1. Introduction
Repurposing bioactive substances is a method, where
already existing moieties, such as the pineal hormone, melatonin,
are used in pharmacological studies, to determine their effect on
emerging and complex diseases (1). A plethora of known drugs in
circulation are being evaluated against COVID-19, as de novo
drug discovery is costly and very time consuming (10 to 15 years);
thus, drug repurposing significantly reduces the cost and time in
treating COVID-19, in this pandemic (2). The ongoing COVID-19 pandemic
continues to advance globally, as the virus spreads to new
geographical areas; therefore, morbidity and mortality rates are
continuously increasing (3).
There is one promising drug, that has recently been identified, as
a potential tool in treating patients with COVID-19, which is
melatonin; thus, it is essential to examine its safety and efficacy
(4).
Melatonin is biosynthesized in the pineal gland,
primarily at night. It has been previously documented, that it
interacts with various cellular proteins and enzymes, resulting in
multiple biological effects (5,6).
The physiological actions of melatonin are exerted via G-protein
coupled seven transmembrane cell membrane receptors (subtypes MT1
and MT2) and non-receptor-dependent mechanisms. The MT1 receptor
has been associated with mammalian brain function, whilst the MT2
receptor is known to be involved in the body's circadian rhythms
(5,6).
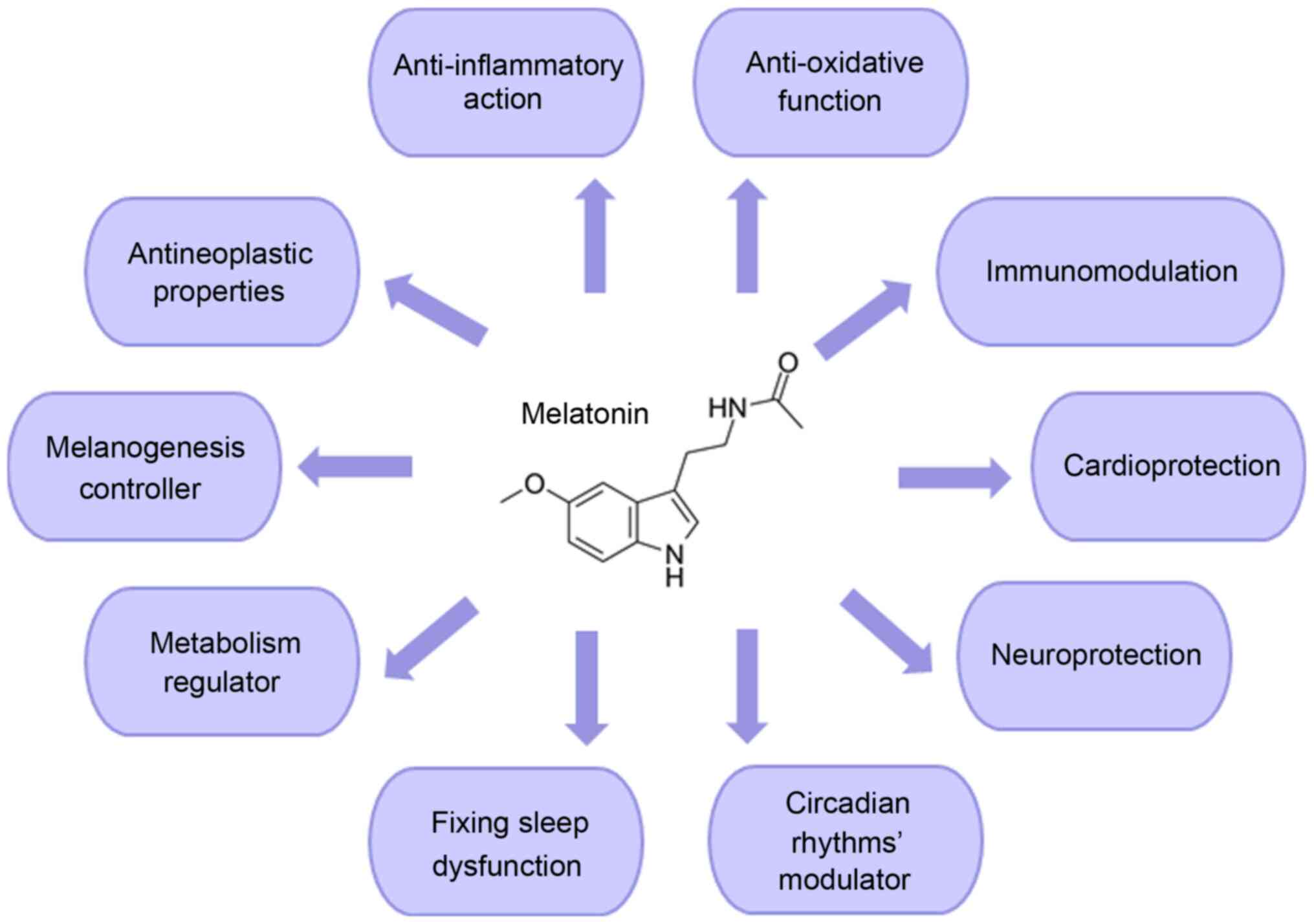
Melatonin's beneficial properties, as a
neuroprotective and cardioprotective agent, have been previously
identified. Furthermore, melatonin plays essential roles in the
female reproduction system/male fertility, resynchronization of
biological rhythms, sleep initiation/maintenance and metabolism,
ocular functions and rheumatological diseases (7-9).
With respect to its oncostatic properties, melatonin easily
interacts with the cell (both intracellularly and onto its surface
receptors) to alter a broad spectrum of important pathways that are
vital for its survival (10-12). These include cellular metabolism,
apoptosis, circadian disruption, cell-to-cell communication and
suppression of angiogenesis (12-14). In addition to these functions,
melatonin is known to exert immunomodulation, anti-inflammatory and
antioxidative effects. Due to these properties, melatonin has been
hypothesized to be capable of limiting viral infections (Fig. 1) (15).
2. Suggested mechanisms of action of
melatonin against viral infections
Melatonin cannot be classified as a viricidal drug;
however, it could, indirectly, target viruses, via its
anti-inflammatory, anti-oxidative and immune system enhancing
actions (4). Melatonin has been
used in the past, in experimental studies, both in vitro and
in vivo, against viral infections with noticeable results
(15-55). In particular, it has been used
against the Venezuelan equine encephalitis/encephalomyelitis (VEE)
virus infection, viral hepatitis, viral myocarditis, respiratory
syncytial virus infection and the Ebola virus.
