Introduction
Bacterial biofilms have long been considered to be
one of the most difficult problems in the field of wound care
(1–8). Defined as complex microbial communities
irreversibly attached to the wound surface and embedded in
self-secreted extracellular polymeric substances (EPS), biofilms
provide bacteria with an effective barrier against host immune
cells and antimicrobial agents (6,9). As the
most common pathogen of wound infection, Staphylococcus
aureus (S. aureus) has been widely studied by
researchers (10–12). The EPS of staphylococcal biofilms are
primarily composed of polysaccharide intercellular adhesin (PIA),
extracellular DNA (eDNA), protein and cellular debris (13,14). In
particular, PIA and eDNA are the main components of the
extracellular matrix of biofilms, and their roles in intercellular
adhesion and biofilm formation have been investigated by numerous
studies (14–20). Furthermore, the compromised open
wounds create an ideal microenvironment for bacterial colonization
and biofilm development (6). A
series of in vitro and in vivo studies have revealed
that wound-associated biofilms grow rapidly and mature within 24 h
post-infection (12,21–23).
Once bacteria form a mature biofilm they are difficult to eradicate
(8). Despite traditional therapies
such as serial debridement and lavage that can remove the majority
of mature biofilms and necrotic tissue, residual bacteria may
rapidly reestablish a robust biofilm architecture, causing pain to
the patients during the process (24,25). The
ultimate consequence is a delay in wound healing and
reepithelialization (8,26–28).
The durability of a mature biofilm highlights the
importance of preventing biofilm formation at the early stages of
wound infection. Although specialized dressings for wound care do
have an inhibitory effect on biofilms, the efficacy varies greatly
with the type, concentration and release of active compound
(29). Antibiofilm agents, such as
dispersin B and DNase I, have been demonstrated to be effective in
the degradation of biofilm matrix both in vitro and in
vivo, although these are lacking in clinical application and
standard treatment regimens (9,30). In
addition, numerous small molecules targeting bacterial signaling
pathways, such as autoinducing peptide, have demonstrated
antibiofilm biological activities, although the clinical efficacy
and safety of these compounds has not been sufficiently evaluated
(9,26,31).
Despite considerable research, a significant improvement in biofilm
prevention in the clinical setting remains lacking.
Physical therapies have emerged in biofilm
management due to their satisfactory efficacy and low risk for
microbial resistance (32). In
particular, negative pressure wound therapy (NPWT) has been shown
to improve the healing process of infected wounds and to avoid
biofilm-associated infections when applied as early as possible
(33–38). Previous studies have attributed these
benefits to the secondary effects of NPWT, including fluid removal,
modulation of inflammation, and the stimulation of wound healing
signaling pathways (38–41). However, investigations into the role
of NPWT in biofilm formation remain limited. Despite individual
studies suggesting its compression effect on established mature
biofilms in vitro (42–44), the
efficacy of NPWT on biofilm prevention remains unclear,
particularly in vivo.
The aim of the present study was to evaluate and
validate the potential effect of NPWT on biofilm prevention when
initiated rapidly following wound contamination. Subsequent changes
in bacterial burden and wound healing secondary to NPWT were also
investigated. The results may provide a better understanding of the
therapeutic regimen required for wound care.
Materials and methods
Ethical statement
All animal experiments in the present study were
approved by the Medical Ethics Committee of the Chinese PLA General
Hospital (Beijing, China) in compliance with the Guidelines for
Care and Use of Animals in Research (45).
Animals
A total of 18 adult female Japanese large-ear white
rabbits (age, 3–6 months; weight, ~3 kg; purchased from the
Laboratory Animal Center of the Academy of Military Medical
Sciences, Beijing, China) were used for this study. The rabbits
were acclimated to standard housing and fed ad libitum under
constant temperature (22°C) and humidity (45%) with a 12-h
light/dark cycle.
Bacterial strains and culture
S. aureus strain RN6390 constitutively
expressing green fluorescent protein (obtained the from Chinese PLA
Institute for Disease Control and Prevention, Beijing, China) was
utilized for wound inoculation. S. aureus was grown
overnight and subcultured in Luria-Bertani broth (AOBOX
Biotechnology Co. Ltd., Beijing, China) at 37°C until log phase.
Cells were harvested by centrifugation at 4°C (5,000 × g), and
washed three times with phosphate-buffered saline (PBS). The final
bacterial resuspension was diluted with PBS to an optical density
of 1.0 at 600 nm equivalent to 105 colony-forming units
(CFUs)/µl empirically (11).
