Introduction
Breast cancer is the most common cancer and is the
leading cause of cancer mortality among females (1). In 2000, more than one million females
were diagnosed with breast cancer and more than three million
females succumbed to the disease (2). Tamoxifen as a selective estrogen
receptor (ER) modulator is widely used in pre- and postmenopausal
breast cancer (3). In 1977,
tamoxifen was initially approved to be administered to cases of
metastatic late breast cancer by the Food and Drug Administration.
It has been utilized to reduce the recurrence and improve survival
for ER-positive breast cancer, and to decrease the incidence of
breast cancer in females (4,5).
In previous years, it has been reported that
endocrine therapy using tamoxifen reduced recurrence by 39% and the
annual mortality rate by 31% (6).
Endocrine therapy with adjuvant tamoxifen for five years also
substantially reduces the rate of recurrence not only during the
treatment period but also throughout the first decade (7). Inversely, no additional benefit from
tamoxifen administered beyond five years has been demonstrated in
females with ER-positive breast cancer and negative axillary lymph
nodes (8). Despite this, strict
criteria were used to select the patients in these clinical trials
and characteristics varied in these patients. In fact, the majority
of studies to establish the safety and efficacy of tamoxifen have
been strict controlled and well-designed clinical studies, and few
can challenge these studies. The reality of clinical trials,
however, is that various factors may influence the study and lead
to less-than-ideal results, for example, a lack of compliance in
patients, which may affect the survival status of patients in
certain ways.
Information management systems provide a new
platform for ‘real world’ research. For example, Barron et
al (9) reported that the
cumulative tamoxifen nonpersistence rate was 22.1% within one year
of commencing treatment with tamoxifen, and the cumulative
nonpersistence rate by the end of follow-up at 3.5 years had
increased to 35.2%. Wigertz et al (10) revealed that 69% of patients were
fully adherent to therapy for three years, and 12% prematurely
discontinued therapy. A systematic review including 29 studies
showed that 47.1% of patients discontinued therapy, which impacted
the prognosis for breast cancer (11). To date, few studies exist on the
therapy status of tamoxifen for Chinese patients with early breast
cancer. Therefore, the aim of the present study was to investigate
the therapy status of tamoxifen in patients with early hormonal
receptor (HR)-positive breast cancer, to provide more information
for clinical practice.
Materials and methods
Study design
This retrospective analysis was based on Chinese
patients with early breast cancer for whom data was included in an
information management system for breast cancer in the Huaxi
Hospital of Sichuan University (Chengdu, China) between 1989 and
2012. The inclusion criteria of this study included: No distant
metastasis during diagnosis with breast cancer; and a diagnosis of
estrogen receptor and/or progesterone receptor (PR)-positive breast
cancer, or an unclear HR status with tamoxifen used as the
preferred drug. This study was approved by the institutional ethics
committee of Huaxi Hospital.
Data source
The information management system for breast cancer
in Huaxi Hospital covered information on diagnosis, surgery,
chemotherapy, targeted therapy, endocrine therapy and radiotherapy.
Information of patients with breast cancer was recorded, including
general characteristics, history, diagnosis, auxiliary examination,
therapy and living conditions. Real-time updates were recorded with
regard to recurrence, metastasis condition and survival status. All
patients received follow-up in outpatient clinics, or by telephone
and email. It was ensured that there were follow-ups at least every
3–6 months within years 1–2 and at least every 6–12 months within
years 3–5 following the diagnosis of breast cancer. When the
updating information of patients was delayed more than once in the
schedule, this was defined as a missing case.
Biomarker expression analysis
The expression of ER, PR and Ki-67 (an essential
biomarker of cellular proliferation) in each patient was detected
using immunohistochemical (IHC) analysis. The expression of ER and
PR was recorded as negative or positive, and the percentages of ER
and PR were calculated. Human epidermal growth factor receptor 2
(HER2) was assayed using the IHC method with the result presented
as 0–3+. Negative HER2 was defined as 0 or 1+, while positive HER2
was defined as 3+. The samples with results of 2+ and 1+ for HER2
were then tested with a fluorescence in situ hybridization
assay.
