng/ml] (31); v) the follow-up time: <12 months or
≥12 months; vi) vitamin D intervention dose: ≤2,000 IU/day or
>2,000 IU/day; vii) intervention with Ca or not; and viii) Jadad
score: <4 points or ≥4 points.
Statistical analysis
Stata software (version 12.0; StataCorp LP, College
Station, TX, USA) was used to analyze the population data. The
statistical heterogeneity was estimated by Q test (α=0.1) and from
the inhibition coefficient (I2). If there was no
statistical heterogeneity among studies, the fixed effect model was
used for analysis; otherwise the random effect model was applied to
analyze data on the premise of excluding clinical heterogeneity and
methodological heterogeneity if statistical heterogeneity existed
(27). In addition, the source of
heterogeneity was investigated by subgroup analysis. Publication
bias was assessed by using funnel plots, Egger's test and Begg's
test (32). P<0.05 was considered
to indicate statistical significance.
Results
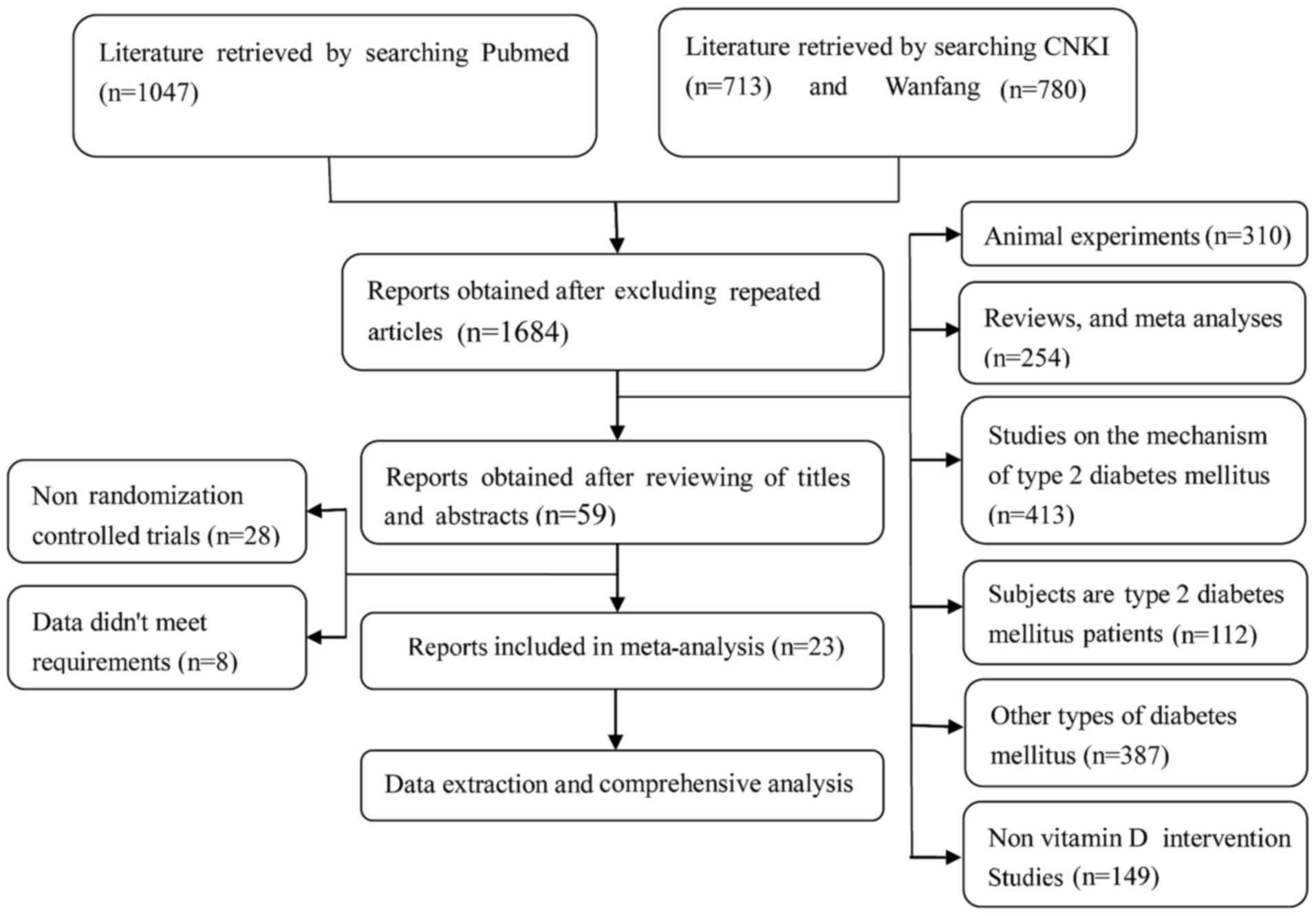
Literature retrieval
A total of 1,047 articles in English and 1,493
articles in Chinese were retrieved in accordance with the search
words established in advance. Of these, 47 English articles and 12
Chinese articles were retained following the exclusion of repeated
literature and after reading the abstracts. Finally, a total of 23
articles (8–19,33–43),
including 22 English articles and 1 Chinese publication, were
included for meta-analysis after reading the full text according to
the inclusion and exclusion criteria. The full literature retrieval
process is outlined in Fig. 1.
Characteristics and bias risk
assessment of included studies
A total of 28 RCTs from 23 studies were included in
the current meta-analysis. Among these studies, the Jadad scores of
16 studies (containing 21 RCTs) were ≥4 points. The basic
characteristics of the studies are summarized in Table I. A total of 17 studies (containing 20
RCTs) reported the methods of generating random allocation
sequences, including computer-generated random number sequences and
stratified randomization sets. A total of 11 studies (containing 13
RCTs) reported the methods of concealment allocation, including
central or pharmacy control, distribution, opaque containers or
sealed envelopes. A double-blinded method was adopted in 20 studies
(containing 25 RCTs). A total of 19 studies (containing 24 RCTs)
described the number and causes of those lost to follow-up. A total
of 5 studies (containing 7 RCTs) were analyzed using the
intention-to-treat (ITT) method (Table
I).
 | Table I.Basic characteristics and bias risk
assessment of included studies. |
Table I.