Wound protocol and bacterial
inoculation
The wounding and bacterial inoculation protocol was
based on the previously published wound model with minor
modifications (12). Briefly,
rabbits were anesthetized by intramuscular injection of a ketamine
(45 mg/kg; Gutian Pharma Co., Ltd., Fujian, China) and xylazine (5
mg/kg; Huamu Animal Health Product Co., Ltd., Jilin, China)
mixture. Ears were shaved and sterilized twice with 70% ethanol.
Following local anesthesia with 1% lidocaine (Yimin Pharmaceutical
Co., Ltd, Beijing, China), six standardized 8 mm diameter
full-thickness dermal wounds were created by an experienced surgeon
on each ventral ear down to the perichondrium using a scalpel.
Following hemostasis, the wounds were dressed with semiocclusive
IV3000 Transparent Adhesive Film Dressing (Smith & Nephew
Healthcare Ltd., Hull, UK). On postoperative day (POD) 3, each
wound was inoculated with 1×106 CFUs of S. aureus
at a volume of 10 µl. Planktonic bacteria were allowed to
proliferate in vivo under the semiocclusive transparent film
for a minimum of 6 h to ensure bacterial adhesion and colonization
(12,41,46,47).
Study design and treatment
protocol
All rabbit ears were used to create acute S.
aureus-contaminated wounds (6 wounds/ear; 36 ears). For each
animal, the two ears were respectively and randomly assigned to the
‘untreated control group’ and the ‘NPWT group’ (18 ears/group),
with the 6 wounds on each ear following the same protocol (32).
The wounds were treated under the previously
published protocol with minor modifications (48). Briefly, 6 h postinoculation on POD 3,
the wounds were dressed with a standard NPWT dressing (consisting
of polyvinyl alcohol foam, semiocclusive transparent dressing and
suction tube; Wuhan VSD Medical Science & Technology Co., Ltd.,
Wuhan, China) trimmed in advance to the appropriate size. The
suction tube was then connected to a vacuum pump device (provided
by Professor Lei Hu, Beihang University, Beijing, China). Wounds
treated with NPWT were subjected to continuous negative pressure at
−125 mmHg throughout the study (41,47).
Dressings were checked daily and changed on PODs 4, 6, 8 and 10, as
recommended for infected wounds by the manufacturer. Animals were
sacrificed via an overdose of intravenous pentobarbital sodium
(100–240 mg/kg; Sigma-Aldrich, St. Louis, MI, USA) on PODs 4 (n=8),
6 (n=2), 8 (n=2), 10 (n=2) and 13 (n=4). Wounds were harvested
using an 8-mm dermal biopsy punch (Miltex, Inc., York, PA, USA) for
PIA, eDNA, viable bacterial count and scanning electron microscopy
(SEM) analyses, or a scalpel for epifluorescence and histological
analyses.
Detection of PIA and eDNA in wound
biofilms
The dorsal side of the wound was removed to
eliminate the interference of non-specific bacteria outside of the
wound surface (32). The tissue
samples were placed in centrifuge tubes with 1 ml PBS, and
sonicated for 2 min to remove bacterial biofilms from the tissue
(32,49). The insoluble material was discarded
by centrifugation at 4°C (13,400 × g). In total, 0.5 ml supernatant
was used for the measurement of PIA, and the remainder was used for
eDNA extraction. An improved Elson-Morgan assay was performed
subsequently to measure the levels of PIA (13,19,20,50).
Briefly, 0.5 ml supernatant was supplemented with 0.1 ml potassium
tetraborate (0.8 mol/l; Vetec; Sigma-Aldrich) in a test tube. Tubes
were heated in a boiling water bath for 3 min and were subsequently
cooled using tap water. A total of 3 ml Ehrlich's reagent (Vetec;
Sigma-Aldrich) was added and, immediately after mixing, the tubes
were placed in a water bath at 37°C for 20 min. The reaction was
terminated by cooling the tubes with tap water. The results were
expressed as the absorbance of the final reaction solution at 585
nm as determined using a spectrophotometer (GeneQuant 1300; GE
Healthcare Life Sciences, Logan, UT, USA) (50).
The remaining supernatant was used for the
extraction of eDNA using the TIANamp Micro DNA kit (Tiangen Biotech
Co., Ltd., Beijing, China) according to the manufacturer's
protocol. The eDNA levels/wound were expressed as the DNA
concentration, quantified using a Qubit® 2.0 fluorometer with a
Qubit® dsDNA BR Assay kit (both Invitrogen; Thermo Fisher
Scientific, Inc., Waltham, MA, USA) according to the manufacturer's
protocol (30).
