Introduction
Fever is among the most common presenting symptoms
in emergency department hospital cases; however, fever may be a
symptom of numerous diseases (1).
Pathogen infection is one of the most common causes of induced
fever. In addition to the basic history assessment and physical
examination of patients, emergency physicians typically require
more information, such as laboratory test results and imaging
examination, to diagnose the causes of fever-associated diseases
(2).
In clinical settings, certain laboratory tests have
been used to facilitate the diagnosis of severe bacterial
infection, such as white blood cell (WBC) count, C-reactive protein
(CRP) and procalcitonin (3,4). As a host immune system recognizes
pathogens and induces production of inflammatory molecules to
resist pathogens, numerous cytokines and chemokines are used as
biomarkers in laboratory research for the diagnosis and prognostic
prediction of infectious diseases (5–13). For
example, studies have shown that inflammatory cytokines levels are
altered as a result of a variety of infections, including
interleukin (IL)-1, IL-6, IL-10, IL-13, IL-18 and tumor necrosis
factor-alpha (TNF-α) (5–8). Elevating plasma concentration of
cytokines such as IL-6 and IL-10 may serve as a diagnostic marker
of sepsis and is correlated with severity and survival of sepsis
patients (9,10). In addition, certain chemokines, such
as Regulated on Activation, Normal T cell Expressed and Secreted
(RANTES), interferon-gamma-inducible protein 10 (IP-10) and
CXCL8/IL-8, are associated with sepsis (11–13).
These markers may provide important information for the early
diagnosis of diseases.
Immune system recognizes different pathogens with
particular characteristics, such as lipopolysaccharides on
gram-negative bacteria, peptidoglycan on gram-positive bacteria and
single-stranded and double-stranded RNA in RNA viruses, using
pattern-recognition receptors (14).
Each characteristic triggers distinct downstream pathways and the
production of inflammatory molecules (15). Since different pathogens induce
different immune responses, we aimed to determine whether the
pathogen species could be identified by patterns of serum
inflammatory molecules. In the present study, we examined whether
bacterial and viral infections, gram type of bacteria, different
species of bacteria, or different types of virus could be
characterized by measuring a variety of cytokines and chemokines
using a cytometric bead array. The expression pattern of seven
cytokines (IL-2, IL-4, IL-6, IL-10, IL-17A, TNF-α and IFN-γ) and
five kinds of chemokines [IL-8, RANTES, monokine induced by
interferon-γ (MIG), monocyte chemoattractant protein 1 (MCP-1) and
IP-10] were detected in fever patients.
Materials and methods
Patient enrollment
This study was approved by the Institutional Review
Board of Kaohsiung Medical University Hospital. Patients visiting
the Emergency Department of Kaohsiung Medical University Hospital
(Taiwan, China) with fever or high body temperature (tympanic
temperature, >38.3°C) were sequentially enrolled between May
2013 and October 2014. Patients received treatments and
examinations according to emergency physicians' evaluation. If
patients agreed and provided informed consent, an extra 10 ml blood
would be collected to undergo cytokine test. Serum was separated by
centrifugation at 1,600 × g for 20 min at 4°C, divided in aliquots
and immediately frozen (−80°C) until the time of the assay.
Clinical information including the patients' age, gender, culture
result, laboratory data at the Emergency Department and diagnosis
were collected by a research nurse.
Cytometric bead array
Cytokines and chemokines from the sepsis patients
were analyzed using the Cytometric Bead Array for human
Th1/Th2/Th17 Cytokine kit (cat no. 560484; including IL-2, IL-4,
IL-6, IL-10, IL-17A, TNF-α and IFN-γ) and a Human Chemokine kit
(cat no. 552990; including IL-8, RANTES, MIG, MCP-1, and IP-10; BD
Biosciences, San Jose, CA, USA) following the manufacturer's
instructions. Data was acquired using a BD Accuri C6 flow cytometer
(BD Biosciences) and the data were analyzed using FCAP Array™
version 3.0.1 Software (BD Biosciences) according to a standard
concentration curve.
