Introduction
Upper tract urothelial carcinoma (UTUC) is a rare
malignant disease of the urinary system, with a relatively higher
prevalence in Taiwan compared with other countries (1-3).
Due to the high risk of disease recurrence and progression, radical
nephroureterectomy (RNU) is considered the gold-standard treatment
for localized UTUC (4). Recent
evidence has shown that neoadjuvant and adjuvant systemic therapy
can improve outcomes in patients with UTUC who have unfavorable
pathological characteristics, including advanced tumor stage,
regional lymph node (LN) metastasis and lymphovascular invasion
(LVI) positivity (5,6). While pathological tumor stage, LN
status and LVI have been considered the most important factors for
survival in patients with UTUC, these factors cannot provide
preoperative treatment planning. Therefore, identifying
preoperative prognostic factors is clinically valuable to make more
precise pre-treatment assessments, such as whether to use systemic
therapy before or after surgery, and to improve postoperative
surveillance.
Aside from the conventional Tumor-Node-Metastasis
(TNM) system, evidence suggests that systemic inflammation is also
strongly associated with cancer growth/development and progression,
and influences survival outcomes. Several clinical studies reported
that pre-operative peripheral blood inflammation biomarkers, such
as the neutrophil-lymphocyte ratio (NLR) (7,8), the
platelet-lymphocyte ratio (PLR) (9-11),
the monocyte-lymphocyte ratio (MLR) (11-13)
and the systemic immune-inflammation index (SII; neutrophil x
platelet/lymphocyte) (14,15) were associated with prognosis in
several solid malignancies, including UTUC.
In addition, some studies reported that an elevated
red cell distribution width (RDW) (16,17) or
a reduced pretreatment lymphocyte percentage (LYM%) (18) was associated with poor survival.
While increased RDW was considered to indirectly reflect
progressive inflammation state, less circulating lymphocytes
implied reduced antitumor immunity. Nevertheless, to the best of
our knowledge, the clinical significance of integrating RDW and
LYM% has not yet been evaluated in UTUC. Combining RDW and LYM%
provides a better indicator than using RDW or LYM% alone, as it
effectively reflects the balance between tumor inflammation and
antitumor immunity. Therefore, the present study aimed to explore
the associations between the pre-treatment RDW-to-LYM% ratio and
clinicopathological parameters, and to identify the prognostic
value of this ratio in UTUC in clinical practice.
Patients and methods
Study populations and data
collection
The present study was approved by the Institutional
Review Board of National Cheng Kung University Hospital (Tainan,
Taiwan; approval no. NCKUH-B-ER-112-218). The cases of 625 patients
(mean age, 69.3±11.0 years) with UTUC who had received an RNU
between January 2008 and June 2020 were retrospectively analyzed.
RNU was performed based on standard procedures, and the regional
LNs were generally dissected if there was a preoperative
presentation of enlargement on imaging studies or intraoperative
findings of palpable nodes. In this study, exclusion criteria
included active infection status, a lack of differential count
information from preoperative complete blood counts (CBCs) 30 days
prior to surgery, bone or distant metastasis at the time of
diagnosis, other cancer diseases, current administration of
immunosuppressive agents and a postoperative follow-up duration of
<30 days. None of the patients received neo-adjuvant
chemotherapy, radiotherapy or any other antitumor therapy. Adjuvant
chemotherapy, consisting of at least 3 cycles of gemcitabine
(800-1,000 mg/m2) and cisplatin (35-70 mg/m2)
(or carboplatin; AUC, 4-6), was administered to patients with
pathological T stage (pT≥2) and over or pathological node
positivity (pN+) within 3 months of RNU.
Preoperative clinical and pathological data,
including sex, age, comorbidities (diabetes mellitus and
hypertension), symptoms (hydronephrosis and hematuria),
preoperative estimated glomerular filtration rate (eGFR), prior or
concomitant bladder urothelial carcinoma, tumor location (renal
pelvis, ureter or synchronous), tumor size, tumor necrosis, pT
stage, LN metastasis, tumor grade, LVI and CBC parameters
(neutrophil/monocyte/lymphocyte percentages, white blood cell
counts and platelet counts) were also recorded for further
analysis. The overall survival (OS) time was defined as the time
from RNU to death from any cause or the last follow-up. The
cancer-specific survival (CSS) time was defined as the time from
RNU until death due to UTUC. The progression-free survival (PFS)
time was defined as the time from RNU until disease progression,
including local recurrence or distant metastasis or death.
Furthermore, bladder or contralateral upper urinary tract relapse
was not defined as local recurrence. TNM classification was
determined according to American Joint Committee on Cancer staging,
7th edition (18), and pathological
grade was based on the 2004 World Health Organization
classification (19). Preoperative
eGFR was calculated with the Modification of Diet in Renal Disease
Study equation as follows: 186 x (serum creatinine)-1.154 x
(age)-0.203 x (0.742 if female) (19). Patients were considered to have
chronic kidney disease if they had an eGFR value of <60
ml/min/1.73 m2 or if they received regular dialysis.
Postoperative follow-up strategies included interval history
taking, physical examination, urinalysis, urine cytology, abdominal
ultrasonography and abdominal computed tomography every 6-12
months. Cystoscopy was performed every 3 months for the first 2
years, every 6 months for the next 2 years and annually
thereafter.
Statistical analysis
Clinical data, including continuous and categorical
variables, were analyzed using SPSS software (version 22.0; IBM
Corp.). Based on cancer-specific death as the endpoint, the optimal
cut-off value of the RDW-to-LYM% ratio was determined using a
receiver operating characteristic (ROC) curve analysis and Youden's
index. After all included patients were dichotomized into two
groups based on the cut-off value of the RDW-to-LYM% ratio,
Fisher's exact test and the χ2 test were used to compare
the differences in clinicopathological variables between the two
groups. Kaplan-Meier analysis was conducted to evaluate the
association between RDW-to-LYM% ratio and OS, CSS and PFS, and the
significant differences were determined using the log-rank test.
Univariate and multivariate Cox regression analyses were performed
to assess each variable for significance in terms of OS, CSS and
PFS. P<0.05 was considered to indicate a statistically
significant difference.
