Introduction
The marked increase in the incidence of cancer
worldwide requires public health actions by governments and health
officers to control this trend and implement preventive measures
(1–3). At present, however, despite
scientific efforts to improve the outcome of cancer patients, an
increased cancer incidence leads to an increased likelihood of
death, particularly in certain tumour subtypes and in certain
geographical areas (4–6). It is important to have systematically
available population-based survival data for cancer patients in
order to aid health planners in allocating resources (1–6).
Data reported by the WHO for the year 2000 clearly
demonstrated that cancer had led to 12% of ∼56 million deaths
worldwide. More importantly, of the 5.3 million men and 4.7 million
women that developed a cancer, over half of the individuals (6.2
million), succumbed to this disease (1–3).
Surveillance of the impact of cancer on the general population by
cancer registries is the most powerful approach to estimate the
magnitude of the problem and plan appropriate strategies to prevent
the onset of the disease or, where not possible, to improve
measures for early detection. Moreover, information concerning the
incidence, prevalence, mortality and survival allows us to assess
the outcomes of screening and diagnostic procedures and the effect
of preventive and therapeutic interventions (4–9).
In 2006, individuals suffering from cancer (i.e.,
the prevalence) in Italy numbered to 2,244,000 (4% of the Italian
population), with a proportion of 4–5% in the Northern-Central
regions and 2–3% in the Southern regions, where the mortality rate
is more elevated. Female outnumbered male survivors (56 vs. 44%).
The Italian estimates are similar to those of Northern Europe, but
at least 15% lower compared to those in the United States (1–6,10).
In Italy, the cancer registries network is
comparable to the surveillance systems present in other
industrialized countries, although in the Southern regions of the
country it is inadequately represented (7–13).
The lack or malfunctioning of cancer registries in most of the
Southern Italian regions explains the wide variability in the
information available on cancer prevalence and incidence in
different areas of the Italian peninsula. The bulk of
epidemiological data on the Southern Italian population of cancer
patients originates from mortality and hospitalization records
(13–17). All the evidence available, however,
have limitations due to study design, confounder elements and
quality of exposure data (18–19).
However, the deficiency of a comprehensive database collecting the
most relevant clinical and biological tumour characteristics causes
a false or confounding perception of the problem in these areas
(18,19).
Data on cancer prevalence, incidence and mortality
in Campania, one of the most heavily populated Southern Italian
regions, are sparse and fragmentary and focus predominantly on
detailed geographical areas near landfills or single waste sites
(14–23). Campania is also the region with the
largest economic deficit due to health expenses. Obtaining
information concerning the impact of cancer incidence and
prevalence in this area may be critical to appropriately employ
human and economic resources, given the high costs of treatment and
diagnostic procedures. An ongoing update database recording patient
clinical and disease characteristics as well as treatment outcomes
may therefore be of great benefit in the development of a coherent
public health program.
In Italy, the National Health Services provide a
general practitioner (GP) to each citizen. The GP is familiar with
the risk factors, co-morbidities and diseases, including cancer,
affecting their particular patient population. Regarding patients
with cancer, data on cancer characteristics, the diagnostic and
therapeutic procedures performed on the patient, the possible
reasons for the selection of one treatment over another and the
clinical outcome are carefully recorded in the GP’s clinical
records. Therefore, the GP clinical chart databases contain all the
most relevant information required to produce an effective
surveillance program on the cancer patient population.
This is a pilot study evaluating the feasibility and
reliability of the characterization of the oncology population of a
central zone of Naples through the analyses of the medical records
of GPs practicing in that area. In the present study we also
evaluated the impact of cancer on the general population residing
in the center of Naples by reviewing GPs’ clinical charts. Relevant
clinical characteristics such as age, gender and site, based on the
International Classification of Disease, ninth revision (ICD-IX),
were analyzed in GP medical databases for cancer patients residing
in that area and the cancer prevalence in Naples was
determined.
