Introduction
Fever of unknown origin (FUO) is a diagnostic
challenge, despite recent advances in diagnostic modalities
(1,2). FUO is defined as a prolonged febrile
illness without a recognized cause, even after comprehensive
laboratory tests and imagining workup. The current definition of
FUO is as follows: i) Body temperature of ≥38.3˚C on at least two
occasions; ii) duration of illness of ≥3 weeks; iii) not an
immunocompromised setting; and iv) uncertain diagnosis despite
thorough history taking, physical examination and laboratory
assessments. These laboratory measures include the erythrocyte
sedimentation rate (ESR), C-reactive protein (CRP), hemoglobin,
platelet count, leukocyte count and differentiation, electrolyte
levels, creatinine level, total serum protein, protein
electrophoresis, alkaline phosphatase, aspartate aminotransferase,
lactate dehydrogenase (LDH), ferritin, microscopic urinalysis,
blood cultures and urine cultures. The most common radiological
investigation includes chest X-ray and abdominal ultrasonography.
Additional tests may include the tuberculin test or an interferon-γ
release assay (3,4). The cause of FUO may be multifactorial
and can be subdivided into four categories: Infections,
malignancies, noninfectious inflammatory processes and
miscellaneous causes (5). FUO is
closely related to inflammation of unknown origin (IUO), and the
causes and workups are the same for both FUO and IUO (6). Early identification of the cause of
FUO is important for guiding the diagnostic workup and for
initiating early and appropriate treatment without notable impacts
on patient care (7).
Conventional anatomic imaging modalities, such as
ultrasonography, and cross-sectional imaging with CT and MRI, are
used as primary diagnostic modalities to manage FUO; however, they
have limited sensitivity and specificity (8). Therefore, a significant number of
patients with FUO (30-50%) leave the hospital without specific
diagnoses (9). Positron emission
tomography (PET)/CT using 18F-fluorodeoxyglucose
(18FDG) is a well-accepted clinical tool for routine use
in a wide range of malignancies. 18FDG is a glucose
analogue that accumulates in cells with high metabolic
requirements, such as tumor and inflammatory cells.
18FDG PET/CT is currently considered a useful
noninvasive imaging modality for the evaluation of patients with
FUO (10-13).
However, only a few studies have assessed 18FDG PET/CT
in patients with FUO. Furthermore, most of these studies were
performed in developed countries and the geographic area of the
study strongly influenced the determination of the final diagnosis.
Studies have shown that the cause of FUO in developing countries
was most often infectious (14,15),
whereas noninfectious inflammatory processes were the most common
drivers of FUO in developed countries.
Several meta-analyses have reported the positive
impact of FDG PET/CT in establishing the final diagnosis of
patients with FUO/IUO. The diagnostic yield of PET CT/CT in this
population is 56-60%, which is ≥30% higher than that of
conventional CT (16,17). However, most studies are
retrospective studies, with significant heterogeneity of baseline
study characteristics, definition of FUO/IUO and imaging parameters
(18,19). In certain studies, FDG PET/CT was
the only imaging modality that was able to establish a final
diagnosis (18,19). The vast majority of the studies
investigated the diagnostic value of PET/CT, with only a few
studies investigating the cost-effectiveness of FDG PET/CT in the
diagnostic work-up of patients with FUO (20). Based on the previous studies,
patients with FUO/IUO are a challenging, heterogeneous population
with a wide variety of differential diagnoses. Furthermore, there
is a lack of an established work-up strategy. According to
published data, it is important to further investigate the
diagnostic impact of PET/CT, the cost-effectiveness, and when and
how to perform PET/CT in the setting of FUO/FUI (21).
The purpose of the present study was to evaluate the
performance and benefit of 18FDG PET/CT in patients who
presented with FUO at a tertiary academic general hospital in
Riyadh, Saudi Arabia.
Patients and methods
Study population
The study was approved by the King Faisal Hospital
and Research Center (Riyadh, Saudi Arabia) Institutional review
board on 11/01/2021 (approval no. 2211019), and the requirement for
informed consent was waived for the present retrospective study. A
total of 105 patients {61 men and 44 women; median [interquartile
range (IQR)] of age, 51 (31-65) years} who underwent
18FDG PET/CT because of FUO between January 2016 and
December 2019 were included in the present retrospective study.
These patients met the definition criteria of FUO (febrile illness
of >38.3˚C and no diagnosis after at least 3 days of inpatient
or 3 weeks of outpatient investigation after thorough history
taking, physical examination and standard diagnostic workup).
Eligible patients were identified in the radiology information
system by searching various categories, including FUO, IUO,
unexplained fever and fever of unknown cause. Patients with
nosocomial infection, known HIV infection, immunocompromised status
and established etiology of FUO/IUO on conventional imaging were
excluded from the present study.