Results
Baseline characteristics of patients
with localized UTUC and high or low pretreatment RDW-to-LYM%
ratios
A total of 625 patients who received RNU for UTUC
were enrolled in this study, with 47.8 months as the median
follow-up time (Table I). In terms
of preoperative clinical baseline parameters, 330 (53%) patients
were >69 years old, 354 (57%) were female, 372 (60%) had chronic
kidney disease (eGFR <60 ml/min/1.73 m2), 361 (58%)
had underlying hypertension or diabetes mellitus, 543 (87%) had
microscopic or gross hematuria and 492 (79%) presented with
hydronephrosis (Table I). In terms
of pathological information, prior and concomitant bladder tumors
were noted in 92 (15%) and 121 (19%) patients, respectively, while
tumor location was in the renal pelvis in 284 (45%) patients, in
the ureter in 206 (33%) patients and in both locations in 135 (22%)
patients. pTis/a/1, T2 and T3/4 stages were found in 229 (37%), 122
(20%) and 274 (44%) patients, respectively, 38 (6%) had positive LN
metastasis and 595 (95%) had a high tumor grade. A total of 453
(72%) patients had larger tumor size (>2 cm), 181 (29%) had LVI,
122 (20%) had tumor necrosis and 61 (10%) received adjuvant
chemotherapy (Table I).
 | Table IAssociations between
clinicopathological characteristics and high (n=470) or low (n=155)
pre-treatment RDW-to-LYM% ratio in patients with upper tract
urothelial carcinoma. |
Table I
Associations between
clinicopathological characteristics and high (n=470) or low (n=155)
pre-treatment RDW-to-LYM% ratio in patients with upper tract
urothelial carcinoma.
| | RDW-to-LYM%
ratio | |
|---|
| Variables | All patients | Low (≤0.80) | High (>0.80) | P-value |
|---|
| Mean age ± SD,
years | 69.3±11.0 | 69.3±10.7 | 69.1±11.8 | |
| Median follow-up time
after surgery, months | 47.8 | 51.5 | 31.1 | |
| Age, n (%) | | | | 0.598 |
|
≤69
years | 295(47) | 219(47) | 76(49) | |
|
>69
years | 330(53) | 251(53) | 79(51) | |
| Sex, n (%) | | | | 0.969 |
|
Male | 271(43) | 204(43) | 67(43) | |
|
Female | 354(57) | 266(57) | 88(57) | |
| Renal function, n
(%) | | | | 0.005 |
|
Pre-eGFR ≥60
ml/min/1.73 m2 | 253(40) | 205(44) | 48(31) | |
|
Pre-eGFR
<60 ml/min/1.73 m2 | 372(60) | 265(56) | 107(69) | |
| HTN or DM, n
(%) | | | | 0.300 |
|
No | 264(42) | 193(41) | 71(46) | |
|
Yes | 361(58) | 277(59) | 84(54) | |
| Hematuria, n
(%) | | | | 0.522 |
|
No | 82(13) | 64(14) | 18(12) | |
|
Yes | 543(87) | 406(86) | 137(88) | |
| Hydronephrosis, n
(%) | | | | 0.363 |
|
No | 133(21) | 96(20) | 37(24) | |
|
Yes | 492(79) | 374(80) | 118(76) | |
| Previous BC, n
(%) | | | | 0.016 |
|
No | 533(85) | 410(87) | 123(79) | |
|
Yes | 92(15) | 60(13) | 32(21) | |
| Concomitant BC, n
(%) | | | | 0.010 |
|
No | 504(81) | 390(83) | 114(74) | |
|
Yes | 121(19) | 80(17) | 41(26) | |
| Tumor location, n
(%) | | | | 0.003 |
|
Pelvis | 284(45) | 210(45) | 74(48) | |
|
Ureter | 206(33) | 170(36) | 36(23) | |
|
Both | 135(22) | 90(19) | 45(29) | |
| Pathologic T stage,
n (%) | | | | <0.001 |
|
Tis/a/1 | 229(37) | 184(39) | 45(29) | |
|
T2 | 122(20) | 101(21) | 21(14) | |
|
T3/4 | 274(44) | 185(39) | 89(57) | |
| Lymph node status,
n (%) | | | | <0.001 |
|
N0 | 109(17) | 70(15) | 39(25) | |
|
Nx | 478(76) | 380(81) | 98(63) | |
|
N+ | 38(6) | 20(4) | 18(12) | |
| Tumor grade, n
(%) | | | | 0.290 |
|
Low | 30(5) | 25(5) | 5(3) | |
|
High | 595(95) | 445(95) | 150(97) | |
| Tumor size, n
(%) | | | | 0.045 |
|
≤2 cm | 172(28) | 139(30) | 33(21) | |
|
>2
cm | 453(72) | 331(70) | 122(79) | |
| Lymphovascular
invasion, n (%) | | | | <0.001 |
|
Absent | 444(71) | 351(75) | 93(60) | |
|
Present | 181(29) | 119(25) | 62(40) | |
| Tumor necrosis, n
(%) | | | | 0.070 |
|
Absent | 503(80) | 386(82) | 117(75) | |
|
Present | 122(20) | 84(18) | 38(25) | |
| Adjuvant
chemotherapy, n (%) | | | | 0.968 |
|
No | 564(90) | 424(90) | 140(90) | |
|
Yes | 61(10) | 46(10) | 15(10) | |
Subsequently, with cancer-specific death as the
endpoint, the optimal cut-off value of the pretreatment RDW-to-LYM%
ratio was determined as 0.80 using ROC analysis (Fig. S1). After stratifying the 625
patients with UTUC into high- and low-level RDW-to-LYM% ratios
(>0.80 and ≤0.80), the clinical and pathological characteristics
were compared between the two groups. As shown in Table I, patients with pre-existing renal
impairment, prior/concomitant bladder cancer, tumors located in
both the renal pelvis and ureter, advanced pT stage (≥T3), lymph
node metastasis, larger tumor size (>2 cm), and positive LVI
tended to have high-level RDW-to-LYM% ratios (all P<0.05).
Conversely, the differences in age, sex, underlying diseases
(diabetes mellitus or hypertension), preoperative clinical symptoms
(hematuria or hydronephrosis), tumor grade, tumor necrosis and
administration of adjuvant chemotherapy were not noted to be
significant between the two groups.
Association between pre-treatment
RDW-to-LYM% ratio and NOC disease and LVI
In the present study, 278 (44%) patients had NOC
disease and 181 (29%) were positive for LVI. Among them, 50%
(138/278) with NOC disease and 54% (98/181) who were positive for
LVI were classified as having a high-level RDW-to-LYM% ratio (data
not shown). In the pre-treatment model to predict NOC disease and
the presence of LVI, multivariate logistic regression analyses
revealed that a high-level RDW-to-LYM% ratio was significantly
associated with NOC disease [odds ratio (OR), 2.107; 95% confidence
interval (CI), 1.446-3.069; P<0.001] and positive LVI (OR,
1.978; 95% CI, 1.338-2.916; P<0.001) (Tables II and III). However, other preoperative
variables, including age, sex, renal function, underlying HTN or
DM, and hematuria/hydronephrosis and bladder cancer history, were
not associated.
| Table IIUnivariate and multivariate logistic
regression preoperative model analyses for prediction of NOC
disease (≥pT3 and/or positive lymph nodes) based on the
pre-treatment RDW-to-LYM% ratio. |
Table II
Univariate and multivariate logistic
regression preoperative model analyses for prediction of NOC
disease (≥pT3 and/or positive lymph nodes) based on the
pre-treatment RDW-to-LYM% ratio.
| | NOC disease |
|---|
| | Univariate | Multivariate |
|---|
| Parameter | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age at RNU | | | | |
|
>69 vs.