Basic characteristics and bias risk
assessment of included studies.
|
|
|
| Blinding |
|
|
|
|---|
|
|
|
|
|
|
|
|
|---|
| Study/(Refs.),
year | Randomization
method | Concealment
allocation | Investigator and
subject | Observer | Integrity of
data | Selective
reporting | Other sources of
bias |
|---|
| Major et al,
2007 (40) | Unclear | Unclear | Yes | Unclear | Drop-out | No | Unclear |
| Pittas et
al, 2007 (10) | Computer-generated
random number sequencev | Unclear | Yes | Yes | Drop-out | No | Unclear |
| de Boer et
al, 2008 (18) | Stratified-block
randomization | Unclear | Yes | Unclear | Unclear | No | Unclear |
| Zittermann et
al, 2009 (42) | Computer-generated
random number sequence | Unclear | Yes | Unclear | Drop-out or loss to
follow-up | No | Unclear |
| Nagpal et
al, 2009 (9) | Computer-generated
random number sequence | Opaque
containers | Yes | Yes | Drop-out, ITT | No | Unclear |
| Jorde et al,
2010 (15) | Stratified-block
randomization | Central
randomization | Yes | Yes | Drop-out or loss to
follow-up | No | Unclear |
| Mitri et al,
2011 (36) | Computer-generated
random number sequence | Unclear | Yes | Yes | Drop-out, ITT | No | Unclear |
| Grimnes et
al, 2011 (14) | Block
randomization | Sealed
envelopes | Yes | Yes | Drop-out or loss to
follow-up | No | Unclear |
| Wood et al,
2012 (41) | Unclear | Opaque
containers | Yes | Unclear | Drop-out | No | Unclear |
| Harris et
al, 2012 (39) | Stratified-block
randomization | Unclear | Yes | Unclear | Drop-out or loss to
follow-up | No | Unclear |
| Iraj et al,
2012 (12) | Unclear | None | No | No | Complete | No | Unclear |
| Salehpour et
al, 2013 (33) | Unclear | Unclear | Yes | Yes | Loss to
follow-up | No | Unclear |
| Belenchia et
al, 2013 (8) | Stratified-block
randomization | Pharmacy
controlled | Yes | Unclear | Loss to
follow-up | No | Unclear |
| Davidson et
al, 2013 (13) | Computer-generated
random number sequence | Pharmacy
controlled | Yes | Unclear | Drop-out | No | Unclear |
| Dutta et al,
2014 (17) | Stratified-block
randomization | None | No | No | Complete | No | Unclear |
| Sollid et
al, 2014 (38) | Computer-generated
random number sequence | Pharmacy
controlled | Yes | Yes | Drop-out | No | Unclear |
| Oosterwerff et
al, 2014 (34) | Stratified-block
randomization | Pharmacy
controlled | Yes | Unclear | Drop-out or lossto
follow-up, ITT | No | Unclear |
| Tuomainen et
al, 2015 (37) | Unclear | Opaque
