Introduction
Bladder cancer (BC) is the most common malignancy of
the urinary tract. At diagnosis, ~75–85% of BCs are confined to the
mucosa [stage Ta and carcinoma in situ (CIS)] or submucosa
(stage T1) (1). These categories
are grouped as non-muscle invasive bladder cancer (NMIBC).
BC cannot be considered as a single nosological
entity, but rather as a chronic, heterogeneous and polychronotopic
neoplastic diathesis, spatially and temporally multicentric. Due to
these characteristics, BC has a largely unpredictable natural
history.
This tumour is, in fact, characterized by various
types of spreading; it may be circumscribed or locally invasive,
multicentered, often with areas of CIS, aggressive, it may grow
rapidly, be invasive and develop early distant metastases.
The unpredictable biological behaviour of BC raises
a number of questions, amongst which why some superficial tumours
remain localized, whereas others, with identical characteristics,
become invasive. The six most significant clinicopathological
factors that determine a prognostic score for BC regarding
recurrence and disease progression are as follows: number of
tumours, size, previous recurrence rate, T stage, presence of
concomitant CIS and tumour grade (2).
With regard to prognosis and treatment, stage T1 BC
requires careful consideration, as a number of these tumours have a
high ratio of undifferentiated cells, with a consequently high risk
of progression and poor prognosis.
The treatment options for patients with high-grade
T1 stage NMIBC are complete resection of the lesion, followed by a
cycle of adjuvant intravesical Bacillus Calmette-Guérin (BCG)
instillation, which was shown to achieve a reduction of the
recurrence rate and, to a lesser extent, reduce or at least delay
the progression of the disease. An alternative treatment option is
radical cystectomy with urinary diversion (3–6).
With conservative therapy, 20–40% of the patients
will develop progression of the disease within 5 years (7). Patients undergoing cystectomy for
muscle invasive tumour progression exhibit a lower disease-free
survival rate compared to those undergoing radical cystectomy for
muscle invasive BC at diagnosis (28 vs. 55%) (8).
We should consider that radical cystectomy as a
primary option may be an overtreatment for ~50% of the patients
(9).
Due to the high risk of progression, the uncertainty
of long-term outcome and the weak efficacy of BCG treatment on
disease progression, we must identify T1 tumours with aggressive
behaviour in order to plan the most appropriate treatment, as they
are prone to recurrence and progression.
Therefore, several authors attempted to subclassify
stage T1 tumours into subgroups, using different anatomical
landmarks with different results (10–27).
A stratification of the T1 stage based on the
infiltration (T1b) or not (T1a) of the muscularis mucosae or its
invasion (T1c), has provided satisfactory results and is possibly
the most accurate evaluation of tumour depth (as regards the
chorion). However, this substaging system may be used in 58–100% of
the cases, due to the absence of the muscularis mucosae in
different histological preparations (10–23,27).
A method which evaluates the depth of invasion (< or >1.5 mm)
of the lamina propria may be more easily achievable, although less
precise (24,28–29).
A number of these substaging systems were found to exhibit a
significant correlation with disease progression (11–12,14–15,19–25,27);
however, few exhibited a significant correlation with overall
survival (OS) (16,23) as well as disease-specific survival
(DSS) (10,23,25,27).
The pathologist should always provide an indication
of the depth of invasion into the subepithelial stroma and should
always report the presence in the sample of muscle bundles
definitely free from invasion and belonging to the detrusor, if
present.
Due to the possibility of a pathological mismatch
regarding the identification of the muscularis mucosae-vascular
plexus (MM-VP), in the attempt to overcome this discrepancy, van
der Aa et al (24) proposed
a new and reliable subclassification system, with the primary aim
of predicting the clinical behaviour of these tumours. This system
does not require the identification of the MM-VP, but applies the
concept of microinvasion (T1m) in the case of single invasion of
the lamina propria with length of <0.5 mm at high magnification
and extensive invasion (T1e) in the presence of multifocal areas of
infiltration or with a length of >0.5 mm (24).
Recently, van Rhijn et al (27), evaluated the impact of the method
suggested by van der Aa et al (24) on clinical outcome and reported a
significant correlation of this substaging system not only with
disease progression, but also with cancer-specific survival. The
aim of this study was to test this new substaging system in our
population of patients with stage T1 NMIBC at diagnosis and assess
its prognostic role in terms of disease progression and DSS.
