Introduction
Sialolithiasis is one of the most common diseases of
the salivary gland, accounting for ~50% of the obstructive and
inflammatory diseases of the major salivary glands (1). The most common symptoms associated with
sialolithiasis are pain and swelling of the affected salivary
gland. Sialolithiasis is most frequent in male patients aged
between 30–60 years (2).
Sialolithiasis affects the submandibular glands and Wharton's duct
in 80–90% of cases (3), and is
mainly unilateral (2,4). Bilateral sialolithiasis is a rare
condition, accounting for 1–3% of cases (5–7). A
sialolith must always be removed, since a long term obstruction of
the salivary gland duct can lead to inflammation and infection.
Surgical treatments, including the incision of Warthon's duct and
sialendoscopy, and non-surgical treatments, including oral
analgesics and antibiotics, have been used for the removal of
sialoliths (8–10). Sialolithectomy is the preferred
method for the removal of the stone, since this treatment results
in immediate relief of the pressure inside the gland by releasing
the retained saliva. Excision of the affected salivary gland and
its associated duct is also an option for the treatment of
sialolithiasis, particularly in cases with recurrent stone
formation. The present study reported the case of an 81-year-old
man with two recurrent calculi and concurrent sialadenitis in the
residual Wharton's duct, who had a history of excision of bilateral
submandibular glands as a sialolithiasis treatment. The present
study aimed to investigate the potential mechanisms underlying
recurrent sialolith formation in residual Wharton's ducts following
excision of the bilateral submandibular glands. Sialodochoplasty of
the submandibular duct and careful removal of calculi may reduce
the possibility of sialolith recurrence.
Case report
In February 2013, an 81-year-old man was admitted to
the First Affiliated Hospital of Dalian Medical University (Dalian,
China), complaining of a solid and painful mass in the left
submandibular area. The pain and swelling had been present for ~6
months. The patient had presented repeated episodes of
sialolithiasis in the right mandibular glands 4 years earlier. A
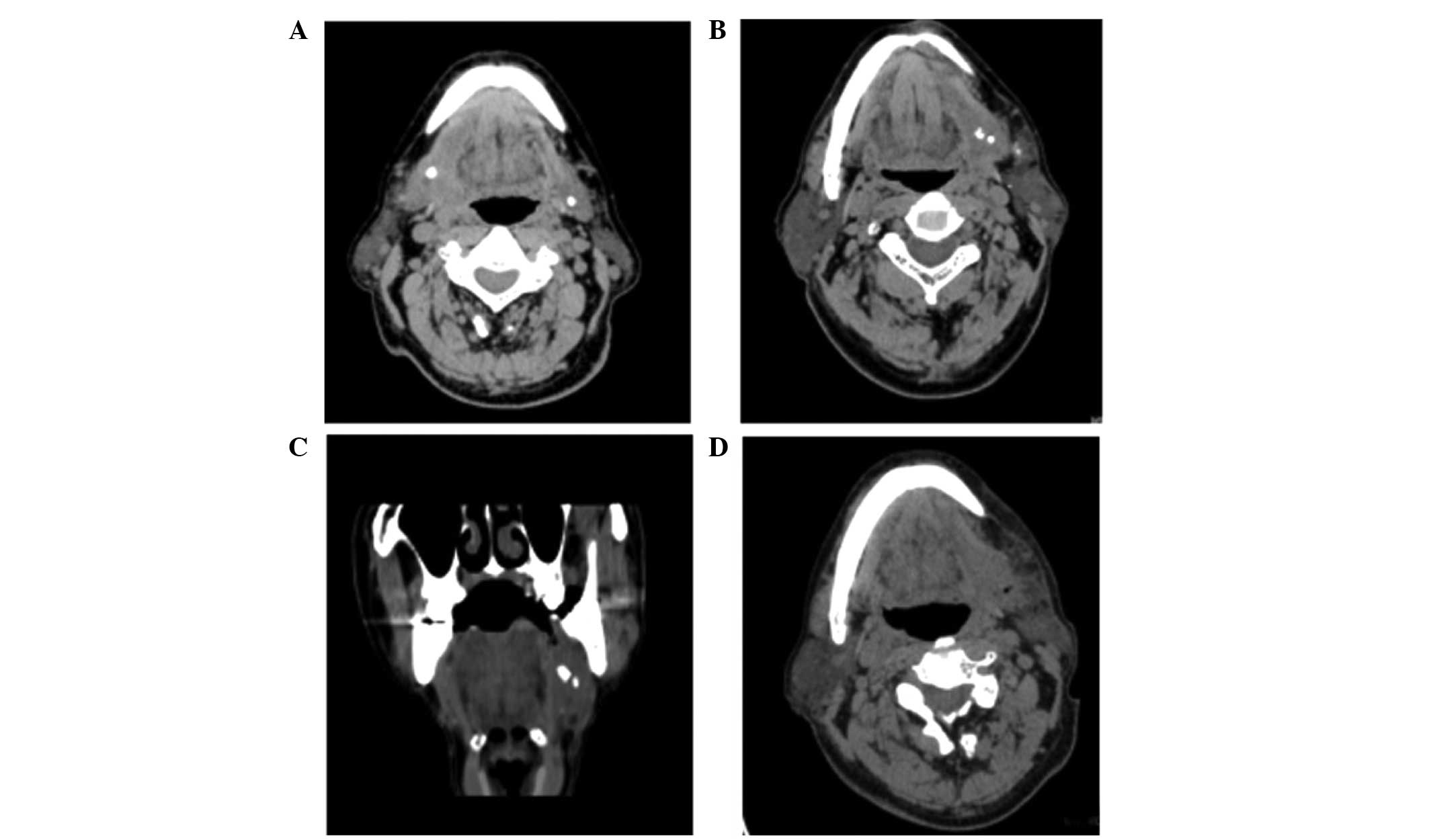
previous computed tomography (CT) scan revealed bilateral salivary
stones in the submandibular glands. The right stone was located in
the Wharton's duct near the glandular hilum, and the left stone was
located in the parenchyma of the gland (Fig. 1A). Excision of bilateral
submandibular glands with the right Wharton's duct was performed in
the First Affiliated Hospital of Dalian Medical University in
November 2009. The patient had no history of alcohol consumption,
smoking or drug abuse.
Clinical examination revealed normal intro-oral and
extra-oral anatomical structures, with the exception of local
indurated swelling in the left submandibular area. A CT scan of the
floor of the mouth and the neck demonstrated the presence of two
calcified masses below the inferior border of the mandible