≤69 years | 0.955
(0.696-1.309) | 0.774 | 1.015
(0.731-1.410) | 0.929 |
| Sex | | | | |
|
Female vs.
male | 0.739
(0.537-1.016) | 0.063 | 0.731
(0.527-1.014) | 0.061 |
| Pre-eGFR | | | | |
|
<60 vs.
≥60 ml/min/1.73 m2 | 0.911
(0.661-1.256) | 0.570 | 0.882
(0.630-1.236) | 0.466 |
| DM or HTN | | | | |
|
Present vs.
absent | 0.934
(0.679-1.285) | 0.675 | 0.998
(0.716-1.390) | 0.998 |
| Previous BC | | | | |
|
Yes vs.
no | 0.773
(0.492-1.215) | 0.264 | 0727
(0.456-1.160) | 0.181 |
| Hematuria | | | | |
|
Present vs.
absent | 0.867
(0.544-1.380) | 0.547 | 0.816
(0.50-1.314) | 0.428 |
| Hydronephrosis | | | | |
|
Present vs.
absent | 0.862
(0.587-1.266) | 0.450 | 0.864
(0.581-1.283) | 0.469 |
| RDW-to-LYM%
ratio | | | | |
|
High vs.
low | 2.005
(1.388-2.897) | <0.001 | 2.107
(1.446-3.069) | <0.001 |
| Table IIIUnivariate and multivariate logistic
regression preoperative model analyses for prediction of presence
of LVI based on pre-treatment RDW-to-LYM% ratio. |
Table III
Univariate and multivariate logistic
regression preoperative model analyses for prediction of presence
of LVI based on pre-treatment RDW-to-LYM% ratio.
| | LVI |
|---|
| | Univariate | Multivariate |
|---|
| Parameter | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age at RNU | | | | |
|
>69 vs.
≤69 years | 0.923
(0.653-1.305) | 0.650 | 1.036
(0.697-1.539) | 0.861 |
| Sex | | | | |
|
Female vs.
male | 0.814
(0.575-1.153) | 0.246 | 0.799
(0.560-1.140) | 0.216 |
| Pre-eGFR | | | | |
|
<60 vs.
≥60 ml/min/1.73 m2 | 1.009
(0.709-1.435) | 0.961 | 0.965
(0.667-1.395) | 0.457 |
| DM or HTN | | | | |
|
Present vs.
absent | 0.952
(0.671-1.350) | 0.783 | 1.020
(0.711-1.464) | 0.914 |
| Previous BC | | | | |
|
Yes vs.
no | 1.087
(0.671-1.760) | 0.736 | 1.015
(0.617-1.667 | 0.955 |
| Hematuria | | | | |
|
Present vs.
absent | 0.806
(0.491-1.326) | 0.396 | 0.744
(0.448-1.236) | 0.254 |
| Hydronephrosis | | | | |
|
Present vs.
absent | 0.747
(0.496-1.126) | 0.163 | 0.742
(0.487-1.130) | 0.164 |
| RDW-to-LYM%
ratio | | | | |
|
High vs.
low | 1.966
(1.341-2.883) | <0.001 | 1.978
(1.338-2.916) | <0.001 |
Association between pre-treatment
RDW-to-LYM% ratio and poor survival outcomes
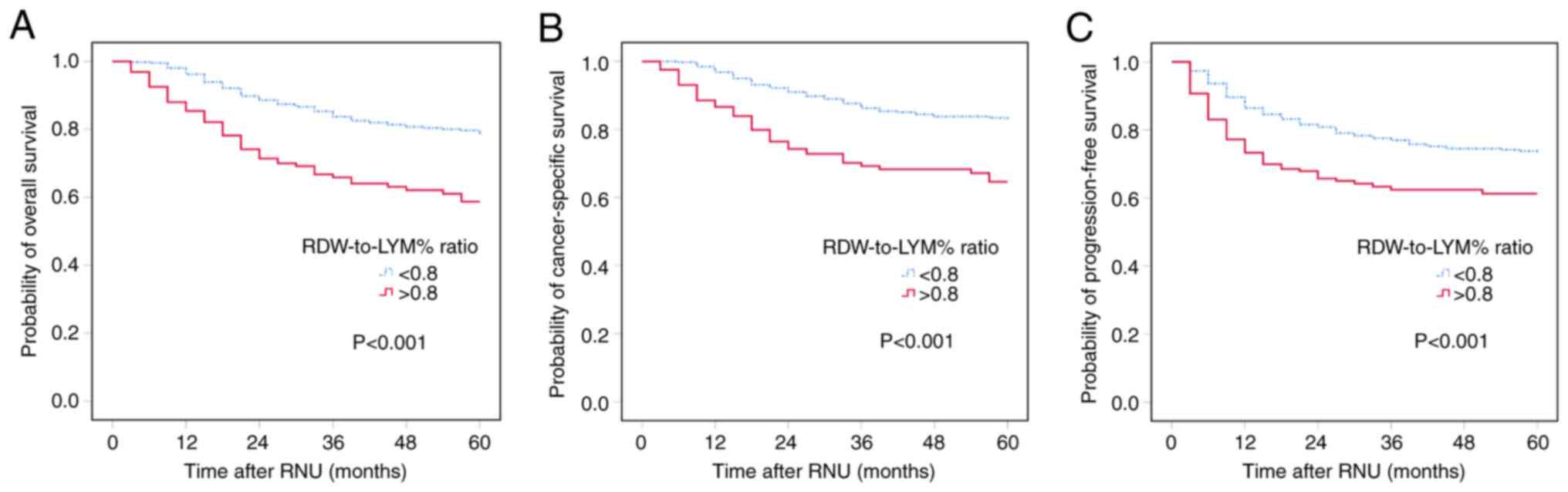
Kaplan-Meier analysis was performed to evaluate the
associations between pre-treatment RDW-to-LYM% ratio and OS, CSS
and PFS. The results showed that the high-level RDW-to-LYM% ratio
was significantly associated with worse OS, CSS and PFS, with all
P<0.001 for all comparisons (Fig.