Material and methods
Patients
All patients with primary stage T1G3 urothelial
carcinoma of the urinary bladder who were referred to our
institution between January, 2000 and December, 2006 were included
in this study. Patients with a history of BC prior to the
occurrence of a T1 tumour were not considered. The pathological
specimens were reviewed in order to confirm the diagnosis of T1 and
the substaging.
We retrospectively identified 40 patients (8 women
and 32 men) with a mean age ± standard deviation (SD) at diagnosis
of 69.9±10.5 years. All the patients had undergone a transurethral
resection of the bladder tumour (TUR-BT). A second TUR-BT within 6
weeks was performed in cases of macroscopic incomplete TUR-BT or
absence of muscularis mucosae after the first endoscopic resection.
All the patients were initially managed conservatively with an
induction course of BCG. Random biopsies, a standard repeat TUR and
a single instillation of chemotherapy following TUR were not
performed (26). The surveillance
of the patients included cystoscopy and cytology every 3–4 months
in the first 2 years and at a lower frequency thereafter (6–12
months) if no recurrence was detected. Upper urinary tract imaging
was performed every 2 years or when indicated by clinical suspicion
(26).
Disease progression was defined as detection of a
muscle-invasive BC in case of recurrence or the presence of local
or distant metastases. The patients were followed up until death or
until their last outpatient follow-up.
Staging
The original slides of 40 primary T1 bladder tumours
were reviewed by one pathologist (M.B.) to determine stage and
grade. The pathologist was blinded to the clinical outcome but was
aware of the original T1 diagnosis. The World Health Organization
1973 and 2004 classifications were used to review the grade. After
confirming stage T1, the pathologist further stratified the
patients according to the following models: i) T1a (the tumour does
not infiltrate the MM-VP), T1b (the tumour partially infiltrates
the MM-VP) and T1c (the tumour infiltrates and invades the MM-VP).
If the MM-VP was not present at the invasion front, the case was
assigned to T1a or T1c, based on the extent of invasion into the
lamina propria by examining the MM-VP in tumour-free areas in the
same or other TUR chips. ii) T1m (maximum diameter of the tumour
infiltrating the lamina propria ≤0.5 mm under a high-resolution
microscope) and T1e (maximum diameter of the tumour infiltrating
the lamina propria >0.5 mm).
Statistical analysis
Statistical analysis was performed using SPSS
software, version 20.0 (IBM, Armonk, NY, USA). Continuous variables
are reported as means ± SD (in cases of normal distribution) or
median and interquartile range (IQR) (in cases of non-normal
distribution). The t-test, Mann-Whitney U test and Pearson’s
Chi-square test were used to compare categorical and continuous
variables. The clinical outcomes, such as disease progression and
DSS, were analyzed using univariate statistical analysis according
to Kaplan-Meier and multivariate analysis using Cox regression, in
order to identify independent prognostic factors among age, gender,
tumour size, tumour multifocality and substaging. A two-sided
P<0.05 was considered to indicate a statistically significant
difference.
Results
Patient and tumour characteristics,
patient distribution and outcomes
Table I summarizes
the demographic characteristics of patients and tumours following
pathological review. The distribution of patients with regard to
the two different models is presented in Table II. The MM-VP was not present at
the tumour invasion front in 3 tumours (7.5%). These cases were all
classified as T1a, as indicated in ‘Patients and methods’. The
median follow-up was 9.5 years (IQR, 3–11.25 years). No patients
experienced disease recurrence at the level of the upper urinary
tract. No patients underwent radical cystectomy for stage T1
disease at diagnosis.
 | Table IPatients and tumour characteristics
after pathological review. |
Table I
Patients and tumour characteristics
after pathological review.
| Variables | No. (%) |
|---|
| No. of patients | 40 (100) |
| Gender |
| Male | 32 (80) |
| Female | 8 (20) |
| No. of tumours |
| Single | 38 (91) |
| Multiple | 2 (9) |
| Tumour size (cm) |
| <3 | 39 (97.5) |
| >3 | 1 (2.5) |
| Concurrent carcinoma
in situ |
| Yes | 0 (0) |
| No | 40 (100) |
| Endovesical
therapy |
| Bacillus
Calmette-Guérin | 21 (52.5) |
| No | 19 (47.5) |
| Table IIDistribution of patients in accordance
with the two modes of T1 substaging. |
Table II
Distribution of patients in accordance
with the two modes of T1 substaging.
| T1 substaging | No. (%) |
|---|
| According to MM-VP
invasion | |
| T1a | 15 (37.5) |
| T1b | 25 (62.5) |
| T1c | 0 (0) |
| According to tumour
diameter invading the lamina propria | |
| T1m | 12 (30) |
| T1e | 28 (70) |
No patients underwent intravesical chemotherapy
after TUR-BT; 21 patients (52.5%) were subjected to intravesical
immunotherapy with BCG. Age, gender, tumour size and multifocality
were not found to be of statistical significance.
