Introduction
Viruses and tumors evade cytotoxic T
lymphocyte-mediated host immunity through the downregulation of
antigen-presentation machineries. This may be achieved by either
the downregulation of transcription of antigen presentation genes,
or the post-translational inactivation of the proteins involved in
antigen presentation (1). The
optimal cell surface expression of human leukocyte antigen (HLA)
molecules requires the coordinated expression of several genes,
such as transporters associated with antigen processing (TAP)-1 and
-2, low molecular weight peptide (LMP)-2 and -7 and tapasin, as
well as HLA class I heavy chain and β2-microglobulin
(β2M). In cases of concurrent tumorigenesis and viral
infection, the expression of these genes and the function of the
encoded proteins are often impaired.
Latent Epstein-Barr virus (EBV) infections are
associated with lymphocyte and epithelial cell malignancies, with
nasopharyngeal carcinoma (NPC) being the most frequent
EBV-associated malignancy (2). The
EBV-associated, undifferentiated form of NPC exhibits the most
consistent association with EBV worldwide and is particularly
common in China and Southeast Asia, reaching a peak incidence of
∼20–30 cases per 100,000 individuals (3). In addition to genetic predisposition,
EBV infection and environmental factors, such as dietary and
geographic components, were considered to be important in the
aetiology of NPC (4–6). Previous studies that used
quantitative polymerase chain reaction to measure circulating
tumor-derived EBV DNA in the blood of NPC patients demonstrated
that the level of pre-treatment EBV DNA was significantly
associated with overall survival and that post-treatment EBV DNA
levels predicted progression-free and overall survival (7,8).
Previous studies on normal nasopharyngeal tissue and premalignant
biopsies indicated that genetic events occur early in the
pathogenesis of NPC and they may predispose to subsequent EBV
infection. The EBV latent-gene expression in NPC is predominantly
restricted to the Epstein-Barr nuclear antigen 1, the latent
membrane proteins (LMP) 2A and 2B and the BamHI-A transcripts, with
approximately 70% of the tumors also expressing the oncogenic LMP1
protein (9–11).
Currently, research is focused on the mechanisms
underlying the escape of NPC from EBV-specific immune destruction
and the development of novel strategies for immune intervention.
BamHI-C fragment rightward reading frame 1 (BCRF-1) that is located
in the EBV gene, is able to produce viral interleukin-10 (vIL-10),
which is the homologue of the human IL-10 (hIL-10). In EBV-infected
B lymphocytes, vIL-10 and hIL-10 are equally capable of
downregulating TAP-1 expression, thereby interfering with the
loading of major histocompatibility complex (MHC) class I
molecules, resulting in empty and unstable MHC class
I/β2M complexes. The BCRF-1 gene and the vIL-10 protein
are highly expressed in NPC tissues (data not shown); therefore, we
aimed to assess whether the expression of TAP-1, TAP-2 and HLA-I
are affected in NPC and investigate whether these proteins may be
prognostic factors for NPC.
Materials and methods
Case specimens
A total of 78 paraffin specimens (biopsy specimens
obtained during surgery) from 58 patients and 20 healthy controls
were collected from the Pathology Department of The Third
Affiliated Hospital of Kunmming Medical University, between 2000
and 2002. The characteristics of the 58 patients are summarized in
Table I. The control group
comprised 20 healthy individuals who were examined at the hospital
and NPC was excluded by pathological examination.
Immunohistochemistry confirmed that all the specimens were
collected prior to medical treatment. Peripheral blood (2 ml) was
collected from each patient in heparin tubes. Approval for this
study was granted by the Ethics Committee of The Third Affiliated
Hospital of Kunming Medical University. The patients provided their
permission for the collection of the specimens. The NPC patients
received medical treatment according to the NCCN Practice
Guidelines for Head and Neck Cancer following pathological
diagnosis. All the patients were followed up after treatment.
 | Table I.Characteristics of study population in
NPC (n=58). |
Table I.
Characteristics of study population in
NPC (n=58).
| Case | No. (%) |
|---|
| Gender | |
| Male | 38 (65.5) |
| Female | 20 (34.5) |
| Age (years) | |
| Mean (range) | 49.23 (14–84) |
| Clinical stage | |
| I | 4 (6.9) |
| II | 18 (31.0) |
| III | 10 (17.3) |
| IV | 26 (44.8) |
| Histological
differentiation | |
| High or
moderate | 5 (8.6) |
| Poor | 53 (91.4) |
| Lymph node
metastasis | |
|
N0 | 17 (29.3) |
|
N1–3 | 41 (70.7) |
| Distant
metastasis | |
|
M0 | 48 (82.8) |
|
M1 | 10 (17.2) |
Immunohistochemistry
Rabbit polyclonal anti-TAP-1 antibody (1:100
dilution; Santa Cruz Biotechnology Inc., Santa Cruz, CA, USA),
rabbit monoclonal anti-HLA-I antibody (1:250 dilution; Epitomics
Inc., Burlingame, CA, USA) and rabbit polyclonal anti-TAP-2
antibody (1:100 dilution; Abcam, Hong Kong, China) were used in
this study. Specimens used as the positive contrast were purchased
from Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd.