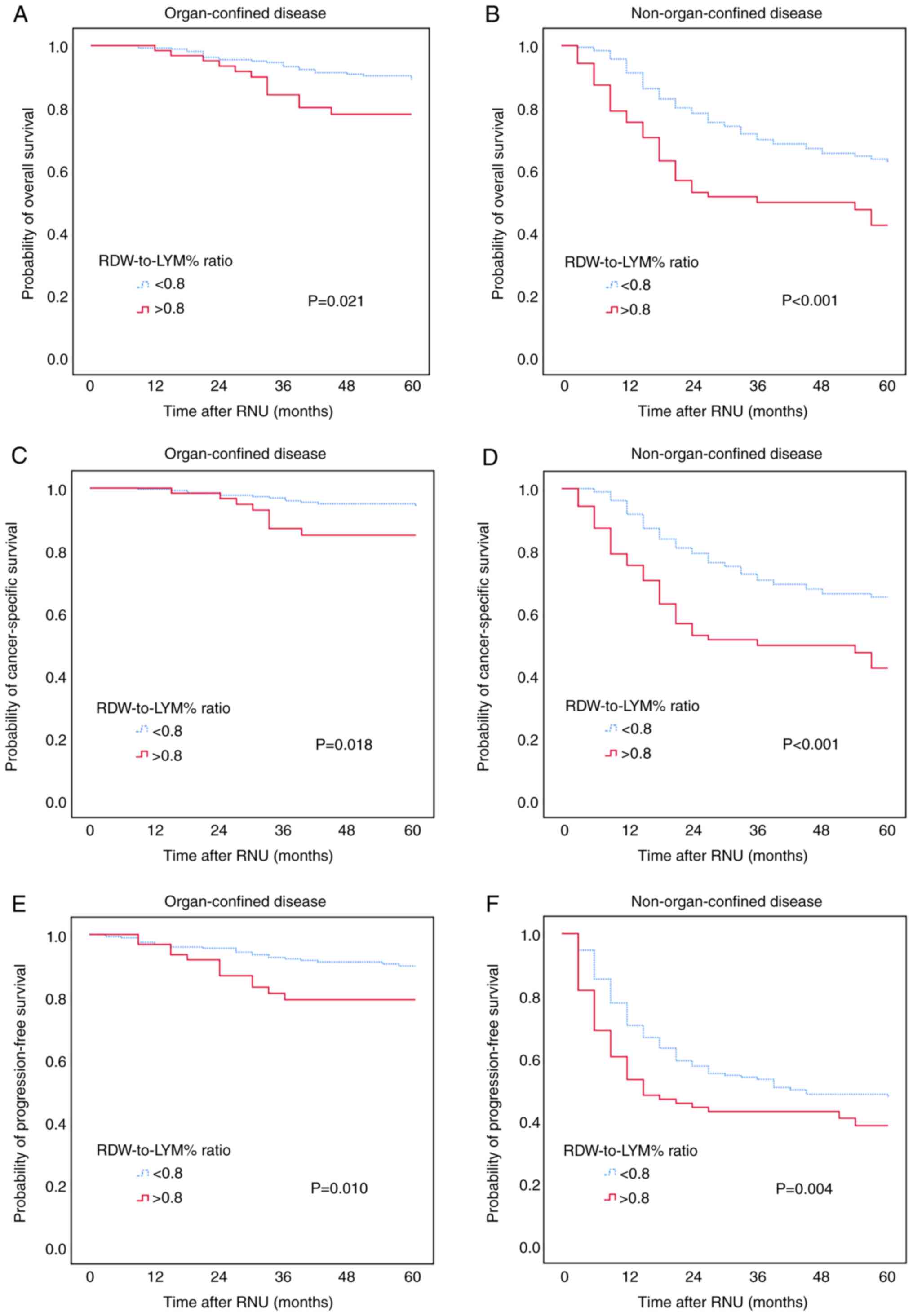
1). The effect of the pre-treatment RDW-to-LYM% ratio on OS,
CSS and PFS in different pathological tumor stages was also
assessed. The patients were sub-grouped into organ-confined and NOC
UTUC. Kaplan-Meier analysis showed that a high-level RDW-to-LYM%
ratio was associated with significantly shorter OS, CSS and PFS
times (all P<0.001) compared with a low RDW-to-LYM% ratio in
both organ-confined and NOC disease (Fig. 2).
Furthermore, a multivariate Cox regression analysis
was conducted to determine the prognostic factors that
independently influenced survival in the patients. From the results
of the multivariate analyses (Table
IV), old age, male, tumor localizing in the ureter or both
ureter and pelvis, advanced pT stage (pT3/4), pN+, positive LVI and
high RDW-to-LYM% ratio significantly conferred the negative impacts
on OS and CSS. Regarding PFS, the high RDW-to-LYM% ratio was still
an independent predicting factor, and other significant factors
included older age, sex, tumors localizing in the ureter or both
ureter and pelvis, advanced pT3/4 stage, LN-positive status and the
presence of LVI.
| Table IVMultivariate analyses for OS, CSS and
PFS. |
Table IV
Multivariate analyses for OS, CSS and
PFS.
| | OS | CSS | PFS |
|---|
| Parameter | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age at RNU years
(continuous variable) | 1.025
(1.009-1.043) | 0.003 | 1.023
(1.005-1.040) | 0.011 | 1.015
(1.001-1.029) | 0.030 |
| Sex | | | | | | |
|
Female vs.
male | 0.627
(0.453-0.868) | 0.005 | 0.575
(0.408-0.810) | 0.002 | 0.729
(0.542-0.979) | 0.036 |
| Renal function | | | | | | |
|
≤60 vs.
>60 ml/min/1.73 m2 | 1.109
(0.762-1.615) | 0.589 | 1.021
(0.691-1.508) | 0.918 | 0.934
(0.673-1.269) | 0.683 |
| HTN or DM | | | | | | |
|
Yes vs.
no | 1.374
(0.972-1.941) | 0.072 | 1.330
(0.927-1.909) | 0.121 | 1.302
(0.967-1.752) | 0.082 |
| Previous BC | | | | | | |
|
Yes vs.
no | 0.958
(0.602-1.525) | 0.905 | 0.889
(0.534-1.480) | 0.651 | 1.196
(0.811-1.765) | 0.367 |
| Concomitant BC | | | | | | |
|
Yes vs.
no | 1.024
(0.695-1.509) | 0.856 | 1.047
(0.699-1.570) | 0.823 | 1.131
(0.810-1.578) | 0.471 |
| Hydronephrosis | | | | | | |
|
Present vs.
absent | 0.824
(0.535-1.269) | 0.380 | 0.826
(0.524-1.302) | 0.410 | 0.784
(0.545-1.128) | 0.190 |
| Hematuria | | | | | | |
|
Present vs.
absent | 1.157
(0.703-1.902) | 0.567 | 1.126
(0.673-1.886) | 0.652 | 1.013
(0.661-1.552) | 0.954 |
| Tumor location | | | | | | |
|
Ureter vs.
renal pelvis | 1.694
(1.068-2.687) | 0.025 | 1.730
(1.065-2.809) | 0.027 | 1.588
(1.079-2.337) | 0.019 |
|
Both vs.
renal pelvis | 2.197
(1.462-3.302) | <0.001 | 2.170
(1.412-3.335) | <0.001 | 1.843
(1.290-2.632) | 0.001 |
| Pathological T
stage | | | | | | |
|
T2 vs.