Disease-free survival (DFS) and
overall survival (OS) analysis
The primary endpoint of this study was DFS, which
was defined as the length of time from the date of diagnosis with
breast cancer to the first recurrence (local, regional, distant
metastasis or contralateral breast cancer), mortality from any
cause or the last follow-up. Locoregional recurrence was defined as
any recurrence of axillary fossa, internal mammary or
supraclavicular lymph nodes in the homolateral breast or lymph
drainage regions. The secondary endpoint was OS, which was defined
as the length of time from the date of diagnosis with breast cancer
to mortality from any cause or to the time of the last follow-up
visit.
Statistical analysis
The information of all patients included in this
study between 1989 and 2012 was exported from the information
management system for breast cancer, and the deadline for follow-up
was set to March 2013. The information was checked and organized by
two researchers, and the statistical analysis was performed by two
experienced researchers. The cumulative rates of continued
tamoxifen treatment and survival time were visualized using
Kaplan-Meier curves. All statistical analyses were performed using
SPSS software, version 13.0 (SPSS, Inc., Chicago, IL, USA).
Results
Patient information
A total of 2,738 patients with HR-positive early
breast cancer were included in this study based on the information
management system. The general information and corresponding
therapies of all patients are listed in Table I. The median age was 44 years,
including 99.4% (2,721/2,738) female and 0.6% (17/2,738) male
patients. Within females, 75.7% (2,059/2,738) were premenopausal