Statistical analysis
Differences between two independent groups were
analyzed by Mann-Whitney U test. Comparisons between three groups
were via use of the Kruskal-Wallis test with Dunn's multiple
comparison test. All calculations were performed using GraphPad
Prism version 5.03 (GraphPad Software, San Diego, CA, USA).
P<0.05 was considered to indicate a statistically significant
difference.
Results
Laboratory data
Enrolled febrile patients were divided into two
groups: Clinically suspected viral infection and bacterial
infection, according to initial diagnosis. C-reactive protein (CRP)
level and white blood cell (WBC) count are crucial indicators of
sepsis (1,2). High levels of CRP (12.81±17.78 vs.
124.91±90.44 mg/l; P<0.0001) and WBC counts
(4.93±2.5×103 vs. 7.84±5.28×103 cells/µl;
P<0.0001) were detected in patients who were diagnosed as having
bacterial infection compared with patients who were diagnosed with
viral infection (Table I). Compared
to viral infection, significantly higher levels of blood urea
nitrogen (BUN), blood glucose, creatinine (Cr), platelet and
significantly lower levels of hemoglobin (Hb) were observed in
bacterial infection patients.
 | Table I.Patient characteristics and laboratory
data. |
Table I.
Patient characteristics and laboratory
data.
| Characteristic | Viral infection
(n=54) | Bacterial infection
(n=78) | P-value |
|---|
| Male/female |
31/23 |
41/37 | – |
| Age (years) |
43.74±15.79 |
63.81±16.4 | <0.0001 |
| CRP (mg/l) |
12.81±17.78 (n=49) |
124.91±90.44 | <0.0001 |
| WBC
(103/µl) |
4.93±2.50 |
11.84±5.28 | <0.0001 |
| Platelet
(103/µl) | 149.74±58.3 |
203.97±99.43 |
0.0011 |
| Hb |
14.02±4.13 |
12.11±2.13 | <0.0001 |
| BUN |
10.95±4.99 (n=35) |
19.73±13.15 (n=73) | <0.0001 |
| Glu |
128.27±33.36 | 176.07±135 |
0.0496 |
| Cr (mmol/l) |
0.93±0.22 (n=44) |
1.30±0.76 (n=76) |
0.0190 |
Association between viral and
bacterial infection and pattern of inflammatory molecule
expression
We further examined the inflammatory molecules in
patients serum (Table II). Patients
with suspected bacterial infection exhibited significantly higher
levels of IL-6 (63.23±265 vs. 2,533±6,559 pg/ml, P<0.0001),
IL-10 (14.27±16.75 vs. 205.11±741.85 pg/ml, P=0.0101), IL-17A
(18.66±54.93 vs. 34.58±63.99 pg/ml, P=0.0162), TNF-α (0.52±1.37 vs.
19±100.22 pg/ml, P=0.0007), IL-8 (30.31±38.01 vs. 1,249±6,944
pg/ml, P<0.0001) and MIG (660.71±661 vs. 4,533±14,580 pg/ml,
P=0.0367). The present results were comparable to those of previous
reports (5–8).
| Table II.Cytokines and chemokines level in
viral infection and bacterial infection patients. |
Table II.
Cytokines and chemokines level in
viral infection and bacterial infection patients.
| Expression
(pg/ml) | Viral infection
(n=54) | Bacterial infection
(n=78) | P-value |
|---|
| IL-2 |
1.46±1.04 |
3.2±6.67 | 0.7680 |
| IL-4 |
0.99±0.94 |
1.47±3.75 | 0.3510 |
| IL-6 |
63.23±265 |
2,533±6,559 | <0.0001 |
| IL-10 |
14.27±16.75 |
205.11±741.85 | 0.0101 |
| IL-17A |
18.66±54.93 |
34.58±63.99 | 0.0162 |
| TNF-α |
0.52±1.37 |
19±100.22 | 0.0007 |
| IFN-γ |
9.54±19.16 |
16.80±39.61 | 0.8494 |
| IP-10 |
1,944±1,299 |
666.72±766 | <0.0001 |
| MCP-1 |
493.31±679 |
4,533±14,580 | 0.3906 |
| MIG |
660.71±661 |
1,377±1,906 | 0.0367 |
| RANTES |
3,424±3,439 |
4,897±5,006 | 0.5866 |
| IL-8 |
30.31±38.01 |
1,249±6,944 | <0.0001 |
Currently, bacteria identification is primarily
dependent on culture diagnosis in hospitals. However, studies have
shown that culture-negative patients account for 28–48% of severe
sepsis patients in North American, French and Canadian intensive
care units (16–18). There were ~40% of culture-negative
cases in a pan-European study and 49% of culture-negative cases in
sepsis patients in the United States (19,20).