The DSS at 5 and 10 years was 80 and 67.5%,
respectively. A total of 13 patients (32.5%) developed disease
progression at 5 years and eventually succumbed to BC.
DSS and disease progression according to
substage
The Kaplan-Meier curves regarding DSS and disease
progression according to the two types of substaging are shown in
Fig. 1. With regard to disease
progression, patients with stage T1a disease exhibited a 5- and
10-year progression rate of 13.3 and 20%, respectively, which was
lower compared to that in patients with stage T1b disease, without
reaching full statistical significance (P=0.058).
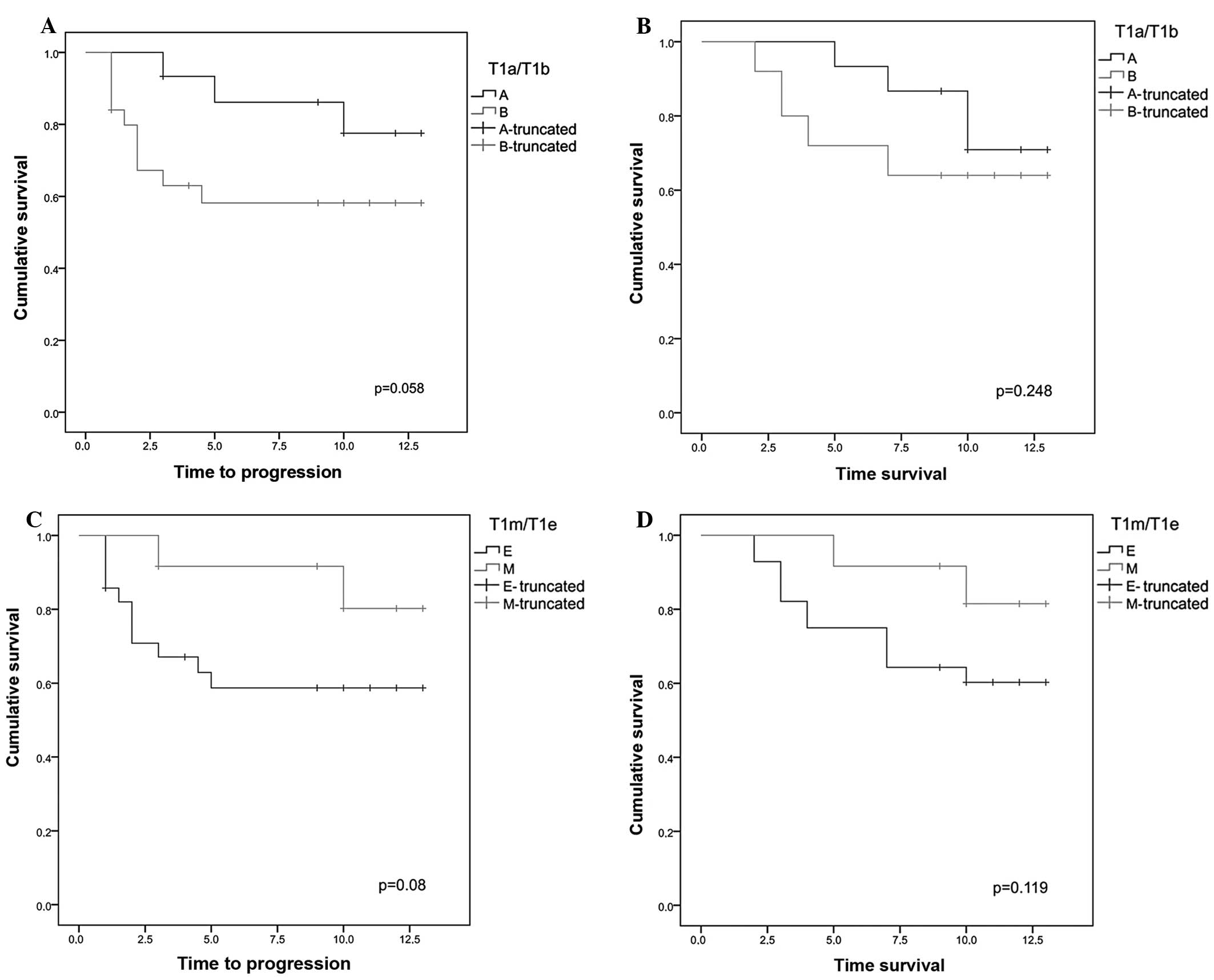 | Figure 1(A) Kaplan-Meier curves regarding
disease progression in groups T1a and T1b. The stage T1a group
exhibited a disease progression rate of 13.3 and 20% at 5 and 10
years, respectively; in the T1b stage group, the disease
progression at 5–10 years was 40% (P=0.058). (B) Kaplan-Meier
curves regarding disease-specific survival (DSS) in groups T1a and
T1b. In the stage T1a group the DSS rate at 5 and 10 years was 93.3
and 73.3%, respectively, whereas the T1b stage group exhibited 5-
and 10-year DSS rate of 72 and 64%, respectively (P=0.248). (C)
Kaplan-Meier curves regarding disease progression in groups T1e and
T1m. In the stage T1m group the percentage of patients free of
disease progression at 5 and 10 years was 91.7 and 83.3%,
respectively, whereas in the stage T1a group it was 60.7% at 5 and
10 years (P=0.08). (D) Kaplan-Meier curves regarding DSS in groups
T1m and T1e. In the stage T1m group the DSS rate at 5 and 10 years
was 91.7 and 83.3%, respectively, whereas in the stage T1e group it
was 71.4 and 60.7% at 5 and 10 years, respectively (P=0.119). |
With regard to DSS, patients with stage T1a disease
exhibited a 5- and 10-year DSS of 93.3 and 73.3%, respectively,
which was higher but not statistically significant compared to that
of the T1b group (72 and 64%, P=0.248).
Using the T1m/T1e substaging system, the group of
patients with stage T1m disease exhibited a disease progression
rate of 8.3 and 16.7% at 5 and 10 years, respectively, which was
lower but not statistically significant compared to that in the
group with stage T1e disease (39.3%, P=0.08).
With regard to DSS, the patients in the T1m group