when diagnosed with early breast cancer, 24.3% (661/2,738) were
postmenopausal, and the median age of menopause was 47 years.
During follow-up of female patients, 59.6% (1,624/2,738) were
premenopausal, 36.3% (987/2,738) were postmenopausal and the
menstruation status of the remaining 4.8% (130/2,738) could not be
confirmed.
 | Table I.General information and corresponding
therapy of patients included in the study. |
Table I.
General information and corresponding
therapy of patients included in the study.
| Patient
information | Patients (n) | Percentage |
|---|
| Total | 2738 | 100.0 |
| Female | 2721 | 99.4 |
| Male | 17 | 0.6 |
| Menstruation when
diagnosed with early breast cancera |
|
|
|
Postmenopause | 661 | 24.3 |
|
Premenopause | 2059 | 75.7 |
|
Unknown | 1 | 0.0 |
| Menstruation during
follow-upa |
|
|
|
Postmenopause | 987 | 36.3 |
|
Premenopause | 1624 | 59.7 |
|
Unknown | 110 | 4.0 |
| Pathological
carcinoma type |
|
|
| Ductal
in situ | 90 | 3.3 |
| Invasive
ductal breast | 2331 | 85.1 |
|
Invasive | 112 | 4.1 |
|
Mucinous | 70 | 2.6 |
| Invasive
lobular | 43 | 1.6 |
|
Others | 92 | 3.4 |
| T status |
|
|
| T0 | 56 | 2.0 |
| Tis | 90 | 3.3 |
| T1 | 772 | 28.2 |
| T2 | 1232 | 45.0 |
| T3 | 183 | 6.7 |
| T4 | 73 | 2.7 |
| TX | 332 | 12.1 |
| N status |
|
|
| N0 | 1423 | 52.0 |
| N1 | 780 | 28.5 |
| N2 | 297 | 10.8 |
| N3 | 222 | 8.1 |
| NX | 16 | 0.6 |
| Estrogen
receptor |
|
|
| – | 374 | 13.7 |
| + | 1262 | 46.1 |
| ++ | 196 | 7.2 |
|
+++ | 605 | 22.1 |
| ± | 51 | 1.9 |
|
Unknown | 250 | 9.1 |
| Progesterone
receptor |
|
|
| – | 382 | 14.0 |
| + | 1320 | 48.2 |
| ++ | 227 | 8.3 |
|
+++ | 492 | 18.0 |
| ± | 45 | 1.6 |
| Progesterone
receptor |
|
Unknown | 272 | 9.9 |
| Human epidermal
growth factor receptor 2 |