These studies suggest that methods development for pathogen species
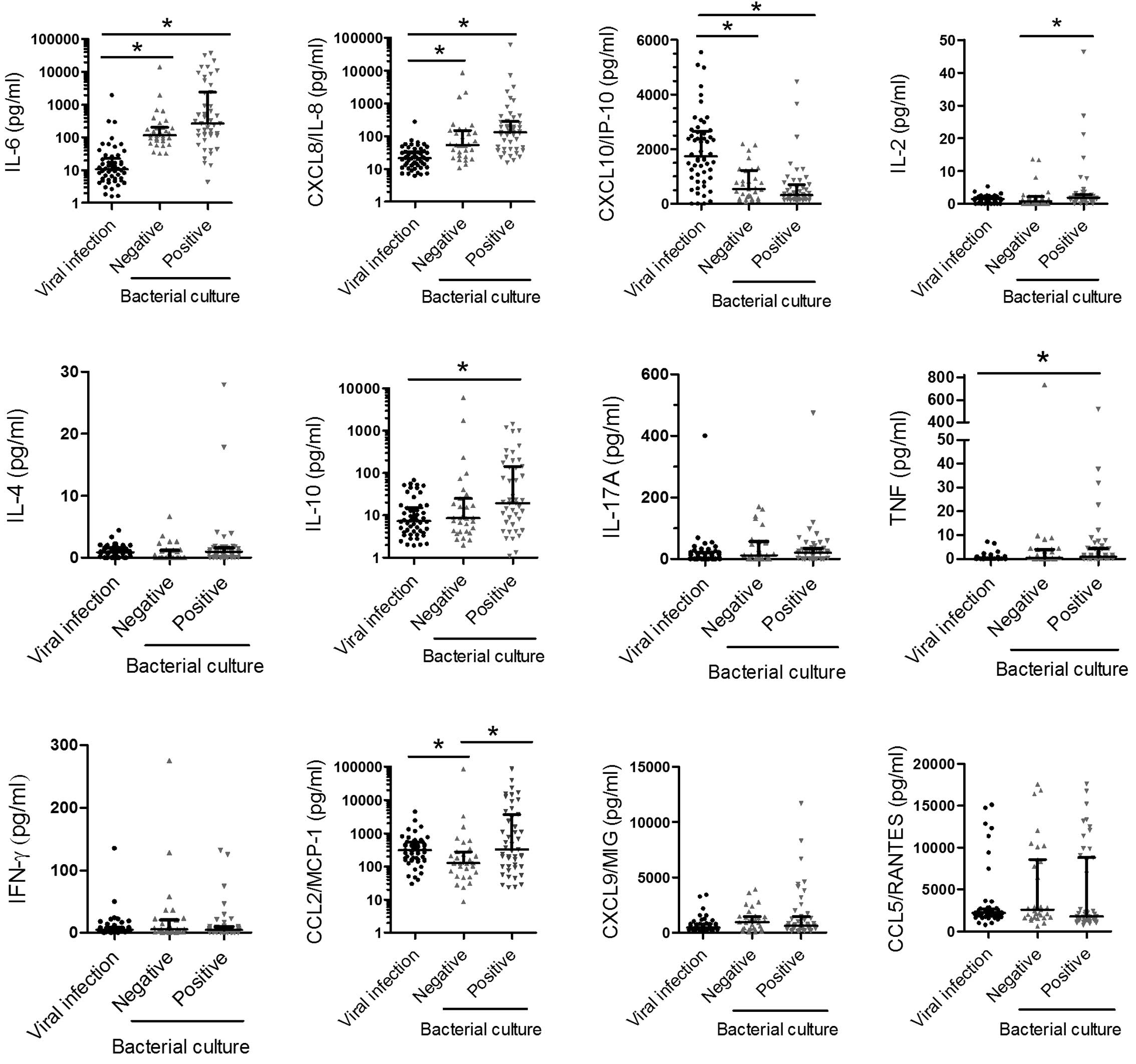
identification is a critical issue. In the present study, there
were 47 culture-positive patients and 37 culture-negative patients.