SEM
Following 2.5% glutaraldehyde and 1% osmium
tetroxide fixation, the tissue samples were dehydrated through a
series of graded ethanol (30, 50, 70, 80, 90 and 100%) and dried
with a critical point dryer (HCP-2; Hitachi, Ltd., Tokyo, Japan) by
flooding with liquid carbon dioxide at 5°C for 20 min and raising
the temperature to the critical point (~35°C). Subsequently,
samples were mounted using double-sided tape and coated with gold
in an auto sputter coater (E-1010; Hitachi, Ltd., Tokyo, Japan).
Imaging of the tissue samples was performed by SEM (S-3400N;
Hitachi, Ltd., Tokyo, Japan) operated at the scanning voltage of 15
kV.
Fluorescent staining and fluorescence
light microscopy
The wounds were bisected at the largest diameter and
embedded in optimal cutting temperature (O.C.T.) Compound (Sakura
Finetek USA, Inc., Torrance, CA, USA), snap-frozen, and stored in
liquid nitrogen until cryosectioning. Tissue sections (6 µm) were
obtained with a Leica CM1950 freezing microtome (Leica Microsystems
GmbH, Wetzlar, Germany). Visualization of biofilm matrix was
accomplished by staining with Concanavalin A Texas Red® Conjugate
(Invitrogen; Thermo Fisher Scientific, Inc.), specific for S.
aureus exopolysaccharides, for 15 min in the dark at room
temperature (12). The tissue
sections were then rinsed three times in PBS and incubated with
4′,6-diamidino-2-phenylindole dilactate (Invitrogen; Thermo Fisher
Scientific, Inc.) for 5 min to visualize the host cells.
Fluorescence microscopy was performed with an Olympus BX51
microscope (Olympus Corporation, Tokyo, Japan).
Viable bacterial count
measurements
Wounds were pretreated as described in the protocol
of PIA measurement. Tissue specimens were homogenized into 1 ml
suspension with sterile PBS, followed by sonication for 2 min to
disrupt bacterial aggregates in the biofilm. Subsequently, the
homogenates were serially diluted with sterile PBS (ranging from
10−1, 10−2, 10−3 to
10−6 times the concentration of the homogenates), plated
on Staphylococcus Isolation Agar (Hardy Diagnostics, Santa
Maria, CA, USA) and incubated at 37°C for 24 h. A standard
colony-counting method was conducted and the results were expressed
as the logarithm of CFUs/wound (12,41).
Measurement of wound closure
From POD 0 (the day of wounding), images of the
wounds were captured with a digital camera (IXUSi; Canon, Inc.,
Tokyo, Japan) on each day of dressing change. Wound size was then
determined by quantifying the wound area using Image-Pro Plus
version 6.0 software (Media Cybernetics, Inc., Rockville, MD, USA).
The rate of wound closure was expressed as a percentage of the
initial wound area (51).
Histological analysis
Wounds were bisected at the maximum diameter and
fixed in 10% neutral formalin (Yili Fine Chemicals Co., Ltd.,
Beijing, China). The tissue samples were then embedded in paraffin,
sectioned into 5-µm sections and stained with hematoxylin and
eosin. The observation of the tissue sections was performed with an
Olympus MVX10 macro-microscope (Olympus Corporation). Images of the
stained wounds were captured and analyzed using Image-Pro Plus
software, version 6.0. The morphometric parameters included the
epithelial and granulation gaps (the distance between the leading
edges of newly formed epithelial or granulation tissue) and the
epithelial or granulation area (the sum of the area of newly formed
epithelial or granulation tissue on the two sides of the wound bed)
(28). The measurements were carried
out by two independent observers who were blinded to the treatment,
and an average result was calculated.
Statistical analysis
Data are reported in graphical form as mean ±
standard deviation. Student's t-test (two-tailed and paired) was
used to compare the PIA/eDNA content, viable bacterial counts and
histological parameters between NPWT-treated wounds and their
untreated control. Wound closure was analyzed using
repeated-measures analysis of variance, followed by the least
significant difference post-hoc test to evaluate the statistical
difference between groups at each time point. All analyses were
performed using SPSS software, version 17.0 (SPSS Inc., Chicago,
IL, USA) at a significance level of α=0.05.