Whole-body 18FDG PET/CT was requested to
determine the cause of fever. 18FDG PET/CT was performed
according to the standard protocol. The patients underwent imaging
from the vertex of the skull to the mid-thigh area. Non-contrast CT
images were used for attenuation correction and for anatomic
localization. Any 18FDG accumulation that could not be
explained by physiologic distribution was designated abnormal. Both
normal and abnormal 18FDG results were evaluated for
their diagnostic contribution to patient assessment. The
18FDG PET/CT results were classified into four
categories: i) True-positive if 18FDG PET/CT identified
the specific etiology of FUO that was confirmed with additional
investigation or response to treatment; ii) false-negative if
18FDG uptake was normal but a specific disease was
identified by another diagnostic test or response to treatment;
iii) false-positive if 18FDG uptake could not identify
the cause of FUO; and iv) true-negative if neither 18FDG
PET/CT nor standard diagnostic procedures found the cause of FUO.
The nuclear medicine physicians reading the 18FDG PET/CT
scans had knowledge of the clinical history and results of prior
imaging studies of each patient.
Statistical analysis
Descriptive statistics are presented as the mean ±
SD for normally distributed numerical variables and as the median
[interquartile range (IQR)] for non-normally distributed numerical
variables. The Shapiro-Wilk test was used to test for normality.
Frequencies and percentages were used for categorical variables.
Comparison of the groups was performed using one-way analysis of
variance for normally distributed numerical variables and the
Kruskal-Wallis test for non-normally distributed numerical
variables. Bonferroni correction was used as the post-hoc test. The
χ2 test was used to compare categorical variables. IBM
SPSS statistics software (version 26; IBM Corp.) was used for the
analysis. P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics
A total of 105 patients were included (61 men and 44
women), and the median (IQR) age was 51 (31-65) years. The mean ±
SD ESR level was 71.5±40.6 mm/h. Additional acute-phase parameters
were as follows: CRP, 139 (51-234) mg/l; white blood cell count
(WBC), 8.9x103/µl (4.5-1,2103/µl); LDH, 249
U/l; and ferritin, 672 (363-1,266) µg/l A total of 21 patients
received corticosteroids before their 18FDG PET/CT
scans, 17 patients (16%) had positive blood cultures and 13
patients (12.4%) had positive urine cultures. Tissue biopsy was
performed for 46 patients (34.3%). Blood cultures, urine cultures
and tissue biopsy were performed according to standard procedures.
Table I shows the patient
characteristics.
 | Table IPatient demographics, laboratory data
and PET/CT results for the total study population (n=105). |
Table I
Patient demographics, laboratory data
and PET/CT results for the total study population (n=105).
| Characteristic
(normal ranges) | Value |
|---|
| Age, years | 51 (31-65) |
| Sex | |
|
Male | 61 (58.1) |
|
Female | 44 (41.9) |
| Laboratory
data | |
|
WBC,
x103/µl (4.5-11.0) | 8.9 (4.5-12) |
|
CRP, mg/l
(8-10) | 139 (51-234) |
|
ESR, mm/h
(<15) | 71.5±40.6 |
|
LDH, U/l
(140-280) | 249 (184-444) |
|
Ferritin,
µg/l (24-336) | 672
(363-1,266) |
|
Positive
blood culture | 17 (16.2) |
|
Positive
urine culture | 13 (12.4) |
| Biopsy
performed | 36 (34.3) |
| Patients treated
with corticosteroids | 21(20) |
| PET/CT results | |
|
True-positive | 51 (48.6) |
|
False-positive | 24 (22.9) |
|
True-negative | 10 (9.5) |
|
False-negative | 20(19) |
Positive and negative 18FDG
PET/CT and classification of 18FDG PET/CT results by
final diagnosis
Of the 105 patients, 75 patients (72%) had positive
PET/CT results and 30 patients (29%) had negative results. The CRP
and ferritin values differed significantly between the two groups.
The median CRP and ferritin levels were higher in the positive
group than in the negative PET/CT group (P=0.019 and P=0.024
respectively; Table II). According
to the final diagnoses, 18FDG PET/CT results were
classified into four categories: Group 1, patients with
true-positive results (n=51; 49%), in whom abnormal
18FDG uptake identified the process that directly led to
the final diagnosis; group 2, patients with false-positive results
(n=24; 23%), in whom 18FDG uptake was not consistent
with the final diagnosis reflecting the etiology of FUO; group 3,
patients with true-negative results (n=10; 9.5%), in whom
18FDG uptake was unremarkable and no final disease was
established through follow-up or other diagnostic tests; and group
4, patients with false-negative results (n=20; 19%), in whom
18FDG PET/CT uptake was normal and final disease was
established with other tests or response to treatment. Patients in
group 1 (true-positive) were heterogeneous and no single gold
standard test was used to establish a final diagnosis. The final
diagnosis was made by the referring physician and supported by
other diagnostic studies, tissue biopsy, other laboratory tests and
continued follow-up. There were no statistically significant
differences among the four groups in terms of age, sex, WBC, ESR,
LDH or ferritin values.