Patients with the VEE virus show flu-like symptoms,
such as a sore throat, fever and weariness; however, in some cases,
patients develop severe neurological complications, that can lead
to encephalitis, chronic neurological deficits and death (16). Studies have shown that this
particular virus, due to its ability to replicate in the brain,
causes inflammation and subsequent blood-brain barrier disruption,
leading to increased permeability, and subsequently to
neuro-invasion and prolonged neurological sequelae (16-20). Furthermore, microglia respond to
the resulting infection by releasing pro-inflammatory agents
(21). VEE virus-infected mice
brain was evaluated and the results indicated a complex immune
response. Treatment with melatonin indicated that, the
immunoregulatory and pro-oxidant properties of melatonin may
exhibit an antiviral profile against the VEE virus by reducing
oxidative stress (22). It has
also been suggested that melatonin could diminish the enhanced
brain expression level of apoptosis marker proteins, the
concentration of malondialdehyde and nitric oxide (NO) in VEE
virus-infected mice. Furthermore, the hormone may enhance the
survival rate (23) and decrease
NO and lipid peroxidation substance levels in the brain of affected
animals (24). A previous study
also demonstrated that melatonin could reduce NO concentrations in
infected splenocytes (25).
These results showed that the VEE virus-infected splenocytes
generated markedly higher counts of NO in the splenic tissue.
Therefore, melatonin could protect the VEE virus-infected mice by
reducing NO levels (15,25).
Melatonin has also been associated with acute liver
failure, also known as viral hepatitis, which is characterized by
jaundice, and the progression of encephalopathy, which leads to
extensive liver necrosis (26).
A previous study suggested that the hepatoprotective role of
melatonin could be noticeably induced by activating the nuclear
factor erythroid 2-related factor 2 pathway, leading to the
reduction of oxidative stress and the emergence of antioxidant
enzymes (27). The suppressive
effects of the hormone on apoptotic damage of the liver was
associated with the inhibition of endoplasmic reticulum (ER)
stress, by regulating the three arms of the unfolded protein
response signaling pathway (15,26).
Apart from the role of melatonin in treating these
viruses, the hormone has been shown to have a beneficial role in
treating viral myocarditis (28). Myocarditis causes inflammation of
the cardiac muscle tissues. Infectious causes of myocarditis
include a wide range of parasites, such as fungi, protozoa,
bacteria and viruses; however, it is most commonly associated with
the inflammatory effects from viral pathogens (28). Previous studies have suggested
that apart from enteroviruses and adenoviruses, such as
coxsackievirus B3 (CVB3), the human herpes virus 6 and parvovirus
B19, are responsible for the emergence of cardiotropic viruses
(28,29). The protective role of melatonin
in viral myocarditis, with a focus on the Mst1-Hippo signaling
pathway, ER stress and mitochondrial dysfunction, has been
investigated. It was found that the hormone improved cardiac
function and repressed virus-induced cardiomyocyte apoptosis. In
addition, Mst1 upregulation, caused by the virus infection, was
rescued by the action of melatonin (30). A previous study investigated the
protective role of melatonin on viral myocarditis in vivo.
Treatment of the hormone significantly healed myocardial injuries,
by repressing inflammation (31). Other possible mechanisms of
melatonin include the regulation of the rate of autophagy and
apoptosis inhibition in mice with CVB3-induced myocarditis
(15,31,32).
Furthermore, melatonin has been hypothesized to
affect thrombin formation and platelet physiology, caused by the
Ebola virus, which increases blood coagulation and damages blood
vessels, leading to hemorrhagic shock and possibly death (33). In addition, it has been suggested
that melatonin increased the protein expression level of the enzyme
heme oxygenase 1, which reduced the replication of the Ebola virus
(15,34,35).
The therapeutic effects of melatonin, in the
respiratory system, have been identified, and it was found to block
nuclear factor-κB (NF-κB), the overexpression of c-Fos, and the
downregulation of matrix metalloproteinases-3 (MMP-3), which leads
to pro-fibrotic and pro-inflammatory cytokine production (36,37). In addition, the beneficial role
of melatonin in pulmonary hypertension has been associated with its
antioxidant, anti-fibrotic and vasodilator effects (34).
Melatonin has also shown a protective effect on
pulmonary tissues, which have been injured following acute lung
injury (38). The novel analogue
of melatonin, 5-hydroxy-2'-isobutyl-streptochlorin (HIS), has
notably anti-inflammatory properties and has been found to inhibit
the entry of immune cells into the lung, and decrease the release
of pro-inflammatory cytokines, such as TNF-α and IL-6. These
anti-inflammatory actions of HIS are mediated by the regulation of
interferon-β and toll-like receptors-dependent signaling pathways
(38). Furthermore, HIS
prevented the secretion of IL-1β, by inhibiting the activation of
the NLRP3 inflammasome (38,39). The lipid peroxidation of the lung
surfactant occurs from the production of oxygen free radicals from
the activated phagocytes, which are responsible for causing acute
lung injury. Melatonin, on its own or in combination with other
antioxidants, reduced lipid peroxidation of the pulmonary
surfactant (40). The
administration of melatonin led to a notable reduction in lung
lesions and the accumulation of neutrophils (a type of granulocyte,
that and constitutes 40-70% of all white blood cells in humans) and
macrophages into the lungs during acute pulmonary injury. In
addition, melatonin was found to inhibit the development of the
NLRP3 inflammasome by suppressing extracellular histone release
(41). Melatonin could act by
prohibiting pulmonary fibrosis in a rat animal model, due to
minimizing chloride channel activity, which was mediated by protein
kinase C (42). In another
study, melatonin modulated pneumonitis and lung fibrosis, caused by
exposure to radiation by decreasing inflammatory cell infiltration,
collagen deposition and alveolar thickening in the lungs (43). It is noteworthy, that melatonin
and its metabolites could regulate the appropriate pro-fibrogenic
and pro-inflammatory signaling pathways, which are involved in the
pathophysiology of pulmonary fibrosis, leading to its protective
effects on the lungs (44).
Melatonin has been hypothesized to remove free radicals, and
therefore may modulate autophagy pathways and apoptosis, which are
critical factors in the development of idiopathic pulmonary
fibrosis (10). In addition, the
use of melatonin in animals (rats and rabbits), with induced
hepatopulmonary syndrome, has been proven to be beneficial in the
reduction of lung fibrosis levels, oxidative stress and
vasodilation (45).
Pulmonary lesions, which have been associated with
inflammation and oxidative stress, and are caused by nitrogen
mustard in rodents, were found to be ameliorated by melatonin, as
it acts as an effective reactive nitrogen and oxygen species
scavenger, and as an anti-inflammatory compound (46-48). Pretreatment with melatonin, alone
or in combination with quercetin in rats, with hypoxia-induced by
sodium nitrite, markedly reduced the plasma levels of IL-6, tumor
necrosis factor-α, CRP, heat shock protein 70 extracellular
(Hsp70e), and VEGF. In addition, melatonin improved the
histopathological changes in the lungs, such as improvement of the
alveoli and alveolar septae, and a marked decrease in cellular
infiltration, acting as a protector at the pulmonary level
(49).
Melatonin has also been found to affect the protein
expression level of hypoxia-inducible factor-1α and NF-κB in a
murine model of hypoxic pulmonary hypertension (50). Furthermore, in vitro
experiments suggested that the hormone could diminish the
proliferation of pulmonary artery smooth muscle cells and the
levels of phosphorylated Akt and extracellular signal-regulated
kinases 1/2 (50). The possible
mechanistic pathways, where melatonin could affect the route of
COVID-19 infection, are illustrated in Fig. 2. In view of this, the well-known
melatonin's anti-inflammatory and anti-oxidative properties can aid
in reducing the production of pro-inflammatory cytokines. A number
of these actions are mediated by its MT1 and MT2 receptors
(37,51).
