Introduction
Aortic aneurysm (AA), defined as an enlargement of
the aorta to greater than 1.5 times normal size (1) is usually asymptotic, but when rupture
occurs, this may lead to internal bleeding, shock and mortality,
unless treated immediately (2).
Although AA is rather rare with an incidence of approximately 10
per 100,000 for thoracic aortic aneurysm (ΤΑΑ) (3) and 55–298 per 100,000 for abdominal
aortic aneurysm (AAA) (4), the
burden of the disease is heavy and may be underestimated (5–7). Given
the high total mortality estimated at 80–100% for ruptured AA
(8,9), the best way to reduce the overall
mortality of the disease may be to detect and treat it prior to
rupture. In fact, many predictors or predictive models of mortality
risk in AA patients have been reported (10–14), but
further validation is required. Herein, we focused on AA patients
in intensive care unit (ICU) and investigated the predictive value
of serum anion gap on ICU mortality, a routine clinical indicator
which has been reported to be associated with mortality of several
diseases (15–18). Although a few studies have reported
the association between anion gap with ICU mortality (19,20), to
the best of our knowledge, no research to date has specially
investigated the association in AA patients admitted to ICU.
Considering the extremely low incidence of AA, we performed a
retrospective analysis on a large publicly accessible clinical
database, hoping to clarify the association between anion gap and
ICU mortality.
Patients and methods
Database introduction
The retrospective analysis was conducted using data
from the Medical Information Mart for Intensive Care III
(MIMIC-III) database (version 1.4) (21), a large and freely-available database
comprising deidentified health-related data of patients admitted to
ICU of the Beth Israel Deaconess Medical Center between 2001 and
2012. The database contains information including demographics,
laboratory test results, and clinical outcomes. The access of the
database was approved by the institutional review boards of both
Beth Israel Deaconess Medical Center and Massachusetts Institute of
Technology Affiliates.
Study design
Adult patients (age ≥18 years old) with first
hospital admission and first ICU admission were considered for
inclusion. AA patients were selected according to their primary
diagnoses based on ICD-9 codes (4412–4415, and 4419), and patients
with a length of ICU stay less than 24 h or a missing value of
admission serum anion gap were excluded.
We used the codes from the MIMIC Code Repository
(https://github.com/MIT-LCP/mimic-code) (22) to extract data from the database.
Variables were extracted or calculated including admission serum
anion gap (item ID=50868 in the database, detected within 24 h
after ICU admission), severity scores including SOFA (23) and APACHE III (24), sepsis defined by ICD-9 codes (99592
and 78552), sepsis defined by Angus criteria (25) and comorbidities (26) based on ICD-9 codes. For patients
>89 years old, date of birth had been shifted to exactly 300
years before by the database to obscure age, therefore this was
corrected (age-300+89) prior to analysis. No informed consent was
required as the data were anonymized.
Outcomes
ICU mortality was chosen as the primary study
outcome before analysis. Hospital mortality, length of ICU stay,
and length of hospital stay were also calculated. Although only
patients of first hospital admission were included, it is possible
for a patient to be transferred from one type of ICU to another. In
this case, the primary outcome ICU mortality and length of ICU stay
were determined only by the first ICU stay. Apart from statistical
description, only the primary outcome was analyzed further.
Statistical analysis
Data are presented as median and interquartile range
(IQR) for continuous variables and numbers and percentages for
categorical variables. Kruskal Wallis and Chi-square (or Fisher's
exact) tests were used to analyze continuous and categorical
variables, respectively. Relationship between admission serum anion
gap and ICU mortality was explored using the smoothing plot with an
adjustment for potential confounders (age, sex, and SOFA were
selected before analysis). A two-piecewise linear regression model
was applied to examine the threshold effect of admission serum
anion gap on ICU mortality according to the smoothing plot. Factors
associated with ICU mortality were evaluated by univariate logistic
analysis and variables that showed statistically significant
association with ICU mortality in the univariate analysis
(P<0.05) were included in the multivariable logistic regression
model, but variables with missing values >10% were excluded.
Considering that there was a certain overlap in the two severity
scores and sepsis based on different criteria, we only selected
SOFA and sepsis based on ICD-9 codes to be enrolled in the
multivariable analysis if the variables were statistically
significant in the univariate analysis. If a nonlinear relationship
and a threshold effect were found in the previous analysis, then
the subjects were stratified according to the threshold level and
the logistic analysis was repeated. Receiver operating
characteristic (ROC) curves were constructed and the area under the
ROC curve (AUC) was calculated to evaluate the predictions.
Consistency of the results in several subgroups was also explored
using logistic regression models. To maximize statistical power and
minimize potential bias that may have occurred if variables with
missing values >10% were excluded from analyses, missing values
of continuous and categorical covariates in outcome analysis were
handled using multiple imputation with 5 imputed data sets, and
results were pooled according to Rubin's rules (27). A multivariable analysis was also
performed after excluding patients with ruptured AA. A P-value of
<0.05 was considered statistically significant. Empower(R)
(www.empowerstats.com; X&Y solutions,
Inc., Boston, MA, USA) and R software, version 3.4.3 (http://www.r-project.org) were used for all
statistical analyses.
Results
Population and baseline
characteristics
A total of 273 patients were included and analyzed
(Fig. 1). The number of missing
values for all variables are presented in Table I. As shown in Table II, The median age of the study
subjects was 73.16 years (IQR 65.14–80.06 years) and 154 of the 273
cases (56.41%) were male. The median admission serum anion gap was
13.00 mEq/l (IQR 11.00–15.00 mEq/l) with a median SOFA score of 5
(IQR 4–8). Among them, 8 (2.93%) patients were diagnosed as sepsis
based on ICD-9 codes and 227 (83.15%) patients required
ventilation. The five most common comorbidities were chronic
pulmonary disease (28.94%), fluid and electrolyte disorders
(27.84%), peripheral vascular disorder (26.01%), coagulopathy
(17.22%), and uncomplicated diabetes (15.02%).
 | Table I.Numbers of subjects with missing
values. |
Table I.
Numbers of subjects with missing
values.
| Variables | Numbers of subjects
with specific missing value |
|---|
| Hemoglobin | 1 |
| Lactate | 61 |
| Platelet | 1 |
| PTT | 11 |
| INR | 12 |
| PT | 12 |
| WBC | 2 |
| Urine output in
first day | 4 |
| Heartrate | 2 |
| Systolic
pressure | 3 |
| Diastolic
pressure | 3 |
| Respiratory
rate | 2 |
| Temperature | 23 |
| SpO2 | 2 |
| Table II.Clinical characteristics of study
subjects. |
Table II.