| – | 1298 | 47.4 |
| + | 602 | 22.0 |
| ++ | 300 | 11.0 |
|
+++ | 165 | 6.0 |
| ± | 25 | 0.9 |
|
Unknown | 348 | 12.7 |
| Ki-67 |
|
|
|
<14% | 379 | 13.8 |
|
≥14% | 1611 | 58.8 |
|
Unknown | 748 | 27.3 |
| WHO
classification |
|
|
| I | 86 | 3.1 |
| II | 576 | 21.0 |
|
III | 750 | 27.4 |
|
Unknown | 1326 | 48.4 |
| Surgeries |
|
|
|
Breast-conserving
resections | 155 | 5.7 |
|
Modified radical
mastectomy | 2380 | 87.0 |
|
Extended radical
mastectomy | 139 | 5.0 |
|
Others | 64 | 2.3 |
| Chemotherapy
types |
|
|
|
Anthracycline-based | 1 094 | 40.0 |
|
Taxol-based | 177 | 6.5 |
|
Anthracycline plus
taxol-based | 891 | 32.5 |
|
Othersb | 362 | 13.2 |
|
None | 214 | 7.8 |
| Adjuvant
radiotherapy |
|
|
|
Yes | 1004 | 36.7 |
| No | 1734 | 63.3 |
Pathological types and treatment of
patients
Among all the patients, the main pathological
carcinoma type was invasive ductal breast (85.1%), followed by
invasive (4.1%), ductal in situ (DCIS, 3.3%), mucinous
(2.6%) and invasive lobular (1.6%). Tumor staging was based on
clinical tumor node metastasis classification, and the rates of
Tis/T0/T1/T2 and T3/T4 were 78.5% (2,150/2,738) and 9.4%
(256/2,738), respectively. The regional node status of the patients
was recorded, and the patients with a negative-regional node (N0)
status accounted for 52.0% (1,423/2,738) of cases, while N1, N2 and
N3 accounted for 28.5% (780/2,738), 10.8% (297/2,738) and 8.1%
(222/2,738), respectively. A total of 374 patients (13.7%) were
ER-negative, and 2,063 patients (75.4%) were ER-positive. For the
PR, there were 14.0% negative cases and 74.5% positive cases.
Patients with Ki-67 values ≥14% accounted for 58.8% (1,611/2,738)
of cases, while 13.8% (379/2,738) of patients exhibited values