We investigated whether different patterns of inflammatory
molecules could be observed between viral infection group,
culture-negative group and culture-positive group, particularly
between viral infection and culture-negative group (Fig. 1). There was a statistically
significant difference in IL-6, IL-8 and IP-10 levels between the
viral infection and culture-negative groups or viral infection and
culture-positive groups (Fig. 1).
Similar results were observed in serum CRP level and WBC count
(Fig. 2). Notably, the IL-2 and
MCP-1 levels in the culture-positive group were higher than those
in culture-negative group. However, neither molecule could not
distinguish viral infection from bacterial infection (Table II). The results suggest that IL-6,
IL-8 and IP-10 may be suitable for distinguishing viral infection
from bacterial infection, even though bacterial culture is
negative.
Association between species of
bacteria and pattern of inflammatory molecule expression
Although serum CRP level and WBC counts were markers
of bacterial infection, they showed no significant difference
between gram-negative and gram-positive groups in the
culture-positive group in the present study (data not shown). IL-8
level in gram-negative bacteria infection was higher compared with
gram-positive bacteria infection group among the 47
culture-positive patients though IL-6 and IP-10 level did not show
statistical difference (Table
III). According to the result of bacterial culture, serum from
Escherichia coli, Klebsiella pneumoniae and
Staphylococcus aureus infected patients were selected.
However, the results might indicate that these molecules were not
sufficient to identify the species of bacteria (Table IV).
| Table III.Cytokines and chemokines level in
gram-positive bacteria and gram-negative bacteria. |
Table III.
Cytokines and chemokines level in
gram-positive bacteria and gram-negative bacteria.
|
| Culture-positives
(n=47) |
|
|---|
|
|
|
|
|---|
| Expression
(pg/ml) | Gram-negative
(n=32) | Gram-positive
(n=15) | P-value |
|---|
| IL-6 |
4,058±7,852 |
3,124±8,194 | 0.8284 |
| IP-10 |
551.1±671.72 |
770.9±1,130 | 0.6896 |
| IL-8 |
2,487±10,603 |
217±388 | 0.0293 |
| Table IV.Cytokines and chemokines level in
different bacterial species. |
Table IV.
Cytokines and chemokines level in
different bacterial species.
| Expression
(pg/ml) | Escherichia
coli (n=16) | Klebsiella
pneumoniae (n=7) | Staphylococcus
aureus (n=7) | P-value |
|---|
| IL-6 |
2,552±4,004 |
4,198±5,464 |
414±256.67 | 0.6630 |
| IP-10 |
632.43±829 |
506.23±459.63 |
660.91±760 | 0.9822 |
| IL-8 |
374.85±750 |
638.15±847 |
72.44±57.87 | 0.0688 |
Association between virus type and
pattern of inflammatory molecule expression
In the viral infection group, influenza virus or
dengue virus-infected patients were enrolled after initial
diagnosis. IL-6 level in influenza virus infection group is higher
compared with the dengue virus infection group. However, the IL-6
level in influenza virus group was significantly lower (P<0.05)
compared with the bacterial infection group (Table II). By contrast, serum from dengue
virus infected patients contained significantly higher levels of
IP-10 compared with serum from influenza virus infected patients
(Table V). These results suggested
that IP-10 levels may be used to distinguish influenza virus
infection from dengue virus infection.
| Table V.Cytokines and chemokines level in
influenza virus and dengue virus. |
Table V.