Tis/a/1 | 1.398
(0.777-2.516) | 0.263 | 3.194
(1.501-6.795) | 0.003 | 1.430
(0.994-2.409) | 0.179 |
|
T3/4 vs.
Tis/a/1 | 2.730
(1.667-4.469) | <0.001 | 6.209
(3.135-12.299) | <0.001 | 3.242
(2.111-4.979) | <0.001 |
| Lymph node
stage | | | | | | |
|
Nx vs.
N0 | 0.907
(0.593-1.387) | 0.651 | 0.804
(0.520-1.244) | 0.327 | 1.079
(0.742-1.569) | 0.689 |
|
N+ vs.
N0 | 2.948
(1.656-5.246) | <0.001 | 2.803
(1.569-5.009) | 0.001 | 2.994
(1.801-4.997) | <0.001 |
| Tumor grade | | | | | | |
|
High vs.
low | 1.737
(0.521-5.793) | 0.369 | 4.355
(0.567-33.426) | 0.157 | 1.369
(0.423-4.429) | 0.600 |
| Tumor size | | | | | | |
|
>2 vs. ≤2
cm | 1.218
(0.762-1.948) | 0.410 | 1.180
(0.711-1.959) | 0.453 | 1.429
(0.960-2.126) | 0.078 |
| Lymphovascular
invasion | | | | | | |
|
Present vs.
absent | 1.798
(1.235-2.619) | 0.002 | 1.785
(1.208-2.638) | 0.004 | 1.933
(1.403-2.662) | <0.001 |
| Tumor necrosis | | | | | | |
|
Present vs.
absent | 1.321
(0.898-1.944) | 0.157 | 1.260
(0.841-1.89) | 0.263 | 1.089
(0.7776-1.527) | 0.622 |
| Adjuvant
chemotherapy | | | | | | |
|
Yes vs.
no | 0.590
(0.330-1.056) | 0.076 | 0.545
(0.302-1.014) | 0.064 | 1.012
(0.957-1.577) | 0.957 |
| RDW-to-LYM%
ratio | | | | | | |
|
High
(>0.80) vs. low (<0.80) | 2.046
(1.441-2.906) | <0.001 | 2.041
(1.415-2.945) | <0.001 | 1.502
(1.105-2.042) | 0.009 |
Development of a nomogram that
includes pre-treatment RDW-to-LYM% ratio to predict survival
outcomes
Considering all independent variables for survival
outcomes in multivariate analyses, a prognostic nomogram was
developed for OS, CSS and PFS in patients with UTUC after RNU
(Fig. 3). This nomogram
incorporated pre-treatment RDW-to-LYM% ratio with age, sex, tumor
location, pT stage, LN status and LVI. According to this nomogram,
the 1-, 3- and 5-year survival rates can be easily obtained.
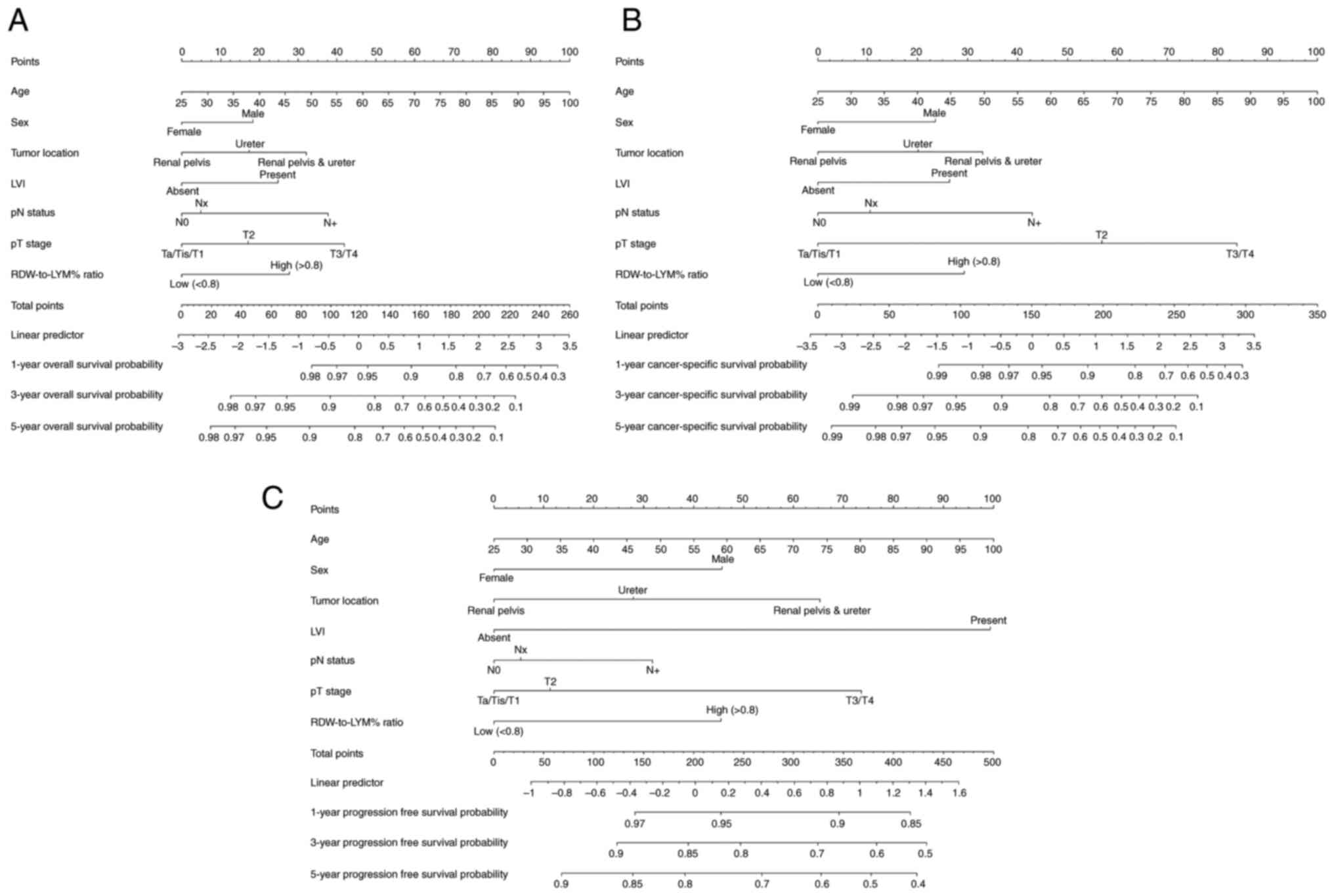 | Figure 3Nomograms for predicting OS, CSS and
PFS. Nomograms based on the independent prognostic factors for the
prediction of 1-, 3- and 5-year (A) OS, (B) CSS and (C) PFS rates.