<14%. Following the IHC assay, 6.0% (165/2,738) of patients were
shown to be HER2-positive.
Among the patients, 87.0% (2,380/2,738) of cases
underwent modified radical mastectomy; 5.7% (155/2,738),
breast-conserving resections; 5.0% (139/2,738), extended radical
mastectomy; and 2.3% (64/2,738), other surgeries. During follow-up,
40.0% (1,094/2,738), 6.5% (177/2,738) and 32.5% (891/2,738) of
patients received anthracycline-, taxol- and anthracycline plus
taxol combination-based chemotherapy treatments, respectively. No
chemotherapy was received by 7.8% (214/2,738) of patients.
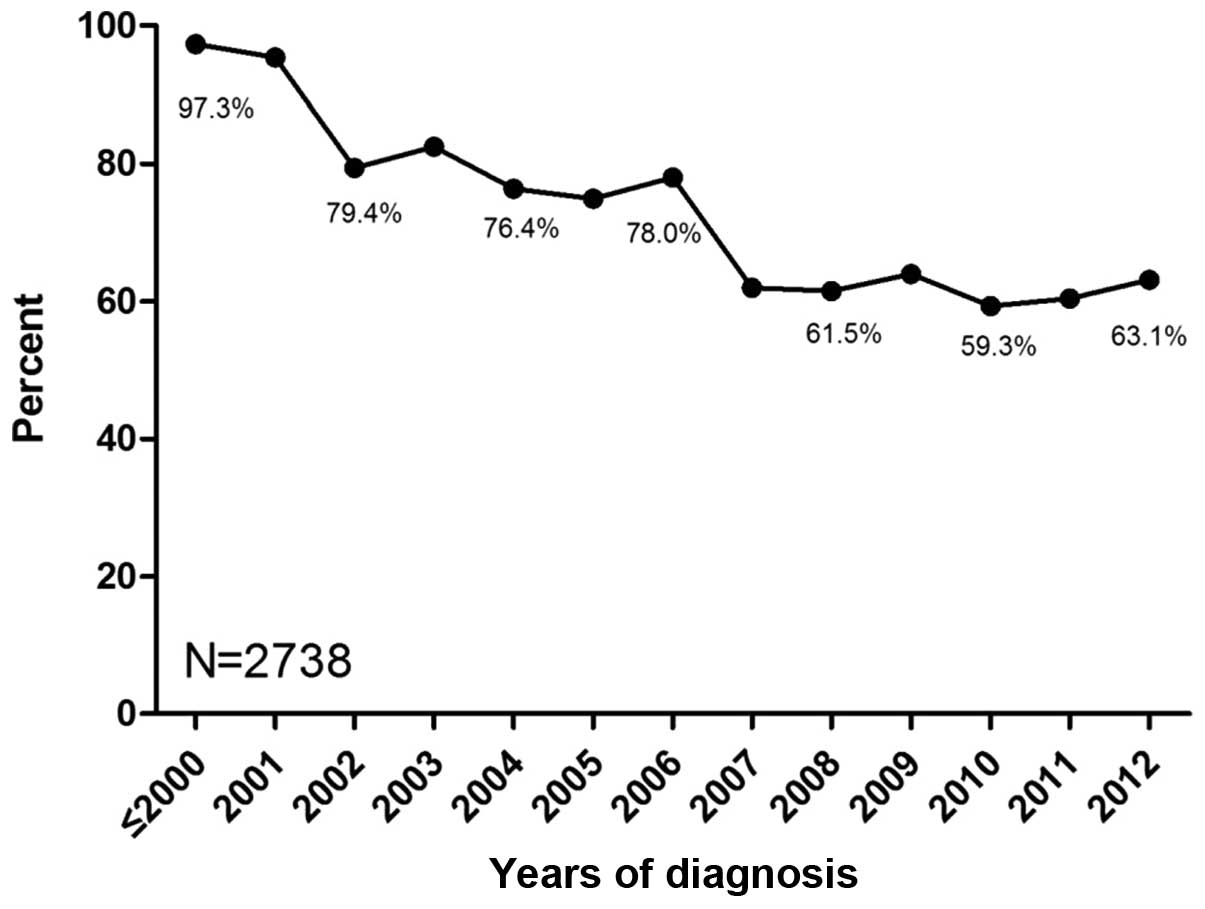
Usage status of tamoxifen
Among the 7,234 patients included with early breast
cancer amongst which the number of patients with HR-positive early
breast cancer is 2,738. A total of 54.1% (3,913/7,234) of
HR-positive and HR-unknown patients underwent more than one type of
endocrine therapy, and the preference of the other patients was
tamoxifen treatment. The percentage of tamoxifen preference in
adjuvant therapy was 97.3% prior to 2000, and decreased to 60.4% in
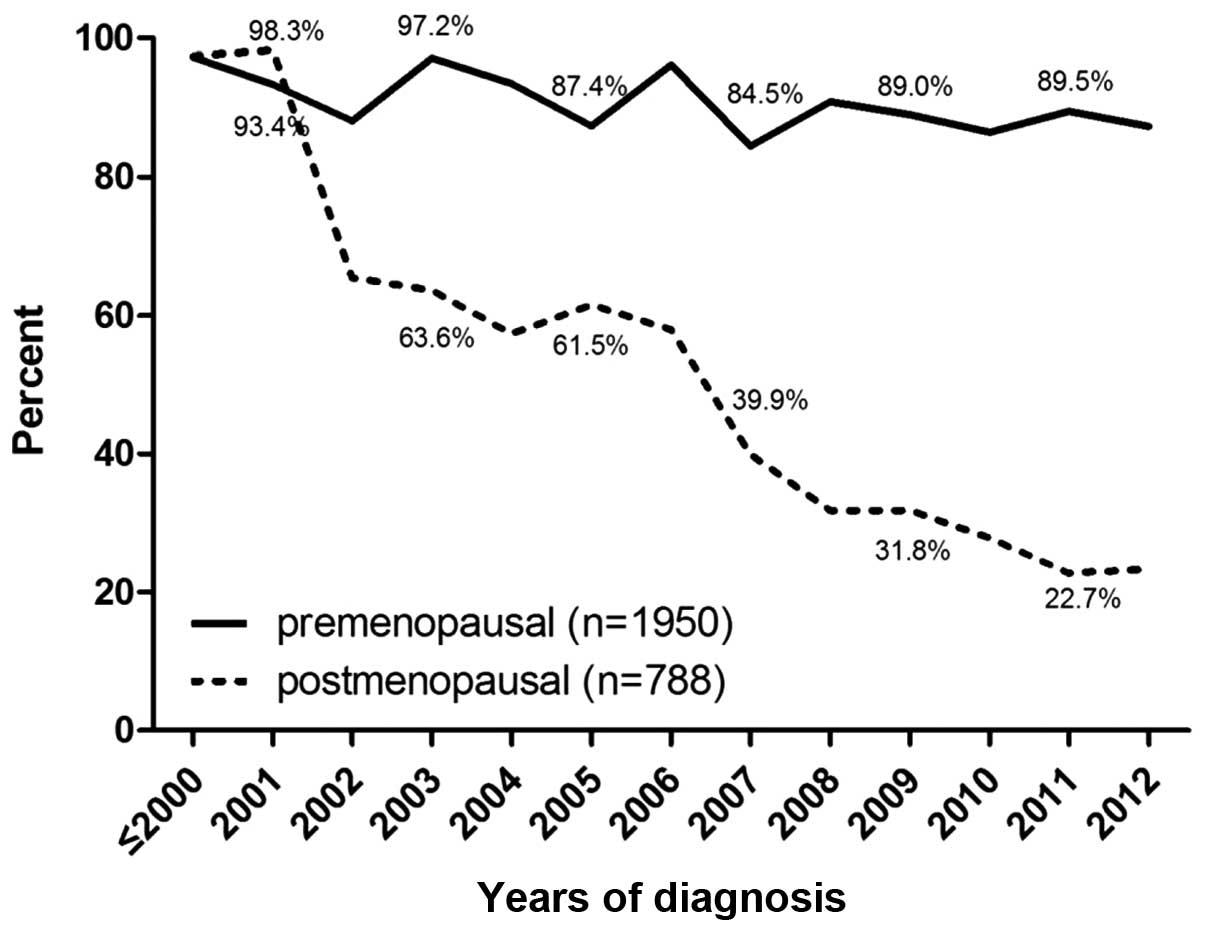
2011 (Fig. 1). Among premenopausal
patients, the percentage of tamoxifen preference reduced from 97.3%
prior to 2000 to 89.5% in 2011, while the percentage in
postmenopausal patients declined from 97.4% prior to 2000 to 22.7%
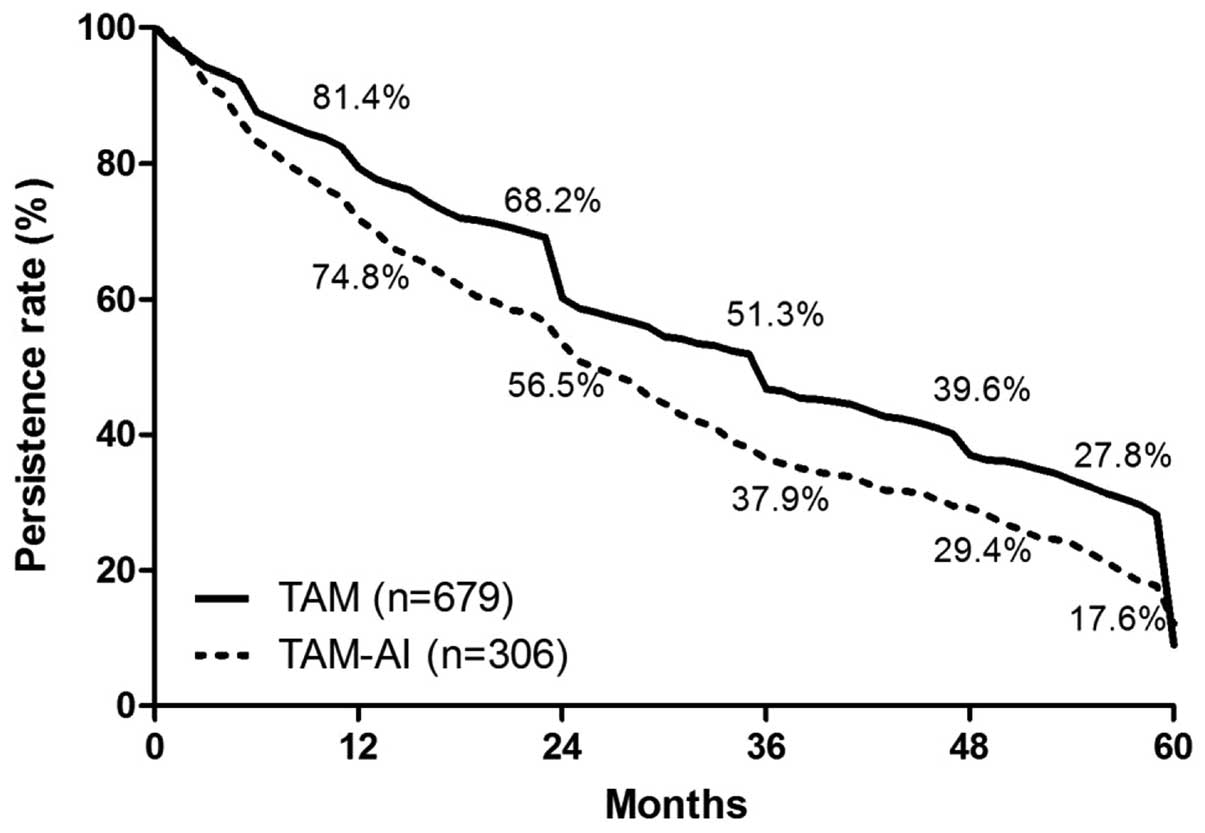
in 2011 (Fig. 2). Among patients
receiving tamoxifen in sequence with aromatase inhibitors, those
who used tamoxifen for one year accounted for 41.8%. Subsequently,
the percentages of patients using tamoxifen for >2, 3, 4, 6 and
6 years were 21.1, 16.0, 7.2, 7.6 and 6.3%, respectively (Fig. 3).