Results
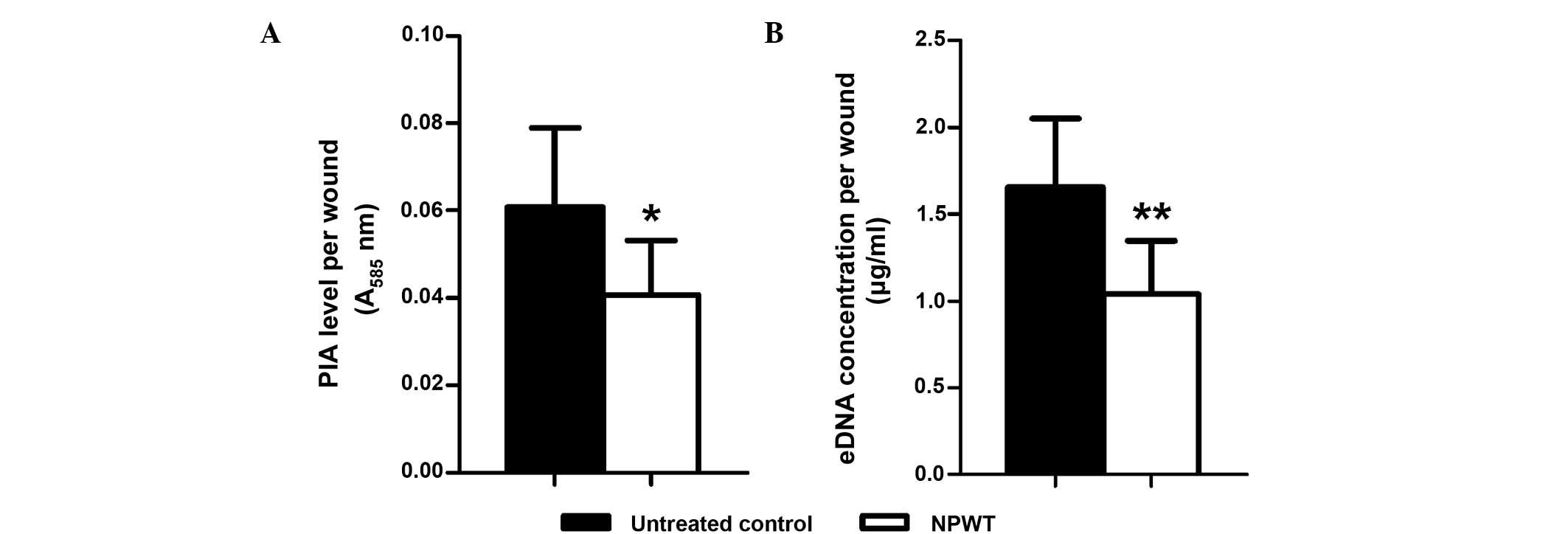
NPWT reduces PIA and eDNA levels and
inhibits the production of extracellular matrix
With the previously established rabbit ear wound
model, S. aureus-contaminated wounds were treated with or
without NPWT from 6 h postinoculation. For the main components of
S. aureus biofilm, namely PIA and eDNA, NPWT resulted in a
significant reduction in their levels in the wound beds (PIA,
P<0.05; eDNA, P<0.01) (Fig.
1). This reduction could be visualized through SEM (Fig. 2). The untreated wounds manifested a
relatively intact biofilm structure (Fig. 2A) with large amounts of cocci-shaped
S. aureus embedded within the lattice-like extracellular
matrix (arrows, Fig. 2B).
Conversely, wounds treaded with NPWT showed comparable amounts of
bacteria but a lack of extracellular matrix (Fig. 2C), which was more visible at a higher
magnification (Fig. 2D). To verify
the results, epifluorescence microscopy was performed, showing a
mature biofilm with large amounts of exopolysaccharide matrix
surrounding the bacteria in untreated wounds (Fig. 3A). By comparison, bacteria in the
NPWT group spread over the wound beds with sparse exopolysaccharide
matrix (Fig. 3B). An uncolonized
area of the wound tissue showed background staining of Concanavalin
A, and served as a negative control (Fig. 3C).
Prolonged NPWT reduces bacterial
load
Viable bacterial counts were measured over time to
investigate the effect of early application of NPWT on bacterial
burden (Fig. 4). On POD 4 and 6, the
bacterial load in the wounds treated with NPWT was not
significantly different from that in the untreated controls with
~107 CFUs/wound. However, from POD 8 there was a
significant decline of the bacterial load in the NPWT group (POD 8,
P<0.05; POD 10, P<0.01). At the end of the study (POD 13),
NPWT resulted in a significant reduction in the bacterial count by
two-log fold compared with the untreated wounds (P<0.001).