LVI, lymphovascular invasion; RDW-to-LYM% ratio, red cell
distribution width to lymphocyte percentage ratio; OS, overall
survival; CSS, cause-specific survival; PFS, progression-free
survival; pN, pathological node; pT, pathological tumor. |
Discussion
Various predictive factors derived from blood-based
inflammatory immune cells have been used to assess the prognosis of
patients with UTUC undergoing RNU. For example, RDW, lymphocyte
counts, NLR, PLR, MLR, lymphocyte-to-monocyte ratio and SII, among
others, have been demonstrated to predict oncological outcomes in
patients with non-metastatic UTUC (7,9,11,13,18).
Previous studies reported that the RDW-to-lymphocyte count ratio
was associated with prognosis in cutaneous malignant melanoma
(20) and renal cell carcinoma
(21). Simultaneously assessing RDW
and LYM% for patients with cancer could provide information about
systemic inflammation and immunity in the presence of tumors.
However, to the best of our knowledge, the combination of RDW and
LYM% has not been evaluated for predicting oncological outcomes in
patients with UTUC after RNU.
In the present study, an increased RDW-to-LYM% ratio
(>0.80) was markedly associated with more aggressive
pathological phenotypes, including synchronous involvement of the
ureter and pelvis, advanced tumor stage, regional LN metastasis and
positive LVI, in patients with UTUC. Patients with renal impairment
or previous/concomitant BC also tended to have a high RDW-to-LYM%
ratio. In the preoperative model, a relatively higher RDW-to-LYM%
ratio had the potency to predict NOC disease and the presence of
LVI. Furthermore, the high-level RDW-to-LYM% ratio was associated
with decreased OS, CSS and PFS times, particularly in NOC disease.
Furthermore, in the present cohort, <20% of patients with
localized advanced (≥pT2 or pN+) UTUC received adjuvant
chemotherapy, as there was no significant evidence on the survival
benefit of adjuvant platinum-based chemotherapy before the POUT
trial (5). In the present study,
adjuvant chemotherapy possibly provided a trend in survival
benefits, but did not reach significance. Notably, the RDW-to-LYM%
ratio was identified as an independent prognostic factor for
predicting worse outcomes, which could potentially aid in treatment
decision-making, such as administering systemic therapy before or
after surgery. To the best of our knowledge, the present study is
the first to describe the prognostic significance of the
pre-treatment RDW-to-LYM% ratio in UTUC.
Tumor progression and metastases are closely
associated with systemic inflammation (22,23).
There is a mutually promoting interaction between inflammation and
tumor progression. Inappropriate inflammation precedes and promotes
tumor development/growth and progression, and tumor progression
induces and drives inflammatory reactions. Numerous clinical
studies in various cancer types, including breast, esophageal,
gastrointestinal, pancreatic and upper urinary tract cancer, found
that changes in peripheral blood immune cell numbers or proportions
indirectly denoted tumor-related inflammation status (7-15).
According to previous studies, peripheral neutrophils, monocytes or
platelets were considered to facilitate tumor malignant behaviors,
whereas lymphocytes were responsible for weakening tumor cell
viability. Decreased lymphocyte counts (abnormally low absolute
lymphocyte counts) were associated with poor outcomes in some solid
cancer types, such as oropharyngeal, cervical, lung and breast
cancer (24-27).
Furthermore, several studies adopted other blood parameters
unrelated to immune cells, such as RDW or C-reactive protein (CRP),
as inflammation biomarkers for predicting outcomes in patients with
cancer (16,17,28-31).
Increasing preoperative RDW was reported to negatively affect
prognosis in bladder and prostate cancer (16,17,28).
RDW was used to diagnose anemia, and indirectly reflected oxidative
stress and inflammation status (32). RDW was also closely linked to
various inflammatory cytokines, such as interleukin-6, enterococcal
surface protein and CRP (33,34).
Elevated RDW may imply an increase in systemic inflammation, thus
potentially enhancing tumor aggressiveness and resulting in tumor
progression and metastasis.
In the present study, increased RDW combined with
decreased LYM% was significantly associated with poorer OS, CSS and
PFS times in patients with UTUC after RNU, particularly in those
with NOC disease. ROC analysis revealed that on their own, RDW or
LYM% did not better predict survival outcomes compared with the
RDW-to-LYM% ratio (Fig. S1). The
pretreatment RDW-to-LYM% ratio as a combination marker is derived
from RDW and LYM% values. Given that RDW and LYM% are pro-tumor and
antitumor inflammation markers, respectively, the RDW-to-LYM% ratio
could reflect the imbalance between pro- and anti-tumor immunity,
rather than RDW or LYM% alone. An increase in the RDW-to-LYM% ratio
value is mathematically attributed to relatively increased RDW
and/or decreased LYM%. As aforementioned, increased RDW levels may
indicate an increase in the systemic inflammation state, and a
reduced lymphocyte distribution may imply a weak immune response to
the tumor. We suggest that an elevated RDW-to-LYM% ratio in
patients UTUC may reflect a clinical state with more inflammatory
burden and less antitumor immunity. As such, patients with a higher
RDW-to-LYM% ratio are at risk of worse survival times and disease
progression. The present study emphasized that the pre-treatment
RDW-to-LYM% ratio remained statistically significant for predicting
OS, CSS and PFS after adjusting several important and relevant risk
factors, including tumor location, pT stage, LN status and LVI.
Furthermore, the pretreatment RDW-to-LYM% ratio had the potency to
predict NOC and the presence of LVI. Since the clinical staging of
UTUC has been dependent on imaging and ureterorenoscopy biopsy to
date, the pretreatment RDW-to-LYM% ratio will provide additional
assistance to improve the accuracy of the clinical staging of
UTUC.
