Introduction
Pregnancy dermatoses represent a diverse group of
mucocutaneous conditions characterized by pruritus and inflammation
occurring only during pregnancy or immediately postpartum (1). The most frequent pathologies include
atopic eruption of pregnancy, polymorphic eruption of pregnancy
(PEP), intrahepatic cholestasis of pregnancy (ICP), pustular
psoriasis of pregnancy (PPP) and pemphigoid gestationis (PG). The
moment of onset should be noted as there are conditions that occur
earlier in pregnancy, such as atopic eruption of pregnancy, and
conditions which complicate the second or third trimester of
pregnancy or even the postpartum period (PG, PEP and ICP) (2).
PG, in the past known as herpes gestationis,
represents an autoimmune bullous disease occurring exclusively
after the second part of the pregnancy (3). PG is a rare disease, its incidence
being 1 out of 20,000 to 50,000 pregnancies. Besides pregnancy, PG
has been reported to appear in several cases of women with
trophoblastic tumors as a paraneoplastic phenomenon (4-6).
The pathogenesis is based on the appearance of
circulating IgG1 antibodies against the bullous pemphigoid antigen,
known as BP180 or collagen XVII. This antigen is in fact a
transmembrane hemidesmosomal glycoprotein, which contributes to the
formation of the cutaneous basement membrane zone (7). In PG, the binding of IgG1 to BP180
creates an inflammatory cascade responsible for the detachment of
the epidermis from the profound layer, the dermis (8). It appears that the placenta is the
initial site of autoimmunity, as these IgG1 antibodies bind also to
the amniotic and chorionic epithelia, in addition to the epidermal
basement membrane zone, which all have ectodermal origin. One
theory sustains the existence of paternal antigens from the second
class of major histocompatibility complex on the chorionic villi,
which generate an immune response from the mother, resulting in
antibodies against the amniotic basement membrane. This theory
suggests that these antibodies could cross-react with the variable
antigens from the maternal skin and induce maternal and even fetal
disease (9). Another hypothesis
sustains a genetic predisposition, as there have been studies that
have shown a possible interconnection between PG and second-class
human leukocyte antigen (HLA), especially the phenotype
HLA-DR3/HLA-DR4(10).
Clinical manifestations of PG include extreme
pruritus, papules and plaques which form tense blisters that
typically appear periumbilical and spread to the trunk and
extremities. The lesions usually spare the face and the mucous
membranes. Although the symptoms may remit spontaneously before
delivery, 75% of cases burst after delivery and 25% of cases burst
monthly during menses or while using contraceptive pills. Usually,
the majority of cases resolve automatically within the first weeks
to several months postpartum. PG may reoccur in a more violent form
with subsequent pregnancies, but it can also be absent (11).
Regarding neonatal outcome, PG is associated with a
higher risk of premature delivery and, due to a moderate placental
failure, women with PG deliver small-for-gestational-age fetuses.
There have been no reports of an elevated risk of miscarriage
(12). One study concluded that the
obstetrical prognosis is influenced by the debut of PG and the
existence of blisters on the patient's skin; an early debut in the
first or second trimester announces an altered prognosis (13). Although there is not enough evidence
to sustain a link between PG and an obscure prognosis, in another
study Al-Saif et al reported the outcome of 32 patients with
PG, from which 6 were preterm deliveries, 2 pregnancies presented
intrauterine growth restriction and another 2 pregnancies finished
with abortion or stillbirth (14).
IgG autoantibodies could pass the placenta and induce neonatal PG
which presents with minor symptoms and resolves spontaneously
within weeks. Due to the maternal systemic treatment of the
disease, adrenal suppression might occur in babies, but there is a
minimum risk even if there were high-dose corticosteroids
administered to the mother (15).
The diagnosis is based on the clinical symptoms and
signs, skin biopsy with direct immunofluorescence (DIF) and serum
level of BP180 antibodies using enzyme-linked immunosorbent assay
(ELISA).