Clinical characteristics of study
subjects.
| Parameter | All (n=273) | Survivors
(n=249) | Non-survivors
(n=24) | P-value |
|---|
| Age (years) | 73.16
(65.14–80.06) | 72.58
(64.59–79.76) | 77.74
(72.11–82.80) | 0.009 |
| Sex (male), n
(%) | 154 (56.41%) | 143 (57.43%) | 11 (45.83%) | 0.274 |
| Type of aortic
aneurysm |
|
|
| 0.002 |
|
Thoracic aneurysm without
mention of rupture | 109 (39.93%) | 104 (41.77%) | 5 (20.83%) |
|
|
Abdominal aneurysm
(ruptured) | 48 (17.58%) | 37 (14.86%) | 11 (45.83%) |
|
|
Abdominal aneurysm without
mention of rupture | 116 (42.49%) | 108 (43.37%) | 8 (33.33%) |
|
| Anion gap
(mEq/l) | 13.00
(11.00–15.00) | 13.00
(11.00–15.00) | 17.50
(15.75–22.50) | <0.001 |
| ICU mortality | 24 (8.79%) |
|
|
|
| Hospital
mortality | 27 (9.89%) | 3 (1.20%) | 24 (100.00%) | <0.001 |
| ICU length of stay
(days) | 3.23
(1.90–9.22) | 3.16
(1.81–8.99) | 10.88
(2.58–15.06) | 0.008 |
| Hospital length of
stay (days) | 9.32
(6.25–16.92) | 9.30
(6.39–17.04) | 10.84
(4.62–16.38) | 0.317 |
| Severity score |
|
|
|
|
|
SOFA | 5.00
(4.00–8.00) | 5.00
(3.00–7.00) | 9.00
(8.00–11.25) | <0.001 |
| APACHE
III | 39.00
(29.00–54.00) | 38.00
(28.00–50.00) | 70.00
(52.00–85.75) | <0.001 |
| Vital signs |
|
|
|
|
|
Heartrate (bpm) | 80.60
(73.07–88.98) | 79.86
(72.69–87.77) | 88.60
(83.54–95.75) | 0.002 |
|
Systolic pressure (mmHg) | 113.98
(106.58–124.29) | 114.80
(106.79–124.01) | 109.67
(104.60–124.98) | 0.273 |
|
Diastolic pressure (mmHg) | 57.68
(52.97–62.38) | 57.32
(52.60–61.97) | 59.78
(57.10–65.19) | 0.036 |
|
Respiratory rate (bpm) | 17.26
(14.96–19.27) | 17.02
(14.94–19.21) | 18.69
(16.13–21.00) | 0.040 |
|
Temperature (°C) | 37.64
(37.10–38.10) | 37.67
(37.18–38.10) | 37.25
(36.72–37.82) | 0.041 |
| SpO2
(%) | 93.00
(91.00–95.00) | 93.00
(91.00–95.00) | 92.00
(86.75–94.00) | 0.023 |
| Urine output in
first day (ml) | 1,670.00
(981.00–2,580.00) | 1,730.00
(1,071.50–2,602.50) | 450.00
(246.25–1,342.00) | <0.001 |
| RTT in first
day | 5 (1.83%) | 2 (0.80%) | 3 (12.50%) | 0.005 |
| Ventilation in
first day | 227 (83.15%) | 205 (82.33%) | 22 (91.67%) | 0.390 |
| Sepsis (based on
ICD-9 codes) | 8 (2.93%) | 4 (1.61%) | 4 (16.67%) | 0.003 |
| Sepsis (based on
Angus criteria) | 78 (28.57%) | 63 (25.30%) | 15 (62.50%) | <0.001 |
| Lab
examination |
|
|
|
|
| WBC
(K/ul) | 12.50
(9.70–15.80) | 12.10
(9.60–15.65) | 14.75
(12.90–16.92) | 0.025 |
|
Platelet (K/ul) | 147.50
(111.88–190.12) | 151.00
(112.38–192.75) | 132.00
(106.00–149.88) | 0.027 |
|
Hemoglobin (g/dl) | 9.00
(7.80–10.30) | 9.25
(7.90–10.33) | 8.20
(6.97–8.80) | 0.002 |
|
Creatinine (mg/dl) | 1.10
(0.80–1.60) | 1.00
(0.80–1.50) | 1.95
(1.45–2.20) | <0.001 |
| BUN
(mg/dl) | 19.00
(15.00–26.00) | 18.00
(15.00–25.00) | 27.50
(21.75–35.75) | <0.001 |
| Glucose
(mg/dl) | 172.00
(140.00–204.00) | 171.00
(138.00–200.00) | 215.00
(155.75–316.25) | 0.005 |
| Lactate
(mmol/l) | 3.15
(1.98–5.30) | 2.80
(1.90–4.60) | 7.00
(5.20–10.80) | <0.001 |
| PTT
(sec) | 35.57
(30.54–42.75) | 34.80
(30.16–42.21) | 42.72
(36.30–65.26) | 0.002 |
|
INR | 1.30
(1.20–1.50) | 1.30
(1.16–1.45) | 1.45
(1.20–1.77) | 0.064 |
| PT
(sec) | 14.45
(13.40–15.85) | 14.40
(13.35–15.64) | 15.85
(13.45–17.35) | 0.082 |
| Comorbidities |
|
|
|
|
|
Congestive heart failure | 11 (4.03%) | 10 (4.02%) | 1 (4.17%) | 1.000 |