NPWT enhances wound healing
The reduction in bacterial burden secondary to NPWT
correlated with a synchronous enhancement in wound healing. Gross
appearance on POD 13 manifested a marked difference between the two
groups. Compared with the film-like exudates overlying the
untreated wounds (Fig. 5A), NPWT
accelerated wound closure and epithelialization, with clean
granulation tissue beds (Fig. 5B).
The rate of wound closure in the NPWT group was significantly
higher compared with that of the untreated group (Fig. 5C). Images of histological tissue
sections showed increased amounts of new epithelial and granulation
tissue in NPWT-treated wounds (Fig.
6B) compared with untreated controls (Fig. 6A). Trends in wound healing were
quantified by measuring the epithelial and granulation gaps and
areas. NPWT led to a significant reduction in epithelial and
granulation gaps (P<0.001) and increase in new epithelial
(P<0.01) and granulation (P<0.001) areas compared with the
untreated wounds (Fig. 6C and
D).
Discussion
Bacterial biofilm remains a challenging issue in the
field of wound care (1–8). Although there is a greater
understanding of the necessity of biofilm prevention, the
therapeutic strategies to prevent biofilm formation are limited in
clinical practice (8,9,24–31). In
an effort to seek safe and effective wound care modalities, early
application of NPWT has been widely acknowledged for its
considerable efficacy and low incidence of biofilm-associated
infections (32–38). However, despite an increasing number
of studies investigating this type of therapy, the potential role
of NPWT in biofilm prevention has yet to be elucidated (37–44). The
present study examined and evaluated the effect of NPWT on biofilm
prevention when initiated rapidly following wound
contamination.
The results indicated that the early application of
NPWT may be an effective approach for the prevention of biofilm
formation in S. aureus-contaminated wounds. Although the
exact mechanism underlying the effects of NPWT has yet to be
established, a possible explanation for the benefits observed
following treatment with NPWT may be the lack of biofilm matrix. As
the structural components of staphylococcal biofilms, PIA and
extracellular DNA have an important role in bacterial aggregation
and biofilm formation (15–18). Scavenging these matrix components or
inhibiting their biosynthesis can effectively prevent biofilm
formation and development (9).
Previous studies have demonstrated the effectiveness of NPWT in
fluid removal and wound cleaning due to the continuous suction
(39). The continuous suction may
also clear PIA and eDNA from the contaminated wounds before these
components are able to form extensive intermolecular crosslinks
around the bacteria. In addition, due to the physical effect of
negative pressure, NPWT leads to an essentially different
microenvironment for wound healing, characterized by hypoxia and
microstress (38). These
environmental factors, which may stimulate host gene expression and
cell proliferation through a variety of signaling pathways
(38,40), may also have an effect on the
bacteria. Therefore, another possible mechanism is that the
environmental factors secondary to NPWT inhibit the biosynthesis of
bacterial biofilm components, such as PIA and eDNA. Therefore, the
early application of NPWT may prevent biofilm formation in S.
aureus-contaminated wound beds.
Without the protection of the biofilm matrix, the
bacteria may be eliminated by host immune cells more effectively
(9), as shown by viable bacterial
counts. Notably, the reduction of the bacterial burden should not
be attributed to physical suction, as the bacterial counts did not
significantly decrease at the early stages of NPWT. The immune
response is more likely to have a leading role in bacterial
clearance, as previously demonstrated (41,46).
Subsequently, a reduction in biofilm matrix and bacterial burden
secondary to NPWT may be beneficial to wound healing, since both of
these factors are thought to inhibit the healing process (26–28). In
addition, NPWT may also improve wound healing through its ability
to stimulate host gene expression and cell proliferation (38–40).
Previous studies have investigated the effect of
topical negative pressure used with or without bactericide on
established mature biofilms in vitro, and demonstrated the
presence of several changes in biofilm morphometric parameters and
a reduction in bacterial counts (42–44).
However, a compression (perhaps fragmentation) effect on biofilm
architecture alone was inferred from the results (42,44).
There was no evidence that NPWT was able to remove an established
mature biofilm. Unlike these previous studies, the present
investigation predominantly focused on the initial stages of wound
infection, and examined the efficacy of NPWT on biofilm formation
and development. For clinicians and researchers, processes that
impede biofilm formation at the initial stage have long been
regarded as a promising approach to prevent biofilm-associated
infections and chronic infections (25,37).
Bacteria without the protection of a biofilm matrix are more
susceptible to immune cells and antimicrobial treatment (9,25). The
results of the present study suggested that the early use of NPWT
rapidly following wound contamination may be more effective than
delayed application in impeding biofilm formation. These results
are concordant with those of previous studies that have
demonstrated a satisfactory efficacy of NPWT on managing acute
wounds with contamination when initiated early (33–36).