(Beijing, China) and phosphate-buffered saline (PBS) was used for
negative contrast. Tumor sections (4 μm) were deparaffinised
and heated in a microwave oven for 10 min for antigen repair. After
cooling, the slides were submerged in a peroxidase quenching
solution containing 1 part of 30% hydrogen peroxide to 9 parts of
absolute methanol for 10 min and were then washed with PBS.
Subsequently, 10% serum was added to each section, followed by
incubation for 20 min and draining. The sections were incubated
with the primary antibodies overnight in a 4°C chamber, then rinsed
with PBS. After rinsing, the sections were treated with
biotin-conjugated antibody for 10 min followed by washing with PBS.
Horseradish peroxidase polymer conjugate was applied to each
section and incubated for 10 min, followed by washing with PBS.
Finally, 3,3’-diaminobenzidine was applied to each section and
incubated for 10 min. The samples were rinsed thoroughly with
distilled water. Subsequently, the slides were counterstained with
hematoxylin, dehydrated and sealed with neutral gum.
The staining of the cores was scored based on signal
intensity (0–3) and the percentage of positive cells (0, <5%; 1,
5–10%; 2, 11–50%; 3, 51%–80%; and 4≥50%) (12). The results defined as positive were
scored based on the product of the two data as follows: 0, negative
(−); 1–4, weak positive (+); 5–8, medium positive (++); and 9–12,
strong positive (+++).
Flow cytometry (FCM)
The collected peripheral blood cells were
immunostained with fluorochrome-conjugated anti-human antibodies
(FITC-conjugated anti-human CD4, PE-conjugated anti-human CD4 and
PC5-conjugated anti-human CD45; Beckman Coulter Inc., Brea, CA,
USA) for 25 min at 4°C. The peripheral blood was dissolved using
Q-prep autohemolysis equipment. The samples were analyzed with a
flow cytometer (EPICS-XL; Beckman Coulter Inc.). The frequency of
CD4+ T cells (CD4-FITC/CD45-PC5) and CD8+ T
cells (CD8-PE/CD45-PC5) among the lymphocytes of different subsets
was calculated, with IgG-FITC/CD45-PC5 and IgG-PE/CD45-PC5 as the
negative controls. Data was analyzed with Expo32 software.
Measurement of IL-10 by enzyme-linked
immunosorbent assay (ELISA)
The blood samples were centrifuged at 3,000 rpm (825
× g) for 25 min. The supernatant was collected, aliquoted and
stored at −80°C until use. The concentrations of IL-10 were
measured using commercial ELISA kits (Biosource International Inc.,
Boshide Company, Wuhan, China), according to the manufacturer’s
instructions.
Statistical analysis
Data were analyzed using SPSS software, version 12.0
(SPSS Inc., Chicago, IL, USA). The correlation of TAP-1, TAP-2 and
HLA-I expression with the clinicopathological variables was
performed with the Chi-square test. The expression of