(Fig. 1B and C). The anterior smooth
mass was adjacent to the location of the previously excised left
Wharton's duct near the hilum of the gland, and the posterior
irregular mass was in proximity to the anterior mass. Inflammation
of the soft tissues around the radiopaque lesions was detected, and
no radiographic evidence of residual left submandibular gland
tissues was observed Based on the history of the patient and CT
findings, the patient was diagnosed with recurrent
sialolithiasis.
Subsequently, the calculi were surgically excised.
Purulence was observed around the calculi, and thus incision and
irrigation of the surrounding soft tissues were performed.
Following surgery, the patient was treated with intravenous
injection of 3 g cefazolin twice a day for 3 days. A postoperative
CT scan showed no radiopaque lesions of the mouth floor and neck
(Fig. 1D). The patient was
discharged without any complications. The patient attended
follow-up sessions every 6 months, and at the latest follow-up
(May, 2014), the patient was disease-free.
Discussion
Sialolithiasis is the most common disease of the
salivary glands, mainly affecting the submandibular glands
(2). However, bilateral
sialolithiasis is a rare condition accounting for <3% of cases
(6). Levy et al reported that
bilateral sialolithiasis occurred in 4 out of 180 cases (2.2%) with
sialolithiasis (7). In addition,
Tholen found that, in a cohort including 97 patients with
sialolithiasis, only 1 patient (1%) presented bilateral
sialolithiasis (5). In the present
case, the patient had a history of bilateral sialolithiasis, and
had undergone excision of the bilateral submandibular glands and
the right Wharton's duct. Recurrent sialolithiasis in the residual
Wharton's duct occurred 4 years after the excision of the
submandibular glands. Similarly, Markiewicz et al reported a
case of recurrent sialolithiasis in a residual Wharton's duct 12
years after the excision of the submandibular glands (10). The case described in the present
study along with that reported by Markiewicz et al (10) demonstrated signs of infection in the
residual submandibular glands, suggesting that a long-term
obstruction may lead to infection in a residual Wharton's duct.
The exact mechanisms underlying sialolith formation
remain unclear. Several factors, such as abnormality in
Ca2+ metabolism, altered pH of saliva and reduced
salivary flow rate, have been suggested to contribute to sialolith
formation (4). The high incidence of
sialolith formation in the Wharton's duct may be due to the
alkaline pH and high Ca2+ content of the saliva. In
addition, a long ascending pathway of the Wharton's duct may
contribute to reduced salivary flow rate due to gravity slowing the
flow rate, as the saliva flows from the lower end to the upper end
of the Wharton's duct, thus leading to sialolith formation
(11). Furthermore, the salivary
flow rate is further decreased subsequent to sialolith formation
and infection, leading to aggravation of sialolithiasis.