DFS and OS analysis of the
patients
Follow-up statuses of the cases at the deadline
revealed the following: 41.2% (1,127/2,738) of cases were receiving
endocrine therapy; 14.2% (388/2,738) were lost due to changes of
the contact information; 2.3% (63/2,738) were deceased without
updating information; 3.5% (97/2,738) lost contact; and 0.1%
(2/2,738) refused follow-up. A duration analysis of the 985
patients (36.0%) that ceased endocrine therapy was performed, and
the duration of tamoxifen treatment for one, two, three, four and
five years accounted for 79.4, 64.6, 47.1, 36.4 and 24.7%,
respectively (Fig. 4). With regard
to the survival times of patients, the rate of one-year DFS was
98.5%, and the DFS rates for two, three, four and five years were
96.2, 93.9, 92.2 and 89.1%, respectively (Fig. 5A). Patients with early breast cancer
had a one-year OS rate of 99.2%, and the rates of OS for two,
three, four and five years were 98.3, 97.7, 96.7 and 95.6%,
respectively (Fig. 5B).
Discussion
‘Real world’ studies are a method of evaluating the
external validity and safety of real therapy, based on a larger
sample covering a representative population (12–14). In
the present study, according to their actual conditions and own
free will, all patients were non-randomly selected for treatment,
and an evaluation of long-term adjuvant therapy with tamoxifen was
performed. To date, randomized controlled trials (RCTs) remain the
gold standard of studies (15).
However, strict inclusion standards do not conform to the
characteristics of patients in clinical practice, and whether the
results can be directly applied to clinical settings is uncertain.
Additionally, sample size determines the effectiveness of
corresponding studies, and the lower incidence is hard to verify in
RCTs. Notably, it may not be possible to perform an RCT due to the
relevant ethics and legal regulations (12,16).
Therefore, information management systems provide
new insights into further studies in the ‘real world’. Integrated
studies combining prospective with retrospective methods have been
used to collect information, which overcomes the selective
migration in retrospective studies, and applies a maximum of
intent-to-treat analysis to ensure more comprehensive data and real
results (17,18). In the present study, the application
status of tamoxifen in patients with early breast cancer was
investigated based on data in an information management system. It
was revealed that the usage of tamoxifen decreased gradually over
time, and the duration of tamoxifen treatment also reduced as well
as the DFS and OS of patients.
Tamoxifen, as the foundation of endocrine therapy
for breast cancer, plays a crucial role in treating patients prior
to menopause. It has been reported that the optimum duration of
tamoxifen treatment is five years (19). It is controversial as to whether
benefits arise from prolonging the treatment time. Recently,
adjuvant therapy with tamoxifen for 10 years was found to reduce
relapse (617/3,428 vs. 711/3,418, P=0.002) and mortality (331 vs.
397, P=0.01) when compared with adjuvant therapy with tamoxifen for
five years (7). In the present
study, it was revealed that the patients who continued tamoxifen
treatment for one, two, three, four and five years accounted for
79.4, 64.6, 47.1, 36.4 and 24.7% of cases, respectively. The usage
of long-term endocrine therapy was lower than that in another
retrospective study by Hershman et al (20), which indicated 49% usage for 4.5
years, and was also lower than the 72–90% usage shown in other
previous RCTs (21–23). Additionally, our previous study
showed that >10% of HR-positive patients did not receive any
endocrine therapy every year (unpublished data). Furthermore, the
DFS and OS differed significantly between patients with and without
endocrine therapy (five year DFS: 88.4 vs.75.1%; five year OS: 95.7
vs. 83.8%), which was consistent with the study by Hershman et
al (20). Overall, in the ‘real
world’, certain patients did not continue to receive endocrine
therapy, and it is recommended that treatment compliance in
patients should be improved to prolong the survival time of
patients with breast cancer.