containers | Yes | Unclear | Drop-out | No | Unclear |
| Kuchay et
al, 2015 (11) | Computer-generated
random number sequence | None | No | No | Drop-out | No | Unclear |
| Qi et al,
2016 (35) | Unclear | Unclear | Yes | Unclear | Complete | No | Unclear |
| Sun et al,
2016 (43) | Stratified-block
randomization | Unclear | Yes | Yes | Drop-out | No | Unclear |
| Jorde et al,
2016 (19) | Computer-generated
random number sequence | Pharmacy
controlled | Yes | Yes | Drop-out, ITT | No | Unclear |
| Moreira-Lucas et
al, 2017 (16) | Block
randomization | Sealed
envelopes | Yes | Yes | Drop-out or lossto
follow-up, ITT | No | Unclear |
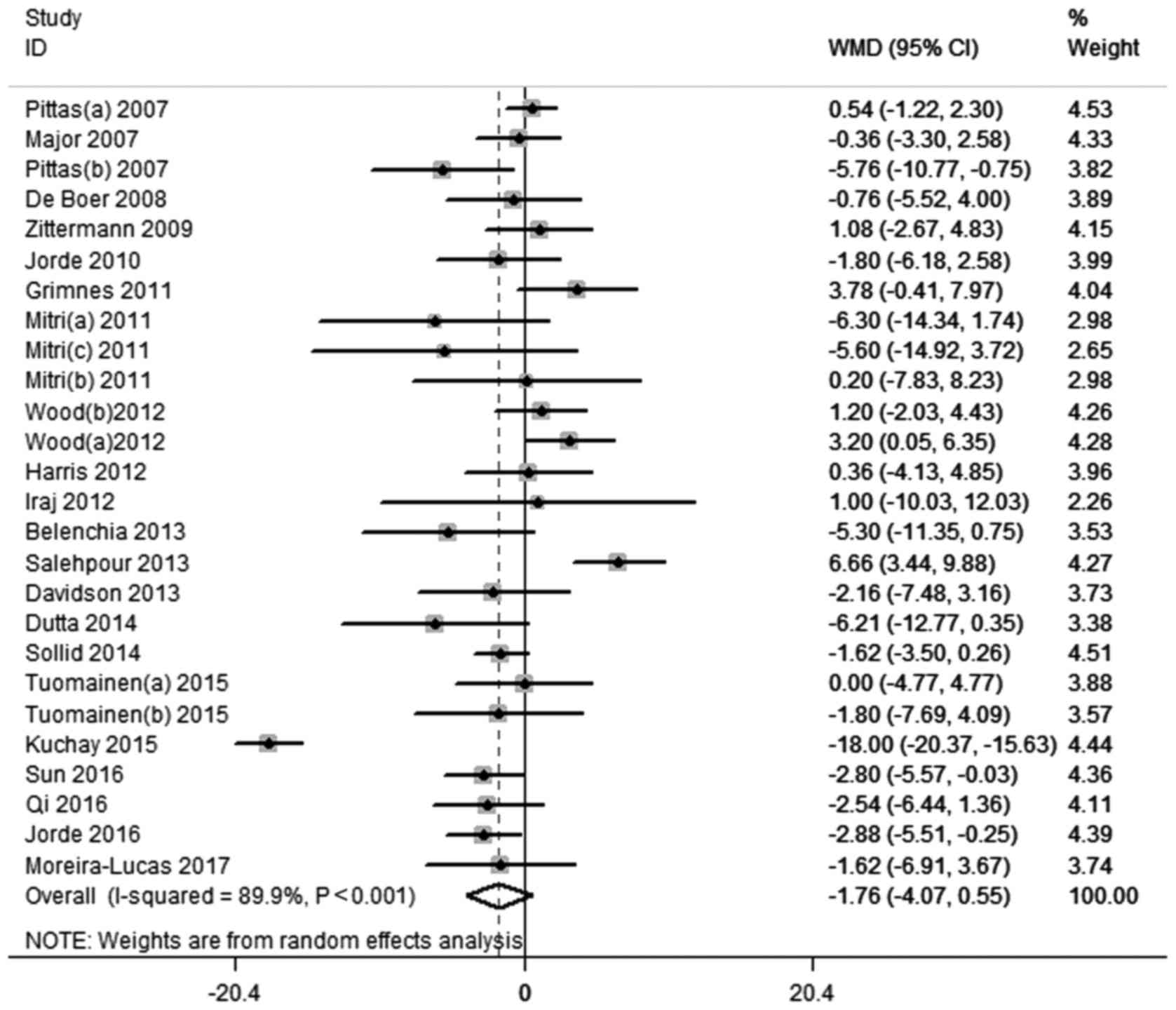
Effect of vitamin D supplementation on
FPG
A total of 21 studies (8,10–19,33,35–43)
containing 26 RCTs reported FPG results. There was statistical
heterogeneity between the studies (I2=89.9%,
P<0.001). Subsequently, the random effect model was used for
analysis. The results indicated that FPG following vitamin D
intervention did not significantly decrease compared with control
(MD=−1.76; 95% CI=−4.07, 0.55, P=0.135; Fig. 2). Subgroup analysis revealed that FPG
levels in pre-diabetic individuals and in those whose BMI <25
with vitamin D supplementation were significantly lower than those
of controls (MD=−3.40; 95% CI=−6.64, −0.15, P=0.041 and MD=−2.80,
95% CI=−5.57, −0.03, P=0.048, respectively; Table II). In the subgroup of baseline
25(OH)D3 insufficiency [20≤ 25(OH)D <30 ng/ml)], the
level of FPG following vitamin D supplementation compared with
control was significantly decreased (MD=−1.99, 95% CI=−3.25, −0.73,
P=0.002; Table II).
| Table II.Results of subgroup and sensitivity
analyses. |
Table II.
Results of subgroup and sensitivity
analyses.
|
| RR | FPG | HOMA-IR |
|---|
|
|
|
|
|
|---|
| Subgroup | RR | 95% CI | P-value | MD | 95% CI | P-value | SMD | 95% CI | P-value |
|---|
| Blood glucose
state |
|
|
|
|
|
|
|
|
|
| Normal
(<6.1 mmol/l) | – | – | – | 1.09 | (−0.89, 3.06) | 0.280 | −0.04 | (−0.21, 0.13) | 0.638 |
|
Prediabetes or early diabetes
(6.1–7.0 mmol/l) | 0.84 | (0.70, 1.00) | 0.047 | −3.40 | (−6.64, −0.15) | 0.041 | −0.02 | (−0.15, 0.12) | 0.817 |
| Age of subjects,
years |
|
|
|
|
|
|
|
|
|
|
<45 | – | – | – | −0.18 | (−4.98, 4.63) | 0.942 | −0.14 | (−0.39, 0.10) | 0.249 |
| 45≤ age
<60 | 0.70 | (0.41, 1.20) | 0.195 | −3.02 | (−8.38, 2.35) | 0.271 | 0.04 | (−0.13, 0.21) | 0.646 |