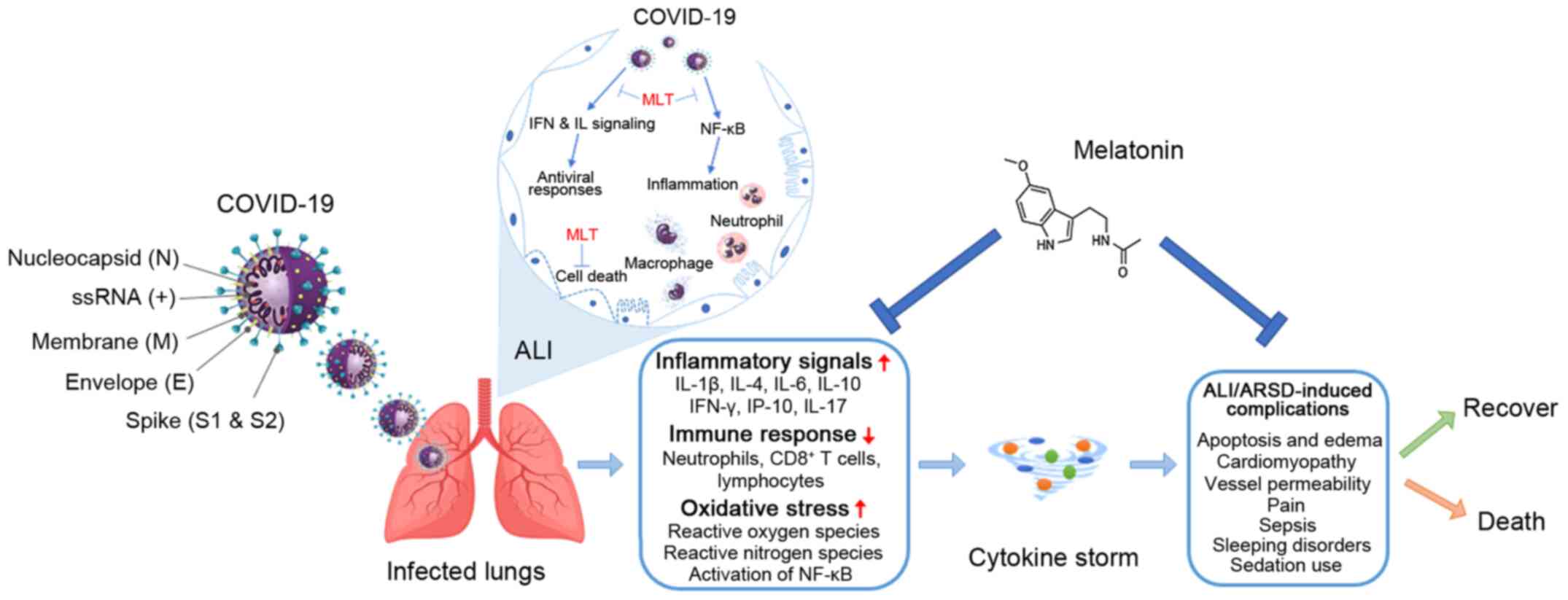 | Figure 2Possible mechanistic routes, in which
melatonin could affect the infection process. Serious inflammation,
oxidation, and an over-reactive immune system response contribute
to COVID-19 pathology, leading to a cytokine storm causing
ALI/ARDS, and frequently death, which could be reduced by the
administration of melatonin. ALI, acute lung injury; ARDS,
respiratory distress syndrome; ss, single strand; MLT,
melatonin. |
In a recent study, the importance of the CD147
glycoprotein and the protective role of melatonin, which is
mediated by CD147 in COVID-19, was investigated. It is known that
CD147 is involved in the increase in the number of cytokines in the
lungs caused by viral invasion. It was found that reduced levels of
melatonin, which are found in patients who are middle-aged (40-60
years old) and elderly (>60 years old) and patients who are
immune-suppressed, should be replenished by the administration of
exogenous melatonin, as an adjuvant, in the treatment of COVID-19
(52).
Furthermore, the administration of the melatonin
receptor drug, Ramelteon, in rats with lung injury, had various
effects (53). In particular, it
markedly reduced pulmonary edema, the serum concentration of
1,3-propanedial, the population of pro-inflammatory cytokines in
the bronchoalveolar lavage fluid, the activation of NF-κB, the
protein expression level of inducible NO synthase in lung cells,
and lung cells apoptosis. In addition, this drug treatment notably
increased the protein expression level of intracellular protective
heat shock protein 70, in lung cells, and the concentration of the
anti-inflammatory cytokine, IL-10, in the bronchoalveolar lavage
fluid. The results from the study recommended that the protective
effects of melatonin on lung disease, were primarily mediated by
its receptor (53).
In a meticulous study investigating the structure
and physicochemical characteristics of melatonin, using electronic
structure techniques and molecular-mechanics software, a vast
amount of information was found regarding the steroelectronic
characteristics of melatonin, which enabled the prediction of its
bioactivity (54). In addition,
the molecular docking investigation predicted the essential
features of the molecules to treat the COVID-19 proteins. The
maximum docking scores of -7.28, -7.20, and -7.06 kcal/mol
indicated that melatonin could be beneficial to protect against the
viral load in vulnerable populations (54).
3. Clinical trials using melatonin to treat
COVID-19
At present, there is a limited number of clinical
trials, using melatonin as a bioactive substance to treat COVID-19;
however, the results so far are promising (55). Randomized controlled clinical
trials are the gold standard for clinical research and they are
required to establish whether there is an actual clinical benefit
in using melatonin to treat COVID-19. The following studies are
indicative of the action of melatonin on the serious symptoms,
which develop as a result of contracting COVID-19.
The augmenting rate of COVID-19 infection and
associated death is of ultimate concern; therefore, it is important
to eliminate the spread and that new clinical trials are designed
to, not only ameliorate the pathological symptoms of COVID-19, but
also to eliminate the high death rate (55). At present, there is not a
promising and effective therapy, that is able to treat
COVID-19.
Pharmaceutical research is focused on the
investigation of novel drugs; however, this is time consuming, due
to drug resistance and repeatedly occurring virus mutations
(56-58). Furthermore, antiviral drugs are
effective in mild to moderate cases of the virus, if used in early
stages; however, they are not able to treat patients who have
severe symptoms, due to overreaction of the innate immune response,
which leads to destructive inflammation (59,60). To overcome the complexity of
viral infection, a symptomatic and non-virus-specific therapy
should be considered (61).
Clinical trials have shown satisfactory safety
results when melatonin was administered orally, at 3, 6 and 10 mg
in patients in intensive care units (ICUs) in hospital (62-64). Furthermore, another clinical
study has shown that there were no adverse reports when melatonin
was used at a high dose of 1 g/day, for a month in humans (65). It has a high safety profile in
humans; however, it is vital that melatonin should be controlled
thoroughly when it is administered to patients with COVID-19
(4,66).