| Table IIPatient characteristics based on
positron emission tomography/CT results in the total study
population (n=105). |
Table II
Patient characteristics based on
positron emission tomography/CT results in the total study
population (n=105).
| Characteristic | Group 1,
true-positive (n=51) | Group 2,
false-positive (n=24) | Group 3,
true-negative (n=10) | Group 4,
false-negative (n=20) | P-value |
|---|
| Age, years | 52 (38-66) | 36 (23.5-65) | 56 (29-72) | 54.5 (30-64.5) | 0.564 |
| Sex | | | | | 0.980 |
|
Male | 30 (58.8) | 13 (54.2) | 6(60) | 12(60) | |
|
Female | 21 (41.2) | 11 (45.8) | 4(40) | 8(40) | |
| WBC,
103/µl | 8 (3.25-12) | 10.1
(5.92-15.145) | 8.9 (5.5-10.3) | 9.5
(4.43-11.5) | 0.595 |
| CRP, mg/l | 146.5 (70-230) | 171 (75-280) | 105 (7.4-154) | 53 (11-234) | 0.120 |
| ESR, mm/h | 154.2±100.6 | 190.4±170.3 | 107.9±106.5 | 115.8±124.9 | 0.179 |
| LDH, U/l | 244 (180-631) | 267.5
(189.5-442) | 263.5
(183-301) | 223.5
(176-305.5) | 0.705 |
| Ferritin, µg/l | 765 (452-1384) | 606.5
(352-1785.5) | 509 (342-782) | 371
(149.5-1061) | 0.135 |
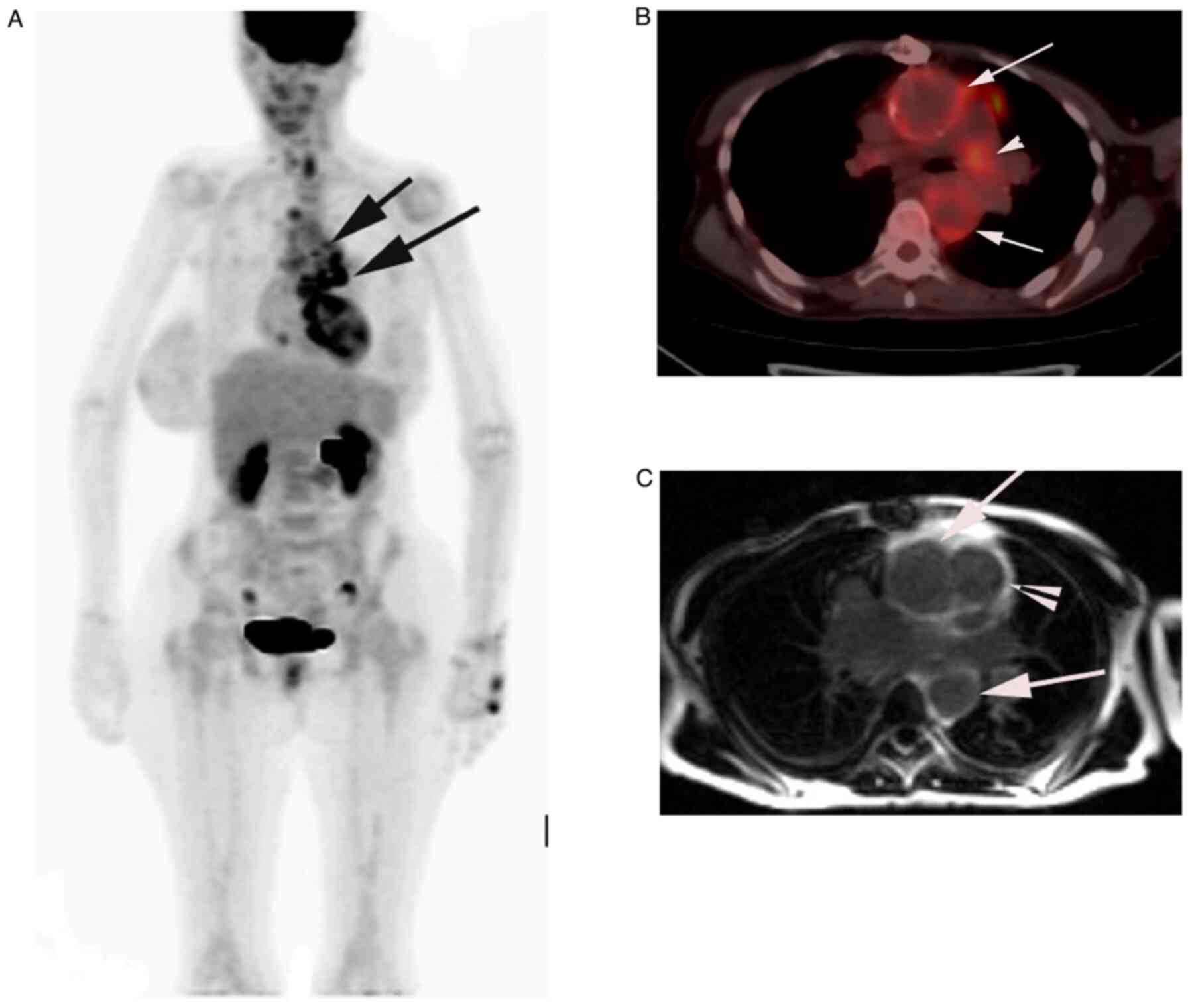
True-positive results
As shown in Table
III, of the 51 patients with true-positive PET/CT results, 26
had infections (51%), 18 (35%) had malignancies and 7 (14%) had
inflammatory noninfectious processes. For these patients, the
different disease categories, infections, neoplasms and
noninfectious inflammatory processes were compared. Examples of
cases with true-positive PET/CT scans are shown in Fig. 1, Fig.