|
≥60 | 0.90 | (0.71, 1.04) | 0.114 | −0.78 | (−2.33, 0.76) | 0.321 | −0.13 | (−0.36, 0.10) | 0.260 |
| Mean BMI,
kg/m2 |
|
|
|
|
|
|
|
|
|
|
<25 | – | – | – | −2.80 | (−5.57, −0.03) | 0.048 | −0.02 | (−0.46, 0.41) | 0.917 |
| 25≤ BMI
<30 | 0.82 | (0.69, 0.98) | 0.032 | −1.78 | (−5.60, 2.05) | 0.363 | −0.08 | (−0.24, 0.09) | 0.384 |
|
≥30 | 1.33 | (0.45, 3.92) | 0.611 | −1.07 | (−2.58, 0.44) | 0.164 | −0.03 | (−0.21, 0.15) | 0.770 |
| Baseline 25(OH)D,
ng/ml |
|
|
|
|
|
|
|
|
|
|
<20 | 0.84 | (0.70, 1.00) | 0.055 | −1.51 | (−6.17, 3.16) | 0.527 | <0.01 | (−0.13, 0.14) | 0.949 |
| 20≤
25(OH)D <30 | 0.95 | (0.68, 1.33) | 0.758 | −1.99 | (−3.25, −0.73) | 0.002 | −0.09 | (−0.38, 0.21) | 0.575 |
|
≥30 | – | – | – | −2.15 | (−8.26,3.95) | 0.489 | −0.49 | (−0.90, −0.07) | 0.021 |
| Duration,
months |
|
|
|
|
|
|
|
|
|
|
<12 | – | – | – | −0.40 | (−2.82, 2.02) | 0.747 | −0.03 | (−0.22, 0.15) | 0.744 |
|
≥12 | 0.86 | (0.74, 1.01) | 0.072 | −2.53 | (−5.83, −0.76) | 0.132 | −0.02 | (−0.15, 0.10) | 0.725 |
| Dose, IU/day |
|
|
|
|
|
|
|
|
|
|
≤2,000 | 0.95 | (0.68, 1.33) | 0.758 | −0.06 | (−1.99, 1.88) | 0.955 | −0.02 | (−0.15, 0.11) | 0.741 |
|
>2,000 | 0.84 | (0.70, 1.00) | 0.047 | −2.84 | (−6.88, 1.20) | 0.169 | −0.03 | (−0.21, 0.14) | 0.724 |
| Intervention with
calcium |
|
|
|
|
|
|
|
|
|
|
Yes | 0.95 | (0.68, 1.33) | 0.758 | −1.07 | (−3.23, 1.10) | 0.334 | −0.06 | (−0.25, 0.13) | 0.553 |
| No | 0.84 | (0.70, 1.00) | 0.047 | −1.70 | (−4.58, 1.18) | 0.247 | −0.01 | (−0.14, 0.11) | 0.859 |
| Sensitivity
analysis (excluding Jadad <4) | 0.87 | (0.73, 1.05) | 0.156 | −0.86 | (−2.02, 0.30) | 0.147 | −0.05 | (−0.13, 0.08) | 0.635 |
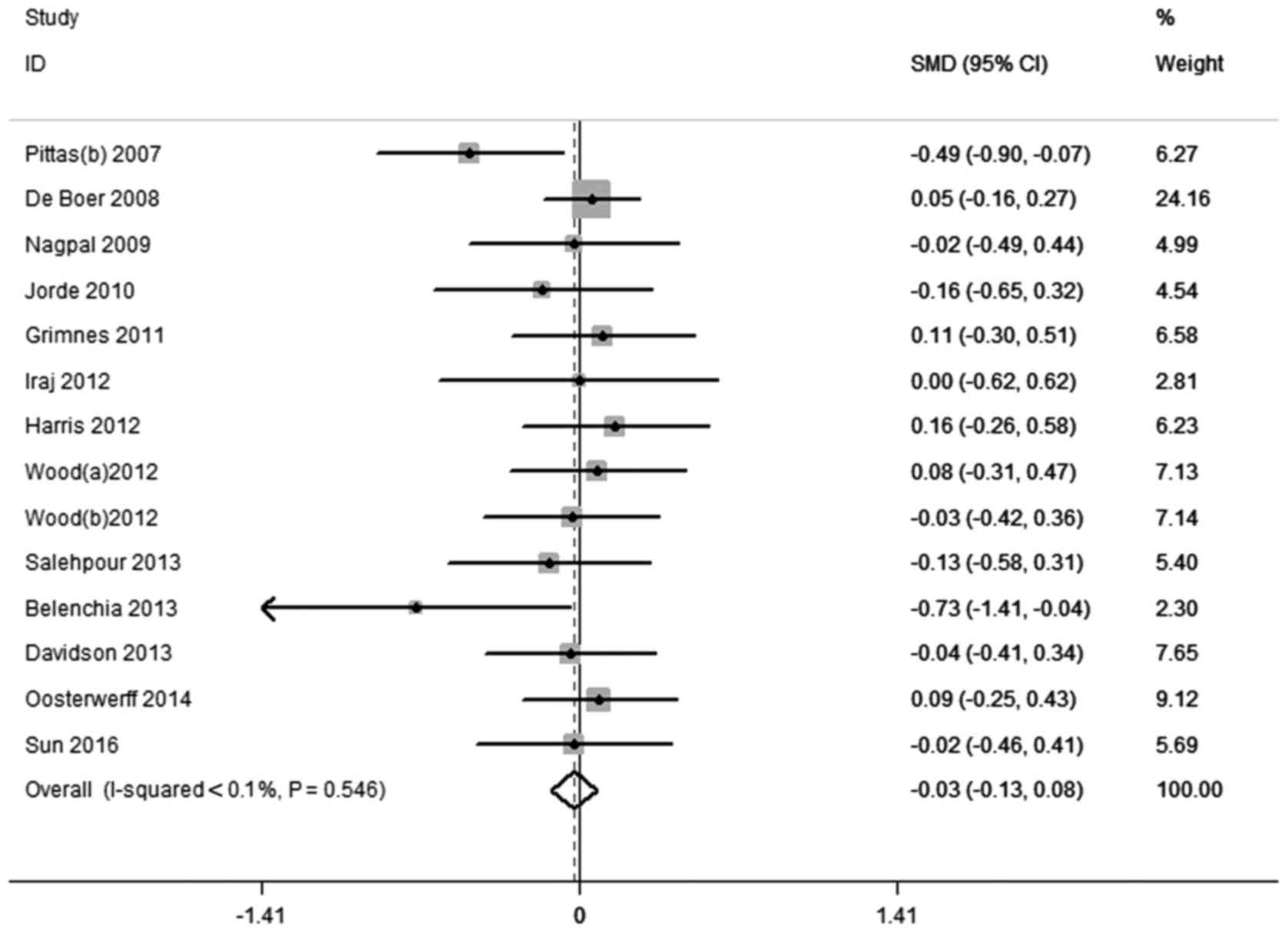
Effect of vitamin D supplementation on
insulin resistance
A total of 13 studies (8–10,12–15,18,33,34,39,41,43)
containing 14 RCTs reported HOMA-IR results. There was no
statistical heterogeneity between the studies
(I2<0.01%, P=0.546). Therefore, the fixed effect
model was applied for analysis of the results. The meta-analysis
indicated that there were no statistically significant changes in
HOMA-IR following vitamin D intervention compared with control
(SMD=−0.03, 95% CI=−0.13, 0.08, P=0.635; Fig. 3). In the subgroup of baseline
25(OH)D3 sufficiency [25(OH)D ≥30 ng/ml)], HOMA-IR
following vitamin D supplementation was significantly lower than
that of controls (SMD=−0.49, 95% CI=−0.90, −0.07, P=0.021; Table II).