Cytokines and chemokines level in
influenza virus and dengue virus.
| Expression
(pg/ml) | Influenza
(n=18) | Dengue (n=36) | P-value |
|---|
| IL-6 |
167.3±441.4 |
11.20±15.56 | <0.0001 |
| IP-10 |
973.4±745.4 |
2,430±1,244 | <0.0001 |
| IL-8 |
40.78±60.72 |
24.76±15.51 |
0.6797 |
Discussion
Clinical laboratory data, including WBC count and
CRP level, is rapid, sensitive and specific method for detecting
bacterial infection (3,4). Platelet, BUN and Cr levels exhibited
significant differences between suspected viral infection and
bacterial infection patients. As patients with dengue fever, which
affected platelet level, were recruited (21), platelet level was lower in viral
infection patients than in bacterial infection patients. Anemia,
hyperglycemia and elevated BUN and creatinine have been shown to be
associated with bacterial infection (22,23);
however, this may be due to patients selected in the clinically
suspected bacterial infection group being older than patients in a
viral infection group. IL-6, IP-10 and IL-8 may be potential
markers for distinguishing viral infection from bacterial
infection, although bacterial culture was negative. Furthermore,
IP-10 level was highly correlated with dengue virus infection.
Culture-negative state is a commonly observed in
patients diagnosed with sepsis (11–15). In
the present study, serum CRP levels and WBC counts were sensitive
and reliable indexes for distinguishing bacterial infection from
viral infection. Numerous serum molecules, including IL-6, IL-8,
IL-10 and TNF-α, have been reported to be markers of sepsis
(5–7,9–11,24,25).
Similar to the results of serum CRP level and WBC counts,
significantly elevated concentrations of IL-6 and IL-8 were
observed in fever patients in the bacterial infection group,
regardless of culture-positive or culture-negative status. IL-10
and TNF-α were observed to have significant differences between
viral and bacterial infection modalities. However, differences in
IL-10 and TNF-α were observed between culture-positive and viral
infection groups, but not between culture-negative and viral
infection groups. The results suggested that IL-6 and IL-8 were
sensitive and specific markers of bacterial infection.
Accurate and rapid identification of bacterial
species improve clinical outcome (26). However, blood culture typically
requires 1–3 days to become positive for detection of bacteria.
Previous reports suggest that microarray or quantitative polymerase
chain reaction analyses may be a faster and sensitive method for
clinical identification of bacterial infection (27). It is reported that procalcitonin, but
not CRP and WBC counts, is associated with gram-negative bacteria
(28). Due to the different
components of the cell walls of gram-positive and gram-negative
bacteria, different patterns of immune responses may be induced
in vitro (29,30). Therefore, we hypothesized that
inflammatory molecules in the serum may provide information for
identifying bacterial species. Gram-negative bacteria induce higher
levels of IL-6, IL-10 and IL-8 compared with gram-positive bacteria
in human monocytes (29–31). To the best of our knowledge, there
are few studies reporting whether cytokines or chemokines could be
markers to distinguish infection of gram-positive or gram-negative
bacteria in patient serum. The present results revealed that IL-8
was the only molecule which exhibited a significant difference in
expression between gram-negative and gram-positive bacteria. In the
present study, bacterial species could not be identified through
the pattern of inflammatory molecules. These results imply that
serum inflammatory molecule levels alone were insufficient data for
identifying bacterial species. As different species of bacteria
have common characteristics (such as lipopolysaccharide on
gram-negative bacteria), a similar pattern of inflammatory
molecules were produced by innate immune system (32). However, in order to identify
bacterial species on the basis of the pattern of serum molecule
expression levels, the present findings suggest that the detection
of more molecules is necessary.
In the present study, IP-10 level in the viral
infection group was found to be higher than in the bacterial
infection group. Previous studies have indicated that IP-10 level
is associated with viral infection, including hepatitis C virus
(HCV) infection and HCV-human immunodeficiency virus co-infection
(33–35). Dengue virus infection is associated
with higher concentrations of IP-10 in patient serum compared with
healthy individuals (36).