CD4+ T cells, CD8+ T cells and IL-10 in the
different groups was assessed with the independent-samples t-test.
Survival was assessed with the Kaplan-Meier analysis and the
log-rank score was used for determining statistical significance.
The relative risk was assessed with the multivariate Cox
proportional hazards model. P<0.05 was considered to indicate a
statistically significant difference.
Results
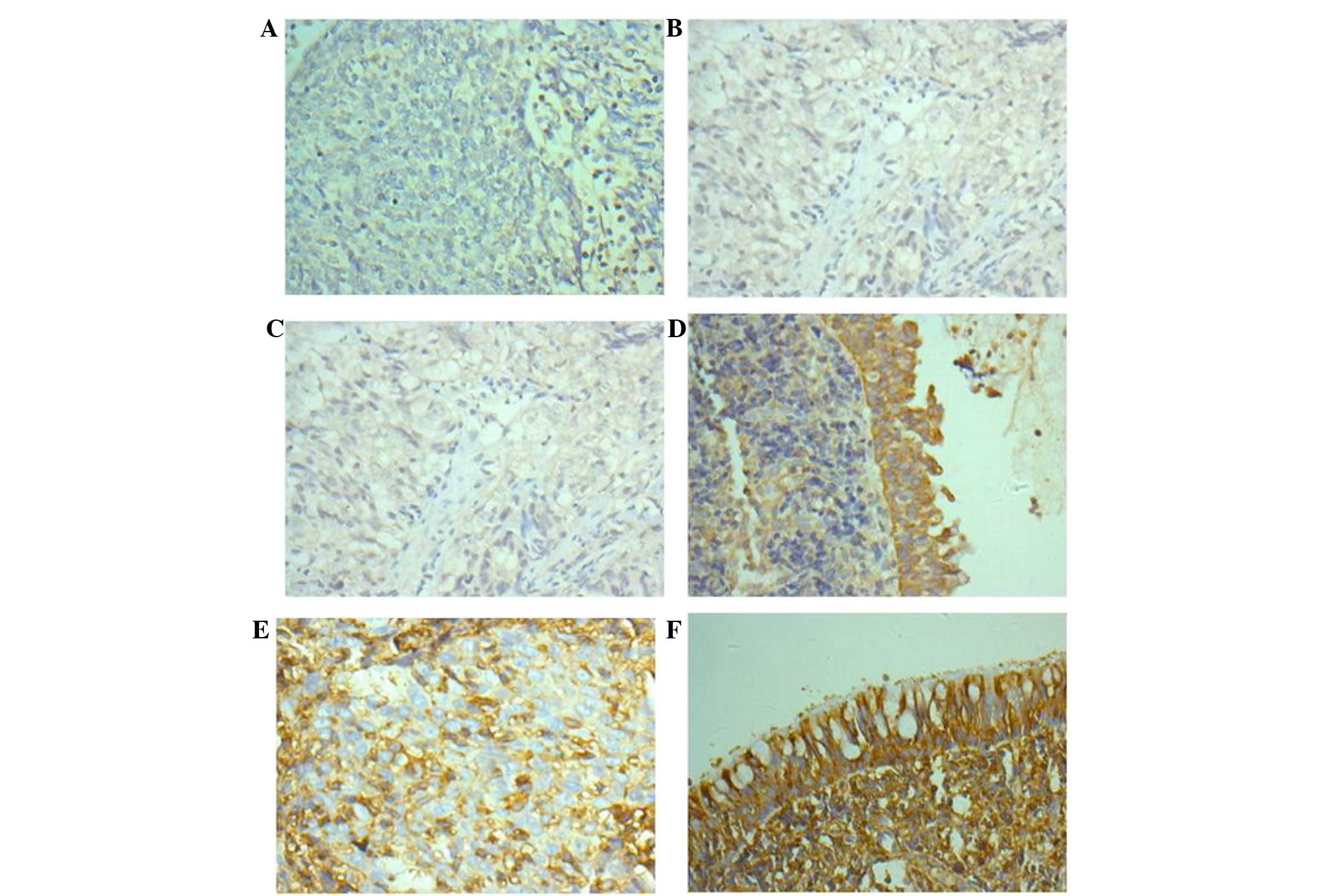
Low TAP-1, TAP-2 and HLA-I expression in
NPC tissue
In NPC, the TAP-1 and TAP-2 immunoreactivity
displayed weak diffuse cytoplasmic staining, whereas HLA-I
displayed weak diffuse cytoplasmic and cytomembranous staining
(Fig. 1A, C and E). By contrast,
normal nasopharyngeal tissues exhibited intense staining for these
proteins (Fig. 1B, D and F). A
total of 25, 27 and 29 of the 58 NPC samples exhibited low
expression of TAP-1, TAP-2 and HLA-I, respectively, whereas 18, 19
and 19 of the 20 normal nasopharyngeal tissue samples exhibited
high expression of TAP-1, TAP-2 and HLA-I, respectively. Therefore,
the expression of TAP-1, TAP-2 and HLA-I in the NPC samples was
distinctly lower compared to that in the normal nasopharyngeal
tissue samples (P<0.05, Table
II).
| Table II.Expression of TAP-1, TAP-2 and HLA-I
in the NPC and the control group. |
Table II.
Expression of TAP-1, TAP-2 and HLA-I
in the NPC and the control group.
| Group | No. | TAP-1 | P-value | TAP-2 | P-value | HLA-I | P-value |
|---|
|
|
|
|---|
| − | + | − | + | − | + |
|---|
| Chronic
inflammation | 20 | 2 | 18 | <0.001 | 1 | 19 | <0.001 | 1 | 19 | <0.001 |
| NPC | 58 | 33 | 25 | | 31 | 27 | | 29 | 29 | |
Changes in CD4+ T cells,
CD8+ T cells and IL-10 in the peripheral blood of NPC
patients
FCM was applied to detect CD4+ T cells,
CD8+ T cells and IL-10 was analyzed by ELISA. The
percentage of CD4+ T cells in the peripheral blood of
NPC patients was 33.41±10.04% (Fig.
2A), which was lower compared to that of the normal subjects,
which was 40.15±3.56% (Fig. 2B)
(P<0.05, Fig. 2E). There was no
significant difference between the NPC and control groups regarding
CD8+ T cells (25.32±8.29 vs. 22.89±2.24%, P>0.05,
Fig. 2C, D and E). The ELISA
results indicated that the expression of IL-10 in NPC was higher
compared to that in the control group (13.12±1.23 vs. 3.69±1.03
ng/ml, respectively; P<0.05, Fig.
2E).
Association between TAP-1, TAP-2 and
HLA-I status and clinical variables
As shown in Table
III, the low expression of TAP-1, TAP-2 and HLA-1 was
significantly associated with TNM stage, lymph node metastasis and
distant metastasis (P<0.05). No association was observed between
their expression with age and gender (P>0.05).
| Table III.Association of TAP-1, TAP-2 and HLA-I
expression with clinical factors in NPC. |
Table III.