2 and Fig. 3. The WBC and
ferritin levels differed significantly among groups (group with
infection, malignancies and inflammatory non-infectious). The WBC
count was highest in patients with infections, i.e. 11.2 (6-13.9)
103/µl compared to patients with neoplasms [3.5
(2-8.12)x103/µl] and patients with
inflammatory/autoimmune disease [8.4 (8-11.52) 103/µl]
(P=0.018). Also, the ferritin levels were significantly different
among the three true-positive groups, including infection, neoplasm
and inflammatory/autoimmune disease (P=0.04).
| Table IIIPatient characteristics and
laboratory test results in true-positive patients (n=51). |
Table III
Patient characteristics and
laboratory test results in true-positive patients (n=51).
| Characteristic | Infection
(n=26) | Neoplasm
(n=18) |
Inflammation/autoimmune (n=7) | P-value |
|---|
| Age, years | 53±21.2 | 47.9±20.3 | 51.4±11 | 0.707 |
| Sex | | | | 0.737 |
|
Male | 14 (53.8) | 11 (61.1) | 5 (71.4) | |
|
Female | 12 (46.2) | 7 (38.9) | 2 (28.6) | |
| WBC,
103/µl | 11.2 (613.9) | 3.5 (28.12) | 8.4 (811.52) | 0.018 |
| CRP, mg/l | 11.5 (55167) | 19.0 (103 270) | 14.4 (54181) | 0.166 |
| ESR, mm/h | 78.3±33.6 | 84.3±32.9 | 96.3±44.9 | 0.477 |
| LDH, U/l | 236.5 (194438) | 346 (216826) | 162 (1211631) | 0.128 |
| Ferritin, µg/l | 714.5 (45 886) | 1115.5
(6713068) | 562 (3771451) | 0.043 |
False-positive results
In addition to the normal physiological distribution
of 18FDG, abnormal 18FDG uptake was reported
in 24 patients (23%), in whom no cause of FUO could be identified.
These results were considered false-positives. The most common
sites of abnormal 18FDG uptake were the multiple lymph
nodes above and below the diaphragm, the bone marrow, the pelvic
and bowl (including focal or diffuse uptake), the head and neck,
and the lung (areas of mediastinal and hilar adenopathy) (data not
shown).
True-negative and false-negative
18FDG PET/CT results
The 18FDG PET/CT showed a normal tracer
distribution and was reported as normal in 10 patients (9.5%), and
no final diagnosis was established. These results were considered
true negatives. False-negative PET/CT results were reported in 20
patients (19%), in whom 18FDG PET/CT was reportedly
normal, but a final diagnosis of infection (such as tuberculosis,
brucellosis or enteric fever), malignancy (such as lymphoma) or
inflammatory noninfectious disease (such as rheumatoid arthritis or
adult-onset Still’s disease) was established by other diagnostic or
laboratory tests, or after a specific therapy (data not shown).
Sensitivity, specificity and positive-
and negative-predictive values of PET/CT
The overall sensitivity, specificity, positive
predictive value, negative predictive value and accuracy was 72,
29, 68, 33 and 58%, respectively (Table IV). However, due to the small
number of patients in each group, no additional analysis of the
diagnostic performance of 18FDG PET/CT was
undertaken.
| Table IVSensitivity, specificity, and
positive and negative predictive value of fluorodeoxyglucose
positron emission tomography/CT. |
Table IV
Sensitivity, specificity, and
positive and negative predictive value of fluorodeoxyglucose
positron emission tomography/CT.
| Diagnostic
performance | Value, % | 95% CI, % |
|---|
| Sensitivity | 71.83 | 59.90-81.87 |
| Specificity | 29.41 | 15.10-47.48 |
| Positive predictive
value | 68.00 | 62.07-73.40 |
| Negative predictive
value | 33.33 | 20.87-48.66 |
| Accuracy | 58.10 | 48.07-67.66 |
Discussion
To the best of our knowledge, the present study was
the first study in Saudi Arabia and the Middle East to investigate
the diagnostic value of 18FDG PET/CT in identifying the
underlying etiology of patients with disease with FUO. The present
study investigated 105 patients with FUO and IUO, and revealed that
18FDG PET/CT helped identify the etiology of the
underlying disease and establish a final diagnosis in 49% of
patients. This group was classified as the true-positive group,
yielding a sensitivity of 72% and a positive predictive value of
68%. PET/CT was negative in 10% of patients, in whom there was no
final diagnosis and PET/CT was considered a true negative, yielding
a low specificity and negative predictive value of 29 and 33%,
respectively. The final diagnoses of FUO etiology in this cohort
included focal or systemic infections (51%), malignancies (35%) and
inflammatory noninfectious processes (14%). These results are
comparable to those of published studies of FUO, in which the
sensitivity varied between 26 and 75% (22-31).