The occurrence of sialoliths is rare, while the
recurrence rate of sialolithiasis has been reported to be ~8.9%
(11). In the present case,
recurrence of sialolithiasis occurred in the left Wharton's duct
following excision of the bilateral submandibular glands. It is
unlikely that the calculi were not detected during the time of the
submandibular gland removal, since the Wharton's ducts were
carefully examined and the right duct was removed due to the
presence of calculi. Anatomically, a communication exists between
the sublingual glandular complex and the submandibular gland duct.
The sublingual gland communicates with the Wharton's duct via the
Bartholin's duct or directly into the floor of the mouth (12). Therefore, the communication between
the sublingual gland and the Wharton's duct is hypothesized to
provide an anatomical basis for sialolith formation. In addition,
the sublingual gland is predominantly a mucus secreting gland, and
the viscous saliva in the relatively stagnant environment within
the residual part of the Wharton's duct further facilitates
sialolith formation (10,13).
In conclusion, the present study described a rare
case of recurrent sialoliths with concurrent sialadenitis in the
residual Wharton's duct subsequent to excision of the bilateral
submandibular glands for the treatment of sialolithiasis. Since the
Wharton's duct can facilitate drainage of the sublingual gland,
preservation of part of the Wharton's duct following excision of
the mandibular gland for sialolithiasis is important in order to
prevent sialadenitis of the sublingual bland. Sialodochoplasty of
the duct of the submandibular gland in combination with careful
massage of the duct from the bottom to the top to remove any
undetected calculi may reduce the possibility of sialolith and
sialadenitis recurrence in the sublingual gland.
References
|
1
|
Epker BN: Obstructive and inflammatory
diseases of the major salivary glands. Oral Surg Oral Med Oral
Pathol. 33:2–27. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Capaccio P, Torretta S, Ottavian F,
Sambataro G and Pignataro L: Modern management of obstructive
salivary diseases. Acta Otorhinolaryngol Ital. 27:161–172.
2007.PubMed/NCBI
|
|
3
|
Bsoul SA, Flint DJ, Terezhalmy GT and
Moore WS: Sialolithiasis. Quintessence Int. 34:316–317.
2003.PubMed/NCBI
|
|
4
|
Haubrich J: Clinical aspects of
non-tumorous diseases of the salivary glands. Arch
Otorhinolaryngol. 213:1–59. 1976.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tholen EF: Sialolithiasis. J Oral Surg
(Chic). 7:63–66. 1949.PubMed/NCBI
|
|
6
|
Sunder VS, Chakravarthy C, Mikkilinine R
and Mahoorkar S: Multiple bilateral submandibular gland
sialolithiasis. Niger J Clin Pract. 17:115–118. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Levy DM, Remine WH and Devine KD: Salivary
gland calculi. Pain, swelling associated with eating. JAMA.
181:1115–1119. 1962. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Juul ML and Wagner N: Objective and
subjective outcome in 42 patients after treatment of sialolithiasis
by transoral incision of Warthon's duct: A retrospective
middle-term follow-up study. Eur Arch Otorhinolaryngol.
271:3059–3066. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zenk J, Koch M, Klintworth N, König B,
Konz K, Gillespie MB and Iro H: Sialendoscopy in the diagnosis and
treatment of sialolithiasis: A study on more than 1000 patients.
Otolaryngol Head Neck Surg. 147:858–863. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Markiewicz MR, Margarone JE III, Tapia JL
and Aguirre A: Sialolithiasis in a residual Wharton's duct after
excision of a submandibular salivary gland. J Laryngol Otol.
121:182–185. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lustmann J, Regev E and Melamed Y:
Sialolithiasis. A survey on 245 patients and a review of the
literature. Int J Oral Maxillofac Surg. 19:135–138. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhang L, Xu H, Cai ZG, Mao C, Wang Y, Peng
X, Zhu ZH and Yu GY: Clinical and anatomic study on the ducts of
the submandibular and sublingual glands. J Oral Maxillofac Surg.
68:606–610. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Capaccio P, Torretta S, Ottavian F,
Sambataro G and Pignataro L: Modern management of obstructive
salivary diseases. Acta Otorhinolaryngol Ital. 27:161–172.
2007.PubMed/NCBI
|