In the findings of the Arimidex®, Tamoxifen, Alone
or in Combination (ATAC) randomized trial in 2002, during adjuvant
endocrine therapy for early breast cancer, the three-year DFS rate
for anastrozole use was improved compared with that for tamoxifen
[89.4 vs. 87.4%; hazard ratio, 0.83; 95% confidence interval (CI),
0.71–0.96; P=0.013], and subgroup analysis revealed increased
benefits in HR-positive patients (24). However, anastrozole is only
considered for use in patients for whom tamoxifen is
contraindicated or not tolerated (25). A study on postmenopausal women with
early breast cancer in 2005 showed that adjuvant treatment with
letrozole reduced the risk of recurrent disease to a greater extent
than tamoxifen as indicated by the five-year DFS rates (84.0% vs.
81.4%; hazard ratio, 0.81; 95%CI, 0.70–0.93; P=0.003), particularly
at distant sites (26). The St
Gallen International Expert Consensus in 2009 recommend that
aromatase inhibitors should form part of the standard endocrine
therapy for postmenopausal women with HR-positive breast cancer
(27). Thus, these observations
challenge the application of tamoxifen in postmenopausal women with
breast cancer, and the results of the present study reflect that
the status of tamoxifen has gradually wavered. With increasing
evidence of the efficacy of aromatase inhibitors, the usage of
tamoxifen was revealed by the present study to be only 19.7% in
2011. Notably, either adjuvant tamoxifen or an aromatase inhibitor
is the first choice in treating postmenopausal women with early
breast cancer, not due to the survival advantage, but for the
long-term efficacy and reduced recurrence rate (26,28).
In conclusion, adjuvant tamoxifen as a treatment for
early breast cancer has been surveyed in this study in a ‘real
world’ context, and the results showed that the usage of tamoxifen
decreased gradually and the duration of use was reduced over time,
as well as the DFS and OS of patients being reduced to some extent.
Additionally, this result suggests that the treatment compliance in
patients was poor. The use of tamoxifen for one year in sequence
with aromatase inhibitors accounted for 41.8% of cases, and whether
this treatment affects the survival of patients requires further
study. It is anticipated that these results may provide new
insights into studies in a ‘real world’ context.
References
|
1
|
Althuis MD, Dozier JM, Anderson WF, Devesa
SS and Brinton LA: Global trends in breast cancer incidence and
mortality 1973–1997. Int J Epidemiol. 34:405–412. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Parkin DM, Bray FI and Devesa SS: Cancer
burden in the year 2000 The global picture. Eur J Cancer. 37:(Suppl
8). S4–S66. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Park WC and Jordan VC: Selective estrogen
receptor modulators (SERMS) and their roles in breast cancer
prevention. Trends Mol Med. 8:82–88. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cohen MH, Hirschfeld S, Flamm Honig S, et
al: Drug approval summaries: arsenic trioxide, tamoxifen citrate,
anastrazole, paclitaxel, bexarotene. Oncologist. 6:4–11. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fisher B, Costantino JP, Wickerham DL, et
al: Tamoxifen for prevention of breast cancer: report of the
National Surgical Adjuvant Breast and Bowel Project P-1 Study. J
Natl Cancer Inst. 90:1371–1388. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Early Breast Cancer Trialists'
Collaborative Group (EBCTCG): Effects of chemotherapy and hormonal
therapy for early breast cancer on recurrence and 15-year survival:
an overview of the randomised trials. Lancet. 365:1687–1717. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Davies C, Pan H, Godwin J, et al: Longer
Against Shorter (ATLAS) Collaborative Group: Long-term effects of
continuing adjuvant tamoxifen to 10 years versus stopping at 5
years after diagnosis of oestrogen receptor-positive breast cancer:
ATLAS, a randomised trial. Lancet. 381:805–816. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fisher B, Dignam J, Bryant J and Wolmark
N: Five versus more than five years of tamoxifen for lymph
node-negative breast cancer: updated findings from the National
Surgical Adjuvant Breast and Bowel Project B-14 randomized trial. J
Natl Cancer Inst. 93:684–690. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Barron TI, Connolly R, Bennett K, Feely J
and Kennedy MJ: Early discontinuation of tamoxifen: a lesson for
oncologists. Cancer. 109:832–839. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wigertz A, Ahlgren J, Holmqvist M, et al:
Adherence and discontinuation of adjuvant hormonal therapy in
breast cancer patients: a population-based study. Breast Cancer Res
Treat. 133:367–373. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Murphy CC, Bartholomew LK, Carpentier MY,
Bluethmann SM and Vernon SW: Adherence to adjuvant hormonal therapy
among breast cancer survivors in clinical practice: a systematic
review. Breast Cancer Res Treat. 134:459–478. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Thorpe KE, Zwarenstein M, Oxman AD, et al:
A pragmatic-explanatory continuum indicator summary (PRECIS): a
tool to help trial designers. J Clin Epidemiol. 62:464–475. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Booth CM and Mackillop WJ: Translating new
medical therapies into societal benefit: the role of
population-based outcome studies. JAMA. 300:2177–2179. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Krumholz HM: Real-world imperative of
outcomes research. JAMA. 306:754–755. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kaptchuk TJ: The double-blind, randomized,
placebo-controlled trial: gold standard or golden calf? J Clin
Epidemiol. 54:541–549. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hershman DL and Wright JD: Comparative
effectiveness research in oncology methodology: observational data.
J Clin Oncol. 30:4215–4222. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Trotter JP: Patient registries: a new gold
standard for ‘real world’ research. Ochsner J. 4:211–214.
2002.PubMed/NCBI
|
|
18
|
Parkin DM: The evolution of the
population-based cancer registry. Nat Rev Cancer. 6:603–612. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Albain KS, Barlow WE, Ravdin PM, et al:
Breast Cancer Intergroup of North America: Adjuvant chemotherapy
and timing of tamoxifen in postmenopausal patients with
endocrine-responsive, node-positive breast cancer: a phase 3,
open-label, randomised controlled trial. Lancet. 374:2055–2063.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hershman DL, Shao T, Kushi LH, et al:
Early discontinuation and non-adherence to adjuvant hormonal
therapy are associated with increased mortality in women with
breast cancer. Breast Cancer Res Treat. 126:529–537. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Goss PE, Ingle JN, Martino S, et al: A
randomized trial of letrozole in postmenopausal women after five
years of tamoxifen therapy for early-stage breast cancer. N Engl J
Med. 349:1793–1802. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Coombes RC, Hall E, Gibson LJ, et al:
Intergroup Exemestane Study: A randomized trial of exemestane after
two to three years of tamoxifen therapy in postmenopausal women
with primary breast cancer. N Engl J Med. 350:1081–1092. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Howell A, Cuzick J, Baum M, et al: ATAC
Trialists' Group: Results of the ATAC (Arimidex, Tamoxifen, Alone
or in Combination) trial after completion of 5 years' adjuvant
treatment for breast cancer. Lancet. 365:60–62. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Baum M, Budzar A, Cuzick J, et al: ATAC
Trialists' Group: Anastrozole alone or in combination with
tamoxifen versus tamoxifen alone for adjuvant treatment of
postmenopausal women with early breast cancer: first results of the
ATAC randomised trial. Lancet. 359:2131–2139. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Goldhirsch A, Wood WC, Gelber RD, et al:
Meeting highlights: updated international expert consensus on the
primary therapy of early breast cancer. J Clin Oncol. 21:3357–3365.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Thürlimann B, Keshaviah A, Coates AS, et
al: Breast International Group (BIG) 1–98 Collaborative Group: A
comparison of letrozole and tamoxifen in postmenopausal women with
early breast cancer. N Engl J Med. 353:2747–2757. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Goldhirsch A, Ingle JN, Gelber RD, et al:
Panel members: Thresholds for therapies: highlights of the St
Gallen International Expert Consensus on the primary therapy of
early breast cancer 2009. Ann Oncol. 20:1319–1329. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Forbes JF, Cuzick J, Buzdar A, et al:
Arimidex, Tamoxifen, Alone or in Combination (ATAC) Trialists'
Group: Effect of anastrozole and tamoxifen as adjuvant treatment
for early-stage breast cancer: 100-month analysis of the ATAC
trial. Lancet Oncol. 9:45–53. 2008. View Article : Google Scholar : PubMed/NCBI
|