Association of TAP-1, TAP-2 and HLA-I
expression with clinical factors in NPC.
| TAP-1 | P-value | TAP-2 | P-value | HLA-I | P-value |
|---|
|
|
|
|---|
| Positive no.
(%) | Negative no.
(%) | Positive no.
(%) | Negative no.
(%) | Positive no.
(%) | Negative no.
(%) |
|---|
| Age (years) | | | | | | | | | |
| ≤43 | 12 (48) | 16 (48.5) | 1.00 | 15 (55.5) | 13 (41.9) | 0.43 | 10 (34.5) | 18 (62.1) | 0.065 |
| >43 | 13 (52) | 17 (51.5) | | 12 (44.4) | 18 (58.1) | | 19 (65.5) | 11 (37.9) | |
| Gender | | | | | | | | | |
| Male | 17 (68) | 21 (63.6) | 0.786 | 16 (59.3) | 22 (71) | 0.413 | 20 (69) | 18 (62.1) | 0.783 |
| Female | 8 (32) | 12 (36.4) | | 11 (40.7) | 9 (29) | | 9 (31) | 11 (37.9) | |
| Clinical stage | | | | | | | | | |
| I+II | 13 (52) | 7 (21.2) | 0.015 | 15 (55.6) | 5 (16.1) | 0.002 | 15 (51.7) | 5 (17.2) | 0.012 |
| III+IV | 12 (48) | 26 (78.8) | | 12 (44.4) | 26 (83.9) | | 14 (48.3) | 24 (82.8) | |
| Lymph node
metastasis | | | | | | | | | |
| Yes | 11 (44) | 30 (90.9) | 0.00 | 12 (44.4) | 29 (93.5) | 0.00 | 13 (44.8) | 28 (96.6) | 0.00 |
| No | 14 (56) | 3 (9.1) | | 15 (55.6) | 2 (6.5) | | 16 (55.2) | 1 (3.4) | |
| Distant
metastasis | | | | | | | | | |
| Yes | 1 (4) | 9 (27.3) | 0.033 | 1 (3.7) | 9 (29) | 0.014 | 0 (0) | 10 (35.7) | 0.00 |
| No | 24 (96) | 24 (72.7) | | 26 (96.3) | 22 (71) | | 29 (100) | 19 (64.3) | |
Correlations of TAP-1, TAP-2 and HLA-I
expression with CD4+ T cells, CD8+ T cells
and IL-10
In order to elucidate whether TAP-1, TAP-2 and HLA-I
expression affected CD4+ T cells, CD8+ T
cells and IL-10, we divided the 58 NPC patients into TAP-1-positive
and -negative groups, TAP-2-positive and -negative groups and
HLA-I-positive and -negative groups and then assessed the
proportion of CD4+ T and CD8+ T cells and the
expression of IL-10 in the subgroups. As shown in Table IV, there was no significant
difference between the positive and negative subgroups regarding
the expression of CD4+ T cells (33.19±9.2 vs.
33.35±8.05%; 33.58±6.4 vs. 32.52±5.2%; and 34.34±6.58 vs.
30.22±3.49%, respectively; P>0.05). The percentage of
CD8+ T cells was higher in the positive compared to the
negative TAP-1, TAP-2 and HLA-I groups (27.93±4.04 vs. 18.43±2.37%;
28.47±3.62 vs. 19.18±2.11%; and 31.35±4.72 vs. 16.65±2.07%,
respectively; P<0.05). The expression of IL-10 was lower in the
positive compared to the negative TAP-1, TAP-2 and HLA-I groups
(9.87±1.24 vs. 16.20±1.48 ng/ml; 8.93±0.56 vs. 16.04±1.75 ng/ml;
and 6.28±0.86 vs. 17.99±2.01 ng/ml, respectively; P<0.05).
| Table IV.Analysis of CD4+ T cells,
CD8+ T cells and IL-10 expression in different TAP-1, -2
and HLA-I expression groups in NPC. |
Table IV.
Analysis of CD4+ T cells,
CD8+ T cells and IL-10 expression in different TAP-1, -2
and HLA-I expression groups in NPC.