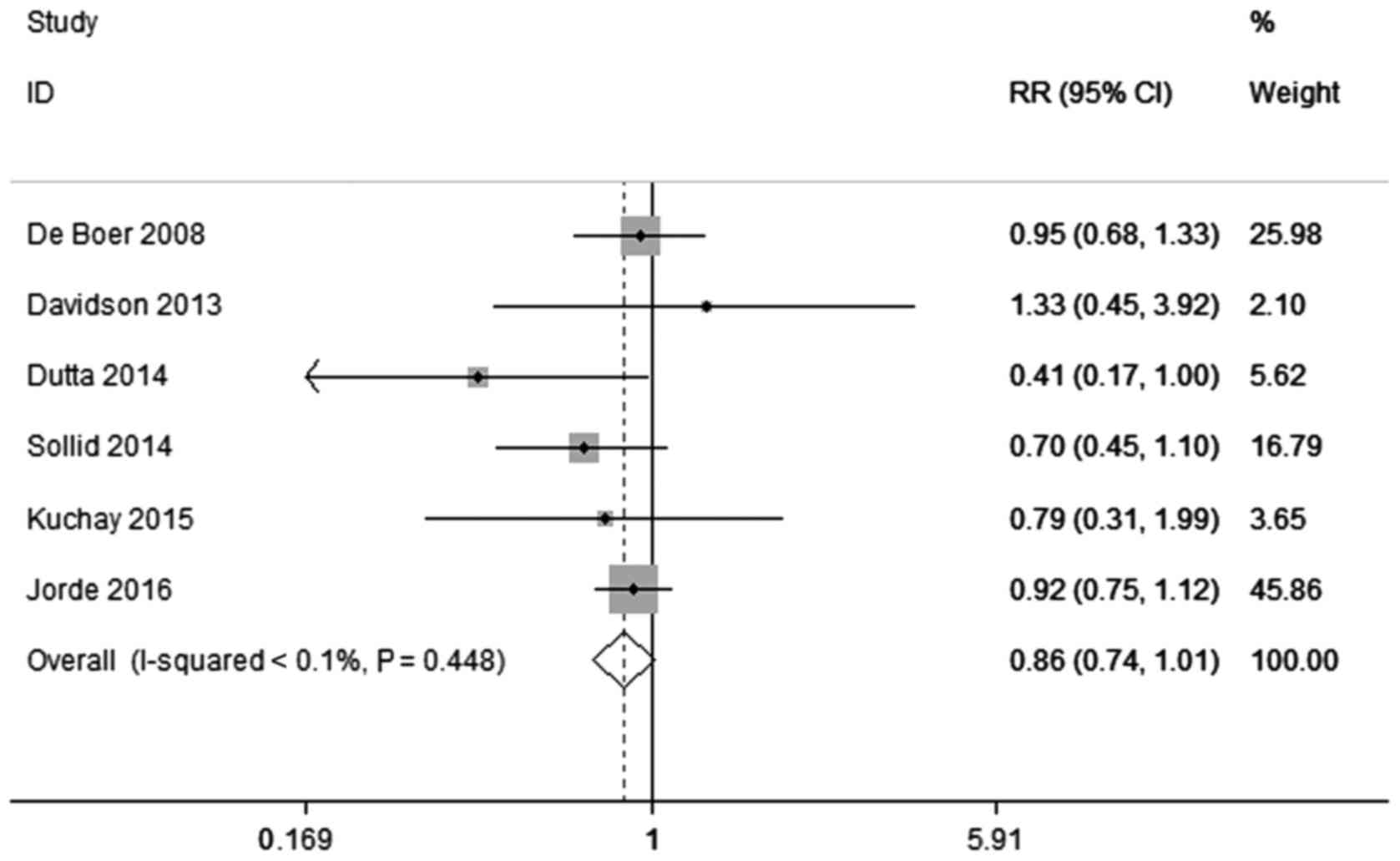
Effect of vitamin D supplementation on
T2DM prevention
A total of 6 studies (11,13,17–19,38)
containing 6 RCTs reported RR results. There was no statistical
heterogeneity between the studies (I2<0.01%,
P=0.448). Subsequently, the fixed effect model was used for
analysis. The results suggested that there was no statistically
significant difference in the incidence of T2DM following vitamin D
intervention or control in the non-diabetic population (RR=0.86,
95% CI=0.74, 1.01, P=0.072; Fig. 4).
Subgroup results indicated that the incidence of T2DM decreased
following intervention with vitamin D supplement dose >2,000
IU/day and in those with intervention without calcium (RR=0.84, 95%
CI=0.70, 1.00, P=0.047 and RR=0.84, 95% CI=0.70, 1.00, P=0.047,
respectively; Table II). In
addition, the incidence rates of T2DM in pre-diabetic individuals
and in overweight (25≤ BMI <30) individuals were lower than that
in controls (RR=0.84, 95% CI=0.70, 1.00, P=0.047 and RR=0.82, 95%
CI=0.69, 0.98, P=0.032, respectively; Table II).
Sensitivity analysis and publication
bias
For each outcome variable, each study was excluded
sequentially, and the results of the remaining studies were
combined to determine the impact of the excluded study on the
overall results. Additionally, following the exclusion of
low-quality studies (Jadad score <4), heterogeneity analysis was
conducted to determine the source of heterogeneity. For the
incidence of T2DM and HOMA-IR, sensitivity analysis indicated that
the results of meta-analysis prior to and following the exclusion
of any one study were similar; however, the result of meta-analysis
of FPG level following the exclusion of one study (11) differed markedly from that prior to its
exclusion (data not shown). Following the exclusion of low quality
studies (11,12,17,18,33,35,40),
the heterogeneity decreased (I2=40.6%, P=0.034; data not
shown). It was hypothesized that literature quality may be a major
source of heterogeneity; on meta-analysis, there were no
significant differences between the effects of vitamin D
intervention and control treatments on RR, FPG and HOMA-IR
following the exclusion of the low-quality studies (Table II). For each outcome variable, there
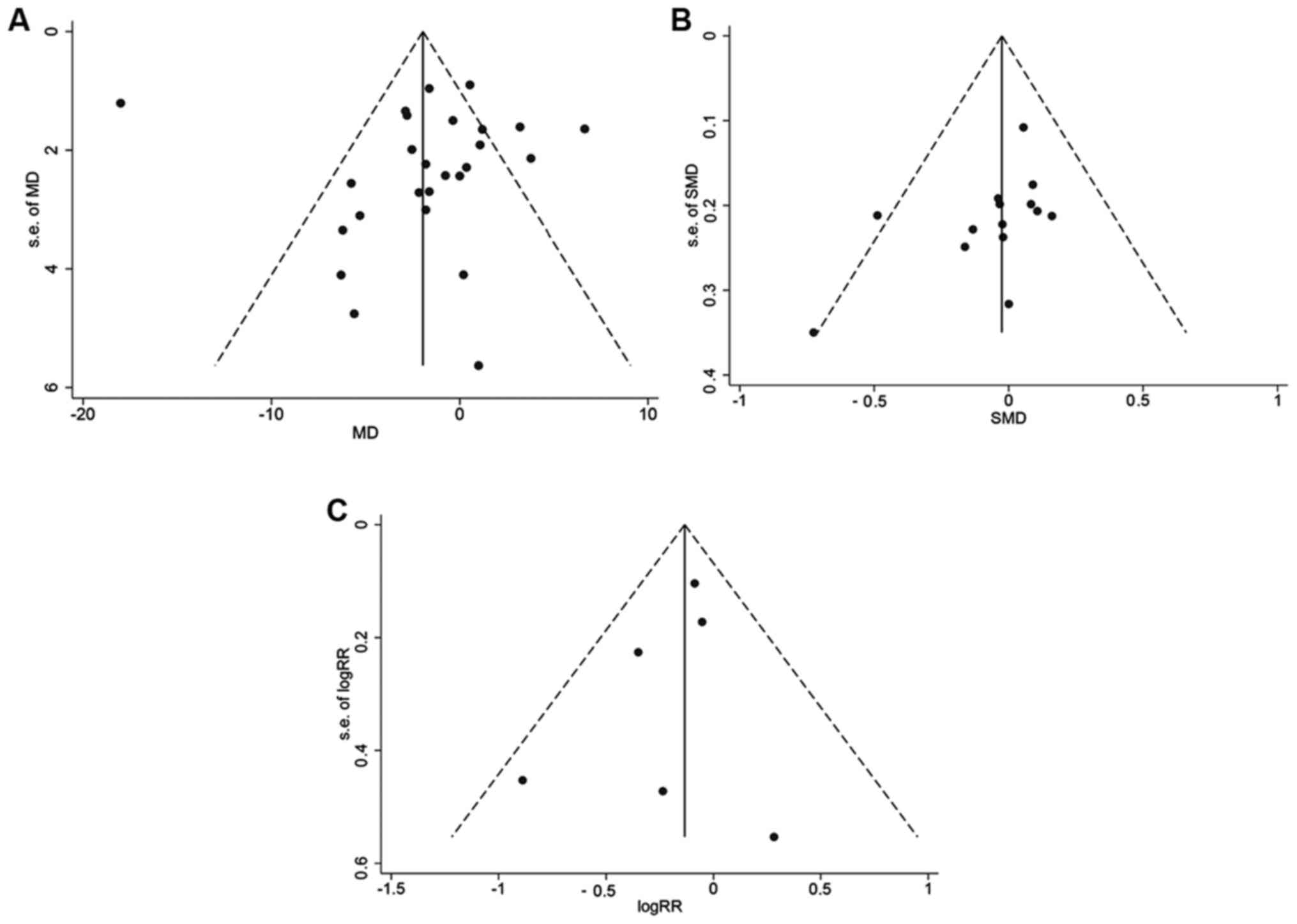
was no obvious asymmetry in funnel plots (Fig. 5). Begg's and Egger's tests also
indicated no significant publication bias for FPG (Begg's test:
P=0.086; Egger's test: P=0.800), insulin resistance (Begg's test:
P=0.125; Egger's test: P=0.080) or T2DM prevention (Begg's test:
P=1.00; Egger's test; P=0.421).
Discussion
To the best of our knowledge, the present report is
the first systematic meta-analysis of the effect of vitamin D
supplementation on FPG, insulin resistance and prevention of T2DM
with consideration of individual variation and intervention
strategy in non-T2DM subjects. Although no significant effect was
identified in the pooled meta-analysis, stratified analysis
suggested that both individual variation and intervention strategy
had influence on the supplementation effect of vitamin D. As T2DM
has a delayed latency and is associated with a variety of
pathogenic factors, the results of the subgroup analysis still have
reference value.
Firstly, the baseline level of 25(OH)D is an
important parameter to consider with vitamin D supplementation. A
significant effect on insulin sensitivity improvement was only
identified for individuals with baseline 25(OH)D levels higher than
30 ng/ml; FPG was decreased significantly by supplementation with