| Cardiac
arrhythmias | 12 (4.40%) | 11 (4.42%) | 1 (4.17%) | 1.000 |
|
Valvular disease | 3 (1.10%) | 2 (0.80%) | 1 (4.17%) | 0.242 |
|
Pulmonary circulation
disorder | 2 (0.73%) | 2 (0.80%) | 0 (0.00%) | 1.000 |
|
Peripheral vascular
disorder | 71 (26.01%) | 64 (25.70%) | 7 (29.17%) | 0.808 |
|
Hypertension | 23 (8.42%) | 19 (7.63%) | 4 (16.67%) | 0.130 |
|
Paralysis | 7 (2.56%) | 6 (2.41%) | 1 (4.17%) | 0.479 |
| Other
neurological disease | 4 (1.47%) | 2 (0.80%) | 2 (8.33%) | 0.040 |
| Chronic
pulmonary disease | 79 (28.94%) | 72 (28.92%) | 7 (29.17%) | 1.000 |
|
Uncomplicated diabetes | 41 (15.02%) | 39 (15.66%) | 2 (8.33%) | 0.549 |
|
Complicated diabetes | 4 (1.47%) | 4 (1.61%) | 0 (0.00%) | 1.000 |
|
Hypothyroidism | 26 (9.52%) | 23 (9.24%) | 3 (12.50%) | 0.487 |
| Renal
failure | 31 (11.36%) | 26 (10.44%) | 5 (20.83%) | 0.167 |
| Liver
disease | 8 (2.93%) | 6 (2.41%) | 2 (8.33%) | 0.150 |
|
Lymphoma | 3 (1.10%) | 3 (1.20%) | 0 (0.00%) | 1.000 |
|
Metastatic cancer | 2 (0.73%) | 2 (0.80%) | 0 (0.00%) | 1.000 |
| Solid
tumor | 4 (1.47%) | 4 (1.61%) | 0 (0.00%) | 1.000 |
|
Rheumatoid arthritis | 8 (2.93%) | 7 (2.81%) | 1 (4.17%) | 0.526 |
|
Coagulopathy | 47 (17.22%) | 39 (15.66%) | 8 (33.33%) | 0.043 |
|
Obesity | 21 (7.69%) | 21 (8.43%) | 0 (0.00%) | 0.233 |
| Weight
loss | 7 (2.56%) | 7 (2.81%) | 0 (0.00%) | 1.000 |
| Fluid
and electrolyte disorders | 76 (27.84%) | 67 (26.91%) | 9 (37.50%) | 0.339 |
| Blood
loss anemia | 5 (1.83%) | 4 (1.61%) | 1 (4.17%) | 0.371 |
|
Deficiency anemias | 35 (12.82%) | 34 (13.65%) | 1 (4.17%) | 0.333 |
| Alcohol
abuse | 8 (2.93%) | 8 (3.21%) | 0 (0.00%) | 1.000 |
|
Psychoses | 4 (1.47%) | 3 (1.20%) | 1 (4.17%) | 0.309 |
|
Depression | 12 (4.40%) | 12 (4.82%) | 0 (0.00%) | 0.608 |
Survival status of the population
The ICU mortality was 8.79% with 24 non-survivors
and 249 survivors and the hospital mortality was 9.89% (27/273).
The median length of ICU stay and hospital stay was 3.23 (IQR
1.90–9.22) and 9.32 (IQR 6.25–16.92) days, respectively. As shown
in Table II, non-survivors had
significantly higher SOFA and APACHE (P<0.001). Furthermore,
they were more likely to suffer from sepsis and require renal
replacement therapy in first day. A significantly lower admission
serum anion gap was observed in survivors (P<0.001).
Association between serum anion gap on
admission and ICU mortality
Further analysis indicated that admission serum
anion gap increased with increased ICU mortality when patients were
stratified according to serum anion gap levels on admission
(Table III), but no significant
nonlinear relationship or threshold effect between them were
observed (Fig. 2 and Table IV). After adjustment for potential
confounders according to the univariate analysis (presented in
Table V), admission serum anion gap
was found to be significantly associated with ICU mortality [odds
ratio (OR) 1.38 per 1 mEq/l increase, 95% confidence interval (CI),
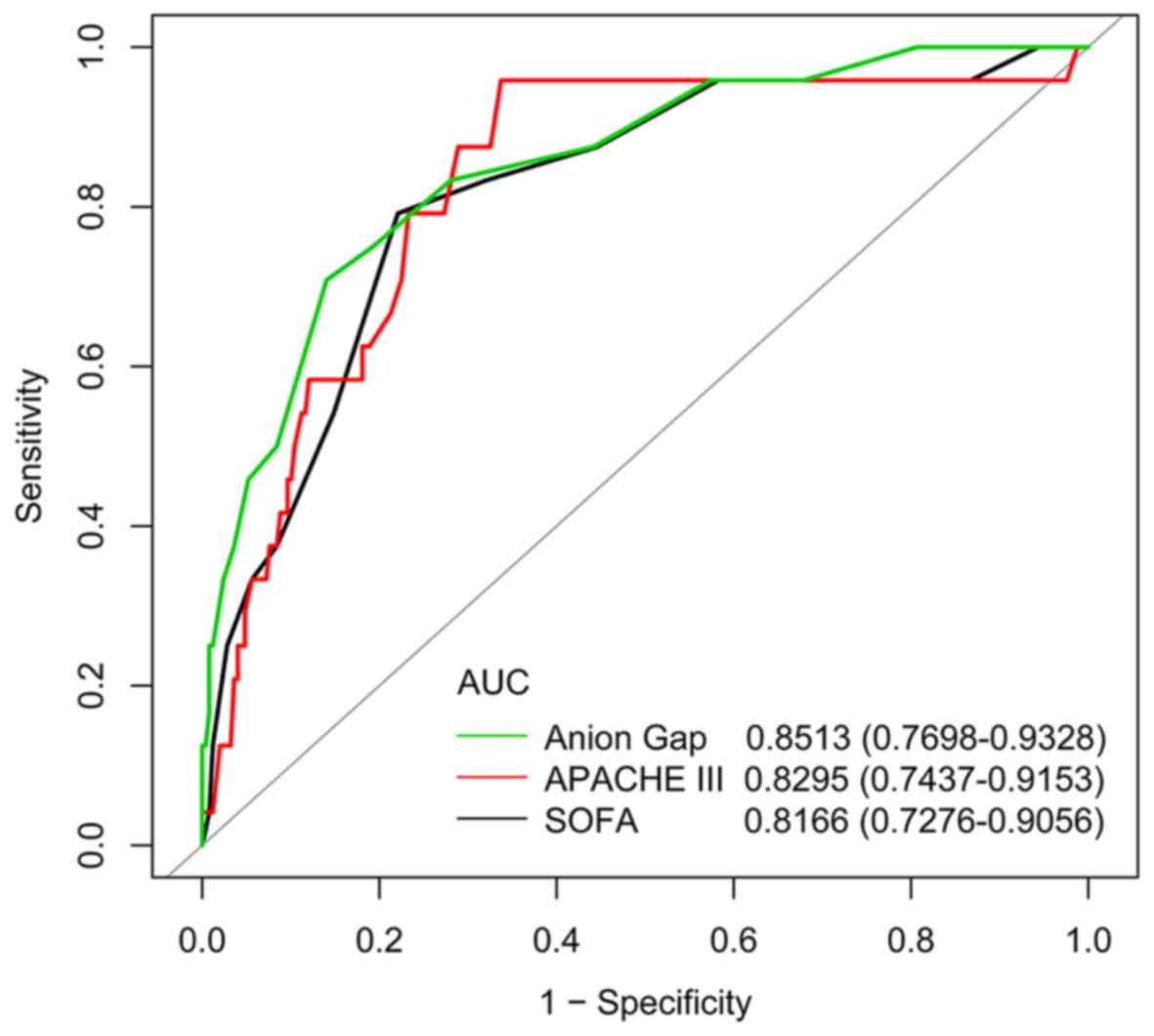
1.08–1.76; P=0.0088] (Table VI). As
shown in Fig. 3, AUC of serum anion
gap for discrimination of survivors and non-survivors was 0.8513
(95% CI, 0.7698–0.9328), which suggested its potentially efficient
predictive role in ICU mortality for AA patients.