In view of the fact that melatonin has been found to
have effective anti-inflammatory and anti-oxidative properties,
which are known to enhance the innate immune system and promote
adaptive immunity (51,55), it can be used as an adjuvant
therapy in treating patients with COVID-19, with lower and
predictive side effects compared to a novel drug, providing a
supportive profile for a direct and safe clinical use in patients
(4,67,68). Furthermore, its safe use has been
corroborated by the fact that melatonin lacks toxicity: A
LD50 value (lethal dose for 50% of the animals used)
could not be established. In addition, a high-dose of 800 mg/kg for
bodyweight was not lethal (69).
Studies, which used human subjects, and were treated with varying
doses of melatonin (1-6.6 g/day) for 30-45 days, have concluded
that, aside from drowsiness, all other side effects (headache,
stomach cramps, persistent sleepiness and somnolence) were not
apparent at the end of the test period (65,70).
At present, there are some ongoing clinical trials,
that have investigated the therapeutic dynamic of melatonin in
treating COVID-19 (Table I). It
has been observed that melatonin was only used in 11 clinical
trials. The time spent on clinical trials, using a bioactive
compound, such as melatonin, is not supported, due to the lack of
protective patents for a natural compound (71). However, this obstacle has to be
surpassed, not only due to its highly safe and effective profile,
but also due to its multifactorial and synergic pharmacological
actions (15,72).
 | Table IClinical trials that include
melatonin in their COVID-19 therapy protocols. |
Table I
Clinical trials that include
melatonin in their COVID-19 therapy protocols.
| Study
identifier | Study title | IMP | Location | Trial start date
(status) |
|---|
| EudraCT:
2020-001808-42a | Phase II clinical
trial, single-blind, randomized, placebo controlled, to explore the
effectiveness and safety of melatonin IV in patients with COVID-19
entered into the ICU | IV melatonina, 6
mg/ml | Spain | 17/06/2020
(ongoing) |
| EudraCT:
2020-001530-35a | Randomized
multicenter clinical trial to evaluate the efficacy of melatonin in
the prophylaxis of SARS-CoV-2 infection in high-risk contacts |
Circadin®, 2 mg | Spain | 09/04/2020
(ongoing) |
| NCT04474483 | Safety and efficacy
of melatonin in outpatients infected with COVID-19 | Melatonin, 10 mg
Placebo | State University of
New York, Buffalo, United States | 06/11/2020
(recruiting) |
| NCT04531748 | Selective estrogen
modulation and melatonin in early COVID-19 | Toremifene, 60 mg
Melatonin, 100 mg Placebo and melatonin, 100 mg | The Cleveland
Clinic, Ohio, United States | 12/2020 (not yet
recruiting) |
| NCT04409522 | Evaluation of
therapeutic effects of melatonin by inhibition of NLRP3
inflammasome in COVID19 patients | Melatonin, 9 mg
Usual treatment | Tehran, Islamic
Republic of Iran | 12/05/2020
(recruiting) |
| NCT04568863 | Efficacy of
intravenous melatonin on mortality in adult patients admitted to
the intensive care unit with COVID-19 | IV melatonin, 5
mg/kg IV placebo | La Paz University
Hospital, Madrid, Spain | 20/06/2020
(recruiting) |
| NCT04530539 | The effect of
melatonin and vitamin C on COVID-19 | Vitamin C, 1,000 mg
Melatonin, 10 mg Placebo Symptom survey | Lancaster,
Pennsylvania, United States | 18/09/2020 (not yet
recruiting) |
| NCT04470297 | Melatonin agonist
on hospitalized patients with confirmed or suspected COVID-19 | Ramelteon, 8
mg | None | 09/2020 (not yet
recruiting) |
| NCT04353128 | Efficacy of
melatonin in the prophylaxis of Coronavirus disease 2019 among
healthcare workers | Melatonin, 2 mg
Placebo | La Paz University
Hospital, Madrid, Spain | 20/04/2020
(recruiting) |
| NCT04570254 | Antioxidants as
adjuvant therapy to standard therapy in patients with COVID-19 | Vitamin C, 1,000 mg
Vitamin E, 800 mg Melatonin, 50 mg N-acetylcysteine, 600 mg
Pentoxifylline, 400 mg | Temporary COVI D-19
Unit at Centro Citibanamex, Mexico City, Mexico | 19/08/2020 (active,
not recruiting) |
|
IRCT20200506047323N5 | Evaluation of the
efficacy and safety of melatonin in moderately ill patients with
COVID-19 | Melatonin, 50
mg | Shahid Mohammadi
Hospital, Bandar Abbas, Iran | 14/08/2020
(ongoing) |
A clinical trial (EudraCT, 2020-001808-42) has been
approved by the Spanish Agency of Medicines and Medical Devices
(AEMPS), which allows the identification of the doses of melatonin,
that can be effective in treating COVID-19 (73,74). This is a phase II, single center,
double-blind, placebo-controlled randomized trial with a two-arm
parallel group design and a 2:1 allocation ratio. The chosen
participants are solely critically ill adult patients, that fulfill
all of the inclusion criteria and none of the exclusion criteria.
The anticipated main outcome is the mortality rate, in each study
group, which is represented in frequency and time-to-event at day
28, after randomization.
Furthermore, the AEMPS has also approved another
randomized clinical trial (EudraCT, 2020-001530-35) (75). This is a randomized multicenter
clinical trial, which will evaluate the efficacy of melatonin for
the prophylaxis of SARS-CoV-2 infection, in patients who are
high-risk, using 2 mg Circadin®, as medication.
Another study (NCT04474483) is being undertaken at
the State University of New York in Buffalo (USA), which is a pilot
randomized, double-blind, placebo-controlled clinical trial
(76). This clinical trial will
evaluate the effect and safety of melatonin in out-patient adults,
possibly infected with COVID-19. The purpose of this study is to
assess the clinical profile of melatonin, compared with that in
patients being treated with a placebo, with respect to
COVID-19-related symptoms. It will also analyze the mortality rate
and define whether the antioxidant and anti-inflammatory actions of
melatonin are able to reduce the threat and severity of COVID-19 in
a mild state infection.
The clinical trial, NCT04531748, is a clinical trial
evaluating a 14-day intervention, with either a combination
treatment of toremifene and melatonin or melatonin alone, in adults
with mild COVID-19 (77). This
study is double-blind, the allocation is randomized and assesses
whether there is amelioration of symptoms (fatigue, fever, cough
and dyspnea) and clinical signs, compared with that in patients
being treated with the placebo, for 30 days.
Another clinical trial (NCT04409522), being
undertaken in Iran, will use melatonin, as an anti-inflammatory
treatment, when severe inflammation occurs in patients with
COVID-19 (78). In this trial,
the pharmacological role of melatonin, in inhibiting the
inflammasome, NLRP3, a mechanism responsible for numerous serious
inflammatory disorders, is examined. It has been hypothesized that
measurements of melatonin levels in the human body are essential to
characterize melatonin as a potential adjuvant in antiviral medical
therapies to treat COVID-19.