vitamin D in individuals with 25(OH)D levels between 20–30 ng/ml;
and vitamin D supplementation may prevent T2DM among individuals
with 25(OH)D levels lower than 20 ng/ml. Therefore, as the effect
of vitamin D supplementation varied in individuals with different
25(OH)D levels, there should be consideration of baseline 25(OH)D
level during vitamin D supplementation.
Secondly, obesity is a factor that requires
consideration during vitamin D supplementation. No significant
effect was identified in obese subjects (BMI ≥30) on decreasing
FPG, improving insulin sensitivity or preventing T2DM following
vitamin D supplementation. By contrast, decreased FPG was achieved
in healthy-weight subjects (BMI <25); and a T2DM preventative
effect was identified in overweight subjects (25≤ BMI <30).
Therefore, obesity may influence the effect of vitamin D
supplementation; vitamin D is a fat-soluble compound, and thus a
high body fat level may limit vitamin D in exerting its functions
(44). Therefore, how to conduct
vitamin D supplementation in obese individuals requires further
study.
Thirdly, blood glucose state is important to
consider for T2DM prevention and FPG control during vitamin D
supplementation. In the current meta-analysis, significant effects
of vitamin D supplement were observed in prediabetes subjects with
regards to preventing T2DM and controlling FPG, but not to
improving insulin sensitivity. Therefore, preferred outcomes may
only be obtained in individuals with impaired fasting
glycaemia.
Fourthly, the supplementation dose of vitamin D had
a marked effect on T2DM prevention: T2DM development was prevented
by supplementation with high-dose vitamin D (>2,000 IU/day).
Thus, higher doses of vitamin D were preferable for T2DM
prevention. It has been reported that supplementation with
high-dose vitamin D was required to increase vitamin D level to a
normal range in individuals with vitamin D deficiency (45,46). Thus,
high-dose vitamin supplementation may be more effective to improve
vitamin D level in vivo. However, the potential toxicity of
vitamin D remains unclear, and supplementation with high-dose
vitamin D requires caution.
Finally, vitamin D supplementation without Ca had a
significant T2DM preventative effect. It is well known that vitamin
D plays an important role in calcium homeostasis and bone
metabolism. It has been reported that intake of vitamin D and Ca at
the same time may improve the function of vitamin D (47). However, the results of the current
study contradict these previous findings. Therefore, further
comprehensive trials are required to verify the present
results.
In conclusion, supplementation with vitamin D had
differing effects on FPG control, insulin sensitivity improvement
and T2DM prevention in different stratified populations. The
strategy of vitamin D supplementation also influenced the outcomes.
Therefore, future trials should focus on the effects of 25(OH)D
baseline level, obesity, blood glucose state, supplementation dose
and the presence or absence of Ca strengthening in the control of
blood glucose and insulin resistance.
Acknowledgements
Not applicable.
Funding
The present study was supported by the National
Natural Science Foundation of China (grant nos. 81703270, 81573151
and 81573243) and the Science and Technology Foundation for
Innovation Talent of Henan Province (grant no. 154200510010).
Availability of data and materials
All data generated or analyzed during the study are
included in this published article.