Patients and methods
General
General practitioner databases (GPDs) containing
health information of patients residing in the center of Naples and
belonging to the local health service area ‘ASL Napoli 1 Centro’
were retrieved. The patients included in the study were assisted by
a GP belonging to the GPs cooperative Group ‘MEDI.CO’. This service
society has been acknowledged by the General Practitioner Regional
Agreement (D.P.R. 270/2000) to be appropriate for the elaboration
of population-based clinical studies. The MEDI.CO cooperative Group
is part of the Consorzio Nazionale delle Cooperative Mediche and
operates according to the scientific indications of SIMG (Italian
Society of General Medicine).
Cancer patients were identified if one of the
following criteria was present: registration of an ICD-IX revision
code diagnostic for malignant cancer (ICD-IX 140-208) based on
histological confirmation or on the presence of the disease code
p048 malignant cancer in health records. Clinical information and
disease characteristics of eligible patients were also searched in
the computerized or paper-based clinical charts and data registered
on preformed standardized sheets. Each GP participating in the
study, identified the cancer patients in his own patient population
and filed a summary diagram showing the number of patients
suffering from cancer compared to the total population. Cancer
patients were further classified according to the histotype and
particular conditions (metastases, double or second tumour).
Data were recorded in a dedicated computerized
database organized for the study using Microsoft Excel software
spreadsheets, according to a standardized shared coding. Informed
consent was obtained from each participant and data were assessed
according to the requirements of the national privacy law. Data
analyses were periodically performed in collaboration with the
Department of Oncology of the University of Naples ‘Federico II’
(24) (http://annonc.oxfordjournals.org/content/16/suppl_7/vii64.full.pdf).
Primary endpoints of the study were estimation of
the impact of cancer on the general population residing in the
center of Naples by analyzing the prevalence and verification of