In a melatonin-COVID-19 study (NCT04568863), being
undertaken at the La Paz University Hospital (Madrid, Spain), which
is a phase II, double-blind, single-center and randomized
placebo-controlled clinical trial, the safety and efficacy of
intravenously administered melatonin in patients with COVID-19, in
the ICUs, is being investigated (79). The clinical condition of the
patients with COVID-19 in the ICUs is characterized by a high risk
of sepsis, respiratory malfunctions and death. This clinical trial
intends on decreasing the mortality rate and ameliorating the
patient's outcome by preventing the creation of free radicals and
the development of sepsis.
There is another double-blind placebo-controlled
clinical trial (NCT04530539), which has been developed at the
Lancaster General Hospital (Pennsylvania, USA) and assesses the
benefits of administering melatonin and vitamin C to patients with
COVID-19 (80).
In another clinical trial for COVID-19 (NCT04470297)
melatonin is being investigated as an antiapoptotic, antioxidative
and anti-inflammatory therapy in treating acute lung injury
(81). In this study, the
medical effects of ramelteon (8 mg), a melatonin receptor selective
agonist, are being determined, and aims to minimize the risk of
clinical downturn and the prolonged hospitalization of patients
with COVID-19.
Melatonin is also being used in another clinical
trial (NCT04353128), undertaken at the La Paz University Hospital
(Spain), and intends to prevent the infection of COVID-19 in
healthcare workers, who are at high risk (82). This is a randomized controlled
trial, in which melatonin is being used for its anti-inflammatory
and anti-oxidative properties, providing an effective shield to
protect healthcare personnel. This investigation suggested that
melatonin offers protection from severe COVID-19 symptoms, when
administered daily, at 2 mg.
In addition, the Cleveland Clinic (Ohio, United
States) published an observational study that analyzed 34 different
drugs used to treat a variety of diseases, such as respiratory,
cardiovascular, neurological, immunological and cancer, using
computational tests (83). Out
of these drugs, melatonin usage was found to lower the chance of a
positive COVID-19 test by 28%, which was confirmed using reverse
transcription-quantitative PCR. The study also found that melatonin
usage was associated with a 52% reduced likelihood of a positive
COVID-19 result in African Americans. Furthermore, melatonin usage
was associated with a reduced likelihood of a SARS-CoV-2 positive
test result compared with that in the use of angiotensin II
receptor blockers or angiotensin-converting enzyme inhibitors
(83). However, as this was an
observational study, its findings only suggest a possible
association between melatonin usage and COVID-19 and not
causation.
Furthermore, the ANTIOX-COVID (NCT04570254) study is
a trial, which administers 5 mg melatonin tablets, every 24 h
(total amount 50 mg) to patients with or without septic shock, in a
simultaneous administration of vitamin C, vitamin E,
N-acetylcysteine and pentoxifylline (a known hemorheologic agent,
which aids blood flow through narrowed arteries) (84). COVID-19 infection due to NO
formation and reactive nitrogen species, may lead to severe
pneumonia with pulmonary alveolar collapse. This trial is a
non-randomized controlled study and intends to examine the results
of a synergistic anti-oxidative effect of melatonin and
pentoxifylline, aimed at regulating the uncontrolled and high
oxidative stress provoked by COVID-19. In addition, this adjunct
treatment, with pentoxifylline and antioxidants, lowers
lipoperoxidation and oxidative stress, eliminating the requirement
for ventilation in patients with or without septic shock and
minimizes the SARS-COV2 pneumonia risk.
Lastly, the efficacy and safety of melatonin in
patients who are moderately ill with COVID-19 was evaluated in Iran
(Shahid Mohammadi Hospital; IRCT20200506047323N5) (85). This study primarily investigated
the recovery rate in patients with clinical symptoms and the oxygen
saturation, as well as, the improvement in the levels of serum
inflammatory parameters (CRP, TNF-α, IL-1β, and IL-6). It also
investigated the improvement of clinical and paraclinical symptoms,
along with the incidence of serious adverse drug reactions
(Table I) (86,87).
4. Conclusion
The so called 'hormone of darkness', melatonin, due
to its synthesis at night-time, has recently attracted the interest
of infectious diseases specialists and epidemiologists, due to its
adjuvant role in treating patients with COVID-19. The recent
clinical trials, which involve melatonin, have been highlighted,
collectively, in the present review, to the best of our knowledge,
for the first time. However, more clinical studies are required, to
understand the mechanism of action, at the molecular level, so that
its multifactorial and synergic pharmacological actions, coupled
with its high safety and effective profile, could be used to treat
patients with COVID-19, and reduce the impact of the pandemic.
Funding
No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
MV contributed to the design of the study and
supervised the writing of the manuscript. AS, AD and SKK retrieved
the data and wrote the manuscript. IPP aided in data extraction and
critically revised the manuscript. AS and AD designed Figs. 1 and 2. SKK and IPP edited and revised the
manuscript. All authors have read and agreed to the final version
of the manuscript. AS, AD, SKK and IPP confirm the authenticity of
the data presented in this manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Acknowledgments
SKK is indebted to the Onassis Foundation for
supporting this work via the scholarship G ZO 011-1/2018-2019.
References
|
1
|
Zhou Y, Wang F, Tang J, Nussinov R and
Cheng F: Artificial intelligence in COVID-19 drug repurposing.
Lancet Digit Heal. 2:e667–e676. 2020. View Article : Google Scholar
|
|
2
|
Konstantinidou S and Papanastasiou I:
Repurposing current therapeutic regimens against SARS-CoV-2
(Review). Exp Ther Med. 2:1845–1855. 2020.
|
|
3
|
Sidiropoulou P, Docea AO, Nikolaou V,
Katsarou MS, Spandidos DA, Tsatsakis A, Calina D and Drakoulis N:
Unraveling the roles of vitamin D status and melanin during
COVID-19 (Review). Int J Mol Med. 47:92–100. 2020. View Article : Google Scholar :
|
|
4
|
Zhang R, Wang X, Ni L, Di X, Ma B, Niu S,
Liu C and Reiter RJ: COVID-19: Melatonin as a potential adjuvant
treatment. Life Sci. 250:1175832020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Turek FW and Gillette MU: Melatonin,
sleep, and circadian rhythms: Rationale for development of specific
melatonin agonists. Sleep Med. 5:523–532. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zlotos DP: Recent advances in melatonin
receptor ligands. Arch Pharm (Weinheim). 338:229–247. 2005.
View Article : Google Scholar
|
|
7
|
Jahanban-Esfahlan R, Mehrzadi S, Reiter
RJ, Seidi K, Majidinia M, Baghi HB, Khatami N, Yousefi B and
Sadeghpour A: Melatonin in regulation of inflammatory pathways in
rheumatoid arthritis and osteoarthritis: Involvement of circadian
clock genes. Br J Pharmacol. 175:3230–3238. 2018. View Article : Google Scholar :
|
|
8
|
Kratz EM and Piwowar A: Melatonin,
advanced oxidation protein products and total antioxidant capacity
as seminal parameters of prooxidant-antioxidant balance and their
connection with expression of metalloproteinases in context of male
fertility. J Physiol Pharmacol. 68:659–668. 2017.
|
|
9
|
Olcese JM: Melatonin and female
reproduction: An expanding universe. Front Endocrinol (Lausanne).