| Table III.Clinical characteristics of study
subjects stratified by anion gap levels on ICU admission. |
Table III.
Clinical characteristics of study
subjects stratified by anion gap levels on ICU admission.
| Parameter | Tertile 1
(n=81) | Tertile 2
(n=61) | Tertile 3
(n=131) | P-value |
|---|
| Age (years) | 69.77
(60.37–79.58) | 69.67
(63.65–78.14) | 76.14
(70.24–82.05) | <0.001 |
| Sex (male),
n(%) | 39 (48.15%) | 35 (57.38%) | 80 (61.07%) | 0.180 |
| Type of aortic
aneurysm |
|
|
| <0.001 |
|
Thoracic aneurysm without
mention of rupture | 45 (55.56%) | 31 (50.82%) | 33 (25.19%) |
|
|
Abdominal aneurysm
(ruptured) | 5 (6.17%) | 7 (11.48%) | 36 (27.48%) |
|
|
Abdominal aneurysm without
mention of rupture | 31 (38.27%) | 23 (37.70%) | 62 (47.33%) |
|
| Anion Gap
(mEq/l) | 10.00
(9.00–11.00) | 13.00
(12.00–13.00) | 16.00
(14.00–17.50) | <0.001 |
| ICU mortality | 1 (1.23%) | 2 (3.28%) | 21 (16.03%) | <0.001 |
| Hospital
mortality | 2 (2.47%) | 3 (4.92%) | 22 (16.79%) | <0.001 |
| ICU length of stay
(days) | 2.27
(1.33–4.10) | 3.11
(1.44–8.55) | 5.75
(2.20–12.60) | <0.001 |
| Hospital length of
stay (days) | 7.84
(5.46–12.28) | 9.27
(6.26–14.63) | 12.22
(6.54–20.45) | 0.002 |
| Severity score |
|
|
|
|
|
SOFA | 5.00
(3.00–6.00) | 4.00
(3.00–7.00) | 6.00
(4.50–9.00) | <0.001 |
| APACHE
III | 33.00
(24.00–44.00) | 36.00
(27.00–46.00) | 49.00
(36.00–64.00) | <0.001 |
| Vital signs |
|
|
|
|
|
Heartrate (bpm) | 79.79
(72.67–86.79) | 79.86
(73.07–87.19) | 81.90
(73.75–91.75) | 0.438 |
|
Systolic pressure (mmHg) | 109.73
(105.03–118.55) | 117.89
(108.29–124.83) | 117.79
(107.62–128.83) | 0.002 |
|
Diastolic pressure (mmHg) | 56.74
(52.82–61.74) | 57.59
(53.28–62.43) | 58.61
(53.25–63.48) | 0.508 |
|
Respiratory rate (bpm) | 16.36
(14.63–18.54) | 17.31
(15.22–18.58) | 18.08
(15.21–19.91) | 0.029 |
|
Temperature (°C) | 37.82
(37.40–38.18) | 37.60
(37.03–38.00) | 37.60
(37.03–38.06) | 0.115 |
| SpO2
(%) | 93.00
(91.00–95.00) | 93.00
(91.00–95.00) | 93.00
(91.00–95.00) | 0.357 |
| Urine output in
first day (ml) | 2,200.00
(1,605.00–2,730.00) | 1,670.00
(1,087.00–2,515.00) | 1,172.00
(650.00–2,229.50) | <0.001 |
| RTT in first
day | 0 (0.00%) | 0 (0.00%) | 5 (3.82%) | 0.085 |
| Ventilation in
first day | 71 (87.65%) | 53 (86.89%) | 103 (78.63%) | 0.158 |
| Sepsis (based on
ICD-9 codes) | 2 (2.47%) | 0 (0.00%) | 6 (4.58%) | 0.257 |
| Sepsis (based on
Angus criteria) | 11 (13.58%) | 15 (24.59%) | 52 (39.69%) | <0.001 |
| Lab
examination |
|
|
|
|
| WBC
(K/ul) | 13.00
(9.70–15.60) | 11.90
(10.10–13.83) | 12.10
(9.22–16.67) | 0.647 |
|
Platelet (K/ul) | 153.50
(121.00–190.00) | 151.00
(108.00–184.00) | 137.50
(108.88–194.00) | 0.747 |
|
Hemoglobin (g/dl) | 8.90
(7.90–10.00) | 9.30
(7.70–10.30) | 9.25
(7.82–10.28) | 0.612 |
|
Creatinine (mg/dl) | 0.80
(0.70–1.10) | 1.00
(0.80–1.30) | 1.40
(1.00–1.95) | <0.001 |
| BUN
(mg/dl) | 16.00
(13.00–19.00) | 17.00
(15.00–21.00) | 24.00
(18.00–30.00) | <0.001 |
| Glucose
(mg/dl) | 160.00
(138.00–180.00) | 162.00
(139.00–191.00) | 185.00
(153.00–236.00) | <0.001 |
| Lactate
(mmol/l) | 2.50
(2.00–3.90) | 3.15
(2.03–4.85) | 3.60
(1.95–6.65) | 0.034 |
| PTT
(sec) | 35.42
(31.22–41.99) | 34.55
(30.40–41.95) | 36.80
(30.57–44.38) | 0.702 |
|
INR | 1.30
(1.20–1.45) | 1.30
(1.15–1.40) | 1.30
(1.20–1.60) | 0.371 |
| PT
(sec) | 14.50
(13.62–15.53) | 14.35
(13.20–15.22) | 14.55
(13.26–16.04) | 0.596 |
| Table IV.Threshold effect analysis of anion
gap on ICU mortality using piecewise linear regression. |
Table IV.