the feasibility and reproducibility of tumour dynamic registries
performed by GPs on their GPDs.
A secondary objective was the investigation of the
distribution and predictive role of recently debated onco-genetic
risk factors such as gender, age and socio-economic position in an
identified cancer patient population, as in the case of the
inhabitants of Campania (14–20).
Statistical analysis
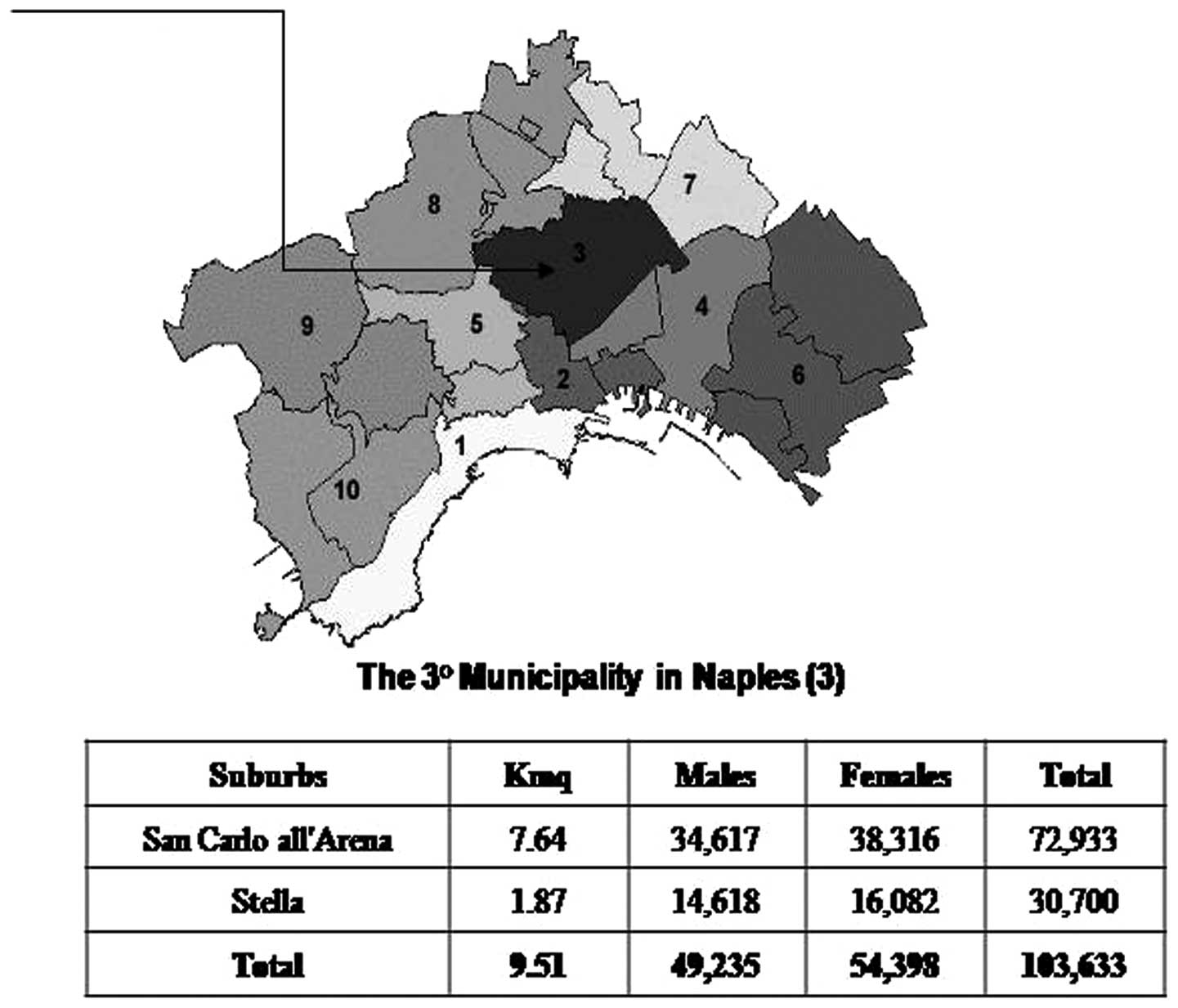
The study was initiated on September, 2004 (24). The patient population examined in
the study were from the ‘Stella’ and ‘San Carlo all’Arena’
geographical areas, located in the historical center of Naples and
representing the largest population governed by a single
municipality in Europe (3rd Municipality of Naples), with 49,235
men and 54,938 women (Fig. 1).
This Municipality corresponds with the Health Care District 29
(D29; 103,633 patients) in the ‘ASL Napoli 1 Centro’ (1,004,500
units) with a M/F ratio of 91.74/100, which is lower compared to
that in the rest of Italy (M/F 93.8/100; Censimento 2001,
www.comune.napoli.it).
Municipalities are the smallest administrative units
(8,100 in all of Italy) where demographic and mortality data are
routinely available. First, we examined the cancer prevalence in
the district (D29). The distribution of cancer according to patient
gender and tumour histotype was then analyzed. Prevalence was
defined as the number or proportion of individuals with a previous
diagnosis of cancer belonging to the specific population.
Tumours were divided according to ICD-IX and were
grouped as follows: gastrointestinal sites (tongue, mouth, pharynx,
oesophagus and stomach) ICD-IX 141–151; colon and rectum ICD-IX
153–154; liver, biliary system and pancreas ICD-IX 155-157; larynx
ICD-IX 161; lung ICD-IX 162; bone and soft tissue sarcomas ICD-IX
170-171; melanoma and skin ICD-IX 172–173; breast cancer ICD-IX
174-175; reproductive system ICD-IX 180-187; kidney and bladder
ICD-IX 188–189; thyroid gland ICD-IX 193; central nervous system
(CNS) ICD-IX 190–191; leukaemia and lymphomas (blood) ICD-IX
200–205 (Tables I and II).
 | Table I.Cancer prevalence in males and age
ranges. |
Table I.
Cancer prevalence in males and age
ranges.
