Introduction
Multiple myeloma (MM) is a hematological malignancy
that primarily affects elderly individuals. The clinical
manifestations of MM, collectively referred to as ‘CRAB’, include
hypercalcemia, renal insufficiency, anaemia and bony lesions,
caused by either direct infiltration by neoplastic plasma cells or
deposition of monoclonal immunoglobulins (Ig), particularly light
chains. Myelomatous pleural effusion (MPE) is an uncommon
manifestation, with only a few cases reported to date (1). Patients with MPE often have
advanced-stage disease and poor prognosis, despite aggressive
treatment. We herein present a case of of MPE diagnosed via
semi-rigid thoracoscopy in a patient with IgA-λ MM, and a review of
the current literature on clinical manifestations, laboratory
examinations and diagnosis of MPE.
Case report
A 70-year-old male patient presented at The First
Affiliated Hospital of Wenzhou Medical University (Wenzhou, China)
with a 1-week history of cough and exertional dyspnea with no
fever, chest pain, purulent sputum and hemoptysis. The patient was
a smoker with >20 pack-years, but his medical, social and family
history were otherwise unremarkable. On physical examination, the
patient appeared pale, with decreased breath sounds and dullness on
percussion over the left posterior thorax. The laboratory findings
were as follows: White blood cell count, 3.9×109/l
(50.9% neutrophils, 32.7% lymphocytes, and 13.5% monocytes, normal
basophils and eosinophils); erythrocyte count,
2.7×1012/l; hemoglobin, 81 g/l; platelet count,
180×109/l; total protein, 85.5 g/l; albumin, 31.8 g/l;