presented with DSS rates of 91.7 and 83.3% at 5 and 10 years,
respectively, which was higher compared to those in the T1e group
(71.4 and 60.7%), although not reaching statistical significance
(P=0.119).
Discussion
The treatment of stage T1 urothelial bladder tumours
represents a therapeutic challenge. Conservative treatment may lead
to disease progression and death; however, a radical intervention,
such as radical cystectomy, may represent an overtreatment of
patients who may not ultimately develop disease progression.
Therefore, it is important to establish a substaging system which
is simple and useful in clinical practice and able to provide
prognostic information, in order to guide the urologist through the
decision-making process for the management of such patients.
Several studies investigated the usefulness of the
MM-VP layer in stratifying stage T1 urothelial carcinoma of the
bladder into T1a, T1b and T1c substages (10–23,27).
The main problem of this system lies with the lack of consensus
regarding the identification of the MM-VP at the level of the
invasive front of the tumour (28,29).
Consequently, the percentages of substaging were highly variable,
between 58 and 100% (10–23,27).
This high variability may be further explained by the different
quality of TUR-BT and by the possible damage to the lamina propria
due to TUR-BT itself and by the intravesical treatment. In our
study, we obtained an overall substaging rate of 92.5%. However, it
is not always possible to obtain a satisfactory excisional biopsy
specimen comprising an adequate sample of muscle layer, making it
difficult to perform this type of substaging.
For this reason, Cheng et al (25) proposed a new staging system based
on the depth of invasion expressed in μm. The authors demonstrated
that millimeter measurement of the depth of invasion in TUR-BT
specimens was possible in 100% of the 83 TUR-BT samples analyzed
and proposed a 1.5-mm cut-off (25). The possible limitations of this
cut-off lie with the variability of the thickness of the lamina
propria.
In order to overcome this limitation, van der Aa
et al (24) modified the
concept of Cheng et al (25), recommending a depth of 0.5 mm to
distinguish microinvasion (T1m) from ‘extended’ invasion (T1e).