| ICD-IX | Sites | Age (years)
| Range 65–74 | ≥75 | Total |
|---|
| 10–34 | 35–64 |
|---|
| 141 | Tongue | | | 2 | | 2 |
| 143–145 | Mouth | | | 1 | | 1 |
| 146–148 | Pharynx | | | 1 | 1 | 2 |
| 150 | Oesophagus | | | | 1 | 1 |
| 151 | Stomach | | 2 | 2 | 1 | 5 |
| 153 | Colon | | 3 | 9 | 3 | 15 |
| 154 | Rectum | | | 2 | 1 | 3 |
| 155 | Liver | | | 4 | 1 | 5 |
| 156 | Biliary system | | 1 | | | 1 |
| 157 | Pancreas | | | | 1 | 1 |
| 161 | Larynx | | 3 | 6 | 1 | 10 |
| 162 | Lung | | 5 | 7 | 2 | 14 |
| 170 | Bone | 1 | 1 | | | 2 |
| 171 | Soft tissue | | | | 1 | 1 |
| 172 | Melanoma | | 3 | 3 | 1 | 7 |
| 173 | Skin | | | 1 | | 1 |
| 185 | Prostate | | 2 | 15 | 13 | 30 |
| 186 | Testicle | 1 | 1 | | | 2 |
| 187 | Penis | | 1 | | | 1 |
| 188 | Bladder | | 7 | 4 | 6 | 17 |
| 189 | Kidney | | | 4 | 3 | 7 |
| 191 | CNS | | 1 | | | 1 |
| 193 | Thyroid | | 3 | | | 3 |
| 201 | HL | 2 | 1 | | | 3 |
| 200,202 | NHL | | 4 | | 1 | 5 |
| 202–205 | Leukaemia | 2 | 2 | 2 | 2 | 8 |
|
| All tumours
(%) | 6 (4) | 40 (27) | 63 (42.6) | 39 (26.4) | 148 |
| Table II.Cancer prevalence in females and age
ranges. |
Table II.
Cancer prevalence in females and age
ranges.
| ICD-IX | Sites | Age (years)
| Range 65–74 | ≥75 | Total |
|---|
| 10–34 | 35–64 |
|---|
| 141 | Tongue | | 1 | | | 1 |
| 143–145 | Mouth | | 2 | | | 2 |
| 146–148 | Pharynx | | 1 | | | 1 |
| 150 | Oesophagus | | | | 1 | 1 |
| 151 | Stomach | | | | | 0 |
| 153 | Colon | | 7 | 7 | 7 | 21 |
| 154 | Rectum | | | 2 | | 2 |
| 155 | Liver | | 1 | 1 | | 2 |
| 156 | Biliary system | | | 1 | | 1 |
| 157 | Pancreas | | | 3 | | 3 |
| 161 | Larynx | | | | | 0 |
| 162 | Lung | | 1 | | | 1 |
| 170 | Bone | 1 | | | | 1 |
| 171 | Soft tissue | | | | 1 | 1 |
| 172 | Melanoma | | 2 | | | 2 |
| 173 | Skin | | | 1 | 2 | 3 |
| 174 | Breast | 2 | 63 | 23 | 14 | 102 |
| 180 | Cervix | | 4 | | | 4 |
| 182 | Uterus | | 11 | 6 | 2 | 19 |
| 183 | Ovary | 1 | 1 | | | 2 |
| 184 | Vulva | | 1 | | | 1 |
| 188 | Bladder | | 1 | 1 | | 2 |
| 189 | Kidney | 1 | 2 | 1 | 2 | 6 |
| 191 | CNS | | 1 | 1 | 1 | 3 |
| 193 | Thyroid | 1 | 5 | 1 | | 7 |
| 201 | HL | 1 | | | | 1 |
| 200,202 | NHL | | 4 | 3 | | 7 |
| 203 | Myeloma | | | 1 | | 1 |
| 202–205 | Leukaemia | | 3 | | 4 | 7 |
|
| All tumours
(%) | 7 (3.4) | 111 (54.4) | 52 (25.5) | 34 (16.7) | 204 |
Results
The study was conducted on a total of 16,927
individuals (patients and healthy subjects) followed for primary
care by the 12 GPs belonging to the MEDI.CO cooperative Group who
agreed to participate in the study. All 12 GPs were employed in
Health Care District 29. The general population age ranged from 6
to 97 years. Of note, the population represented in this study
corresponds to 16.3% of the general population residing in the
geographical areas involved.
Patients with cancer represented 2% (342/16,927) of
the total population. Based on these data, the overall cancer
prevalence was estimated to be 2,020/100,000 inhabitants. Each GP
recruited in the study reported a cancer prevalence range of
1.1–3%.