| TAP-1 | P-value | TAP-2 | P-value | HLA-I | P-value |
|---|
|
|
|
|---|
| Positive | Negative | Positive | Negative | Positive | Negative |
|---|
| CD4+ T
cell (%) | 33.19±9.20 | 33.35±8.05 | 0.970 | 33.58±6.40 | 32.52±5.20 | 0.815 | 34.34±6.58 | 30.22±3.49 | 0.379 |
| CD8+ T
cell (%) | 27.93±4.04 | 18.43±2.37 | 0.013 | 28.47±3.62 | 19.18±2.11 | 0.018 | 31.35±4.72 | 16.65±2.07 | 0.005 |
| IL-10 (ng/ml) | 9.87±1.24 | 16.20±1.48 | 0.021 | 8.93±0.56 | 16.04±1.75 | 0.015 | 6.28±0.86 | 17.99±2.01 | 0.008 |
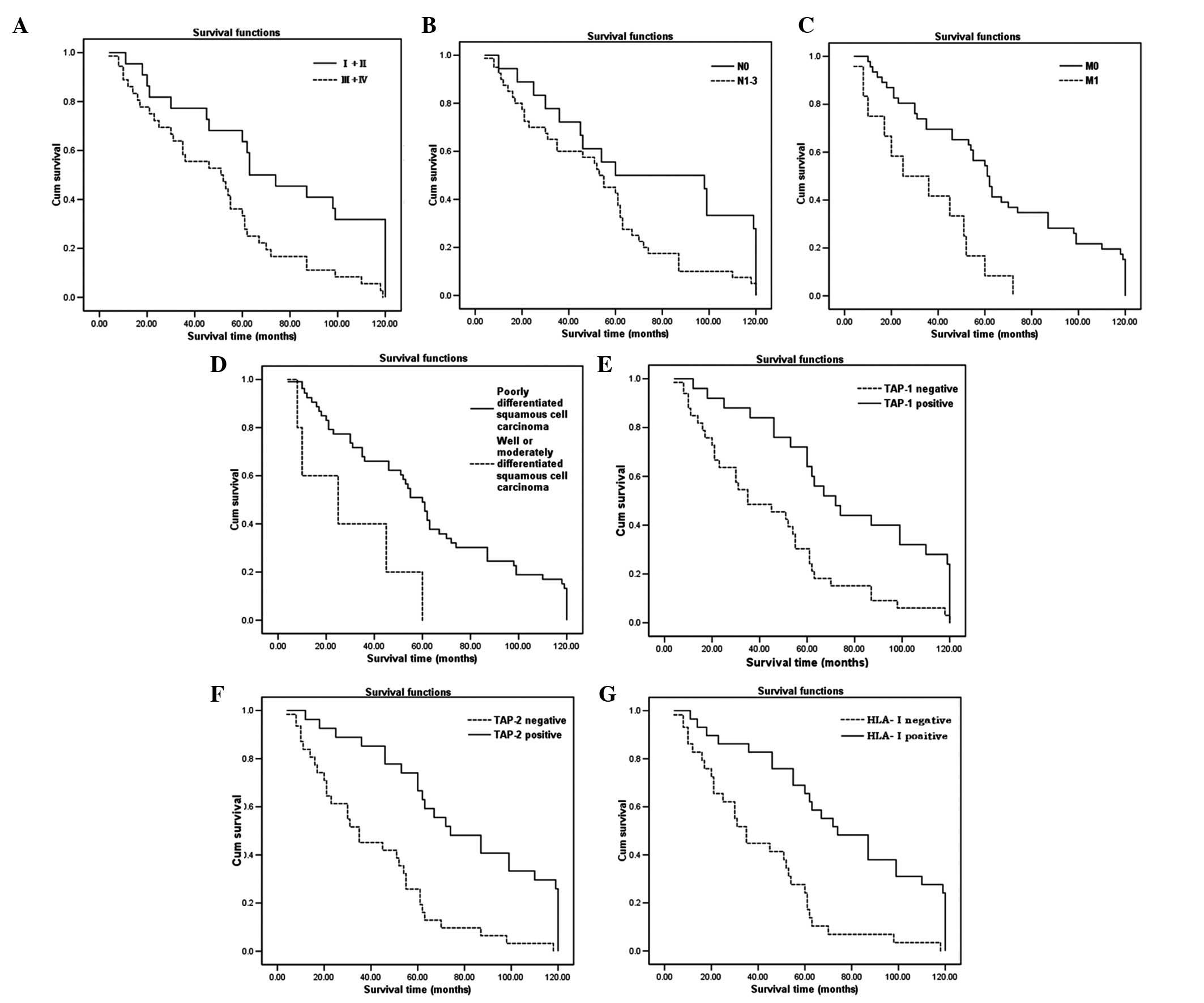
Follow-up and univariate survival
analysis
A total of 58 patients received standard treatment
and were regularly followed up. The Kaplan-Meier analysis was used
to analyze single factors considered to affect disease progression
including age, gender, TNM stage, lymph node metastasis or lack
thereof, distant organ metastasis or lack thereof, pathological
type, TAP-1 expression, TAP-2 expression and HLA-I expression. We
observed that clinical stage, lymph node metastasis, distant organ
metastasis, histological differentiation, TAP-1 expression, TAP-2
expression and HLA-I expression exerted a significant effect on the
overall survival of NPC patients (Fig.
3 and Table V, P<0.05).
| Table V.Univariate survival analysis in
patients with NPC. |
Table V.