11:852020. View Article : Google Scholar
|
|
10
|
Hosseinzadeh A, Javad-Moosavi SA, Reiter
RJ, Yarahmadi R, Ghaznavi H and Mehrzadi S: Oxidative/nitrosative
stress, autophagy and apoptosis as therapeutic targets of melatonin
in idiopathic pulmonary fibrosis. Expert Opin Ther Targets.
22:1049–1061. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hosseinzadeh A, Javad-Moosavi SA, Reiter
RJ, Hemati K, Ghaznavi H and Mehrzadi S: Idiopathic pulmonary
fibrosis (IPF) signaling pathways and protective roles of
melatonin. Life Sci. 201:17–29. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Luchetti F, Canonico B, Betti M,
Arcangeletti M, Pilolli F, Piroddi M, Canesi L, Papa S and Galli F:
Melatonin signaling and cell protection function. FASEB J.
24:3603–3624. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hill SM, Belancio VP, Dauchy RT, Xiang S,
Brimer S, Mao L, Hauch A, Lundberg PW, Summers W, Yuan L, et al:
Melatonin: An inhibitor of breast cancer. Endocr Relat Cancer.
22:R183–R204. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Carlberg C: Gene regulation by melatonin.
Ann N Y Acad Sci. 917:387–396. 2000. View Article : Google Scholar
|
|
15
|
Bahrampour Juybari K, Pourhanifeh MH,
Hosseinzadeh A, Hemati K and Mehrzadi S: Melatonin potentials
against viral infections including COVID-19: Current evidence and
new findings. Virus Res. 287:1981082020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Weaver SC, Ferro C, Barrera R, Boshell J
and Navarro JC: Venezuelan equine encephalitis. Annu Rev Entomol.
49:141–174. 2004. View Article : Google Scholar
|
|
17
|
Schoneboom BA, Lee JS and Grieder FB:
Early expression of IFN-alpha/beta and iNOS in the brains of
Venezuelan equine encephalitis virus-infected mice. J Interferon
Cytokine Res. 20:205–215. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Schoneboom BA, Fultz MJ, Miller TH,
McKinney LC and Glieder FB: Astrocytes as targets for Venezuelan
equine encephalitis virus infection. J Neurovirol. 5:342–354. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Schoneboom BA, Catlin KMK, Marty AM and
Grieder FB: Inflammation is a component of neurodegeneration in
response to Venezuelan equine encephalitis virus infection in mice.
J Neuroimmunol. 109:132–146. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Cain MD, Salimi H, Gong Y, Yang L,
Hamilton SL, Heffernan JR, Hou J, Miller MJ and Klein RS: Virus
entry and replication in the brain precedes blood-brain barrier
disruption during intranasal alphavirus infection. J Neuroimmunol.
308:118–130. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Keck F, Kortchak S, Bakovic A, Roberts B,
Agrawal N and Narayanan A: Direct and indirect pro-inflammatory
cytokine response resulting from TC-83 infection of glial cells.
Virulence. 9:1403–1421. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Valero N, Mosquera J, Alcocer S, Bonilla
E, Salazar J and Álvarez-Mon M: Melatonin, minocycline and ascorbic
acid reduce oxidative stress and viral titers and increase survival
rate in experimental Venezuelan equine encephalitis. Brain Res.
1622:368–376. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Montiel M, Bonilla E, Valero N, Mosquera
J, Espina LM, Quiroz Y and Álvarez-Mon M: Melatonin decreases brain
apoptosis, oxidative stress, and CD200 expression and increased
survival rate in mice infected by Venezuelan equine encephalitis
virus. Antivir Chem Chemother. 24:99–108. 2015. View Article : Google Scholar
|
|
24
|
Valero N, MarinaEspina L, Bonilla E and
Mosquera J: Melatonin decreases nitric oxide production and lipid
peroxidation and increases interleukin-1 beta in the brain of mice
infected by the Venezuelan equine encephalomyelitis virus. J Pineal
Res. 42:107–112. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Valero N, Meleán E, Bonilla E, Arias J,
Espina LM, Chacin-Bonilla L, Larreal Y, Maldonado M and Añez F: In
vitro, melatonin treatment decreases nitric oxide levels in murine
splenocytes cultured with the venezuelan equine encephalomyelitis
virus. Neurochem Res. 30:1439–1442. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tuñõn MJ, San-Miguel B, Crespo I, Laliena
A, Vallejo D, Álvarez M, Prieto J and González-Gallego J: Melatonin
treatment reduces endoplasmic reticulum stress and modulates the
unfolded protein response in rabbits with lethal fulminant
hepatitis of viral origin. J Pineal Res. 55:221–228. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Crespo I, Miguel BS, Laliena A, Álvarez M,
Culebras JM, González-Gallego J and Tuñón MJ: Melatonin prevents
the decreased activity of antioxidant enzymes and activates nuclear
erythroid 2-related factor 2 signaling in an animal model of
fulminant hepatic failure of viral origin. J Pineal Res.
49:193–200. 2010.PubMed/NCBI
|
|
28
|
Verdonschot J, Hazebroek M, Merken J,
Debing Y, Dennert R, Brunner-La Rocca HP and Heymans S: Relevance
of cardiac parvovirus B19 in myocarditis and dilated
cardiomyopathy: Review of the literature. Eur J Heart Fail.
18:1430–1441. 2016. View
Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kühl U, Pauschinger M, Seeberg B, Lassner
D, Noutsias M, Poller W and Schultheiss HP: Viral persistence in
the myocardium is associated with progressive cardiac dysfunction.
Circulation. 112:1965–1970. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ouyang H, Zhong J, Lu J, Zhong Y, Hu Y and
Tan Y: Inhibitory effect of melatonin on Mst1 ameliorates
myocarditis through attenuating ER stress and mitochondrial
dysfunction. J Mol Histol. 50:405–415. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Sang Y, Gu X, Pan L, Zhang C, Rong X, Wu
T, Xia T, Li Y, Ge L, Zhang Y and Chu M: Melatonin ameliorates
coxsackievirus B3-induced myocarditis by regulating apoptosis and
autophagy. Front Pharmacol. 9:13842018. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Simko F, Hrenak J, Dominguez-Rodriguez A
and Reiter RJ: Melatonin as a putative protection against
myocardial injury in COVID-19 infection. Expert Rev Clin Pharmacol.
13:921–924. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Junaid A, Tang H, van Reeuwijk A,
Abouleila Y, Wuelfroth P, van Duinen V, Stam W, van Zonneveld AJ,
Hankemeier T and Mashaghi A: Ebola hemorrhagic shock
Syndrome-on-a-Chip. iScience. 23:1007652020. View Article : Google Scholar :
|
|
34
|
Martín Giménez VM, Inserra F, Tajer CD,
Mariani J, Ferder L, Reiter RJ and Manucha W: Lungs as target of
COVID-19 infection: Protective common molecular mechanisms of
vitamin D and melatonin as a new potential synergistic treatment.