Threshold effect analysis of anion
gap on ICU mortality using piecewise linear regression.
| Inflection point of
anion gap on ICU mortality (mEq/l) | β (95% CI) | ∆β (95% CI) | P-value | P for ∆β |
|---|
| <17 | 1.51 (1.12,
2.04) |
| 0.0074 |
|
| >17 | 1.14 (0.97,
1.34) |
| 0.1148 |
|
|
|
| 0.76
(0.51–1.12) |
| 0.1580 |
| Table V.Univariate analysis of intensive care
unit mortality. |
Table V.
Univariate analysis of intensive care
unit mortality.
| Variable | OR (95% CI) | P-value |
|---|
| Age | 1.07 (1.01,
1.12) | 0.0116 |
| Sex |
|
|
|
Male | 1.0 |
|
|
Female | 1.59 (0.69,
3.70) | 0.2772 |
| Type of aortic
aneurysm |
|
|
|
Thoracic aneurysm without
mention of rupture | 1.0 |
|
|
Abdominal aneurysm
(ruptured) | 6.18 (2.01,
18.98) | 0.0015 |
|
Abdominal aneurysm without
mention of rupture | 1.54 (0.49,
4.86) | 0.4610 |
| Anion Gap
(mEq/l) | 1.36 (1.22,
1.52) | <0.0001 |
| Severity score |
|
|
|
SOFA | 1.46 (1.26,
1.69) | <0.0001 |
|
APSIII | 1.05 (1.03,
1.07) | <0.0001 |
| Vital signs |
|
|
|
Heartrate (bpm) | 1.07 (1.03,
1.10) | 0.0004 |
|
Systolic pressure (mmHg) | 0.98 (0.95,
1.02) | 0.3266 |
|
Diastolic pressure (mmHg) | 1.04 (0.99,
1.10) | 0.1182 |
|
Respiratory rate (bpm) | 1.15 (1.02,
1.29) | 0.0183 |
|
Temperature (°C) | 0.59 (0.32,
1.09) | 0.0909 |
| SpO2
(%) | 0.97 (0.93,
1.01) | 0.0993 |
| Urine output in
first day (ml) | 1.00 (1.00,
1.00) | 0.0014 |
| RTT in first
day |
|
|
| No | 1.0 |
|
|
Yes | 17.64 (2.79,
111.52) | 0.0023 |
| Ventilation in
first day |
|
|
| No | 1.0 |
|
|
Yes | 2.36 (0.54,
10.41) | 0.2564 |
| Sepsis (based on
ICD-9 codes) |
|
|
| No | 1.0 |
|
|
Yes | 12.25 (2.85,
52.69) | 0.0008 |
| Sepsis (based on
Angus criteria) |
|
|
| No | 1.0 |
|
|
Yes | 4.92 (2.05,
11.8) | 0.0004 |
| Lab
examination |
|
|
| White
blood cell (K/ul) | 1.05 (0.98,
1.13) | 0.1357 |
| Table VI.Multivariate logistic regression for
effects of anion gap on intensive care unit mortality. |
Table VI.
Multivariate logistic regression for
effects of anion gap on intensive care unit mortality.
| Variable | Odds ratio | 95% confidence
interval | P-value |
|---|
| Non-adjusted | 1.36 | 1.22–1.52 | <0.0001 |
| Model I | 1.26 | 1.11–1.42 | 0.0003 |
| Model II | 1.38 | 1.08–1.76 | 0.0088 |
Subgroup analysis
The results of the stratified and interaction
analyses of the association between admission serum anion gap and
ICU mortality are presented in Fig.
4 and Table VII. The
association appeared to be similar when compared with the results
of the multivariable analysis shown in Table VI. A significant interaction
(P<0.05) was found among subgroups of tertile of hemoglobin.
| Table VII.Subgroup analysis of associations
between anion gap and intensive care unit mortality. |
Table VII.
Subgroup analysis of associations
between anion gap and intensive care unit mortality.
| Variable | n | OR | 95% CI Low | 95% CI High | P-value | P-value
(interaction) |
|---|
| Type of aortic
aneurysm |
|
|
|
|
| 0.1361 |
|
Thoracic aneurysm without
mention of rupture | 109 | 1.22 | 0.98 | 1.53 | 0.0781 |
|
|
Abdominal aneurysm
(ruptured) | 48 | 1.25 | 1.00 | 1.57 | 0.0464 |
|
|
Abdominal aneurysm without
mention of rupture | 116 | 2.02 | 1.19 | 3.42 | 0.0087 |
|
| Sepsis (based on
Angus criteria) |
|
|
|
|
| 0.8300 |
| No | 195 | 1.29 | 1.07 | 1.55 | 0.0069 |
|
|
Yes | 78 | 1.25 | 1.03 | 1.52 | 0.0216 |
|
| Coagulopathy |
|
|
|
|
| 0.2672 |
| No | 226 | 1.39 | 1.15 | 1.67 | 0.0006 |
|
|
Yes | 47 | 1.19 | 0.98 | 1.44 | 0.0814 |
|
| Hemoglobin |
|
|
|
|
| 0.0134 |
|
Low | 91 | 1.13 | 0.99 | 1.28 | 0.0727 |
|
|
Middle | 86 | 1.94 | 1.20 | 3.13 | 0.0065 |
|
|
High | 95 | 1.53 | 1.00 | 2.35 | 0.0522 |
|
| Fluid and
electrolyte disorders |
|
|
|
|
| 0.9546 |
| No | 197 | 1.27 | 1.09 | 1.49 | 0.0022 |
|
|
Yes | 76 | 1.26 | 1.04 | 1.54 | 0.0197 |
|
Sensitive analysis
The imputation of missing variables did not affect
the results (Table VIII), which
were virtually unchanged (<10%) after excluding ruptured AA
patients (Table IX and X).
| Table IX.Univariate analysis of ICU mortality
after excluding patients with ruptured aortic aneurysm. |
Table IX.