Although further investigations are required in order to clarify
the role of biofilm matrix reduction in wound care, the present
study provides a possible mechanism of action for this therapy.
Despite rigorous methods and significant results,
there were limitations to the study. In particular, the effect of
NPWT on S. aureus alone was investigated. As the majority of
clinical cases are mixed infections, the investigation of other
bacterial species is required during further studies to validate
the results discussed herein. In addition, compared with previous
studies, NPWT was not combined with traditional therapies, such as
bactericide or irrigation. Although biofilm formation and
development were inhibited by NPWT alone, viable bacterial counts
did not decrease until immune cells infiltrated the wounds.
Combined treatment is may have the potential to enhance the
elimination of bacteria.
In view of the fact that mature biofilms are
difficult to eradicate, the demand for effective and practical
measures to avoid biofilm-associated infections is rising in
clinical settings. Early application of NPWT to wounds contaminated
with S. aureus has shown a significant efficacy on biofilm
prevention in the present study. With an increasing number of
clinical trials to validate its role in wound infection management,
NPWT appears to reduce the accumulation of biofilm matrix,
providing more opportunities for host cells or antimicrobial
treatments to eliminate the unprotected bacteria. A better
understanding of the potential role of NPWT in wound management and
biofilm prevention should contribute to innovations in the field of
wound care.
Acknowledgements
The present study was supported by a grant from the
National Natural Science Foundation of China (grant no.
81472112).
References
|
1
|
Costerton JW, Stewart PS and Greenberg EP:
Bacterial biofilms: A common cause of persistent infections.
Science. 284:1318–1322. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hall-Stoodley L, Costerton JW and Stoodley
P: Bacterial biofilms: From the natural environment to infectious
diseases. Nat Rev Microbiol. 2:95–108. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Parsek MR and Singh PK: Bacterial
biofilms: An emerging link to disease pathogenesis. Annu Rev
Microbiol. 57:677–701. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Edwards R and Harding KG: Bacteria and
wound healing. Curr Opin Infect Dis. 17:91–96. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sen CK, Gordillo GM, Roy S, Kirsner R,
Lambert L, Hunt TK, Gottrup F, Gurtner GC and Longaker MT: Human
skin wounds: A major and snowballing threat to public health and
the economy. Wound Repair Regen. 17:763–771. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lindsay D and von Holy A: Bacterial
biofilms within the clinical setting: What healthcare professionals
should know. J Hosp Infect. 64:313–325. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
James GA, Swogger E, Wolcott R, Pulcini E,
Secor P, Sestrich J, Costerton JW and Stewart PS: Biofilms in
chronic wounds. Wound Repair Regen. 16:37–44. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bjarnsholt T, Kirketerp-Møller K, Jensen
PØ, Madsen KG, Phipps R, Krogfelt K, Høiby N and Givskov M: Why
chronic wounds will not heal: A novel hypothesis. Wound Repair
Regen. 16:2–10. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Boles BR and Horswill AR: Staphylococcal
biofilm disassembly. Trends Microbiol. 19:449–455. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Moet GJ, Jones RN, Biedenbach DJ, Stilwell
MG and Fritsche TR: Contemporary causes of skin and soft tissue
infections in North America, Latin America, and Europe: Report from
the SENTRY Antimicrobial Surveillance Program (1998-2004). Diagn
Microbiol Infect Dis. 57:7–13. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Seth AK, Geringer MR, Nguyen KT, Agnew SP,
Dumanian Z, Galiano RD, Leung KP, Mustoe TA and Hong SJ:
Bacteriophage therapy for Staphylococcus aureus
biofilm-infected wounds: A new approach to chronic wound care.
Plast Reconstr Surg. 131:225–234. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gurjala AN, Geringer MR, Seth AK, Hong SJ,
Smeltzer MS, Galiano RD, Leung KP and Mustoe TA: Development of a
novel, highly quantitative in vivo model for the study of
biofilm-impaired cutaneous wound healing. Wound Repair Regen.
19:400–410. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sadovskaya I, Vinogradov E, Flahaut S,
Kogan G and Jabbouri S: Extracellular carbohydrate-containing
polymers of a model biofilm-producing strain, Staphylococcus
epidermidis RP62A. Infect Immun. 73:3007–3017. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Otto M: Staphylococcal biofilms. Curr Top
Microbiol Immunol. 322:207–228. 2008.PubMed/NCBI
|
|
15
|
Arciola CR, Campoccia D, Speziale P,
Montanaro L and Costerton JW: Biofilm formation in
Staphylococcus implant infections. A review of molecular
mechanisms and implications for biofilm-resistant materials.