Determining the diagnostic value and accuracy of 18FDG
PET/CT in the setting of FUO is complex and at times controversial.
The sensitivity and specificity of 18FDG PET/CT are
difficult to establish in FUO because of the numerous potential
differential diagnoses. The most common malignancy identified in
the present cohort was lymphoma and leukemia, and other few
miscellaneous malignancy as outlined in Table SI. Gafter-Gvili et al
(13) reported 14 cases of
malignancy out of a total of 84 positive on FDG PET/CT (14%); of
them, nine were non-Hodgkin's, two were Hodgkin's lymphoma, two
were lung cancer and one was a sarcoma. In the present population,
the prevalence of infectious disease was 51%, which is relatively
higher than that in previous studies (32-34).
According to several studies on FUO, the disease-associated FUO
differs between developed countries and other countries. The
percentages of classification of FUO were 19, 24, 12, 8 and 38% for
infection, non-infection inflammatory, cancer, various etiologies
and unknown, respectively in the developed countries, in contrast
to 43, 20, 14, 7 and 16%, respectively, in developing countries
(35). The main difference in cases
of FUO between developed countries and developing countries is the
high incidence of infectious disease; for instance, infectious
disease was the most common cause of FUO in Iran (14) and Pakistan, in particular
tuberculosis (15). The usefulness
of PET/CT in the diagnostic process of FUO is also debatable. It is
unknown whether only the true-positive findings can guide the final
diagnosis or whether true-negative PET/CT results may rule out
infection, inflammation or malignancies (36).
In contrast to a previous study, in which age >50
years, CRP level >30 mg/l and absence of fever were predictive
of true-positive 18FDG PET/CT results (37), the present study revealed no
statistically significant association between PET/CT results and
age, sex, WBC, CRP, ESR, LDH or ferritin levels among different
diagnostic groups. This lack of association may be due to the wide
variety of disease distribution and prevalence in FUO. In a
previous study of more specific inflammatory diseases, such as
rheumatoid arthritis, an association existed between CRP levels and
18FDG uptake (38). When
searching for clinical and laboratory tests associated with
true-positive PET/CT results, elevated WBC counts and elevated
serum levels of ferritin were associated with infection (P=0.018
and P=0.034, respectively) in the present study. Conversely, a
previous study revealed no significant association between WBC
values and 18FDG PET/CT scan results, the clinical
impact of 18FDG PET/CT or the provision of additional
information. Other studies showed that anemia, lymphadenopathy and
male sex correlated with diagnostic 18FGD PET/CT results
(13,23).
A significant number of false-positive results were
reported in the present patients (23%), which reduced the positive
predictive value to 68% and the overall diagnostic value in the
study to 58%. This observation was most likely related to the
normal physiological distribution of 18FDG (in the
kidney, urinary bladder, and small and large intestines). The
discrimination between pathological and normal physiological uptake
in such organs is difficult, which may explain the relatively high
number of false-positives in the present study. In addition,
18FDG uptake in the bone marrow and lymph nodes may be
remarkable. Some investigators have suggested reclassifying
18FDG uptake in the setting of FUO as a nonspecific sign
of inflammation and considering the scan in such cases a true
negative. This reclassification could greatly improve the positive
predictive value and accuracy (39). Several issues may cause
false-negative findings as well. For instance, small structures are
not readily identified with PET/CT, as these small structures (such
as temporal arteries) are beyond the resolution of PET/CT. The
detection limit is ~10 mm. Furthermore, certain cancer types, such
as prostate carcinoma and hepatocellular carcinoma, are not very
FDG-avid (40).
Multiple previous studies have reported the value of
18FDG PET/CT. However, comparing these studies is
difficult, since the majority of these studies (including the
present study) were retrospective with different inclusion and
exclusion criteria with a possibility of selection bias. In
addition, patients who undergo normal conventional imaging are more
likely to have PET/CT scans than patients with positive
conventional imaging results. In addition, certain studies included
immunocompromised patients and comparing these patients with
non-immunocompromised patients is difficult (41). Furthermore, in most studies, the
definition of FUO was unspecified (42,43).