As there are few cases of PG, there is yet no
standard treatment; the management is mostly based on the
clinician's experience combined with the existing literature of
bullous pemphigoid and with the collaboration of a dermatologist
and a pathologist (16,17). The first recommendation is to use
high-potency topical corticosteroids. The second treatment line is
represented by systemic corticosteroids, such as prednisone 0.5
mg/kg daily, which appears to be effective. Postpartum, prednisone
can be administered up to 2 mg/kg daily in severe cases. Other
successful postpartum administered therapies include azathioprine,
cyclosporine, doxycycline, high-dose intravenous immunoglobulins,
cyclophosphamide, rituximab, nicotinamide and immunoapheresis. Oral
antihistamines such as chlorpheniramine or loratadine could aid
with the control of the pruritus (18,19).
In this article, we present the case of a pregnancy
complicated with PG with the aim to highlight the difficulties in
the differential diagnosis of pregnancy dermatoses, the management
of this particular pathology and the importance of monitoring such
a pregnancy with high obstetrical risk.
Case report
A 40-year-old woman presented to our obstetrics
clinic, Life Memorial Hospital (Bucharest, Romania) one year before
for early diagnosis and monitoring of a singleton pregnancy. From
the gynecologic history, we noted a surgery for a benign condition
2 years prior complicated with an unspecified dermatitis
immediately after. Her medical history included the presence of
autoimmune thyroiditis. A noninvasive prenatal test was performed
and the major chromosomal abnormalities were excluded. The course
of the pregnancy was uneventful, and the ultrasound and
paraclinical monitoring were normal. We noted nothing abnormal on
the blood tests and the fetal growth was according to the
gestational age, until the 30th week of pregnancy, when the patient
presented with pruritus and papules on the abdomen. The patient was
counseled to undergo a dermatologic consultation. The first
clinical diagnosis was contact dermatitis and the patient received