Taken together, the results of the present study
are, to the best of our knowledge, the first to report the
prognostic significance of combining RDW and LYM% for determining
OS, CSS and PFS in patients with UTUC after RNU. The optimal
cut-off value of 0.80 for the pre-treatment RDW-to-LYM% ratio
significantly distinguished high-risk patients who had unfavorable
outcomes after surgery from the cohort. As the rising RDW-to-LYM%
ratio was attributed to increased RDW or/and decreased LYM%, it
contributed to benefit the survival and proliferation of the tumor,
and even metastasis, eventually leading to adverse patient survival
outcomes. Assessment of the pre-treatment RDW-to-LYM% ratio before
surgery was low in cost and easily accessible in clinical practice.
Furthermore, a pre-treatment RDW-to-LYM% ratio was employed to
establish a nomogram for predicting prognosis in UTUC. This
nomogram can be clinically applied to understand the specific
survival probabilities and risk factors for each patient; it can
serve as a decision-support tool, helping clinicians identify
patients with a high risk of post-operative recurrence, and it
further assists in deciding the timing and intensity of adjuvant
treatment.
There are some limitations to the present study.
First, this was a single-center and retrospective study, which
might give rise to selection bias. Secondly, all patients in this
study were Taiwanese, and Taiwan is known for its high incidence of
UTUC. The single ethnic group and limited area might affect the
result. Last but not least, this study lacked convincing molecular
biomarkers that involved the systemic inflammation and tumor
microenvironment, such as CRP, CD4 or CD8 for T cells, or CD68 and
CD163 for macrophages. All of these limitations may indicate that
future multicenter and prospective studies are required.
In conclusion, the present study found that an
elevated pre-treatment RDW-to-LYM% ratio was associated with more
advanced stage UTUC and a poorer prognosis after RNU. Moreover, the
pre-treatment RDW-to-LYM% ratio was demonstrated to be an
independent prognostic factor, potentially aiding in treatment
planning for patients with UTUC.
Supplementary Material
AUC to determine the predictive
ability of cancer-specific survival according to RDW, LYM% or
RDW-to-LYM% ratio. RDW-to-LYM% ratio, red cell distribution width
to lymphocyte percentage ratio; AUC, area under the
receiver-operating characteristic curve; CI, confidence
interval.
Acknowledgements
The authors are grateful to Dr Sheng-Hsiang Lin and
Ms. Wan-Ni Chen from the Biostatistics Consulting Center, Clinical
Medicine Research Center, National Cheng Kung University Hospital
(Tainan, Taiwan) for providing statistical consulting services.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
YCH and HCJ conceived the study and analyzed data.
THC, CYH, WHY, CHO and HCJ collected data. CAW, CYH, WHY and CHO
interpreted the data. YCH, THC and CAW wrote the manuscript draft.
CHO and HCJ supervised the study and reviewed and edited the
manuscript. YCH, THC, CAW, CHO and HCJ confirm the authenticity of
all the raw data. All authors read and approved the final version
of the manuscript.
Ethics approval and consent to
participate
The study received approval from the Institutional
Review Board of National Cheng-Kung University Hospital (Tainan,
Taiwan; approval no. NCKUH-B-ER-112-218). The board waived the
necessity for informed consent from the participants and granted
access to follow-up clinical records. The study adhered to the
guidelines outlined in the Declaration of Helsinki.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Use of artificial intelligence tools
During the preparation of this work, AI tools were
used to improve and revise the manuscript's grammar as necessary.
The authors take full responsibility for the ultimate content of
the present manuscript.
References
|
1
|
Rouprêt M, Babjuk M, Burger M, Capoun O,
Cohen D, Compérat EM, Cowan NC, Dominguez-Escrig JL, Gontero P,
Hugh Mostafid A, et al: European association of urology guidelines
on upper urinary tract urothelial carcinoma: 2020 Update. Eur Urol.
79:62–79. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Siegel RL, Miller KD and Jemal A: . Cancer
statistics, 2019. CA Cancer J Clin. 69:7–34. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Chang YH, Hsu WL, Lee YK, Chiang CJ, Yang
YW, You SL, Chen YC and Lai TS: Trends and sex-specific incidence
of upper urinary tract cancer in Taiwan: A birth cohort study.
Cancer Med. 12:15350–15357. 2023.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Margulis V, Shariat SF, Matin SF, Kamat
AM, Zigeuner R, Kikuchi E, Lotan Y, Weizer A, Raman JD and Wood CG:
Upper Tract Urothelial Carcinoma CollaborationThe Upper Tract
Urothelial Carcinoma Collaboration. Outcomes of radical
nephroureterectomy: A series from the upper tract urothelial
carcinoma collaboration. Cancer. 115:1224–1233. 2009.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Birtle A, Johnson M, Chester J, Jones R,
Dolling D, Bryan RT, Harris C, Winterbottom A, Blacker A, Catto
JWF, et al: Adjuvant chemotherapy in upper tract urothelial
carcinoma (the POUT trial): A phase 3, open-label, randomised
controlled trial. Lancet. 395:1268–1277. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Leow JJ, Chong YL, Chang SL, Valderrama
BP, Powles T and Bellmunt J: Neoadjuvant and adjuvant chemotherapy
for upper tract urothelial carcinoma: A 2020 systematic review and
meta-analysis, and future perspectives on systemic therapy. Eur
Urol. 79:635–654. 2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Vartolomei MD, Kimura S, Ferro M,
Vartolomei L, Foerster B, Abufaraj M and Shariat SF: Is
neutrophil-to-lymphocytes ratio a clinical relevant preoperative
biomarker in upper tract urothelial carcinoma? A meta-analysis of
4385 patients. World J Urol. 36:1019–1029. 2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Duan J, Pan L and Yang M: Preoperative
elevated neutrophil-to-lymphocyte ratio (NLR) and derived NLR are
associated with poor prognosis in patients with breast cancer: A
meta-analysis. Medicine (Baltimore). 97(e13340)2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Dalpiaz O, Krieger D, Ehrlich GC, Pohlmann
K, Stojakovic T, Pummer K, Zigeuner R, Pichler M and Hutterer GC:
Validation of the preoperative platelet-to-lymphocyte ratio as a
prognostic factor in a European cohort of patients with upper tract
urothelial carcinoma. Urol Int. 98:320–327. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Feng JF, Huang Y and Chen QX: Preoperative
platelet lymphocyte ratio (PLR) is superior to neutrophil
lymphocyte ratio (NLR) as a predictive factor in patients with
esophageal squamous cell carcinoma. World J Surg Oncol.