One meta-analysis determined that only a true-positive scan is
helpful in diagnoses (44). In the
present study, 51 patients (49%) had true-positive scans. However,
this diagnostic approach has been questioned in a more recent
meta-analysis, which suggested that true-negative scans must also
be considered helpful, since patients with true-negative scans tend
to have favorable prognoses and high spontaneous remission rates
(45). Large, prospective,
multicenter studies are needed to better investigate the role and
value of 18FDG PET/CT in patients with FUO.
The present study has certain important strengths
and limitations. The study was a retrospective, small,
single-tertiary care center study, and thus, the possibility of
referral bias cannot be excluded. There was no structured protocol
for a work-up of FUO. Both the diagnostic workup before
18FDG PET/CT and the timing of the scan itself were
performed according to the preference of the referring physicians.
The significant variations among patients may have affected the
disease prevalence and diagnostic accuracy of the test, which is
one limitation of the study; the specificity was relatively low,
only 29%, most likely due to heterogeneity of the population of the
present study. The gold standard approach for patients with FUO/IUO
is not well defined because of different patient populations among
studies and the wide variety of etiologies. Finally, another
limitation is that the cost of FDG PET/CT is relatively high and
there is limited availability.
In conclusion, the present findings demonstrated
that 18FDG PET/CT substantially contributed to the
establishment of a final diagnosis of FUO in a high percentage of
patients (72%). 18FDG PET/CT can detect metabolically
active foci that may indicate infection, malignancies and
inflammatory noninfectious processes, all of which may be the
underlying etiology of the fever. PET/CT may be helpful by
eliminating additional examinations that rule out focal processes;
however, identifying focal 18FDG activity may indicate
false-positive findings and initiate additional examinations. Based
on the present results and previous studies, it appears that
18FDG PET/CT scans have a potential role in the initial
diagnostic workup for investigation of the etiology of FUO.
However, larger, prospective, multicenter studies with more
specific referral criteria are warranted to better investigate the
role and cost-effectiveness of 18FDG PET/CT scans in the
management of FUO.
Supplementary Material
Final diagnosis based on PET/CT
findings (true-positive group).
Acknowledgements
Part of this work was presented as an oral abstract
presentation (abstract no. RPS 2606-6) at the European Congress of
Radiology (July 13-July 17), Vienna, Austria on 17. July 2022.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
AF conceived the study, wrote the draft, prepared
the figures and tables, and reviewed and edited the final
manuscript. RB collected and analyzed data and prepared the draft
of the manuscript. AF and RB confirm the authenticity of all the
raw data. AA analyzed data and wrote, reviewed and edited the final
manuscript. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
All procedures were performed in line with the
ethical standards of the institutional research committee and
conform to the 1964 Helsinki Declaration and its later amendments
or comparable ethical standards. The study was conducted at the
King Faisal Specialist Hospital and Research Centre (Riyadh, Saudi
Arabia) after obtaining ethical approval from the Institutional
Review Board on 11/01/2021 (approval reference no. 2211019). The
consent to participate was waived by the ethics committee.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gaeta GB, Fusco FM and Nardiello S: Fever
of unknown origin: A systematic review of the literature for
1995-2004. Nuc Med Commun. 27:205–211. 2006.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Knockaert DC, Vanderschueren S and
Blockmans D: Fever of unknown origin in adults: 40 Years on. J
Intern Med. 253:263–275. 2003.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Bleeker-Rovers CP, Vos FJ, de Kleijn EMHA,
Mudde AH, Dofferhoff TS, Richter C, Smilde TJ, Krabbe PFM, Oyen WJG
and van der Meer JWM: A prospective multicenter study on fever of
unknown origin: The yield of a structured diagnostic protocol.
Medicine (Baltimore). 86:26–38. 2007.PubMed/NCBI View Article : Google Scholar
|
|
4
|
de Kleijn EM, van Lier HJ and van der Meer
JW: Fever of unknown origin (FUO). II. Diagnostic procedures in a
prospective multicenter study of 167 patients. The Netherlands FUO
study group. Medicine (Baltimore). 76:401–414. 1997.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Vanderschueren S, Knockaert D,
Adriaenssens T, Demey W, Durnez A, Blockmans D and Bobbaers H: From
prolonged febrile illness to fever of unknown origin: The challenge
continues. Arch Intern Med. 163:1033–1041. 2003.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Vanderschueren S, Del Biondo E, Ruttens D,
Van Boxelaer I, Wauters E and Knockaert DD: Inflammation of unknown
origin versus fever of unknown origin: Two of a kind. Eur Intern
Med. 20:415–418. 2009.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Mansueto P, Di Lorenzo G, Rizzo M, Di Rosa
S, Vitale G, Rini G, Mansueto S and Affronti M: Fever of unknown
origin in a Mediterranean survey from a division of internal
medicine: Report of 91 cases during a 12-year-period (1991-2002).
Intern Emerg Med. 3:219–225. 2008.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Jaruskova M and Belohlavek O: Role of
FDG-PET and PET/CT in the diagnosis of prolonged febrile states.
Eur J Nucl Med Mol Imaging. 33:913–918. 2006.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Mourad O, Palda V and Detsky AS: A
comprehensive evidence-based approach to fever of unknown origin.