This new substaging tool is easy to apply, reproducible, useful in
100% of cases and more reliable compared to other substaging
systems (28).
Recently, van Rhijn et al (27) analyzed the T1a/T1b/T1c and T1m/T1e
substaging system, demonstrating a higher prognostic value in terms
of disease progression as well as DSS. In fact, in this study, the
prognostic value of the T1a/T1b/T1c system was statistically
significant only for disease progression and only at the univariate
analysis. However, this substaging was only possible in 63% of the
samples; the number of patients was not sufficient to corroborate
the result. In our study, it was not possible to identify any
prognostic significance for this system, neither for disease
progression nor for DSS, although substaging was possible in 92.5%
of the cases. However, the sample size of our study was
insufficient for a reliable statistical evaluation.
Faivre d’Arcier et al (23), analyzing a population 3 times more
numerous and with a substaging percentage of 100%, reported a
significant prognostic value for such substaging, not only with
regard to the disease progression, but also with regard to the
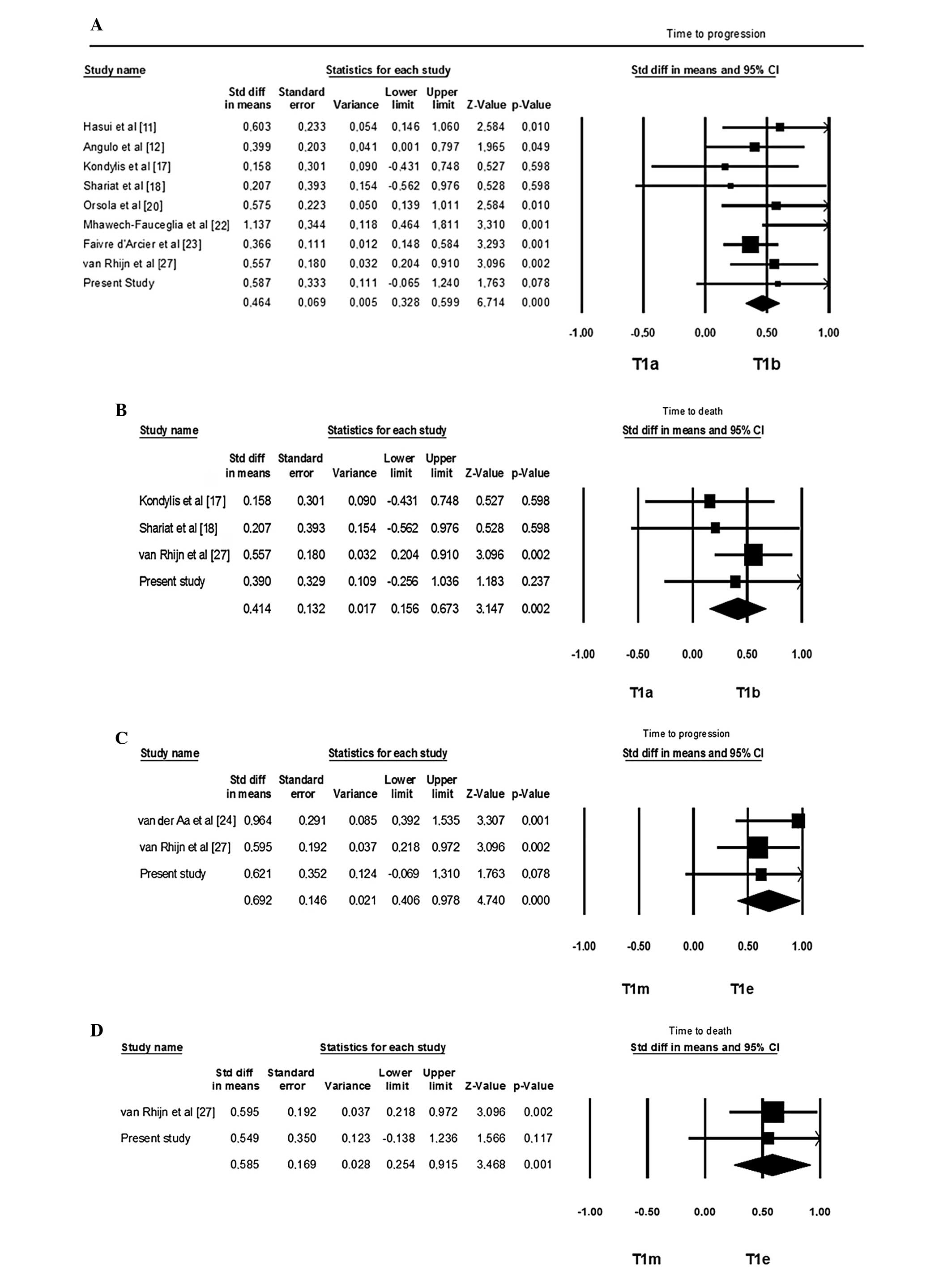
cancer-specific survival and OS. When performing a pooled analysis
of data in the literature (including our own), despite the
considerable heterogeneity among the studies, a significant
prognostic role for T1a/T1b/T1c substaging emerged, with regard to
disease progression and DSS (Fig.