Univariate survival analysis in
patients with NPC.
| Factor | No. | 3-year survival
rate (%) | 5-year survival
rate (%) | Log-rank value | P-value |
|---|
| Age (years) | | | | | |
| ≤43 | 38 | 68.42 | 47.37 | 1.63 | 0.202 |
| >43 | 20 | 60.00 | 40.00 | | |
| Gender | | | | | |
| Male | 38 | 79.50 | 65.00 | 0.26 | 0.610 |
| Female | 20 | 71.05 | 44.74 | | |
| Clinical stage | | | | | |
| I+II | 22 | 77.27 | 56.25 | 10.14 | 0.001 |
| III+IV | 36 | 55.56 | 38.89 | | |
| N stage | | | | | |
|
N0 | 17 | 76.47 | 47.06 | 5.36 | 0.021 |
|
N1-3 | 41 | 58.54 | 43.90 | | |
| M stage | | | | | |
|
M0 | 48 | 69.57 | 54.35 | 6.77 | 0.009 |
|
M1 | 10 | 41.67 | 8.33 | | |
| Histological
differentiation | | | | | |
|
High/moderate | 5 | 36.00 | 0 | 6.02 | 0.014 |
| Poor | 53 | 67.92 | 49.06 | | |
| TAP-1
expression | | | | | |
| Positive | 25 | 80.00 | 60.00 | 11.77 | 0.001 |
| Negative | 33 | 51.52 | 33.33 | | |
| TAP-2
expression | | | | | |
| Positive | 27 | 81.48 | 62.96 | 19.38 | 0.000 |
| Negative | 31 | 48.39 | 29.03 | | |
| HLA-I
expression | | | | | |
| Positive | 29 | 82.76 | 65.52 | 18.90 | 0.000 |
| Negative | 29 | 44.83 | 24.14 | | |
Multivariate survival analysis
Since the factors mentioned above were shown to
exert a significant effect on the survival of NPC patients, a
multivariate analysis was performed to assess the independent
predictive value of each of these factors for overall survival. Of
note, distant metastasis and HLA-I expression status were shown to
be potential independent prognostic factors for NPC patients
(P=0.041 and P=0.042, respectively, Table VI).
| Table VI.Multivariate Cox regression
analysis. |
Table VI.
Multivariate Cox regression
analysis.
| Variable | Wald | OR | 95.0% CI | P-value |
|---|
| Age | 0.595 | 1.290 | 0.675–2.465 | 0.440 |
| Gender | 0.014 | 1.037 | 0.570–1.886 | 0.904 |
| TNM stage | 0.004 | 0.952 | 0.220–4.128 | 0.948 |
| Lymph node
metastasis | 0.112 | 1.155 | 0.497–2.687 | 0.737 |
| Distant
metastasis | 4.598 | 2.609 | 0.971–5.974 | 0.041 |
| Histological
differentiation | 0.016 | 0.922 | 0.262–3.242 | 0.899 |
| TAP-1
expression | 0.005 | 1.071 | 0.168–6.819 | 0.942 |
| TAP-2
expression | 0.412 | 1.925 | 0.260–14.250 | 0.521 |
| HLA-I
expression | 4.557 | 2.586 | 0.389–8.186 | 0.042 |
Discussion
During the tumor immune response process, the MHC
class I molecules (mainly HLA-I) play a crucial role in the
elimination of virally infected and transformed cells by cytotoxic
T cells (CTLs). The CTLs recognize virally infected or malignant T
cells by foreign peptides presented on the cell surface in
association with class I antigens. The HLA-I antigen processing and
presentation pathway starts with proteins being degraded by the
proteasome, which consists of multiple catalytic subunits (mainly
LMP-2 and -7). The peptides are then translocated across the
endoplasmic reticulum (ER) membrane via the antigen-processing
subunits TAP-1 and -2. The HLA-I heavy chain is synthesized in the
ER, where it forms a complex with β2M. The
HLA-I/β2M complex then interacts with TAP-associated
peptides and facilitates peptide loading into
HLA-I/β2M/peptide complexes, which are transported to
the surface.
TAP plays a pivotal role in the peptide loading of
the HLA-I molecules and is therefore essential for their expression
on the cell surface. Thus, the transport of the HLA-I complexes to
the cell surface may be prevented if TAP is malfunctioning, leading
to antigen not being recognized by CTLs and escaping the immune
supervision (13–15). The absence of TAP-1, LMP-2, LMP-7
and HLA-I have been reported to occur in small-cell lung carcinoma
(16), colorectal cancer, breast
cancer (17), malignant melanoma,
malignant tumors of the head and neck (18) and malignant brain tumors (19) and may represent a mechanism of
tumor escape from the control of the immune system. An increase in
the expression of LMP-2, LMP-7 and HLA-I may be induced if TAP
transfection is performed.
In our study, the expression of TAP-1, TAP-2 and
HLA-I in NPC were distinctly reduced. In the peripheral blood of
NPC patients, the expression of IL-10, which has immunosuppressive
function, was increased and the percentage of CD4+ T
cells, which help B lymphocytes secrete antibodies, was decreased.