Life Sci. 254:1178082020. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Hill-Batorski L, Halfmann P, Neumann G and
Kawaoka Y: The cytoprotective enzyme heme Oxygenase-1 suppresses
ebola virus replication. J Virol. 87:13795–13802. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hazra S, Chaudhuri AG, Tiwary BK and
Chakrabarti N: Matrix metallopeptidase 9 as a host protein target
of chloroquine and melatonin for immunoregulation in COVID-19: A
network-based meta-analysis. Life Sci. 257:1180962020. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Habtemariam S, Daglia M, Sureda A,
Selamoglu Z, Fuat Gulhan M and Mohammad Nabavi S: Melatonin and
respiratory diseases: A review. Curr Top Med Chem. 17:467–488.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Shim DW, Shin HJ, Han JW, Ji YE, Jang CH,
Koppula S, Kang TB and Lee KH: A novel synthetic derivative of
melatonin, 5-hydroxy-2'-isobutyl-streptochlorin (HIS), inhibits
inflammatory responses via regulation of TRIF-dependent signaling
and inflammasome activation. Toxicol Appl Pharmacol. 284:227–235.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Reiter RJ, Sharma R, Ma Q,
Dominquez-Rodriguez A, Marik PE and Abreu-Gonzalez P: Melatonin
inhibits COVID-19-induced cytokine storm by reversing aerobic
glycolysis in immune cells: A mechanistic analysis. Med Drug
Discov. 6:1000442020. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Bouhafs RKL and Jarstrand C: Effects of
antioxidants on surfactant peroxidation by stimulated human
polymorphonuclear leukocytes. Free Radic Res. 36:727–734. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zhang Y and Li X, Grailer JJ, Wang N, Wang
M, Yao J, Zhong R, Gao GF, Ward PA, Tan DX and Li X: Melatonin
alleviates acute lung injury through inhibiting the NLRP3
inflammasome. J Pineal Res. 60:405–414. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Soussia I Ben, Mies F, Naeije R and
Shlyonsky V: Melatonin down-regulates volume-sensitive chloride
channels in fibroblasts. Pflugers Arch. 464:273–285. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Farhood B, Aliasgharzadeh A, Amini P,
Rezaeyan A, Tavassoli A, Motevaseli E, Shabeeb D, Musa AE and
Najafi M: Mitigation of radiation-induced lung pneumonitis and
fibrosis using metformin and melatonin: A histopathological study.
Medicina (Kaunas). 55:4172019. View Article : Google Scholar
|
|
44
|
Hong S, Kim CY, Lee JE and Seong GJ:
Agmatine protects cultured retinal ganglion cells from tumor
necrosis factor-alpha-induced apoptosis. Life Sci. 84:28–32. 2009.
View Article : Google Scholar
|
|
45
|
Bosco AD, Schedler FB, Colares JR,
Schemitt EG, Hartmann RM, Forgiarini Junior LA, Dias AS and Marroni
NP: Melatonin effects on pulmonary tissue in the experimental model
of hepatopulmonary syndrome. J Bras Pneumol. 45:e201701642019.In
English, Portuguese. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Pita R, Marco-Contelles J, Ramos E, Del
Pino J and Romero A: Toxicity induced by chemical warfare agents:
Insights on the protective role of melatonin. Chem Biol Interact.
206:134–142. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Macit E, Yaren H, Aydin I, Kunak ZI, Yaman
H, Onguru O, Uysal B, Korkmaz A, Turel S and Kenar L: The
protective effect of melatonin and S-methylisothiourea treatments
in nitrogen mustard induced lung toxicity in rats. Environ Toxicol
Pharmacol. 36:1283–1290. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Llinàs L, Peinado VI, Ramon Goñi J,
Rabinovich R, Pizarro S, Rodriguez-Roisin R, Barberà JA and Bastos
R: Similar gene expression profiles in smokers and patients with
moderate COPD. Pulm Pharmacol Ther. 24:32–41. 2011. View Article : Google Scholar
|
|
49
|
Al-Rasheed NM, Fadda L, Attia HA, Sharaf
IA, Mohamed AM and Al-Rasheed NM: Pulmonary prophylactic impact of
melatonin and/or quercetin: A novel therapy for inflammatory
hypoxic stress in rats. Acta Pharm. 67:125–135. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Jin H, Wang Y, Zhou L, Liu L, Zhang P,
Deng W and Yuan Y: Melatonin attenuates hypoxic pulmonary
hypertension by inhibiting the inflammation and the proliferation
of pulmonary arterial smooth muscle cells. J Pineal Res.
57:442–450. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Hardeland R: Aging, melatonin, and the
pro-and anti-inflammatory networks. Int J Mol Sci. 20:12332019.
View Article : Google Scholar
|
|
52
|
Sehirli AO, Sayiner S and Serakinci N:
Role of melatonin in the treatment of COVID-19; as an adjuvant
through cluster differentiation 147 (CD147). Mol Biol Rep.
47:8229–8233. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Wu GC, Peng CK, Liao WI, Pao HP, Huang KL
and Chu SJ: Melatonin receptor agonist protects against acute lung
injury induced by ventilator through up-regulation of IL-10
production. Respir Res. 21:652020. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Al-Zaqri N, Pooventhiran T, Alsalme A,
Warad I, John AM and Thomas R: Structural and physico-chemical
evaluation of melatonin and its solution-state excited properties,
with emphasis on its binding with novel coronavirus proteins. J Mol
Liq. 318:1140822020. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Kleszczyński K, Slominski AT, Steinbrink K
and Reiter RJ: Clinical trials for use of melatonin to fight
against COVID-19 are urgently needed. Nutrients. 12:25612020.
View Article : Google Scholar
|
|
56
|
Wang R, Hozumi Y, Yin C and Wei GW:
Mutations on COVID-19 diagnostic targets. Genomics. 112:5204–5213.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Shariare MH, Parvez MAK, Karikas GA and
Kazi M: The growing complexity of COVID-19 drug and vaccine
candidates: Challenges and critical transitions. J Infect Public
Health. 14:214–220. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Shneider A, Kudriavtsev A and Vakhrusheva
A: Can melatonin reduce the severity of COVID-19 pandemic? Int Rev
Immunol. 39:153–162. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Shi J, Xiao Y, Zhang Y, Geng D, Cong D,
Shi KX and Knapp RJ: Challenges of drug development during the
COVID-19 pandemic: Key considerations for clinical trial designs.
Br J Clin Pharmacol. Oct 29–2020.Epub ahead of print. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Parvathaneni V and Gupta V: Utilizing drug
repurposing against COVID-19-Efficacy, limitations, and challenges.
Life Sci. 259:1182752020. View Article : Google Scholar
|
|
61
|
Acuña-Castroviejo D, Escames G, Figueira
JC, de la Oliva P, Borobia AM and Acuña-Fernández C: Clinical trial
to test the efficacy of melatonin in COVID-19. J Pineal Res.