Arch Intern Med. 163:545–551. 2003.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Dong MJ, Zhao K, Liu ZF, Wang GL, Yang SY
and Zhou GJ: A meta-analysis of the value of
fluorodeoxyglucose-PET/PET-CT in the evaluation of fever of unknown
origin. Euro J Rad. 80:834–844. 2011.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Meller J, Sahlmann CO and Scheel AK:
18F-FDG PET and PET/CT in fever of unknown origin. J Nuc Med.
48:35–45. 2007.PubMed/NCBI
|
|
12
|
Buch-Olsen KM, Andersen RV, Hess S, Braad
PE and Schifter S: 18F-FDG-PET/CT in fever of unknown origin:
Clinical value. Nuc Med Commun. 35:955–960. 2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Gafter-Gvili A, Raibman S, Grossman A,
Avni T, Paul M, Leibovici L, Tadmor B, Groshar D and Bernstine H:
[18F]FDG-PET/CT for the diagnosis of patients with fever of unknown
origin. QJM. 108:289–298. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Alavi SM, Nadimi M and Zamani GA: Changing
pattern of infectious etiology of fever of unknown origin (FUO) in
adult patients in Ahvaz, Iran. Caspian J Intern Med. 4:722–726.
2013.PubMed/NCBI
|
|
15
|
Mahmood K, Akhtar T, Naeem M, Talib A,
Haider I and Siraj-Us-Salikeen : Fever of unknown origin at a
teritiary care teaching hospital in Pakistan. Southeast Asian J
Trop Med Public Health. 44:503–511. 2013.PubMed/NCBI
|
|
16
|
Takeuchi M, Nihashi T, Gafter-Gvili A,
García-Gómez FJ, Andres E, Blockmans D, Iwata M and Terasawa T:
Association of 18F-FDG PET or PET/CT results with spontaneous
remission in classic fever of unknown origin: A systematic review
and meta-analysis. Medicine (Baltimore). 97(e12909)2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Wright WF, Kandiah S, Brady R, Shulkin BL,
Palestro CJ and Jain SK: Nuclear medicine imaging tools in fever of
unknown origin: Time for a revisit and appropriate use criteria.
Clin Infect Dis. 78:1148–1153. 2024.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Buchrits S, Gafter-Gvili A, Eynath Y,
Bernstine H, Guz D and Avni T: The yield of F18 FDG
PET-CT for the investigation of fever of unknown origin, compared
with diagnostic CT. Euro J Intern Med. 93:50–56. 2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Eynath Y, Halperin E, Buchrits S,
Gafter-Gvili A, Bernstine H, Catalano O and Avni T: Predictors for
spontaneous resolution of classical FUO in patients undergoing
PET-CT. Intern Emerg Med. 18:367–374. 2023.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Chen J, Xing M, Xu D, Xie N, Zhang W, Ruan
Q and Song J: Diagnostic models for fever of unknown origin based
on 18F-FDG PET/CT: A prospective study in China. EJNMMI
Res. 12(69)2022.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Hess S, Noriega-Álvarez E, Leccisotti L,
Treglia G, Albano D, Roivainen A, Glaudemans AWJM and Gheysens O:
EANM consensus document on the use of [18F]FDG PET/CT in
fever and inflammation of unknown origin. Eur J Nucl Med Mol
Imaging. 51:2597–2613. 2024.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Balink H, Collins J, Bruyn GA and Gemmel
F: F-18 FDG PET/CT in the diagnosis of fever of unknown origin.
Clin Nucl Med. 34:862–868. 2009.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Crouzet J, Boudousq V, Lechiche C, Pouget
JP, Kotzki PO, Collombier L, Lavigne JP and Sotto A: Place of
(18)F-FDG-PET with computed tomography in the diagnostic algorithm
of patients with fever of unknown origin. Eur J Clin Microbiol
Infect Dis. 31:1727–1733. 2012.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Ergül N, Halac M, Cermik TF, Ozaras R,
Sager S, Onsel C and Uslu I: The diagnostic role of FDG PET/CT in
patients with fever of unknown origin. Mol Imaging Radionucl Ther.
20:19–25. 2011.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Federici L, Blondet C, Imperiale A,
Sibilia J, Pasquali JL, Pflumio F, Goichot B, Blaison G, Weber JC,
Christmann D, et al: Value of (18)F-FDG-PET/CT in patients with
fever of unknown origin and unexplained prolonged inflammatory
syndrome: A single centre analysis experience. Inte J Clin Pract.