The percentage of the CD8+ T cells, which are crucial in
eliminating the infected or malignant T cells had no detectable
change. However, we observed that the percentage of CD8+
T cells exhibited a consistently positive correlation with the
expression of TAP-1, TAP-2 and HLA-I, whereas the expression of
IL-10 had a negative correlation with the expression of TAP-1,
TAP-2 and HLA-I in NPC. These results suggest that the reduction in
the expression of TAP-1, TAP-2 and HLA-I may contribute to the
immunosuppression associated with in NPC, which may help tumor
cells escape immune surveillance (20).
An association between the downregulation of TAP-1,
TAP-2 and HLA-I expression and cancer prognosis has been reported
in a wide range of malignancies (21–24).
The correlation between TAP-1, TAP-2 and HLA-I and prognosis in NPC
has been investigated (25). Our
data demonstrated that the downregulation of the expression of
TAP-1, TAP-2 and HLA-I became more prominent in more advanced
clinical stages. The Cox regression model indicated that HLA-I
expression and distant metastasis were independent prognostic
factors. Distant metastasis was the major cause of mortality in
patients with NPC, even following successful locoregional control
with radiotherapy or/and chemotherapy. According to a previous
study, ∼11–36% of NPC patients with controlled locoregional disease
will develop distant metastasis (26). Distant metastasis was shown to be a
negative prognostic factor in the present study, although the
difference was not considered statistically significant (P= 0.041).
Several factors may have affected the results: i) distant
metastasis may not have been diagnosed by pathological examination.
It has been suggested that
18F-fluorodeoxyglucose-positron emission
tomography/computed tomography is the most sensitive, specific and
accurate modality for distant metastasis staging of NPC; ii)
gender, pretreatment quality of life variables, treatment,
metastatic spread to different organs and short-term treatment
response may affect the prognosis of NPC with distant metastasis
(27,28); iii) an increase in the follow-up of
NPC cases is required. Of note, the expression of HLA-I, but not
that of TAP-1 and/or TAP-2, was an independent prognostic factor in
NPC. The HLA-I molecules play a central role in antigen submission,
during which TAP molecules are involved in antigen transport and
the antigen/HLA assembly. Thus, the downregulation of HLA-I
expression correlates in part with the decrease in the TAPs
(12). This study suggested that
the down-regulation of HLA-I expression was particularly associated
with a poor prognosis in NPC patients. Due to the limited patient
sample, it could not be determined whether this constitutes a
biological property or is due to the limited data availability.
In conclusion, we demonstrated that the expression
of TAP-1, TAP-2 and HLA-I were downregulated in NPC and this
downregulation may contribute to immunosuppression in NPC patients.
Of note, distant metastasis and HLA-I expression may be considered
as independent prognostic factors in NPC. Further studies are
required to elucidate the molecular mechanisms through which TAP-1,
TAP-2 and HLA-I expression affect immunity and investigate the
possibility of designing a biological treatment that will enhance
HLA-I molecule expression in NPC patients.
Acknowledgements
We would like to thank the patients
and healthy donors for participating in this study. This study was
supported in part by grants from the National Natural Science
Foundation of China (no. 81260312), the Research Project Foundation
of Health Science and Technology of Yunnan Province (no.
2011WS0068), the Technological Plan of Society Development of
Yunnan Province (Fundamental Research Program) (no. 2009ZC119M) and
the Technological Plan of Society Development of Yunnan Province
(Key Fundamental Research Program) (no. 2009CC026).
References
|
1.
|
Yang T, McNally BA, Ferrone S, Liu Y and
Zheng P: A single-nucleotide deletion leads to rapid degradation of
TAP-1 mRNA in a melanoma cell line. J Biol Chem. 278:15291–15296.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Vujanovic L, Whiteside TL, Potter DM, Chu
J, Ferrone S and Butterfield LH: Regulation of antigen presentation
machinery in human dendritic cells by recombinant adenovirus.
Cancer Immunol Immunother. 58:121–133. 2009. View Article : Google Scholar
|
|
3.
|
Young LS and Rickinson AB: Epstein-Barr
virus: 40 years on. Nat Rev Cancer. 4:757–768. 2004.
|
|
4.
|
Gallicchio L, Matanoski G, Tao XG, et al:
Adulthood consumption of preserved and nonpreserved vegetables and
the risk of nasopharyngeal carcinoma: a systematic review. Int J
Cancer. 119:1125–1135. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Bei JX, Jia WH and Zeng YX: Familial and
large-scale case-control studies identify genes associated with
nasopharyngeal carcinoma. Semin Cancer Biol. 22:96–106. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Jia WH and Qin HD: Non-viral environmental
risk factors for nasopharyngeal carcinoma: a systematic review.
Semin Cancer Biol. 22:117–126. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Shao JY, Zhang Y, Li YH, et al: Comparison
of Epstein-Barr virus DNA level in plasma, peripheral blood cell
and tumor tissue in nasopharyngeal carcinoma. Anticancer Res.