2).
With regard to the T1m/T1e substaging, two studies
investigated its prognostic value on disease progression (24,27)
and only one on the DSS (27);
those studies identified a significance at the multivariate
analysis, which was not fully confirmed, however, by our study.
However, at the cumulative analysis of the
literature data (including our own study), this substaging system
was of significant prognostic value on disease progression and DSS,
although with the same limitations regarding heterogeneity as in
the other substaging system (Fig.
2).
All studies available in the literature, including
ours, present with several limitations, such as the retrospective
design, the small sample size and the lack of a standard TUR-BT.
The advantage of the T1m/T1e substaging system is represented by
its greater reproducibility and feasibility, regardless of the
presence of the MM-VP.
In conclusion, although in our study the two
substaging systems of T1 carcinoma of the bladder were not proven
to be fully prognostic regarding tumour progression or DSS, the
cumulative analysis of the literature indicated that both systems,
namely the T1a vs. T1b/T1c and the T1m vs. T1 appear to be
predictive of the behaviour of BC.
The T1m/T1e system may be more applicable and
reproducible, being independent from the presence of MM-VP on the
sample and independent from the quality of the initial TUR-BT.
Therefore, this system may be a valid and useful prognostic tool
for guiding the decision-making process for the treatment of
patients with stage T1 BC.
However, further prospective, properly designed and
well conducted cohort studies with adequate sample size are
required in order to determine the optimal prognostic substaging
model for T1 BC.
References
|
1
|
Anastasiadis A and de Reijke TM: Best
practice in the treatment of nonmuscle invasive bladder cancer.
Ther Adv Urol. 4:13–32. 2012. View Article : Google Scholar
|
|
2
|
Sylvester RJ, van der Meijden AP,
Oosterlinck W, et al: Predicting recurrence and progression in
individual patients with stage Ta T1 bladder cancer using EORTC
risk tables: a combined analysis of 2596 patients from seven EORTC
trials. Eur Urol. 49:466–477. 2006. View Article : Google Scholar
|
|
3
|
van Rhijn BW, Burger M, Lotan Y, et al:
Recurrence and progression of disease in non-muscle-invasive
bladder cancer: from epidemiology to treatment strategy. Eur Urol.
56:430–442. 2009.PubMed/NCBI
|
|
4
|
Sylvester RJ, van der Meijden AP and Lamm
DL: Intravesical bacillus Calmette-Guerin reduces the risk of
progression in patients with superficial bladder cancer: a
meta-analysis of the published results of randomized clinical
trials. J Urol. 168:1964–1970. 2002. View Article : Google Scholar
|
|
5
|
Babjuk M, Oosterlinck W, Sylvester R, et
al: EAU guidelines on non-muscle-invasive urothelial carcinoma of
the bladder, the 2011 update. Eur Urol. 59:997–1008. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Herr HW: Is maintenance Bacillus
Calmette-Guérin really necessary? Eur Urol. 54:971–973. 2008.
|
|
7
|
Stein JP: Indications for early
cystectomy. Urology. 62:591–595. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Schrier BP, Hollander MP, van Rhijn BW,
Kiemeney LA and Witjes JA: Prognosis of muscle-invasive bladder
cancer: difference between primary and progressive tumours and
implications for therapy. Eur Urol. 45:292–296. 2004. View Article : Google Scholar
|
|
9
|
Stein JP and Penson DF: Invasive T1
bladder cancer: indications and rationale for radical cystectomy.
BJU Int. 102:270–275. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Younes M, Sussman J and True LD: The
usefulness of the level of the muscularis mucosae in the staging of
invasive transitional cell carcinoma of the urinary bladder.