topical corticosteroids, which had a favorable effect on the
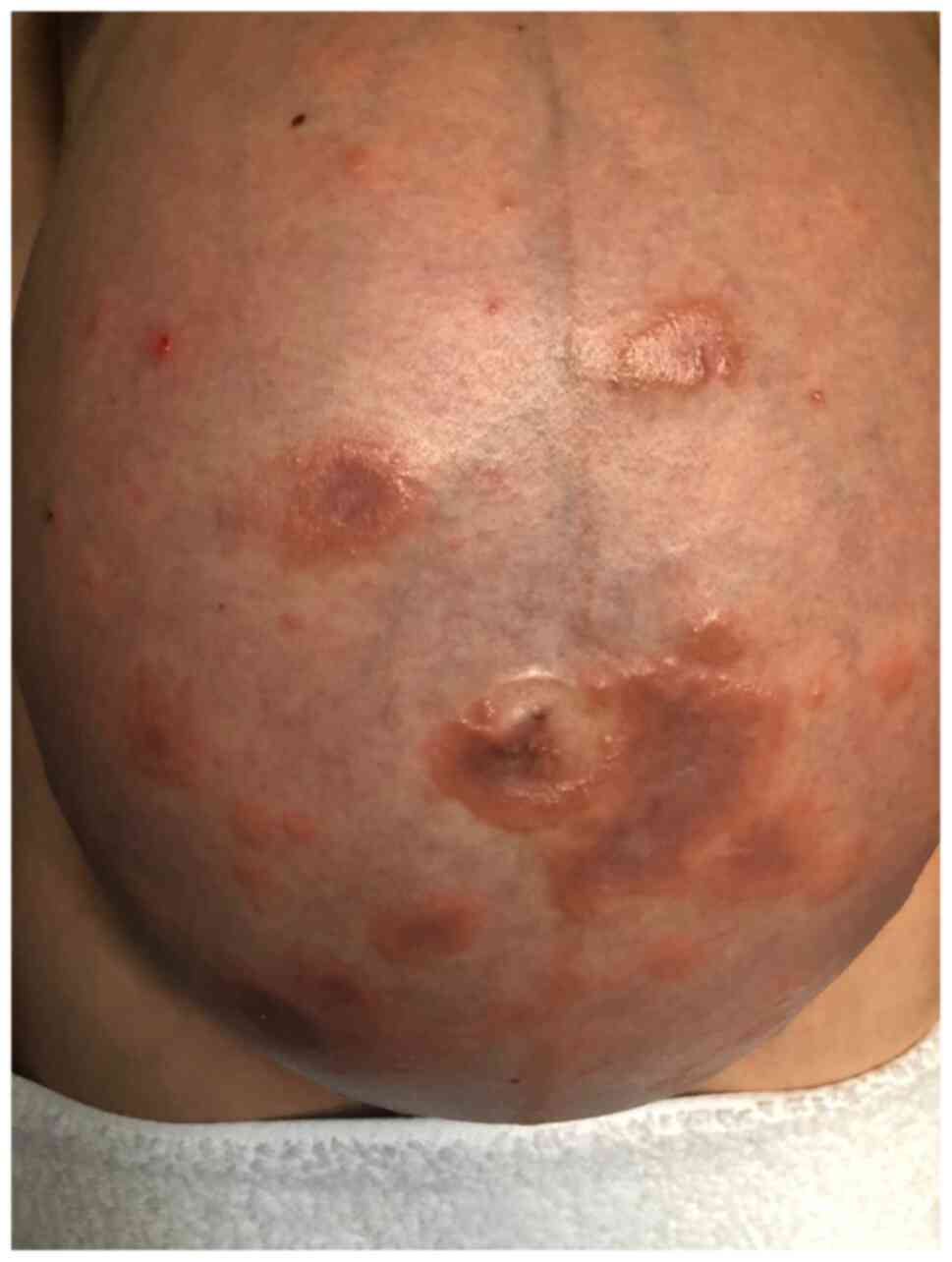
remission of the pruritus and cutaneous lesions. After two weeks,
the patient returned with generalized and intense pruritus and
papules, which raised the suspicion of PG (Fig. 1). Topic corticosteroids administered
this time were ineffective and at 35-weeks gestation she receives
systemic corticosteroids consisting of 4 doses of 8 mg
dexamethasone, as the severity of the symptoms was increasing and
the pruritus became unbearable. The skin biopsy performed revealed
superficial perivascular dermatitis with lymphocytes and
eosinophils, with superficial perivascular lymphocytic and
eosinophilic infiltrate and interstitial eosinophilic infiltrate,
with some eosinophils in groups located subepidermal (Fig. 2). The direct immunofluorescence
showed linear and continuous deposit of IgG and C3 in the
dermoepidermal junction, with no IgA, IgM or C1q deposits (Fig. 3). The existence of a linear deposit
of C3 in the dermoepidermal junction, more specifically at the
basement membrane zone, is pathognomonic for PG. Anti BP180
antibodies were not performed, but the skin biopsy, along with the
direct immunofluorescence and symptoms confirmed the diagnosis.
At 35 weeks of gestation, due to acute fetal
distress, a male fetus of 2,900 g with an APGAR score at 1 min of 9
was delivered by Cesarean section. The fetus had a good adaptation
and a normal neonatal period, without any pemphigoid lesions.
The patient had an exacerbation of the disease
immediately postpartum (Fig. 4) and
received topic and systemic corticosteroids, and the evolution of
PG was favorable under treatment. The systemic corticosteroids were
reduced to a minimum dose with a maximum effect on the remission of
the disease. The patient was counseled to use sulphur soap,
antihistaminic drugs, fusidic acid and sulfadiazinum for the skin
lesions, but all of these increased the rush due to skin dryness; a
general recommendation was to avoid ordinary laundry detergent and
to replace it with another one for sensitive skin, with no perfume.