Furthermore, IP-10 is induced by viral and bacterial infection.
Higher levels of IP-10 may be detected in sepsis, severe sepsis and
septic shock groups compared with systemic inflammatory response
syndrome (37). High levels of IP-10
have previously been detected in preterm infants with bacterial
infection (12). Although bacterial
and viral infection induce IP-10 level, the highest levels of IP-10
in the present study were observed among influenza virus,
culture-negative and culture-positive groups (data not shown).
IP-10 is a ligand for CXCR3 chemokine receptor, and expression of
IP-10 recruits CXCR3 expressing NK and T cells (38). CXCR3 and IP-10 defective mice
exhibited a lower survival rate compared with wild type mice in a
dengue infection model (39). The
CXCR3-IP-10 pathway may be essential for clearance of dengue virus,
which may explain why dengue virus induced the highest level of
IP-10 expression in the present study.
In summary, bacterial infection was associated with
the production of IL-6, IL-8 and IP-10. In addition, an increased
IL-8 level was associated with gram-negative bacteria and a high
IP-10 level was associated with dengue virus infection. Although
the pattern of inflammatory molecules alone could not be used to
identify bacteria species, these molecules may provide useful
information for diagnosis and clinical treatment.
Acknowledgements
The present study was supported by grants from the
Ministry of Science and Technology (grant no.
104-2320-B-037-014-MY3) and the Kaohsiung Medical University
Hospital Research Foundation (grant no. KMUH101-1M65).
References
|
1
|
Fernández Lopez A, Luaces Cubells C,
García García JJ and Fernández Pou J: Spanish Society of Pediatric
Emergencies: Procalcitonin in pediatric emergency departments for
the early diagnosis of invasive bacterial infections in febrile
infants: Results of a multicenter study and utility of a rapid
qualitative test for this marker. Pediatr Infect Dis J. 22:895–903.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fitch MT and van de Beek D: Emergency
diagnosis and treatment of adult meningitis. Lancet Infect Dis.
7:191–200. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Andreola B, Bressan S, Callegaro S,
Liverani A, Plebani M and Da Dalt L: Procalcitonin and C-reactive
protein as diagnostic markers of severe bacterial infections in
febrile infants and children in the emergency department. Pediatr
Infect Dis J. 26:672–677. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hatherill M, Tibby SM, Sykes K, Turner C
and Murdoch IA: Diagnostic markers of infection: Comparison of
procalcitonin with C reactive protein and leucocyte count. Arch Dis
Child. 81:417–421. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
van der Poll T, de Waal Malefyt R, Coyle
SM and Lowry SF: Antiinflammatory cytokine responses during
clinical sepsis and experimental endotoxemia: Sequential
measurements of plasma soluble interleukin (IL)-1 receptor type II,
IL-10, and IL-13. J Infect Dis. 175:118–122. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Damas P, Reuter A, Gysen P, Demonty J,
Lamy M and Franchimont P: Tumor necrosis factor and interleukin-1
serum levels during severe sepsis in humans. Crit Care Med.
17:975–978. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Damas P, Ledoux D, Nys M, Vrindts Y, De
Groote D, Franchimont P and Lamy M: Cytokine serum level during
severe sepsis in human Il-6 as a marker of severity. Ann Surg.
215:356–362. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Grobmyer SR, Lin E, Lowry SF, Rivadeneira
DE, Potter S, Barie PS and Nathan CF: Elevation of IL-18 in human
sepsis. J Clin Immunol. 20:212–215. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Patel RT, Deen KI, Youngs D, Warwick J and
Keighley MR: Interleukin-6 is a prognostic indicator of outcome in
severe intra-abdominal sepsis. Br J Surg. 81:1306–1308. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Casey LC, Balk RA and Bone RC: Plasma
cytokine and endotoxin levels correlate with survival in patients
with the sepsis syndrome. Ann Intern Med. 119:771–778. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kurt AN, Aygun AD, Godekmerdan A, Kurt A,
Dogan Y and Yilmaz E: Serum IL-1beta, IL-6, IL-8, and TNF-alpha
levels in early diagnosis and management of neonatal sepsis.