We identified 342 patients with invasive cancer:
their median age was 65 years and ranged from 10 (leukaemia) to 93
(epithelioma) years. The majority of the cancer cases were recorded
among women (199 cases, 1.2%) compared to men (143 cases, 0.8%)
(M/F ratio, 0.7). Of the 342 cancer patients, 10 patients (5 men
and 5 women), were affected by more than one primary cancer; thus,
for the purpose of our analyses, a total of 352 malignant cancers
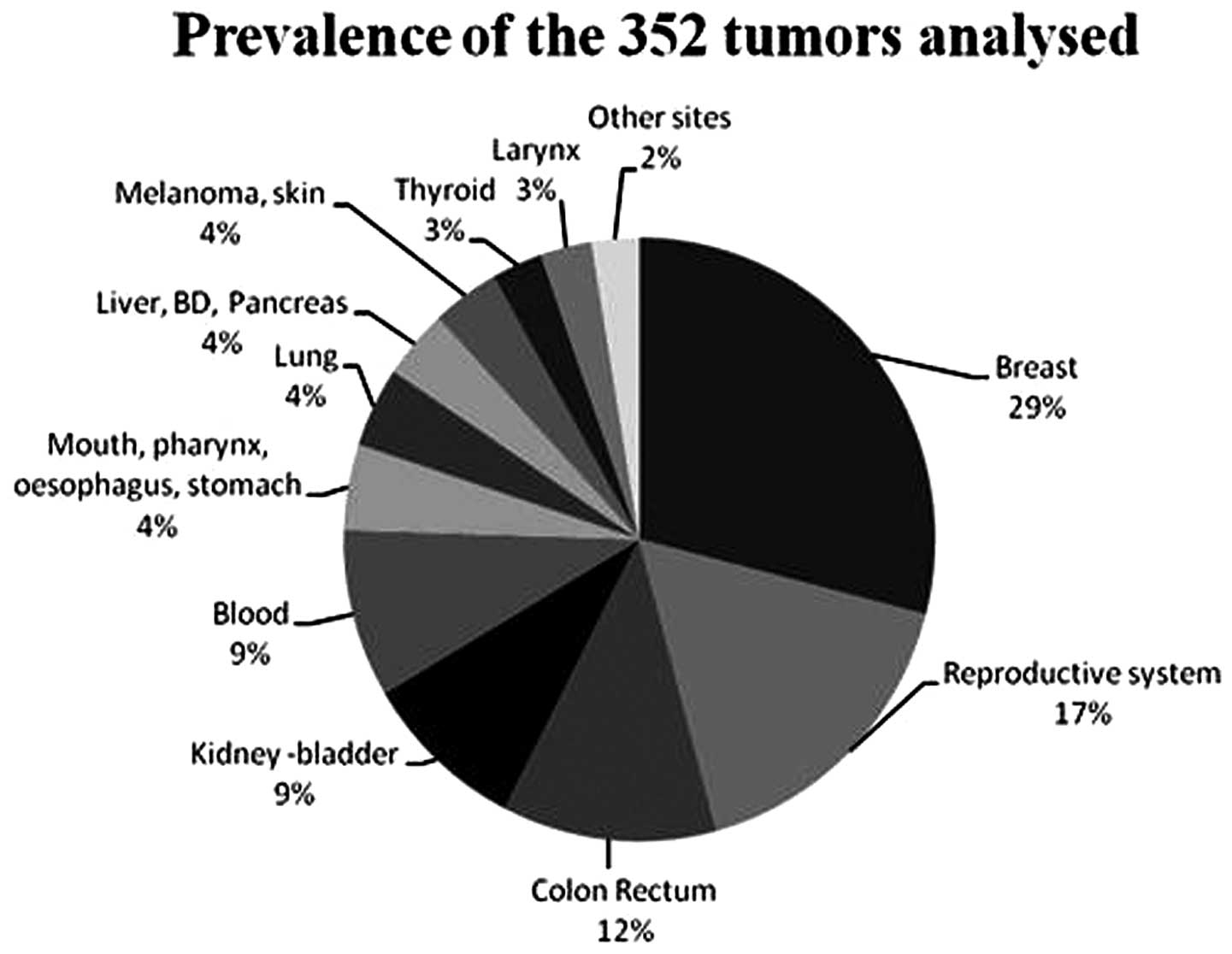
were considered. Fig. 2 shows the
distribution of cancer by primary site in the cancer
population.