Biomaterials. 33:5967–5982. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bayles KW: The biological role of death
and lysis in biofilm development. Nat Rev Microbiol. 5:721–726.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cramton SE, Gerke C, Schnell NF, Nichols
WW and Götz F: The intercellular adhesion (ica) locus is present in
Staphylococcus aureus and is required for biofilm formation.
Infect Immun. 67:5427–5433. 1999.PubMed/NCBI
|
|
18
|
O'Gara JP: ica and beyond: Biofilm
mechanisms and regulation in Staphylococcus epidermidis and
Staphylococcus aureus. FEMS Microbiol Lett. 270:179–188.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wu X, Wang Y and Tao L: Sulfhydryl
compounds reduce Staphylococcus aureus biofilm formation by
inhibiting PIA biosynthesis. FEMS Microbiol Lett. 316:44–50. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sadovskaya I, Chaignon P, Kogan G, Chokr
A, Vinogradov E and Jabbouri S: Carbohydrate-containing components
of biofilms produced in vitro by some staphylococcal strains
related to orthopaedic prosthesis infections. FEMS Immunol Med
Microbiol. 47:75–82. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Schaber JA, Triffo WJ, Suh SJ, Oliver JW,
Hastert MC, Griswold JA, Auer M, Hamood AN and Rumbaugh KP:
Pseudomonas aeruginosa forms biofilms in acute infection
independent of cell-to-cell signaling. Infect Immun. 75:3715–3721.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Harrison-Balestra C, Cazzaniga AL, Davis
SC and Mertz PM: A wound-isolated Pseudomonas aeruginosa
grows a biofilm in vitro within 10 hours and is visualized by light
microscopy. Dermatol Surg. 29:631–635. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Akiyama H, Huh WK, Yamasaki O, Oono T and
Iwatsuki K: Confocal laser scanning microscopic observation of
glycocalyx production by Staphylococcus aureus in mouse
skin: Does S. aureus generally produce a biofilm on damaged
skin? Br J Dermatol. 147:879–885. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Seth AK, Geringer MR, Gurjala AN, Hong SJ,
Galiano RD, Leung KP and Mustoe TA: Treatment of Pseudomonas
aeruginosa biofilm-infected wounds with clinical wound care
strategies: A quantitative study using an in vivo rabbit ear model.
Plast Reconstr Surg. 129:262e–274e. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wolcott RD, Rumbaugh KP, James G, Schultz
G, Phillips P, Yang Q, Watters C, Stewart PS and Dowd SE: Biofilm
maturity studies indicate sharp debridement opens a time-dependent
therapeutic window. J Wound Care. 19:320–328. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Schierle CF, De la Garza M, Mustoe TA and
Galiano RD: Staphylococcal biofilms impair wound healing by
delaying reepithelialization in a murine cutaneous wound model.
Wound Repair Regen. 17:354–359. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Roche ED, Renick PJ, Tetens SP, Ramsay SJ,
Daniels EQ and Carson DL: Increasing the presence of biofilm and
healing delay in a porcine model of MRSA-infected wounds. Wound
Repair Regen. 20:537–543. 2012.PubMed/NCBI
|
|
28
|
Seth AK, Geringer MR, Galiano RD, Leung
KP, Mustoe TA and Hong SJ: Quantitative comparison and analysis of
species-specific wound biofilm virulence using an in vivo,
rabbit-ear model. J Am Coll Surg. 215:388–399. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Brackman G, De Meyer L, Nelis HJ and
Coenye T: Biofilm inhibitory and eradicating activity of wound care
products against Staphylococcus aureus and Staphylococcus
epidermidis biofilms in an in vitro chronic wound model. J Appl
Microbiol. 114:1833–1842. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Watters C, Everett JA, Haley C, Clinton A
and Rumbaugh KP: Insulin treatment modulates the host immune system
to enhance Pseudomonas aeruginosa wound biofilms. Infect
Immun. 82:92–100. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kaplan JB: Biofilm dispersal: Mechanisms,
clinical implications, and potential therapeutic uses. J Dent Res.
89:205–218. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Seth AK, Nguyen KT, Geringer MR, Hong SJ,
Leung KP, Mustoe TA and Galiano RD: Noncontact, low-frequency
ultrasound as an effective therapy against Pseudomonas
aeruginosa-infected biofilm wounds. Wound Repair Regen.