64:55–60. 2010.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Ferda J, Ferdová E, Záhlava J, Matejovic M
and Kreuzberg B: Fever of unknown origin: A value of
(18)F-FDG-PET/CT with integrated full diagnostic isotropic CT
imaging. Euro J Radiol. 73:518–525. 2010.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Kei PL, Kok TY, Padhy AK, Ng DC and Goh
AS: [18F] FDG PET/CT in patients with fever of unknown origin: A
local experience. Nucl Med Commun. 31:788–792. 2010.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Keidar Z, Gurman-Balbir A, Gaitini D and
Israel O: Fever of unknown origin: The role of 18F-FDG PET/CT. J
Nucl Med. 49:1980–1985. 2008.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Kim YJ, Kim SI, Hong KW and Kang MW:
Diagnostic value of 18F-FDG PET/CT in patients with fever of
unknown origin. Intern Med J. 42:834–837. 2012.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Manohar K, Mittal BR, Jain S, Sharma A,
Kalra N, Bhattacharya A and Varma S: F-18 FDG-PET/CT in evaluation
of patients with fever of unknown origin. Jpn J Radiol. 31:320–327.
2013.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Pedersen TI, Roed C, Knudsen LS, Loft A,
Skinhoj P and Nielsen SD: Fever of unknown origin: A retrospective
study of 52 cases with evaluation of the diagnostic utility of
FDG-PET/CT. Scand J Infect Dis. 44:18–23. 2012.PubMed/NCBI View Article : Google Scholar
|
|
32
|
De Kleijn EM, Vandenbroucke JP and van der
Meer JW: Fever of unknown origin (FUO). I A. prospective
multicenter study of 167 patients with FUO, using fixed
epidemiologic entry criteria. The Netherlands FUO study group.
Medicine (Baltimore). 76:392–400. 1997.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Fusco FM, Pisapia R, Nardiello S, Cicala
SD, Gaeta GB and Brancaccio G: Fever of unknown origin (FUO): Which
are the factors influencing the final diagnosis? A 2005-2015
systematic review. BMC Infect Dis. 19(653)2019.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Torné Cachot J, Baucells Azcona JM, Blanch
Falp J and Camell Ilari H: Classic fever of unknown origin:
Analysis of a cohort of 87 patients according to the definition
with qualitative study criterion. Med Clin (Barc). 156:206–213.
2021.PubMed/NCBI View Article : Google Scholar : (In English,
Spanish).
|
|
35
|
Minamimoto R: Optimal use of the
FDG-PET/CT in the diagnostic process of fever of unknown origin
(FUO): A comprehensive review. Jpn J Radiol. 40:1121–1137.
2022.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Hess S: FDG-PET/CT in fever of unknown
origin, bacteremia, and febrile neutropenia. PET Clin. 15:175–185.
2020.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Schönau V, Vogel K, Englbrecht M, Wacker
J, Schmidt D, Manger B, Kuwert T and Schett G: The value of
18F-FDG-PET/CT in identifying the cause of fever of
unknown origin (FUO) and inflammation of unknown origin (IUO): Data
from a prospective study. Ann Rheum Dis. 77:70–77. 2018.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Kubota K, Ito K, Morooka M, Mitsumoto T,
Kurihara K, Yamashita H, Takahashi Y and Mimori A: Whole-body
FDG-PET/CT on rheumatoid arthritis of large joints. Ann Nucl Med.
23:783–791. 2009.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Kubota K, Nakamoto Y, Tamaki N, Kanegae K,
Fukuda H, Kaneda T, Kitajima K, Tateishi U, Morooka M, Ito K, et
al: FDG-PET for the diagnosis of fever of unknown origin: A
Japanese multi-center study. Ann Nucl Med. 25:355–364.
2011.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Long NM and Smith CS: Causes and imaging
features of false positives and false negatives on F-PET/CT in
oncologic imaging. Insights imaging. 2:679–698. 2011.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Pereira AMV, Husmann L, Sah BR, Battegay E
and Franzen D: Determinants of diagnostic performance of 18F-FDG
PET/CT in patients with fever of unknown origin. Nucl Med Commun.
37:57–65. 2016.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Sheng JF, Sheng ZK, Shen XM, Bi S, Li JJ,
Sheng GP, Yu HY, Huang HJ, Liu J, Xiang DR, et al: Diagnostic value
of fluorine-18 fluorodeoxyglucose positron emission
tomography/computed tomography in patients with fever of unknown
origin. Europ J Intern Med. 22:112–116. 2011.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Kouijzer IJE, Mulders-Manders CM,
Bleeker-Rovers CP and Oyen WJG: Fever of Unknown Origin: The Value
of FDG-PET/CT. Semin in Nucl Med. 48:100–107. 2018.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Besson FL, Chaumet-Riffaud P, Playe M,
Noel N, Lambotte O, Goujard C, Prigent A and Durand E: Contribution
of (18)F-FDG PET in the diagnostic assessment of fever of unknown
origin (FUO): A stratification-based meta-analysis. Eur J Nucl Med
Mol Imaging. 43:1887–1895. 2016.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Betrains A, Moreel L, Wright WF, Blockmans
D and Vanderschueren S: Negative 18F-FDG-PET imaging in fever and
inflammation of unknown origin: now what? Intern Emerg Med.
18:1865–1869. 2023.PubMed/NCBI View Article : Google Scholar
|