Among all histotypes, breast cancer was the most
frequent (29%, 102/352) among affected patients. Cancers of the
reproductive system, i.e., cervix, uterus, ovary, vulva, prostate,
testicle and penis, were the second most prevalent group (17%,
59/352). Among these, prostatic cancer (30/352) in men and uterine
cancer (19/352) in women were the most frequent reproductive
histotypes. Among gastrointestinal (GI) cancers, colorectal cancer
represented 41/352 cases (12%), whereas upper GI tract histotypes
were recorded in only 4% (16/352) of the cases. Of note, kidney and
bladder cancer was identified in 32/352 cases, with a prevalence of
9%, identical to that of blood malignancies. All other histotypes
taken together did not exceed 4% of the cases. The most frequently
observed types of cancer were breast, urogenital and colorectal
cancers.
Results recorded regarding different histotypes and
ICD-IX were analyzed according to gender and age range of the
patients. Tables I and II show the prevalence of different cancer
types in males and females.
Among the 352 tumours, 148 cases were recorded in
males and most of these were observed in the age range of 65–74
years (42.6%, 63/148). Prostate cancer was the most frequent type
of tumour among males (20%, 30/148), followed by kidney and bladder
tumours (16%, 24/148), which exhibited a prevalence identical with
that of laryngeal and pulmonary tumours (16%, 24/148). Colorectal
cancer was also identified among males (12%, 18/148). Among the 352
tumours, 204 cases were recorded in females, predominantly in the
age range of 35–64 years (54.4%, 111/204). Breast cancer was the
most frequent type of tumour among females (50%, 102/204), followed
by colorectal (11%, 23/204) and uterine (9%, 19/204) cancers.
Fig. 3 shows the percentages of
prevalence distributed according to gender.
Discussion
The almost complete lack of tumour registries in
Southern Italy and, most importantly, in the Campania region, one
of the most crowded and polluted areas of the Italian peninsula,
makes the estimation of the annual rate of new cancer cases and
cancer prevalence in this district challenging (7,10,13–18).
Furthermore, the impact of legal or illegal landfills in rural and
urban areas of Campania, such as neighborhoods situated around
Naples or Caserta, on population health and, particularly, on the
risk of cancer development, may not be accurately determined due to
lack of epidemiological data in the entire region (10,14–19).
However, this issue is a major health concern for the population
residing in these areas and there is a pressing need for definitive
answers.
Over the last few years there has been an ongoing
effort, directed towards the creation of tumour registries that
cover the entire Campania area. At present, however, the only
available and reliable source of data on cancer incidence,
prevalence and mortality in Campania remains the tumour registry of
the local health service no. 4, also known as ‘Azienda Sanitaria
Locale’ Napoli 4 (ASL Napoli 4), that covers only a small part of
the entire Campania population (16). Data on cancer prevalence, incidence
and mortality in Campania, one of the most heavily populated
regions of Southern Italy, are sparse and fragmentary and focus
predominantly on detailed geographical areas near landfills or
single waste sites (10,14–23).
GPs in Italy are responsible for primary and
secondary cancer prevention and, more importantly, are the only
ones entitled to prescribe Day Hospital admission or patient
hospitalization for cancer treatment, provide medical exemption
certificates for cancer patients and prescribe medication for the
treatment of cancer or cancer-related symptoms. Therefore, GPs keep
reliable records on the number of cancer patients among their
patient population, as well as on diagnostic and therapeutic
methods. Several GPs practicing in the same district in Campania
and, to a certain extent, in the rest of Italy, operate in groups
called ‘service societies’. Several service societies have also
joined together in an organization called Consorzio Nazionale delle
Cooperative Mediche. This consortium currently comprises >500
GPs, assisting ∼844,297 patients in the entire region of Campania.
GPs belonging to this network record patient clinical information
in commonly shared software and participate in innovative research
protocols or clinical courses to improve their clinical skills and
patient information retrieval through electronic patient charts, in
order to ensure uniformity of data entry and extraction. At
present, there is an ongoing analysis on cancer prevalence and
incidence in the entirety of Campania.