Immediately postpartum, the patient received 64 mg of
methylprednisolone daily and the dose was reduced gradually to a
maintenance dose of 32 mg every two days at 3 months postpartum,
that proved to be a minimum dose under which the pathology remained
under control. The complete remission has not been achieved even 18
months after delivery.
Discussion
The particularity of this case of pemphigoid
gestationis (PG) consists in the difficulties encountered in the
differential diagnosis of pregnancy dermatoses that are able to
modify the normal course of the pregnancy and in the atypical
complication that imposed iatrogenic prematurity with short- and
long-term possible modified fetal prognosis (20). Another particularity of our case
were the areas affected by papules and blisters, that atypically
included the face, neck, ears and scalp. Any pregnant woman
presenting pruritus and skin lesions should be referred to a
dermatologist and undergo the necessary investigations, along with
the clinical examination of the skin and a detailed medical
history. It is of high importance to establish the correct
diagnosis so that the patient can receive the optimum healthcare;
the evaluation of maternal and fetal prognosis is dependent on the
type of dermatoses of pregnancy, as polymorphic eruption of
pregnancy (5) and atopic eruption
of pregnancy (4,5) do not endanger the pregnancy outcome,
while pustular psoriasis of pregnancy (21,22),
intrahepatic cholestasis of pregnancy (23) and PG (12) could convert the normal uneventful
course of pregnancy into a high-risk pregnancy. In order to make
the differential diagnosis between intrahepatic cholestasis of
pregnancy and PG, the laboratory evaluation should include bile
acids, prothrombin time, liver function tests and especially serum
anti-BP180 antibodies (23,24). Anti-BP180 antibodies have a
specificity and sensitivity between 96 and 100% for the diagnosis
of PG (25). This differential
diagnosis is extremely important as the first line treatment for
ICP includes ursodeoxycholic acid (26) and for PG consists in topical
corticosteroids (16). Furthermore,
a skin biopsy, completed with a direct immunofluorescence test,
should be performed to differentiate PGs from pustular psoriasis of
pregnancy. These two dermatoses present different monitoring of the
maternal status. For example, in PG, anti-BP180 antibodies can be
used to monitor the course of the pathology and the efficiency of
the treatment (27) and in pustular
psoriasis of pregnancy, a complete metabolic panel should be
performed to evaluate electrolyte abnormalities, renal and liver
function, possible hypoalbuminemia and the risk for hypocalcemia
(22).
In our case, the diagnosis was made considering the
clinical features and the result of the skin biopsy. Taking into
account the positive diagnosis of PG, the monitoring of the
pregnancy was modified as the clinical, blood tests and ultrasound
examinations were more frequent. Although, the disease appeared in
the third trimester, the fetal growth was not affected despite the
intensified activity of the disease and topical and systemic
corticosteroid administration. Fetal well-being status was
carefully monitored by cerebro-placental ratio and nonstress tests,
allowing us to detect the fetal bradycardia in good time.
Fetal myocardium and conduction tissue injury
present in systemic lupus erythematosus are due to circulating
antibodies to Ro (SSA) and La (SSB), which pass the placenta and
affect the normal function of the fetal heart, varying from
transient first-degree heart block to complete atrio-ventricular
block and hydrops (28). From our
knowledge, there are no studies confirming a specific effect of
anti-BP180 antibodies on the fetal sinus node or whether these
antibodies have a particular affinity for this tissue by a similar
mechanism, which implies immune-mediated inflammatory response.
In conclusion, differential diagnosis is the first
key to monitoring PG and to ensure the best maternal and fetal
outcome. Additionally, there is a real need for further studies
concerning the treatment standardization because being a rare
cutaneous disease associated exclusively with pregnancy, there is
not enough data in the literature to sustain a certain therapeutic
attitude and management of this autoimmune pathology.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Any additional information concerning the study can
be requested from the corresponding author on reasonable
request.