Mediators Inflamm. 2007:313972007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ng PC, Li K, Chui KM, Leung TF, Wong RP,
Chu WC, Wong E and Fok TF: IP-10 is an early diagnostic marker for
identification of late-onset bacterial infection in preterm
infants. Pediatr Res. 61:93–98. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ng PC, Li K, Leung TF, Wong RP, Li G, Chui
KM, Wong E, Cheng FW and Fok TF: Early prediction of sepsis-induced
disseminated intravascular coagulation with interleukin-10,
interleukin-6, and RANTES in preterm infants. Clin Chem.
52:1181–1189. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Akira S, Uematsu S and Takeuchi O:
Pathogen recognition and innate immunity. Cell. 124:783–801. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
O'Shea JJ and Murray PJ: Cytokine
signaling modules in inflammatory responses. Immunity. 28:477–487.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kumar A, Roberts D, Wood KE, Light B,
Parrillo JE, Sharma S, Suppes R, Feinstein D, Zanotti S, Taiberg L,
et al: Duration of hypotension before initiation of effective
antimicrobial therapy is the critical determinant of survival in
human septic shock. Crit Care Med. 34:1589–1596. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Martin CM, Priestap F, Fisher H, Fowler
RA, Heyland DK, Keenan SP, Longo CJ, Morrison T, Bentley D and
Antman N: STAR Registry Investigators: A prospective, observational
registry of patients with severe sepsis: The Canadian sepsis
treatment and response registry. Crit Care Med. 37:81–88. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Brun-Buisson C, Meshaka P, Pinton P and
Vallet B: EPISEPSIS Study Group: EPISEPSIS: A reappraisal of the
epidemiology and outcome of severe sepsis in French intensive care
units. Intensive Care Med. 30:580–588. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Martin GS, Mannino DM, Eaton S and Moss M:
The epidemiology of sepsis in the United States from 1979 through
2000. N Engl J Med. 348:1546–1554. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Vincent JL, Sakr Y, Sprung CL, Ranieri VM,
Reinhart K, Gerlach H, Moreno R, Carlet J, Le Gall JR and Payen D:
Sepsis Occurrence in Acutely Ill Patients Investigators: Sepsis in
European intensive care units: Results of the SOAP study. Crit Care
Med. 34:344–353. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hottz ED, Medeiros-de-Moraes IM,
Vieira-de-Abreu A, de Assis EF, Vals-de-Souza R, Castro-Faria-Neto
HC, Weyrich AS, Zimmerman GA, Bozza FA and Bozza PT: Platelet
activation and apoptosis modulate monocyte inflammatory responses
in dengue. J Immunol. 193:1864–1872. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Van Cromphaut SJ, Vanhorebeek I and Van
den Berghe G: Glucose metabolism and insulin resistance in sepsis.
Curr Pharm Des. 14:1887–1899. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yegenaga I, Hoste E, Van Biesen W,
Vanholder R, Benoit D, Kantarci G, Dhondt A, Colardyn F and Lameire
N: Clinical characteristics of patients developing ARF due to
sepsis/systemic inflammatory response syndrome: Results of a
prospective study. Am J Kidney Dis. 43:817–824. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Livaditi O, Kotanidou A, Psarra A,
Dimopoulou I, Sotiropoulou C, Augustatou K, Papasteriades C,
Armaganidis A, Roussos C, Orfanos SE and Douzinas EE: Neutrophil
CD64 expression and serum IL-8: sensitive early markers of severity
and outcome in sepsis. Cytokine. 36:283–290. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wunder C, Eichelbrönner O and Roewer N:
Are IL-6, IL-10 and PCT plasma concentrations reliable for outcome
prediction in severe sepsis? A comparison with APACHE III and SAPS
II. Inflamm Res. 53:158–163. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Andrade SS, Bispo PJ and Gales AC:
Advances in the microbiological diagnosis of sepsis. Shock.