In our study, the MEDI.CO service society serve the
suburbs of ‘Stella’ and ‘San Carlo all’Arena’, which are located in
the historical center of Naples. Of note, the patient population
registered with MEDI.CO GPs represents 16.3% of the general
population residing in these two geographical areas. Data from
clinical patient charts retrieved from GPs belonging to the MEDI.CO
society are therefore representative of the cancer prevalence and
incidence in the metropolitan area of Naples. Therefore, in the
present study we aimed to test the reliability of MEDI.CO GP
clinical databases in the assessment of cancer prevalence and
histotype distribution for the population residing in the ‘Stella’
and ‘San Carlo all’Arena’ (3rd Municipality of Naples) suburbs
registered with MEDI. CO practitioners.
Overall, cancer patients represented 2% (342/16,927)
of the entire population considered. For each GP recruited in the
study, the recorded cancer prevalence range was 1.1–3%. This is in
concordance with the previously reported cancer prevalence in the
Campania area according to indirect estimates from the ‘ASL Napoli
4’ tumour registry. In agreement with national data, in our dataset
females appeared to be more frequently affected by cancer compared
to males (10).
The most common cancer histotypes among men were
prostatic, bladder, colon, lung and laryngeal cancer and among
women breast, colon and uterine cancer. The prevalence of prostatic
cancer was higher among older men, whereas the prevalence of
bladder cancer was not significantly affected by age. Lung, colon
and laryngeal cancer in our dataset was more prevalent among
middle-aged men and breast cancer was the most prevalent histotype
among middle-aged women, followed by uterine cancer. There were no
differences according to age in the prevalence of colon cancer. The
overall cancer prevalence was slightly lower compared to that in
the general Italian population (2,683/100,000 inhabitants), but
higher compared to the prevalence previously reported in different
Southern Italian cities (7,8,10,12,13).
However, histotype distribution according to gender and age range
were in accordance with the expected rates estimated from data
obtained from tumori.net, the most accredited source of
epidemiological data for cancer disease (http://www.tumori.net/it/banca_dati/query.php)
and recent epidemiological national data (7–10).
The present study demonstrated that evaluating
cancer prevalence from GP patient charts is feasible,
cost-effective and reliable, provided that the patient population
included in the service society is representative of the total
population of the area registered with the GPs clinical practice.
Therefore, the width of the GP network is positively correlated
with the extent of data retrieval from a specific region and the
relative measures of cancer incidence and prevalence.
Currently, in Campania, epidemiological data on
cancer prevalence estimated from GP patient charts is the single
and most complete data source available. However, reviewing GP
patient charts is not a substitute for specific cancer registries,
which remain the most reliable source of epidemiological data for
cancer. Data on cancer patients obtained from GPs may corroborate
information collected from tumour registries and also provide
further insight on patient co-morbidities, types of treatment
performed and geographical distribution of hospitals and centers
specializing in cancer care. Careful interpretation of data
collected from GP databases is required, considering all potential
biases due to the non-homogeneous distribution of GP practices
among different areas of Campania and its largest cities. Further
development of the GP service society network is required, in order
to optimize data collection and retrieval and provide an almost
complete coverage of the whole Campania region and, in the future,
the entire Italian peninsula.
References
|
1.
|
Greenlee RT, Murray T, Bolden S and Wingo
PA: Cancer statistics, 2000. CA Cancer J Clin. 50:7–33. 2000.
View Article : Google Scholar
|
|
2.
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
statistics, 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar
|
|
3.
|
World Health Organization: Regional Office
for Europe: Population health and waste management: scientific data
and policy opinions. Report of a WHO workshop. Rome, Italy.
29–30–March. 2007
|
|
4.
|
Berrino F, Verdecchia A, Lutz JM, Lombardo
C, Micheli A and Capocaccia R; EUROCARE Working Group: Comparative
cancer survival information in Europe. Eur J Cancer. 45:901–908.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Lillini R, Vercelli M, Quaglia A, Micheli
A and Capocaccia R: Use of socio-economic factors and healthcare
resources to estimate cancer survival in European countries with
partial national cancer registration. Tumori. 97:265–274. 2011.
|
|
6.
|
Micheli A, Mugno E, Krogh V, et al
EUROPREVAL Working Group: Cancer prevalence in European registry
areas. Ann Oncol. 13:840–865. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Mariotto A, Dally LG, Micheli A, Canario F
and Verdecchia A: Cancer prevalence in Italian regions with local
cancer registries. Tumori. 85:400–407. 1999.PubMed/NCBI
|
|
8.
|
Micheli A, Francisci S, Krogh V, Rossi AG
and Crosignani P: Cancer prevalence in Italian cancer registry
areas: the ITAPREVAL study. ITAPREVAL Working Group. Tumori.