21:266–274. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Costello JP, Amling JK, Emerson DA, Peer
SM, Afflu DK, Zurakowski D, Jonas RA and Nath DS: Negative pressure
wound therapy for sternal wound infections following congenital
heart surgery. J Wound Care. 23:31–36. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cheng HT, Hsu YC and Wu CI: Risk of
infection with delayed wound coverage by using negative-pressure
wound therapy in Gustilo Grade IIIB/IIIC open tibial fracture: An
evidence-based review. J Plast Reconstr Aesthet Surg. 66:876–878.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Steingrimsson S, Gottfredsson M,
Gudmundsdottir I, Sjögren J and Gudbjartsson T: Negative-pressure
wound therapy for deep sternal wound infections reduces the rate of
surgical interventions for early re-infections. Interact Cardiovasc
Thorac Surg. 15:406–410. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Anagnostakos K and Mosser P: Negative
pressure wound therapy in the management of postoperative
infections after musculoskeletal tumour surgery. J Wound Care.
23:191–194, 196-197. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Bradley BH and Cunningham M: Biofilms in
chronic wounds and the potential role of negative pressure wound
therapy: An integrative review. J Wound Ostomy Continence Nurs.
40:143–149. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Huang C, Leavitt T, Bayer LR and Orgill
DP: Effect of negative pressure wound therapy on wound healing.
Curr Probl Surg. 51:301–331. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Orgill DP, Manders EK, Sumpio BE, Lee RC,
Attinger CE, Gurtner GC and Ehrlich HP: The mechanisms of action of
vacuum assisted closure: More to learn. Surgery. 146:40–51. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Morykwas MJ, Simpson J, Punger K, Argenta
A, Kremers L and Argenta J: Vacuum-assisted closure: State of basic
research and physiologic foundation. Plast Reconstr Surg. 117(7
Suppl): 121S–126S. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Liu D, Zhang L, Li T, Wang G, Du H, Hou H,
Han L and Tang P: Negative-pressure wound therapy enhances local
inflammatory responses in acute infected soft-tissue wound. Cell
Biochem Biophys. 70:539–547. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Ngo QD, Vickery K and Deva AK: The effect
of topical negative pressure on wound biofilms using an in vitro
wound model. Wound Repair Regen. 20:83–90. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Phillips PL, Yang Q and Schultz GS: The
effect of negative pressure wound therapy with periodic
instillation using antimicrobial solutions on Pseudomonas
aeruginosa biofilm on porcine skin explants. Int Wound J.
10(Suppl 1): 48–55. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Valente PM, Deva A, Ngo Q and Vickery K:
The increased killing of biofilms in vitro by combining topical
silver dressings with topical negative pressure in chronic wounds.
Int Wound J. doi: 10.1111/iwj.12248. PubMed/NCBI
|
|
45
|
Institute of Laboratory Animal Resources
(US). Committee on Care, Use of Laboratory Animals, and National
Institutes of Health (US). Division of Research Resources: Guide
for the care and use of laboratory animals (8th). (Washington, DC).
National Academies Press. 2011.
|
|
46
|
Lalliss SJ, Stinner DJ, Waterman SM,
Branstetter JG, Masini BD and Wenke JC: Negative pressure wound
therapy reduces Pseudomonas wound contamination more than
Staphylococcus aureus. J Orthop Trauma. 24:598–602. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Assadian O, Assadian A, Stadler M,
Diab-Elschahawi M and Kramer A: Bacterial growth kinetic without
the influence of the immune system using vacuum-assisted closure
dressing with and without negative pressure in an in vitro wound
model. Int Wound J. 7:283–289. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Chen SZ, Li J, Li XY and Xu LS: Effects of
vacuum-assisted closure on wound microcirculation: An experimental
study. Asian J Surg. 28:211–217. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Burian M, Rautenberg M, Kohler T, Fritz M,
Krismer B, Unger C, Hoffmann WH, Peschel A, Wolz C and Goerke C:
Temporal expression of adhesion factors and activity of global
regulators during establishment of Staphylococcus aureus
nasal colonization. J Infect Dis. 201:1414–1421. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Reissig JL, Storminger JL and Leloir LF: A
modified colorimetric method for the estimation of N-acetylamino
sugars. J Biol Chem. 217:959–966. 1955.PubMed/NCBI
|
|
51
|
Lim Y, Levy MA and Bray TM: Dietary
supplementation of N-acetylcysteine enhances early inflammatory
responses during cutaneous wound healing in protein malnourished
mice. J Nutr Biochem. 17:328–336. 2006. View Article : Google Scholar : PubMed/NCBI
|