Cancer. 66:543–548. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hasui Y, Osada Y, Kitada S, et al:
Significance of invasion to the muscularis mucosae on the
progression of superficial bladder cancer. Urology. 43:782–786.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Angulo JC, Lopez JI, Grignon DJ, et al:
Muscularis mucosa differentiates two populations with different
prognosis in stage T1 bladder cancer. Urology. 45:47–53. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Platz CE, Cohen MB, Jones MP, et al: Is
microstaging of early invasive cancer of the urinary bladder
possible or useful? Mod Pathol. 9:1035–1039. 1996.PubMed/NCBI
|
|
14
|
Holmang S, Hedelin H, Anderstrom C, et al:
The importance of the depth of invasion in stage T1 bladder
carcinoma: a prospective cohort study. J Urol. 157:800–804. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Smits G, Schaafsma E, Kiemeney L, et al:
Microstaging of pT1 transitional cell carcinoma of the bladder:
identification of subgroups with distinct risks of progression.
Urology. 52:1009–1014. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hermann GG, Horn T and Steven K: The
influence of the level of lamina propria invasion and the
prevalence of p53 nuclear accumulation on survival in stage T1
transitional cell bladder cancer. J Urol. 159:91–94. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kondylis FI, Demirci S, Ladaga L, et al:
Outcomes after intravesical bacillus Calmette-Guerin are not
affected by substaging of high grade T1 transitional cell
carcinoma. J Urol. 163:1120–1123. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shariat SF, Weizer AZ, Green A, et al:
Prognostic value of p53 nuclear accumulation and histopathologic
features in T1 transitional cell carcinoma of the urinary bladder.
Urology. 56:735–740. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bernardini S, Billerey C, Martin M, et al:
The predictive value of muscularis mucosae invasion and p53 over
expression on progression of stage T1 bladder carcinoma. J Urol.
165:42–46. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Orsola A, Trias I, Raventos CX, et al:
Initial high-grade T1 urothelial cell carcinoma: feasibility and
prognostic significance of lamina propria invasion microstaging
(T1a/b/c) in BCG-treated and BCG-non-treated patients. Eur Urol.
48:231–238. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Andius P, Johansson SL and Holmang S:
Prognostic factors in stage T1 bladder cancer: tumor pattern (solid
or papillary) and vascular invasion more important than depth of
invasion. Urology. 70:758–762. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mhawech-Fauceglia P, Fischer G, Alvarez V
Jr, et al: Predicting outcome in minimally invasive (T1a and T1b)
urothelial bladder carcinoma using a panel of biomarkers: a high
throughput tissue microarray analysis. BJU Int. 100:1182–1187.
2007.PubMed/NCBI
|
|
23
|
Faivre d’Arcier B, Celhay O, Safsaf A, et
al: T1 bladder carcinoma: prognostic value of the muscularis
mucosae invasion (T1a/T1b). A multicenter study by the French
Urological Association (CCAFU). Prog Urol. 20:440–449. 2010.(In
French).
|
|
24
|
van der Aa MN, van Leenders GJ, Steyerberg
EW, et al: A new system for substaging pT1 papillary bladder
cancer: a prognostic evaluation. Hum Pathol. 36:981–986.
2005.PubMed/NCBI
|
|
25
|
Cheng L, Neumann RM, Weaver AL, et al:
Predicting cancer progression in patients with stage T1 bladder
carcinoma. J Clin Oncol. 17:3182–3187. 1999.PubMed/NCBI
|
|
26
|
van Rhijn BW, van der Kwast TH,
Kakiashvili D, et al: Pathological stage review is indicated in
primary pT1 bladder cancer. BJU Int. 106:206–211. 2010.
|
|
27
|
van Rhijn BW, van der Kwast TH, Alkhateeb
SS, et al: A new and higly prognostic system to discern T1 bladder
cancer substage. Eur Urol. 61:378–384. 2012.
|
|
28
|
Nieder AM, Brausi M, Lamm D, et al:
Management of stage T1 tumors of the bladder: International
Consensus Panel. Urology. 66(Suppl 1): 108–125. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Eble J, Sauter G, Epstein JI and
Sesterhenn IA: Pathology and Genetics of Tumours of the Urinary
System and Male Genital Organs. IARC Press; Lyon: 2004
|