Univariate analysis of ICU mortality
after excluding patients with ruptured aortic aneurysm.
| Variable | OR (95% CI) | P-value |
|---|
| Age | 1.07 (1.00,
1.14) | 0.0523 |
| Sex |
|
|
|
Male | 1.0 |
|
|
Female | 3.36 (1.00,
11.27) | 0.0494 |
| Type of aortic
aneurysm |
|
|
|
Thoracic aneurysm without
mention of rupture | 1.0 |
|
|
Abdominal aneurysm without
mention of rupture | 1.54 (0.49,
4.86) | 0.4610 |
| Anion gap
(mEq/l) | 1.44 (1.19,
1.75) | 0.0002 |
| Severity score |
|
|
|
SOFA | 1.38 (1.16,
1.65) | 0.0002 |
|
APSIII | 1.05 (1.02,
1.08) | 0.0003 |
| Vital signs |
|
|
|
Heartrate (bpm) | 1.06 (1.01,
1.10) | 0.0161 |
|
Systolic pressure (mmHg) | 0.98 (0.94,
1.03) | 0.4983 |
|
Diastolic pressure (mmHg) | 1.02 (0.95,
1.09) | 0.5753 |
|
Respiratory rate (bpm) | 1.12 (0.96,
1.31) | 0.1427 |
|
Temperature (°C) | 0.52 (0.23,
1.18) | 0.1193 |
| SpO2
(%) | 0.97 (0.93,
1.01) | 0.1316 |
| Urine output in
first day (ml) | 1.00 (1.00,
1.00) | 0.1029 |
| RTT in first
day |
|
|
| No | 1.0 |
|
|
Yes | 8.75 (0.74,
103.44) | 0.0852 |
| Ventilation in
first day |
|
|
| No | 1.0 |
|
|
Yes | 2.79 (0.35,
22.09) | 0.3309 |
| Sepsis (based on
ICD-9 codes) |
|
|
| No | 1.0 |
|
|
Yes | 23.11 (4.96,
107.61) | 0.0001 |
| Sepsis (based on
angus criteria) |
|
|
| No | 1.0 |
|
|
Yes | 5.62 (1.75,
17.98) | 0.0036 |
| Lab
examination |
|
|
| WBC
(K/ul) | 1.04 (0.94,
1.14) | 0.4594 |
|
Platelet (K/ul) | 0.99 (0.98,
1.00) | 0.0758 |
|
Hemoglobin (g/dl) | 0.70 (0.50,
0.98) | 0.0398 |
|
Creatinine (mg/dl) | 1.66 (1.05,
2.64) | 0.0310 |
| BUN
(mg/dl) | 1.06 (1.01,
1.10) | 0.0106 |
| Glucose
(mg/dl) | 1.01 (1.00,
1.01) | 0.0585 |
| Lactate
(mmol/l) | 1.53 (1.21,
1.93) | 0.0004 |
| PTT
(sec) | 1.02 (0.99,
1.05) | 0.1386 |
|
INR | 1.43 (0.26,
7.73) | 0.6795 |
| PT
(sec) | 0.95 (0.72,
1.27) | 0.7441 |
| Comorbidities |
|
|
|
Congestive heart failure |
|
No | 1.0 |
|
|
Yes | 2.44 (0.28,
21.47) | 0.4213 |
| Cardiac
arrhythmias |
|
|
|
No | 1.0 |
|
|
Yes | 2.12 (0.25,
18.41) | 0.4938 |
|
Valvular disease |
|
|
|
No | 1.0 |
|
|
Yes | 8.75 (0.74,
103.44) | 0.0852 |
|
Pulmonary circulation
disorder |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9935 |
|
Peripheral vascular
disorder |
|
|
|
No | 1.0 |
|
|
Yes | 1.92 (0.60,
6.14) | 0.2693 |
|
Hypertension |
|
|
|
No | 1.0 |
|
|
Yes | 3.67 (0.92,
14.71) | 0.0659 |
|
Paralysis |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9908 |
| Other
neurological disease |
|
|
|
No | 1.0 |
|
|
Yes | 17.58 (1.04,
298.62) | 0.0473 |
| Chronic
pulmonary disease |
|
|
|
No | 1.0 |
|
|
Yes | 1.51 (0.48,
4.80) | 0.4832 |
|
Uncomplicated diabetes |
|
|
|
No | 1.0 |
|
|
Yes | 0.45 (0.06,
3.59) | 0.4529 |
|
Complicated diabetes |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9908 |
|
Hypothyroidism |
|
|
|
No | 1.0 |
|
|
Yes | 1.85 (0.38,
8.95) | 0.4462 |
| Renal
failure |
|
|
|
No | 1.0 |
|
|
Yes | 2.59 (0.66,
10.13) | 0.1712 |
| Liver
disease |
|
|
|
No | 1.0 |
|
|
Yes | 3.45 (0.37,
31.91) | 0.2752 |
|
Lymphoma |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9921 |
|
Metastatic cancer |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9930 |
| Solid
tumor |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9908 |
|
Rheumatoid arthritis |
|
|
|
No | 1.0 |
|
|
Yes | 2.44 (0.28,
21.47) | 0.4213 |
|
Coagulopathy |
|
|
|
No | 1.0 |
|
|
Yes | 2.80 (0.81,
9.7) | 0.1034 |
|
Obesity |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9913 |
| Weight
loss |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9921 |
| Fluid
and electrolyte disorders |
|
|
|
No | 1.0 |
|
|
Yes | 0.97 (0.26,
3.67) | 0.9666 |
| Blood
loss anemia |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9921 |
|
Deficiency anemias |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9895 |
| Alcohol
abuse |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9916 |
|
Psychoses |
|
|
|
No | 1.0 |
|
|
Yes | 8.75 (0.74,
103.44) | 0.0852 |
|
Depression |
|
|
|
No | 1.0 |
|
|
Yes | 0.00 (0.00,
Inf) | 0.9901 |
| Table X.Multivariate logistic regression for
effects of anion gap on ICU mortality after excluding patients with
ruptured aortic aneurysm. |
Table X.