30(Suppl 1): S41–S46. 2008. View Article : Google Scholar
|
|
27
|
Tissari P, Zumla A, Tarkka E, Mero S,
Savolainen L, Vaara M, Aittakorpi A, Laakso S, Lindfors M,
Piiparinen H, et al: Accurate and rapid identification of bacterial
species from positive blood cultures with a DNA-based microarray
platform: An observational study. Lancet. 375:224–230. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Charles PE, Ladoire S, Aho S, Quenot JP,
Doise JM, Prin S, Olsson NO and Blettery B: Serum procalcitonin
elevation in critically ill patients at the onset of bacteremia
caused by either gram negative or gram positive bacteria. BMC
Infect Dis. 8:382008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Skovbjerg S, Martner A, Hynsjö L, Hessle
C, Olsen I, Dewhirst FE, Tham W and Wold AE: Gram-positive and
gram-negative bacteria induce different patterns of cytokine
production in human mononuclear cells irrespective of taxonomic
relatedness. J Interferon Cytokine Res. 30:23–32. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Hessle CC, Andersson B and Wold AE:
Gram-positive and Gram-negative bacteria elicit different patterns
of pro-inflammatory cytokines in human monocytes. Cytokine.
30:311–318. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Engel A, Mack E, Kern P and Kern WV: An
analysis of interleukin-8, interleukin-6 and C-reactive protein
serum concentrations to predict fever, gram-negative bacteremia and
complicated infection in neutropenic cancer patients. Infection.
26:213–221. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Feezor RJ, Oberholzer C, Baker HV, Novick
D, Rubinstein M, Moldawer LL, Pribble J, Souza S, Dinarello CA,
Ertel W and Oberholzer A: Molecular characterization of the acute
inflammatory response to infections with gram-negative versus
gram-positive bacteria. Infect Immun. 71:5803–5813. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Berres ML, Trautwein C, Schmeding M,
Eurich D, Tacke F, Bahra M, Neuhaus P, Neumann UP and Wasmuth HE:
Serum chemokine CXC ligand 10 (CXCL10) predicts fibrosis
progression after liver transplantation for hepatitis C infection.
Hepatology. 53:596–603. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zeremski M, Markatou M, Brown QB, Dorante
G, Cunningham-Rundles S and Talal AH: Interferon gamma-inducible
protein 10: A predictive marker of successful treatment response in
hepatitis C virus/HIV-coinfected patients. J Acquir Immune Defic
Syndr. 45:262–268. 2007.PubMed/NCBI
|
|
35
|
Reiberger T, Aberle JH, Kundi M,
Kohrgruber N, Rieger A, Gangl A, Holzmann H and Peck-Radosavljevic
M: IP-10 correlates with hepatitis C viral load, hepatic
inflammation and fibrosis and predicts hepatitis C virus relapse or
non-response in HIV-HCV coinfection. Antivir Ther. 13:969–976.
2008.PubMed/NCBI
|
|
36
|
Conroy AL, Gélvez M, Hawkes M, Rajwans N,
Liles WC, Villar-Centeno LA and Kain KC: Host biomarkers
distinguish dengue from leptospirosis in Colombia: A case-control
study. BMC Infect Dis. 14:352014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Punyadeera C, Schneider EM, Schaffer D,
Hsu HY, Joos TO, Kriebel F, Weiss M and Verhaegh WF: A biomarker
panel to discriminate between systemic inflammatory response
syndrome and sepsis and sepsis severity. J Emerg Trauma Shock.
3:26–35. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Loetscher M, Gerber B, Loetscher P, Jones
SA, Piali L, Clark-Lewis I, Baggiolini M and Moser B: Chemokine
receptor specific for IP10 and Mig: Structure, function, and
expression in activated T-lymphocytes. J Exp Med. 184:963–969.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Hsieh MF, Lai SL, Chen JP, Sung JM, Lin
YL, Wu-Hsieh BA, Gerard C, Luster A and Liao F: Both CXCR3 and
CXCL10/IFN-inducible protein 10 are required for resistance to
primary infection by dengue virus. J Immunol. 177:1855–1863. 2006.
View Article : Google Scholar : PubMed/NCBI
|