Authors' contributions
CGP and REB conceived the concept of the article
after successful management of the presented case to which IM and
ADC contributed. BMM, CG and CAZ performed the literature search
and wrote the draft of manuscript. CGP and DPO conducted the
follow-up of the patient. IM and ADC contributed to the
pathological examination of the skin biopsy. CGP, REB, BMM and CG
collected, assembled and interpreted the data, making the revision
of the manuscript, critically for important intellectual content.
All authors have read and approved the final manuscript for
publication.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the World Medical Association Declaration of Helsinki and was
approved by the Institutional Ethics Board of the ‘Life Memorial
Hospital’ (Bucharest, Romania) (approval no. is 24/03.08.2021).
Patient consent for publication
The patient provided informed consent for
publication of the case report.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ambros-Rudolph CM: Dermatoses of
pregnancy-clues to diagnosis, fetal risk and therapy. Ann Dermatol.
23:265–275. 2011.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ambros-Rudolph CM, Müllegger RR,
Vaughan-Jones SA, Kerl H and Black MM: The specific dermatoses of
pregnancy revisited and reclassified: Results of a retrospective
two-center study on 505 pregnant patients. J Am Acad Dermatol.
54:395–404. 2006.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Lipozenčić J, Ljubojevic S and
Bukvić-Mokos Z: Pemphigoid gestationis. Clin Dermatol. 30:51–55.
2012.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Roger D, Vaillant L, Fignon A, Pierre F,
Bacq Y, Brechot JF, Grangeponte MC and Lorette G: Specific pruritic
diseases of pregnancy. A prospective study of 3192 pregnant women.
Arch Dermatol. 130:734–739. 1994.PubMed/NCBI
|
|
5
|
Shornick JK: Dermatoses of pregnancy.
Semin Cutan Med Surg. 17:172–181. 1998.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Jenkins RE, Jones SA and Black MM:
Conversion of pemphigoid gestationis to bullous pemphigoid-two
refractory cases highlighting this association. Br J Dermatol.
135:595–598. 1996.PubMed/NCBI
|
|
7
|
Di Zenzo G, Calabresi V, Grosso F, Caproni
M, Ruffelli M and Zambruno G: The intracellular and extracellular
domains of BP180 antigen comprise novel epitopes targeted by
pemphigoid gestationis autoantibodies. J Invest Dermatol.
127:864–873. 2007.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Kasperkiewicz M, Zillikens D and Schmidt
E: Pemphigoid diseases: Pathogenesis, diagnosis, and treatment.
Autoimmunity. 45:55–70. 2012.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Sadik CD, Lima AL and Zillikens D:
Pemphigoid gestationis: Toward a better understanding of the
etiopathogenesis. Clin Dermatol. 34:378–382. 2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Shornick JK, Jenkins RE, Artlett CM,
Briggs DC, Welsh KI, Kelly SE, Garvey MP and Black MM: Class II MHC
typing in pemphigoid gestationis. Clin Exp Dermatol. 20:123–126.
1995.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Jenkins RE, Hern S and Black MM: Clinical
features and management of 87 patients with pemphigoid gestationis.
Clin Exp Dermatol. 24:255–259. 1999.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Shornick JK and Black MM: Fetal risks in
herpes gestationis. J Am Acad Dermatol. 26:63–68. 1992.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Chi CC, Wang SH, Charles-Holmes R,
Ambros-Rudolph C, Powell J, Jenkins R, Black M and Wojnarowska F:
Pemphigoid gestationis: Early onset and blister formation are
associated with adverse pregnancy outcomes. Br J Dermatol.
160:1222–1228. 2009.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Al-Saif F, Elisa A, Al-Homidy A, Al-Ageel
A and Al-Mubarak M: Retrospective analysis of pemphigoid
gestationis in 32 Saudi patients-clinicopathological features and a
literature review. J Reprod Immunol. 116:42–45. 2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Aoyama Y, Asai K, Hioki K, Funato M, Kondo
N and Kitajima Y: Herpes gestationis in a mother and newborn:
Immunoclinical perspectives based on a weekly follow-up of the
enzyme-linked immunosorbent assay index of a bullous pemphigoid
antigen noncollagenous domain. Arch Dermatol. 143:1168–1172.