85:309–369. 1999.PubMed/NCBI
|
|
9.
|
De Angelis R, Grande E, Inghelmann R, et
al: Cancer prevalence estimates in Italy from 1970 to 2010. Tumori.
93:392–397. 2007.PubMed/NCBI
|
|
10.
|
AIRTUM Working Group: Italian cancer
figures, report 2010: cancer prevalence in Italy. Patients living
with cancer, long-term survivors and cured patients. Epidemiol
Prev. 34:1–188. 2010.PubMed/NCBI
|
|
11.
|
Crocetti E and Buzzoni C; AIRTUM Working
Group: Italy is one of the European countries with the greatest
population observed by cancer registries. Epidemiol Prev.
34:822010.PubMed/NCBI
|
|
12.
|
AIRTUM Working Group; Crocetti E and
Buzzoni C: New incidence and mortality data. 2003–2005. Epidemiol
Prev. 33:e1–e3. e5–e26. 2009.(In Italian).
|
|
13.
|
Grande E, Inghelmann R, Francisci S, et
al: Regional estimates of all cancer malignancies in Italy. Tumori.
93:345–351. 2007.PubMed/NCBI
|
|
14.
|
Fazzo L, Belli S, Minichilli F, et al
Working Group: Cluster analysis of mortality and malformations in
the provinces of Naples and Caserta (Campania Region). Ann Ist
Super Sanita. 44:99–111. 2008.PubMed/NCBI
|
|
15.
|
Martuzzi M, Mitis F, Bianchi F, Minichilli
F, Comba P and Fazzo L: Cancer mortality and congenital anomalies
in a region of Italy with intense environmental pressure due to
waste. Occup Environ Med. 66:725–732. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Fazzo L, De Santis M, Mitis F, Benedetti
M, Martuzzi M, Comba P and Fusco M: Ecological studies of cancer
incidence in an area interested by dumping waste sites in Campania
(Italy). Ann Ist Super Sanita. 47:181–191. 2011.PubMed/NCBI
|
|
17.
|
Altavista P, Belli S, Bianchi F, et al:
Cause-specific mortality in an area of Campania with numerous waste
disposal sites. Epidemiol Prev. 28:311–321. 2004.PubMed/NCBI
|
|
18.
|
Barba M, Mazza A, Guerriero C, et al:
Wasting lives: the effects of toxic waste exposure on health. The
case of Campania, Southern Italy. Cancer Biol Ther. 12:106–111.
2011. View Article : Google Scholar
|
|
19.
|
Guerriero C and Cairns J: The potential
monetary benefits of reclaiming hazardous waste sites in the
Campania region: an economic evaluation. Environ Health. 8:282009.
View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Bidoli E, Franceschi S and Montella M:
Cancer mortality by urbanization and proximity to the sea coast in
Campania Region, southern Italy. Tumori. 84:460–466.
1998.PubMed/NCBI
|
|
21.
|
Picone GM, Pizzi C, Quartuccio A,
Scognamiglio G, et al: Incidence and pathological characteristics
of prostate cancer in Italy: a contribution to the screening
debate. Cancer Detect Prev. 30:455–458. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Riccardi F, Nappi O, Balzano A, et al:
Neuroendocrine tumors diagnosed at the Antonio Cardarelli hospital
(Naples, Italy) between 2006–2009: a single-institution analysis.
Int J Immunopathol Pharmacol. 24:251–256. 2011.PubMed/NCBI
|
|
23.
|
Fusco M, Pezzi A, Benatti P, et al:
Clinical features and colorectal cancer survival: an attempt to
explain differences between two different Italian regions. Eur J
Cancer. 46:142–149. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Pizzi C, Acampora G, Aiello N, De Rosa A,
et al: Cancer prevalence in Naples: analysis in a general
practitioners network. Ann Oncol. 16(Suppl 7): H362005.
|