24:4059–4066. 2004.
|
|
8.
|
Chan AT, Lo YM, Zee B, et al: Plasma
Epstein-Barr virus DNA and residual disease after radiotherapy for
undifferentiated nasopharyngeal carcinoma. J Natl Cancer Inst.
94:1614–1619. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Bar-Sela G, Kuten A, Minkov I, Gov-Ari E
and Ben-Izhak O: Prevalence and relevance of EBV latency in
nasopharyngeal carcinoma in Israel. J Clin Pathol. 57:290–293.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Raab-Traub N: Epstein-Barr virus in the
pathogenesis of NPC. Semin Cancer Biol. 12:431–441. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Horikawa T, Yoshizaki T, Kondo S, Furukawa
M, Kaizaki Y and Pagano JS: Epstein-Barr virus latent membrane
protein 1 induces Snail and epithelial-mesenchymal transition in
metastatic nasopharyngeal carcinoma. Br J Cancer. 104:1160–1167.
2011. View Article : Google Scholar
|
|
12.
|
Li W, Deng XM, Wang CX, et al:
Down-regulation of HLA class I antigen in human papillomavirus type
16 E7 expressing HaCaT cells: correlate with TAP-1 expression. Int
J Gynecol Cancer. 20:227–232. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Li XL, Zhang D, Knight D, et al: Priming
of immune responses against transporter associated with antigen
processing (TAP)-deficient tumours: tumour direct priming.
Immunology. 128:420–428. 2009. View Article : Google Scholar
|
|
14.
|
Everett MW and Edidin M: Tapasin increases
efficiency of MHC I assembly in the endoplasmic reticulum but does
not affect MHC I stability at the cell surface. J Immunol.
179:7646–7652. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Tourkova IL, Shurin GV, Ferrone S and
Shurin MR: Interferon regulatory factor 8 mediates tumor-induced
inhibition of antigen processing and presentation by dendritic
cells. Cancer Immunol Immunother. 58:567–574. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Singal DP, Ye M and Bienzle D:
Transfection of TAP 1 gene restores HLA class I expression in human
small-cell lung carcinoma. Int J Cancer. 75:112–116. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Wang X, Ni J, Hsu CL, et al: Reduced
expression of tocopherol-associated protein (TAP/Sec14L2) in human
breast cancer. Cancer Invest. 27:971–977. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Lopez-Albaitero A, Nayak JV, Ogino T, et
al: Role of antigen-processing machinery in the in vitro resistance
of squamous cell carcinoma of the head and neck cells to
recognition by CTL. J Immunol. 176:3402–3409. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Facoetti A, Nano R, Zelini P, et al: Human
leukocyte antigen and antigen processing machinery component
defects in astrocytic tumors. Clin Cancer Res. 11:8304–8311. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Tanaka K, Tsuchikawa T, Miyamoto M, et al:
Down-regulation of human leukocyte antigen class I heavy chain in
tumors is associated with a poor prognosis in advanced esophageal
cancer patients. Int J Oncol. 40:965–974. 2012.PubMed/NCBI
|
|
21.
|
Cresswell AC, Sisley K, Laws D, Parsons
MA, Rennie IG and Murray AK: Reduced expression of TAP-1 and TAP-2
in posterior uveal melanoma is associated with progression to
meta-static disease. Melanoma Res. 11:275–281. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Seliger B, Atkins D, Bock M, et al:
Characterization of human lymphocyte antigen class I
antigen-processing machinery defects in renal cell carcinoma
lesions with special emphasis on transporter-associated with
antigen-processing down-regulation. Clin Cancer Res. 9:1721–1727.
2003.
|
|
23.
|
Han LY, Fletcher MS, Urbauer DL, et al:
HLA class I antigen processing machinery component expression and
intratumoral T-cell infiltrate as independent prognostic markers in
ovarian carcinoma. Clin Cancer Res. 14:3372–3379. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Liu Q, Hao C, Su P and Shi J:
Down-regulation of HLA class I antigen-processing machinery
components in esophageal squamous cell carcinomas: association with
disease progression. Scand J Gastroenterol. 44:960–969. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Moss DJ, Khanna R, Sherritt M, Elliott SL
and Burrows SR: Developing immunotherapeutic strategies for the
control of Epstein-Barr virus-associated malignancies. J Acquir
Immune Defic Syndr. 1:S80–S83. 1999.PubMed/NCBI
|
|
26.
|
Chua ML, Ong SC, Wee JT, et al: Comparison
of 4 modalities for distant metastasis staging in endemic
nasopharyngeal carcinoma. Head Neck. 31:346–354. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Wang CT, Cao KJ, Li Y, Xie GF and Huang
PY: Prognosis analysis of nasopharyngeal carcinoma patients with
distant metastasis. Chin J Cancer. 26:212–215. 2007.(In
Chinese).
|
|
28.
|
Fang FM, Tsai WL, Chien CY, et al:
Pretreatment quality of life as a predictor of distant metastasis
and survival for patients with nasopharyngeal carcinoma. J Clin
Oncol. 28:4384–4389. 2010. View Article : Google Scholar : PubMed/NCBI
|