Multivariate logistic regression for
effects of anion gap on ICU mortality after excluding patients with
ruptured aortic aneurysm.
| Variable | OR | 95% CI | P-value |
|---|
| Non-adjusted | 1.44 | 1.19–1.75 | 0.0002 |
| Model I | 1.33 | 1.08–1.62 | 0.0064 |
| Model II | 1.46 | 1.09–1.97 | 0.0112 |
Discussion
The present study examined for the first time the
predictive value of serum anion gap on ICU mortality in AA
patients, and the results suggested that the risk of ICU mortality
may increase by 38% per 1 mEq/l increase in admission serum anion
gap.
Many studies have explored the relationship between
anion gap and clinical outcomes of critically ill patients. In
fact, as early as 1987, Shackleton et al (14) noted that an elevation of the
unmeasured anion gap was significantly and independently associated
with mortality for ruptured AAA patients. Grist and Thomas
(28) reported that anion gap is a
risk factor in long-term extracorporeal support. Kim et al
(19) found a similar association in
a pediatric ICU. However, Rocktaeschel et al (29) concluded that unmeasured anions,
irrespective of the calculated methods, were not practical
predictors of hospital mortality in critically ill patients. In
addition, the use of anion gap for risk stratification in
critically ill patients is not supported for the significant
statistical heterogeneity according to a recent systematic review
and meta-analysis conducted by Glasmacher and Stones
(20). Considering the urgent need
for a practical and useful predictive model of AA (30), which is notorious for high mortality,
it is essential to keep exploring predictors of clinical outcomes
for AA patients. As anion gap is routinely determined in all
patients admitted to ICU and there is no extra cost for this
potential beneficial test, a study that specifically focused on AA
patients was necessary, given the extremely low incidence of AA.
The results of our study validated the association between serum
anion gap and ICU mortality, which was in accordance with most
previous studies (20), suggesting
that serum anion gap may serve as a mortality predictor for AA
patients in ICU. The AUC of anion gap was similar to the SOFA and
APACHE III values in our study. As anion gap is a traditional tool
used to assess acid-base status, most previous studies usually
attribute the association to acid-base disorders, which contribute
significantly to morbidity and mortality in critically ill patients
(31). Taylor et al (32) reported that anion gap is
independently associated with higher blood pressure, which is
associated with negative outcomes for AA patients (33), thus the underlying mechanism requires
further research.
Several limitations of our study should be noted.
First, although hypoalbuminemia could affect its interpretation,
anion gap was not corrected for serum albumin level in our study as
most subjects analyzed lacked albumin records. Second, although
attempts were taken to control bias and confounders, many other
known or unknown factors may still exist and have contributed to
bias. For example, although we took into consideration fluid and
electrolyte disorders (identified by ICD-9 codes) as a potential
confounder, the quantities and types of intravenous infusion fluids
before ICU admission may have affected the value of serum anion gap
on ICU admission. Other potential confounders including smoking
status, diameters of the aorta, and surgical procedures were not
considered in the study. In addition, given the observational
nature of our study, it is not possible to conclude that the
relationship between admission serum anion gap and ICU mortality
reflects cause and effect.
In summary, the present retrospective observational
study provided confirmation of the association between serum anion
gap on admission and ICU mortality of AA patients. However, further
prospective clinical studies are still required, particularly to
explore the potential value of anion gap in improving various
predictive models for ICU outcomes.
Acknowledgements
Not applicable.
Funding
This work was supported by the Natural Science
Foundation of Guangdong Province China (grant number
2015A030310346); the Special Funds for the Cultivation of Guangdong
College Students' Scientific and Technological Innovation
(‘Climbing Program’ Special Funds).
Availability of data and materials
The datasets generated and analyzed during the
current study are available in the PhysioBank repository,
https://mimic.physionet.org/.
Authors' contributions
KH, QCC, and QGC designed the study. QCC, QGC, LL,
XL, and SIC performed data extraction and the data were analyzed by
QCC, QGC, YL, ZT, and WL. The manuscript draft was prepared by LL
and revised by KH, QCC and QGC. All authors approved the final
manuscript.
Ethics approval and consent to
participate
The access of the database was approved by the
institutional review boards of both Beth Israel Deaconess Medical
Center and Massachusetts Institute of Technology Affiliates. No
informed consent was required because the data are anonymized.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
ICU
|
intensive care unit
|
|
AA
|
aortic aneurysm
|
|
IQR
|
interquartile range
|
|
OR
|
odds ratio
|
|
CI
|
confidence interval
|
|
TAA
|
thoracic aortic aneurysm
|
|
AAA
|
abdominal aortic aneurysm
|
|
MIMIC-III
|
Medical Information Mart for Intensive
Care III
|
|
ROC
|
receiver operating characteristic
|
|
AUC
|
area under the ROC curve
|
|
SOFA
|
Sepsis-related Organ Failure
Assessment
|
|
APACHE III
|
Acute Physiology and Chronic Health
Evaluation III
|
|
ICD-9
|
International Classification of
Diseases, 9th Revision
|
References
|
1
|
Johnston KW, Rutherford RB, Tilson MD,
Shah DM, Hollier L and Stanley JC: Suggested standards for
reporting on arterial aneurysms. Subcommittee on reporting
standards for arterial aneurysms, Ad Hoc Committee on Reporting
Standards, Society for Vascular Surgery and North American Chapter,
International Society for Cardiovascular Surgery. J Vasc Surg.
13:452–458. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Isselbacher EM: Thoracic and abdominal
aortic aneurysms. Circulation. 111:816–828. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Elefteriades JA, Sang A, Kuzmik G and
Hornick M: Guilt by association: Paradigm for detecting a silent
killer (thoracic aortic aneurysm). Open Heart. 2:e0001692015.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Howard DP, Banerjee A, Fairhead JF, Handa
A, Silver LE and Rothwell PM: Oxford Vascular Study: Age-specific
incidence, risk factors and outcome of acute abdominal aortic
aneurysms in a defined population. Br J Surg. 102:907–915. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Stuntz M: Modeling the burden of abdominal
aortic aneurysm in the USA in 2013. Cardiology. 135:127–131. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nair N, Shaw C, Sarfati D and Stanley J:
Abdominal aortic aneurysm disease in New Zealand: Epidemiology and
burden between 2002 and 2006. N Z Med J. 125:10–20. 2012.PubMed/NCBI
|
|
7
|
Robertson EN and Jeremy RW: Abstract
10144: Uncovering the burden of familial thoracic aortic aneurysm
disease. Circulation. 128:A101442013.
|
|
8
|
Johansson G, Markström U and Swedenborg J:
Ruptured thoracic aortic aneurysms: A study of incidence and
mortality rates. J Vasc Surg. 21:985–988. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Soden PA and Schermerhorn ML: The
epidemiology of ruptured abdominal aortic aneurysm (rAAA)Ruptured
abdominal aortic aneurysm: The definitive manual. Starnes BW, Mehta
M and Veith FJ: Cham: Springer International Publishing; pp. 15–48.