2007.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Joly P, Roujeau JC, Benichou J, Picard C,
Dreno B, Delaporte E, Vaillant L, D'Incan M, Plantin P, Bedane C,
et al: A comparison of oral and topical corticosteroids in patients
with bullous pemphigoid. N Engl J Med. 346:321–327. 2002.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kirtschig G, Middleton P, Bennett C,
Murrell DF, Wojnarowska F and Khumalo NP: Interventions for bullous
pemphigoid. Cochrane Database Syst Rev.
2010(CD002292)2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Gan DC, Welsh B and Webster M: Successful
treatment of a severe persistent case of pemphigoid gestationis
with antepartum and postpartum intravenous immunoglobulin followed
by azathioprine. Australas J Dermatol. 53:66–69. 2012.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Nguyen T, Alraqum E and Razzaque Ahmed A:
Positive clinical outcome with IVIg as monotherapy in recurrent
pemphigoid gestationis. Int Immunopharmacol. 26:1–3.
2015.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Turcan N, Bohiltea RE, Ionita-Radu F,
Furtunescu F, Navolan D, Berceanu C, Nemescu D and Cirstoiu MM:
Unfavorable influence of prematurity on the neonatal prognostic of
small for gestational age fetuses. Exp Ther Med. 20:2415–2422.
2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Oumeish OY and Parish JL: Impetigo
herpetiformis. Clin Dermatol. 24:101–104. 2006.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Bellman B and Berman B: Skin diseases
seriously affecting fetal outcome and maternal health. In: Skin
Changes and Diseases in Pregnancy. Harahap K and Wallach RC (eds).
Marcel Dekker, Inc., New York, NY pp129, 1996.
|
|
23
|
Ovadia C, Seed PT, Sklavounos A, Geenes V,
Di Ilio C, Chambers J, Kohari K, Bacq Y, Bozkurt N, Brun-Furrer R,
et al: Association of adverse perinatal outcomes of intrahepatic
cholestasis of pregnancy with biochemical markers: Results of
aggregate and individual patient data meta-analyses. Lancet.
393:899–909. 2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Radoi VE, Ursu RI, Poenaru E, Arsene C,
Bohiltea CL and Bohiltea R: Frequency of the UGT1A1*28 polymorphism
in a Romanian cohort of Gilbert syndrome individuals. J
Gastrointestin Liver Dis. 26:25–28. 2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Al Saif F, Jouen F, Hebert V, Chiavelli H,
Darwish B, Duvert-Lehembre S and Joly P: French Study Group on
Autoimmune Bullous Skin Diseases: Sensitivity and specificity of
BP180 NC16A enzyme-linked immunosorbent assay for the diagnosis of
pemphigoid gestationis. J Am Acad Dermatol. 76:560–562.
2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Society for Maternal-Fetal Medicine
(SMFM). Electronic address: simplepubs@smfm.org. Lee RH, Mara
Greenberg, Metz TD and Pettker CM: Society for maternal-fetal
medicine consult series #53: Intrahepatic cholestasis of pregnancy:
Replaces consult #13, April 2011. Am J Obstet Gynecol. 224:B2–B9.
2021.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Huilaja L, Surcel HM, Bloigu A and Tasanen
K: Elevated serum levels of BP180 antibodies in the first trimester
of pregnancy precede gestational pemphigoid and remain elevated for
a long time after remission of the disease. Acta Derm Venereol.
95:843–844. 2015.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Srinivasana S and Strasburger J: Overview
of fetal arrhythmias. Curr Opin Pediatr. 20:522–531.
2008.PubMed/NCBI View Article : Google Scholar
|