Authors' contributions
SH and ZZ were responsible for literature retrieving
and data extraction. CW and YW performed the data analysis. SY and
WL were responsible for the study design and writing of the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
T2DM
|
type 2 diabetes mellitus
|
|
25(OH)D
|
25-hydroxyvitamin D
|
|
RCT
|
randomized clinical trial
|
|
FPG
|
fasting plasma glucose
|
|
HOMA-IR
|
homeostasis model insulin resistance
index
|
|
BMI
|
body mass index
|
|
SD
|
standard deviation
|
|
CI
|
confidence interval
|
|
RR
|
relative risk
|
|
MD
|
mean difference
|
|
SMD
|
standardized mean difference
|
|
WMD
|
weighted mean difference
|
|
ITT
|
intention-to-treat
|
References
|
1
|
van Driel M and van Leeuwen JPTM: Vitamin
D endocrinology of bone mineralization. Mol Cell Endocrinol.
453:46–51. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bikle DD: Extraskeletal actions of vitamin
D. Ann N Y Acad Sci. 1376:29–52. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Autier P, Boniol M, Pizot C and Mullie P:
Vitamin D status and ill health: A systematic review. Lancet
Diabetes Endocrinol. 2:76–89. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang H, Chen W, Li D, Yin X, Zhang X,
Olsen N and Zheng SG: Vitamin D and chronic diseases. Aging Dis.
8:346–353. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pannu PK, Piers LS, Soares MJ, Zhao Y and
Ansari Z: Vitamin D status is inversely associated with markers of
risk for type 2 diabetes: A population based study in Victoria,
Australia. PLoS One. 12:e01788252017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lucato P, Solmi M, Maggi S, Bertocco A,
Bano G, Trevisan C, Manzato E, Sergi G, Schofield P, Kouidrat Y, et
al: Low vitamin D levels increase the risk of type 2 diabetes in
older adults: A systematic review and meta-analysis. Maturitas.
100:8–15. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Berridge MJ: Vitamin D deficiency and
diabetes. Biochem J. 474:1321–1332. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Belenchia AM, Tosh AK, Hillman LS and
Peterson CA: Correcting vitamin D insufficiency improves insulin
sensitivity in obese adolescents: A randomized controlled trial. Am
J Clin Nutr. 97:774–781. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nagpal J, Pande JN and Bhartia A: A
double-blind, randomized, placebo-controlled trial of the
short-term effect of vitamin D3 supplementation on
insulin sensitivity in apparently healthy, middle-aged, centrally
obese men. Diabet Med. 26:19–27. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pittas AG, Harris SS, Stark PC and
Dawson-Hughes B: The effects of calcium and vitamin D
supplementation on blood glucose and markers of inflammation in
nondiabetic adults. Diabetes Care. 30:980–986. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kuchay MS, Laway BA, Bashir MI, Wani AI,
Misgar RA and Shah ZA: Effect of vitamin D supplementation on
glycemic parameters and progression of prediabetes to diabetes: A
1-year, open-label randomized study. Indian J Endocrinol Metab.
19:387–392. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Iraj B, Aminorroaya A and Amini M: Does
the intramuscular injection of vitamin D increase insulin
resistance? J Res Pharm Pract. 1:60–65. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Davidson MB, Duran P, Lee ML and Friedman
TC: High-dose vitamin D supplementation in people with prediabetes
and hypovitaminosis D. Diabetes Care. 36:260–266. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Grimnes G, Figenschau Y, Almås B and Jorde
R: Vitamin D, insulin secretion, sensitivity, and lipids: Results
from a case-control study and a randomized controlled trial using
hyperglycemic clamp technique. Diabetes. 60:2748–2757. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Jorde R, Sneve M, Torjesen P and
Figenschau Y: No improvement in cardiovascular risk factors in
overweight and obese subjects after supplementation with vitamin D3
for 1 year. J Intern Med. 267:462–472. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Moreira-Lucas TS, Duncan AM, Rabasa-Lhoret
R, Vieth R, Gibbs AL, Badawi A and Wolever TM: Effect of vitamin D
supplementation on oral glucose tolerance in individuals with low
vitamin D status and increased risk for developing type 2 diabetes
(EVIDENCE): A double-blind, randomized, placebo-controlled clinical
trial. Diabetes Obes Metab. 19:133–141. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dutta D, Mondal SA, Choudhuri S, Maisnam
I, Reza Hasanoor AH, Bhattacharya B, Chowdhury S and Mukhopadhyay
S: Vitamin-D supplementation in prediabetes reduced progression to
type 2 diabetes and was associated with decreased insulin
resistance and systemic inflammation: An open label randomized
prospective study from Eastern India. Diabetes Res Clin Pract.
103:e18–e23. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
de Boer IH, Tinker LF, Connelly S, Curb
JD, Howard BV, Kestenbaum B, Larson JC, Manson JE, Margolis KL,
Siscovick DS and Weiss NS: Women's Health Initiative Investigators:
Calcium plus vitamin D supplementation and the risk of incident
diabetes in the Women's Health Initiative. Diabetes Care.
31:701–707. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jorde R, Sollid ST, Svartberg J, Schirmer
H, Joakimsen RM, Njølstad I, Fuskevåg OM, Figenschau Y and
Hutchinson MY: Vitamin D 20,000 IU per week for five years does not
prevent progression from prediabetes to diabetes. J Clin Endocrinol
Metab. 101:1647–1655. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wu C, Qiu S, Zhu X and Li L: Vitamin D
supplementation and glycemic control in type 2 diabetes patients: A
systematic review and meta-analysis. Metabolism. 73:67–76. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee CJ, Iyer G, Liu Y, Kalyani RR, Bamba
N, Ligon CB, Varma S and Mathioudakis N: The effect of vitamin D
supplementation on glucose metabolism in type 2 diabetes mellitus:
A systematic review and meta-analysis of intervention studies. J
Diabetes Complications. 31:1115–1126. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Akbari M, Moosazadeh M, Lankarani KB,
Tabrizi R, Samimi M, Karamali M, Jamilian M, Kolahdooz F and Asemi
Z: Correction: The effects of vitamin D supplementation on glucose
metabolism and lipid profiles in patients with gestational
diabetes: A systematic review and meta-analysis of randomized
controlled trials. Horm Metab Res. Aug 2–2017.(Epub ahead of
print).
|
|
23
|
Jamka M, Woźniewicz M, Jeszka J, Mardas M,
Bogdański P and Stelmach-Mardas M: The effect of vitamin D
supplementation on insulin and glucose metabolism in overweight and
obese individuals: Systematic review with meta-analysis. Sci Rep.