69:e126832020. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Bourne RS, Mills GH and Minelli C:
Melatonin therapy to improve nocturnal sleep in critically ill
patients: Encouraging results from a small randomised controlled
trial. Crit Care. 12:R522008. View
Article : Google Scholar : PubMed/NCBI
|
|
63
|
Mistraletti G, Umbrello M, Sabbatini G,
Miori S, Taverna M, Cerri B, Mantovani ES, Formenti P, Spanu P,
D'Agostino A, et al: Melatonin reduces the need for sedation in ICU
patients: A randomized controlled trial. Minerva Anestesiol.
81:1298–1310. 2015.PubMed/NCBI
|
|
64
|
Mistraletti G, Sabbatini G, Taverna M,
Figini MA, Umbrello M, Magni P, Ruscica M, Dozio E, Esposti R,
DeMartini G, et al: Pharmacokinetics of orally administered
melatonin in critically ill patients. J Pineal Res. 48:142–147.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Nordlund JJ and Lerner AB: The effects of
oral melatonin on skin color and on the release of pituitary
hormones. J Clin Endocrinol Metab. 45:768–774. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Biancatelli RMLC, Berrill M, Mohammed YH
and Marik PE: Melatonin for the treatment of sepsis: The scientific
rationale. J Thorac Dis. 12(Suppl 1): S54–S65. 2020. View Article : Google Scholar
|
|
67
|
Herrera EA and González-Candia A: Comment
on melatonin as a potential adjuvant treatment for COVID-19. Life
Sci. 253:1177392020. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Moghadam SO: A review on currently
available potential therapeutic options for covid-19. Int J Gen
Med. 13:443–467. 2020. View Article : Google Scholar
|
|
69
|
Barchas J, DaCosta F and Spector S: Acute
Pharmacology of melatonin. Nature. 214:919–920. 1967. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Papavasiliou PS, Cotzias GC, Duby SE,
Steck AJ, Bell M and Lawrence WH: Melatonin and Parkinsonism. JAMA.
221:881972. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Pandi-Perumal SR, Cardinali DP, Reiter RJ
and Brown GM: Low melatonin as a contributor to SARS-CoV-2 disease.
Melatonin Res. 3:558–576. 2020. View Article : Google Scholar
|
|
72
|
Öztürk G, Akbulut KG and Güney Ş:
Melatonin, aging, and COVID-19: Could melatonin be beneficial for
COVID-19 treatment in the elderly? Turkish J Med Sci. 50:1504–1512.
2020. View Article : Google Scholar
|
|
73
|
EU Clinical Trials Register:
Eudract_number: 2020-001808-42. https://www.clinicaltrialsregister.eu/ctr-search/trial/2020-001808-42/ES.
Accessed December 5, 2020.
|
|
74
|
Rodríguez-Rubio M, Figueira JC,
Acuña-Castroviejo D, Borobia AM, Escames G and de La Oliva P: A
phase II, single-center, double-blind, randomized
placebo-controlled trial to explore the efficacy and safety of
intravenous melatonin in patients with COVID-19 admitted to the
intensive care unit (MelCOVID study): A structured summary of a
study protocol for a randomized controlled trial. Trials.
21:6992020. View Article : Google Scholar
|
|
75
|
EU Clinical Trials Register:
Eudract_number: 2020-001530-35. https://www.clinicaltrialsregister.eu/ctr-search/trial/2020-001530-35/ES.
Accessed December 5, 2020.
|
|
76
|
ClinicalTrials.gov: Safety and Efficacy of
Melatonin in Outpatients Infected With COVID-19. https://clinicaltrials.gov/ct2/show/NCT04474483?term=melatonin&cond=Covid19&draw=2&rank=1.
Accessed December 5, 2020.
|
|
77
|
ClinicalTrials.gov: Selective Estrogen
Modulation and Melatonin in Early COVID-19. https://clinicaltrials.gov/ct2/show/NCT04531748?term=melatonin&cond=Covid19&draw=2&rank=2.
December 5, 2020.
|
|
78
|
ClinicalTrials.gov: Evaluation of
Therapeutic Effects of Melatonin by Inhibition of NLRP3
Inflammasome in COVID19 Patients. https://clinicaltrials.gov/ct2/show/NCT04409522?term=melatonin&cond=Covid19&draw=1&rank=3.
Accessed December 5, 2020.
|
|
79
|
ClinicalTrials.gov: Efficacy of
Intravenous Melatonin on Mortality in Adult Patients Admitted to
the Intensive Care Unit With COVID-19. https://clinicaltrials.gov/ct2/show/NCT04568863?term=melatonin&cond=Covid19&draw=1&rank=4.
Accessed December 5, 2020.
|
|
80
|
ClinicalTrials.gov: The Effect of
Melatonin and Vitamin C on COVID-19. https://clinicaltrials.gov/ct2/show/NCT04530539?term=melatonin&cond=Covid19&draw=1&rank=5.
Accessed December 5, 2020.
|
|
81
|
ClinicalTrials.gov: Melatonin Agonist on
Hospitalized Patients With Confirmed or Suspected COVID-19.
https://clinicaltrials.gov/ct2/show/NCT04470297?term=melatonin&cond=Covid19&draw=1&rank=6.
Accessed December 5, 2020.
|
|
82
|
ClinicalTrials.gov: Efficacy of Melatonin
in the Prophylaxis of Coronavirus Disease 2019 (COVID-19) Among
Healthcare Workers. https://clinicaltrials.gov/ct2/show/NCT04353128?term=melatonin&cond=Covid19&draw=1&rank=7.
Accessed December 5, 2020.
|
|
83
|
Zhou Y, Hou Y, Shen J, Mehra R, Kallianpur
A, Culver DA, Gack MU, Farha S, Zein J, Comhair S, et al: A network
medicine approach to investigation and population-based validation
of disease manifestations and drug repurposing for COVID-19. PLoS
Biol. 18:e30009702020. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
ClinicalTrials.gov: Antioxidants as
Adjuvant Therapy to Standard Therapy in Patients With COVID-19.
https://clinicaltrials.gov/ct2/show/NCT04570254?term=melatonin&cond=Covid19&draw=1&rank=8.
Accessed December 5, 2020.
|
|
85
|
Hassaniazad M, Bazram A, Hassanipour S and
Fathalipour M: Evaluation of the efficacy and safety of favipiravir
and interferon compared to lopinavir/ritonavir and interferon in
moderately ill patients with COVID-19: A structured summary of a
study protocol for a randomized controlled trial. Trials.
21:8862020. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
ClinicalTrials.gov: Search of:
Melatonin|Covid19-List Results. https://clinicaltrials.gov/ct2/results?recrs=&cond=Covid19&term=melatonin&cntry=&state=&city=&dist=.
Accessed December 5, 2020.
|
|
87
|
EU Clinical Trials Register: Search for
covid-19 and melatonin. https://www.clinicaltrialsregister.eu/ctr-search/search?query=covid-19+and+melatonin.
Accessed December 5, 2020.
|