12(58)2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Jan HC, Hu CY, Yang WH and Ou CH:
Combination of platelet-lymphocyte ratio and monocyte-lymphocyte
ratio as a new promising prognostic factor in upper tract
urothelial carcinoma with large tumor sizes >3 cm. Clin
Genitourin Cancer. 18:e484–e500. 2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Li T, Xu H, Yang L, Tan P and Wei Q:
Predictive value of preoperative lymphocyte-to-monocyte ratio for
patients with upper tract urothelial carcinoma. Clin Chim Acta.
492:50–56. 2019.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Cananzi FCM, Minerva EM, Samà L, Ruspi L,
Sicoli F, Conti L, Fumagalli Romario U and Quagliuolo VL:
Preoperative monocyte-to-lymphocyte ratio predicts recurrence in
gastrointestinal stromal tumors. J Surg Oncol. 119:12–20.
2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Jan HC, Yang WH and Ou CH: Combination of
the preoperative systemic immune-inflammation index and
monocyte-lymphocyte ratio as a novel prognostic factor in patients
with upper-tract urothelial carcinoma. Ann Surg Oncol. 26:669–684.
2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Aziz MH, Sideras K, Aziz NA, Mauff K, Haen
R, Roos D, Saida L, Suker M, van der Harst E, Mieog JS, et al: The
systemic-immune-inflammation index independently predicts survival
and recurrence in resectable pancreatic cancer and its prognostic
value depends on bilirubin levels: A retrospective multicenter
cohort study. Ann Surg. 270:139–146. 2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ma W, Mao S, Bao M, Wu Y, Guo Y, Liu J,
Wang R, Li C, Zhang J, Zhang W and Yao X: Prognostic significance
of red cell distribution width in bladder cancer. Transl Androl
Urol. 9:295–302. 2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Huang TB, Zhu LY, Zhou GC and Ding XF:
Pre-treatment red blood cell distribution width as a predictor of
clinically significant prostate cancer. Int Urol Nephrol.
53:1765–1771. 2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Huang H, Li L, Luo W, Yang Y, Ni Y, Song
T, Zhu Y, Yang Y and Zhang L: Lymphocyte percentage as a valuable
predictor of prognosis in lung cancer. J Cell Mol Med.
26:1918–1931. 2022.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Levey AS, Bosch JP, Lewis JB, Greene T,
Rogers N and Roth D: A more accurate method to estimate glomerular
filtration rate from serum creatinine: A new prediction equation.
Modification of diet in renal disease study group. Ann Intern Med.
130:461–470. 1999.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Edge SB and Compton CC: The American joint
committee on cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474.
2010.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Eble JN, Sauter G, Epstein JI and
Sesterhenn IA (eds): Pathology and genetics of tumours of the
urinary system and male genital organs. WHO Classification of
Tumours. IARC Press, Lyon, 2004.
|
|
22
|
Coussens LM and Werb Z: Inflammation and
cancer. Nature. 420:860–867. 2002.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Dolan RD, Lim J, McSorley ST, Horgan PG
and McMillan DC: The role of the systemic inflammatory response in
predicting outcomes in patients with operable cancer: Systematic
review and meta-analysis. Sci Rep. 7(16717)2017.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Price JM, Mistry HB, Betts G, Cheadle EJ,
Dixon L, Garcez K, Illidge T, Iyizoba-Ebozue Z, Lee LW, McPartlin
A, et al: Pretreatment lymphocyte count predicts benefit from
concurrent chemotherapy with radiotherapy in oropharyngeal cancer.
J Clin Oncol. 40:2203–2212. 2022.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Thiangphak E, Pruegsanusak K and Buhachat
R: Pretreatment lymphocyte count as independent prognostic factor
in patients with locally advanced cervical cancer treated with
concurrent chemoradiotherapy. Int J Gynaecol Obstet. 159:672–678.
2022.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Kobayashi N, Usui S, Kikuchi S, Goto Y,
Sakai M, Onizuka M and Sato Y: Preoperative lymphocyte count is an
independent prognostic factor in node-negative non-small cell lung
cancer. Lung Cancer. 75:223–227. 2012.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Jimbo H, Horimoto Y, Ishizuka Y, Nogami N,
Shikanai A, Saito M and Watanabe J: Absolute lymphocyte count
decreases with disease progression and is a potential prognostic
marker for metastatic breast cancer. Breast Cancer Res Treat.
196:291–298. 2022.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Fukuokaya W, Kimura T, Miki J, Kimura S,
Watanabe H, Bo F, Okada D, Aikawa K, Ochi A, Suzuki K, et al: Red
cell distribution width predicts time to recurrence in patients
with primary non-muscle-invasive bladder cancer and improves the
accuracy of the EORTC scoring system. Urol Oncol.
38:638.e15–638.e23. 2020.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Thurner EM, Krenn-Pilko S, Langsenlehner
U, Stojakovic T, Pichler M, Gerger A, Kapp KS and Langsenlehner T:
The elevated C-reactive protein level is associated with poor
prognosis in prostate cancer patients treated with radiotherapy.
Eur J Cancer. 51:610–619. 2015.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Szkandera J, Stotz M, Absenger G,
Stojakovic T, Samonigg H, Kornprat P, Schaberl-Moser R, Alzoughbi
W, Lackner C, Ress AL, et al: Validation of C-reactive protein
levels as a prognostic indicator for survival in a large cohort of
pancreatic cancer patients. Br J Cancer. 110:183–188.
2014.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Iivanainen S, Ahvonen J, Knuuttila A,
Tiainen S and Koivunen JP: Elevated CRP levels indicate poor
progression-free and overall survival on cancer patients treated
with PD-1 inhibitors. ESMO Open. 4(e000531)2019.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Salvagno GL, Sanchis-Gomar F, Picanza A
and Lippi G: Red blood cell distribution width: A simple parameter
with multiple clinical applications. Crit Rev Clin Lab Sci.
52:86–105. 2015.PubMed/NCBI View Article : Google Scholar
|
|
33
|
de Gonzalo-Calvo D, de Luxán-Delgado B,
Rodríguez-González S, García-Macia M, Suárez FM, Solano JJ,
Rodríguez-Colunga MJ and Coto-Montes A: Interleukin 6, soluble
tumor necrosis factor receptor I and red blood cell distribution
width as biological markers of functional dependence in an elderly
population: A translational approach. Cytokine. 58:193–198.
2012.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Lippi G, Targher G, Montagnana M, Salvagno
GL, Zoppini G and Guidi GC: Relation between red blood cell
distribution width and inflammatory biomarkers in a large cohort of
unselected outpatients. Arch Pathol Lab Med. 133:628–632.
2009.PubMed/NCBI View Article : Google Scholar
|