5:161422015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kresevic DM, Denton JE, Burant CJ and
Pallaki M: Racial difference in response to vitamin D
supplementation. J Natl Med Assoc. 107:18–24. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Dasarathy J, Varghese R, Feldman A,
Khiyami A, McCullough AJ and Dasarathy S: Patients with
nonalcoholic fatty liver disease have a low response rate to
vitamin D supplementation. J Nutr. 147:1938–1946. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
American Diabetes Association: Diagnosis
and classification of diabetes mellitus. Diabetes Care. 33 Suppl
1:S62–S69. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Higgins and Green JPT S: Cochrane Handbook
for Systematic Reviews of Interventions, version 5.1.0. The
Cochrane Collaboration. 2282011.
|
|
28
|
Jadad AR, Moore RA, Carroll D, Jenkinson
C, Reynolds DJ, Gavaghan DJ and McQuay HJ: Assessing the quality of
reports of randomized clinical trials: is blinding necessary?
Control Clin Trials. 17:1–12.. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Follmann D, Elliott P, Suh I and Cutler J:
Variance imputation for overviews of clinical trials with
continuous response. J Clin Epidemiol. 45:769–773. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Flegal KM, Kit BK, Orpana H and Graubard
BI: Association of all-cause mortality with overweight and obesity
using standard body mass index categories: A systematic review and
meta-analysis. JAMA. 309:71–82. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Gallagher JC and Sai AJ: Vitamin D
insufficiency, deficiency, and bone health. J Clin Endocrinol
Metab. 95:2630–2633. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Jin ZC, Zhou XH and He J: Statistical
methods for dealing with publication bias in meta-analysis. Stat
Med. 34:343–360. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Salehpour A, Shidfar F, Hosseinpanah F,
Vafa M, Razaghi M and Amiri F: Does vitamin D3
supplementation improve glucose homeostasis in overweight or obese
women? A double-blind, randomized, placebo-controlled clinical
trial. Diabet Med. 30:1477–1481. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Oosterwerff MM, Eekhoff EM, Van Schoor NM,
Boeke AJ, Nanayakkara P, Meijnen R, Knol DL, Kramer MH and Lips P:
Effect of moderate-dose vitamin D supplementation on insulin
sensitivity in vitamin D-deficient non-Western immigrants in the
Netherlands: A randomized placebo-controlled trial. Am J Clin Nutr.
100:152–160. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Qi M, Song Y, Li J, Tian L, Wang L, Xie Y,
Gup Y and Bao Y: Effect of vitamin D supplementation on
postprandial glucose in the elder with vitamin D deficiency and
impaired glucose tolerance. Chin J Mod Drug Appl. 10:196–197.
2016.(In Chinese).
|
|
36
|
Mitri J, Dawson-Hughes B, Hu FB and Pittas
AG: Effects of vitamin D and calcium supplementation on pancreatic
β cell function, insulin sensitivity, and glycemia in adults at
high risk of diabetes: The calcium and vitamin D for diabetes
mellitus (CaDDM) randomized controlled trial. Am J Clin Nutr.
94:486–494. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Tuomainen TP, Virtanen JK, Voutilainen S,
Nurmi T, Mursu J, de Mello VD, Schwab U, Hakumäki M, Pulkki K and
Uusitupa M: Glucose metabolism effects of vitamin D in prediabetes:
The VitDmet randomized placebo-controlled supplementation study. J
Diabetes Res. 2015:6726532015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Sollid ST, Hutchinson MY, Fuskevåg OM,
Figenschau Y, Joakimsen RM, Schirmer H, Njølstad I, Svartberg J,
Kamycheva E and Jorde R: No effect of high-dose vitamin D
supplementation on glycemic status or cardiovascular risk factors
in subjects with prediabetes. Diabetes Care. 37:2123–2131. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Harris SS, Pittas AG and Palermo NJ: A
randomized, placebo-controlled trial of vitamin D supplementation
to improve glycaemia in overweight and obese African Americans.
Diabetes Obes Metab. 14:789–794. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Major GC, Alarie F, Doré J, Phouttama S
and Tremblay A: Supplementation with calcium + vitamin D enhances
the beneficial effect of weight loss on plasma lipid and
lipoprotein concentrations. Am J Clin Nutr. 85:54–59.
2007.PubMed/NCBI
|
|
41
|
Wood AD, Secombes KR, Thies F, Aucott L,
Black AJ, Mavroeidi A, Simpson WG, Fraser WD, Reid DM and Macdonald
HM: Vitamin D3 supplementation has no effect on conventional
cardiovascular risk factors: A parallel-group, double-blind,
placebo-controlled RCT. J Clin Endocrinol Metab. 97:3557–3568.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Zittermann A, Frisch S, Berthold HK,
Götting C, Kuhn J, Kleesiek K, Stehle P, Koertke H and Koerfer R:
Vitamin D supplementation enhances the beneficial effects of weight
loss on cardiovascular disease risk markers. Am J Clin Nutr.
89:1321–1327. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Sun X, Cao ZB, Tanisawa K, Ito T, Oshima S
and Higuchi M: Vitamin D supplementation reduces insulin resistance
in Japanese adults: A secondary analysis of a double-blind,
randomized, placebo-controlled trial. Nutr Res. 36:1121–1129. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Vimaleswaran KS, Berry DJ, Lu C, Tikkanen
E, Pilz S, Hiraki LT, Cooper JD, Dastani Z, Li R, Houston DK, et
al: Genetic Investigation of Anthropometric Traits-GIANT
Consortium: Causal relationship between obesity and vitamin D
status: Bi-directional Mendelian randomization analysis of multiple
cohorts. PLoS Med. 10:e10013832013. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Gowda U, Ruwanpathirana T, Fong DP, Kaur A
and Renzaho AM: Efficacy of high dose vitamin D supplementation in
improving serum 25(OH)D among migrant and non migrant population: A
retrospective study. BMC Health Serv Res. 16:5792016. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Yang Y, Li Z, Yan G, Jie Q and Rui C:
Effect of different dose of vitamin D supplementation on preterm
infants- an updated meta-analysis. J Matern Fetal Neonatal Med. Oct
5–2017.(Epub ahead of print). View Article : Google Scholar
|
|
47
|
Pittas AG, Dawson-Hughes B, Li T, Van Dam
RM, Willett WC, Manson JE and Hu FB: Vitamin D and calcium intake
in relation to type 2 diabetes in women. Diabetes Care. 29:650–656.
2006. View Article : Google Scholar : PubMed/NCBI
|