2017, View Article : Google Scholar
|
|
10
|
Polzer S and Gasser TC: Biomechanical
rupture risk assessment of abdominal aortic aneurysms based on a
novel probabilistic rupture risk index. J R Soc Interface.
12:201508522015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tambyraja A, Murie J and Chalmers R:
Predictors of outcome after abdominal aortic aneurysm rupture:
Edinburgh ruptured aneurysm score. World J Surg. 31:2243–2247.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Marković M, Davidović L, Maksimović Z,
Kostić D, Cinara I, Cvetković S, Sindjelic R, Seferović PM and
Ristić AD: Ruptured abdominal aortic aneurysm. Predictors of
survival in 229 consecutive surgical patients. Herz. 29:123–129.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gutiérrez-Morlote J, Llorca J, de Elejalde
Ibáñez E, Lobato A and José San JM: Predictors of mortality in
patients undergoing surgery for ruptured aortic aneurysm. Vasa.
31:265–268. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shackleton CR, Schechter MT, Bianco R and
Hildebrand HD: Preoperative predictors of mortality risk in
ruptured abdominal aortic aneurysm. J Vasc Surg. 6:583–589. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lee SW, Kim S, Na KY, Cha RH, Kang SW,
Park CW, Cha DR, Kim SG, Yoon SA, Han SY, et al: Serum anion gap
predicts all-cause mortality in patients with advanced chronic
kidney disease: A retrospective analysis of a randomized controlled
study. PLoS One. 11:e01563812016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Leskovan JJ, Justiniano CF, Bach JA, Cook
CH, Lindsey DE, Eiferman DS, Papadimos TJ, Steinberg SM, Bergese
SD, Stawicki SP and Evans DC: Anion gap as a predictor of trauma
outcomes in the older trauma population: Correlations with injury
severity and mortality. Am Surg. 79:1203–1206. 2013.PubMed/NCBI
|
|
17
|
Honore PM, Joannes-Boyau O and Boer W:
Strong ion gap and outcome after cardiac arrest: Another nail in
the coffin of traditional acid-base quantification. Intensive Care
Med. 35:189–191. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sahu A, Cooper HA and Panza JA: The
initial anion gap is a predictor of mortality in acute myocardial
infarction. Coron Artery Dis. 17:409–412. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kim MJ, Kim YH, Sol IS, Kim SY, Kim JD,
Kim HY, Kim KW, Sohn MH and Kim KE: Serum anion gap at admission as
a predictor of mortality in the pediatric intensive care unit. Sci
Rep. 7:14562017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Glasmacher SA and Stones W: Anion gap as a
prognostic tool for risk stratification in critically ill
patients-a systematic review and meta-analysis. BMC Anesthesiol.
16:682016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Johnson AE, Pollard TJ, Shen L, Lehman LW,
Feng M, Ghassemi M, Moody B, Szolovits P, Celi LA and Mark RG:
MIMIC-III, a freely accessible critical care database. Sci Data.
3:1600352016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Johnson AE, Stone DJ, Celi LA and Pollard
TJ: The MIMIC Code Repository: Enabling reproducibility in critical
care research. J Am Med Inform Assoc. 25:32–39. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Vincent JL, Moreno R, Takala J, Willatts
S, De Mendonça A, Bruining H, Reinhart CK, Suter PM and Thijs LG:
The SOFA (Sepsis-related Organ Failure Assessment) score to
describe organ dysfunction/failure. On behalf of the Working Group
on Sepsis-Related Problems of the European Society of Intensive
Care Medicine. Intensive Care Med. 22:707–710. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Knaus WA, Wagner DP, Draper EA, Zimmerman
JE, Bergner M, Bastos PG, Sirio CA, Murphy DJ, Lotring T, Damiano
A, et al: The APACHE III prognostic system. Risk prediction of
hospital mortality for critically ill hospitalized adults. Chest.
100:1619–1636. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Angus DC, Linde-Zwirble WT, Lidicker J,
Clermont G, Carcillo J and Pinsky MR: Epidemiology of severe sepsis
in the United States: Analysis of incidence, outcome, and
associated costs of care. Crit Care Med. 29:1303–1310. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Steiner C, Elixhauser A and Schnaier J:
The healthcare cost and utilization project: An overview. Eff Clin
Pract. 5:143–151. 2002.PubMed/NCBI
|
|
27
|
Donders AR, van der Heijden GJ, Stijnen T
and Moons KG: Review: A gentle introduction to imputation of
missing values. J Clin Epidemiol. 59:1087–1091. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Grist G and Thomas D: Blood anion gaps and
venoarterial carbon dioxide gradients as risk factors in long-term
extracorporeal support. J Extra Corpor Technol. 29:6–10.
1997.PubMed/NCBI
|
|
29
|
Rocktaeschel J, Morimatsu H, Uchino S and
Bellomo R: Unmeasured anions in critically ill patients: Can they
predict mortality? Crit Care Med. 31:2131–2136. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Thompson PC, Dalman RL, Harris EJ, Chandra
V, Lee JT and Mell MW: Predictive models for mortality after
ruptured aortic aneurysm repair do not predict futility and are not
useful for clinical decision making. J Vasc Surg. 64:1617–1622.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Al-Jaghbeer M and Kellum JA: Acid-base
disturbances in intensive care patients: Etiology, pathophysiology
and treatment. Nephrol Dial Transplant. 30:1104–1111. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Taylor EN, Forman JP and Farwell WR: Serum
anion gap and blood pressure in the national health and nutrition
examination survey. Hypertension. 50:320–324. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kent KC, Zwolak RM, Egorova NN, Riles TS,
Manganaro A, Moskowitz AJ, Gelijns AC and Greco G: Analysis of risk
factors for abdominal aortic aneurysm in a cohort of more than 3
million individuals. J Vasc Surg. 52:539–548. 2010. View Article : Google Scholar : PubMed/NCBI
|