globulin, 53.7 g/l; serum calcium, 3.6 mmol/l [normal limit (NL):
2.1–2.6 mmol/l]; serum creatinine, 180 µmol/l (NL: 44–97 µmol/l);
urea nitrogen, 8.7 mol/l; C-reactive protein, 30.5 mg/l; lactate
dehydrogenase (LDH), 364.0 µ/l; β2-microglobulin, 21.1
µg/ml (NL: 0.9–2.7 µg/ml); serum κ light chain, 3.4 g/l (NL:
6.3–13.5 g/l); serum λ light chain, 28.3 g/l (NL: 3.1–7.2 g/l);
serum IgA, 24.3 g/l; IgM, 153.00 mg/l; IgG, 4.4 g/l; and IgM, 0.43
g/l; the IgE and IgD levels were normal. Carcinoembryonic antigen
(CEA), carbohydrate antigen 19-9 and brain natriuretic peptide
levels were within normal limits, and the T-SPOT®
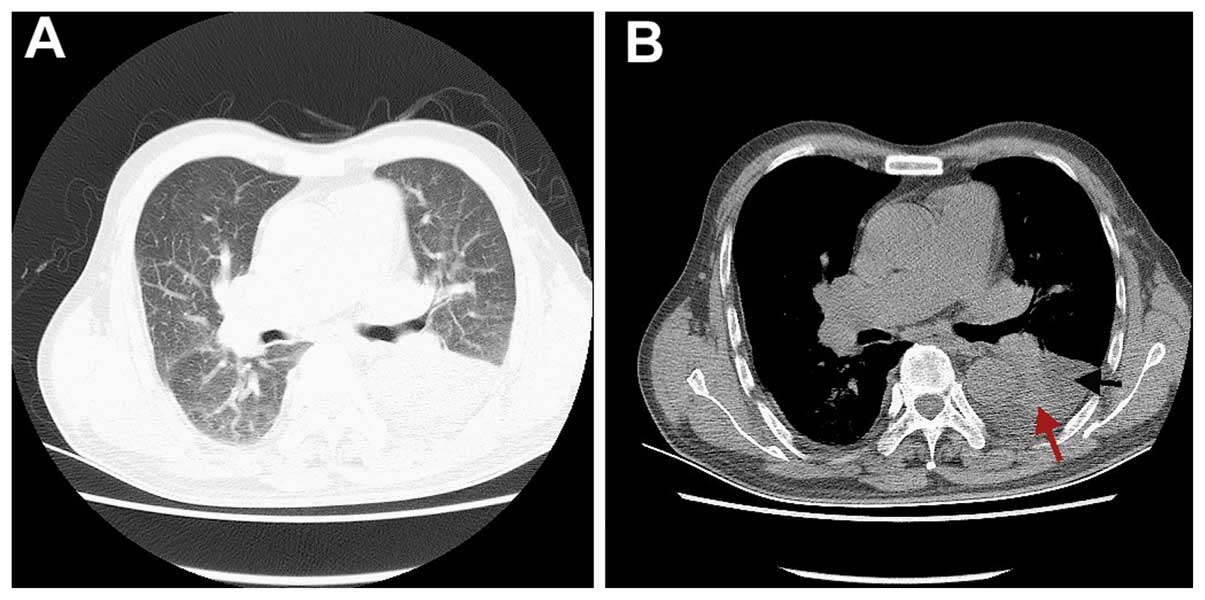
tuberculosis test was negative. Computed tomography (CT) revealed
left pleural effusion and atelectasis of the lower lobe of the left
lung (Fig. 1). Fiberoptic
bronchoscopy revealed no endobronchial lesions. The patient
underwent thoracentesis and the pleural fluid was highly cellular,
with a nucleated cell count of 1.7×109/l (42%
mononuclear cells), and contained total protein at 46.1 g/l, LDH at
193.0 U/l, adenosine deaminase at 20.0 U/l and CEA at 1.5 µg/l;
thus, the effusion was considered as exudative according to the
Light criteria (2). Malignant cells
were not found in the pleural fluid. Immune fixation
electrophoresis of the blood revealed IgA-λ-type monoclonal
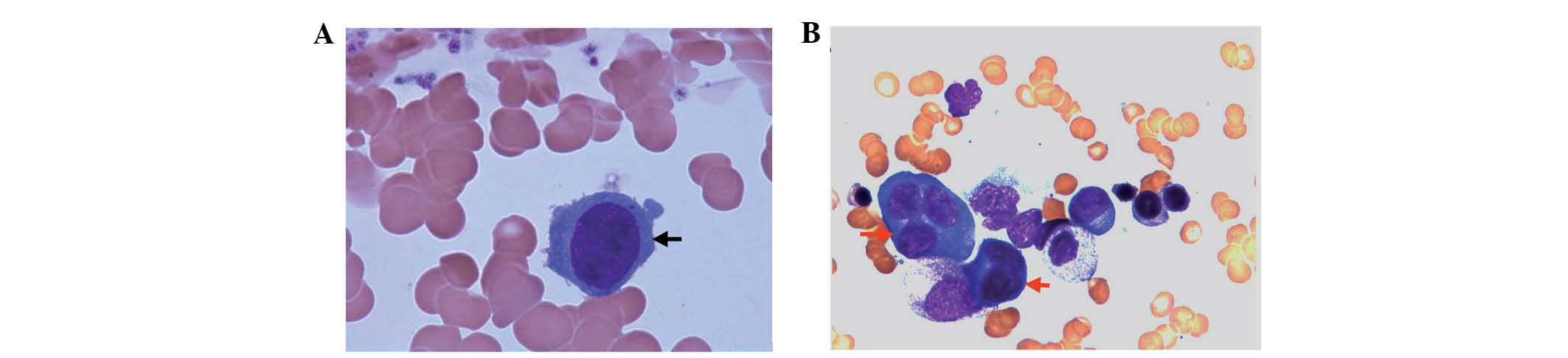
immunoglobulin. The patient underwent bone marrow aspiration biopsy
twice. The first bone marrow biopsy showed no significant
abnormalities (Fig. 3A), while the
second revealed a mildly hypercellular marrow with 13% plasma cells
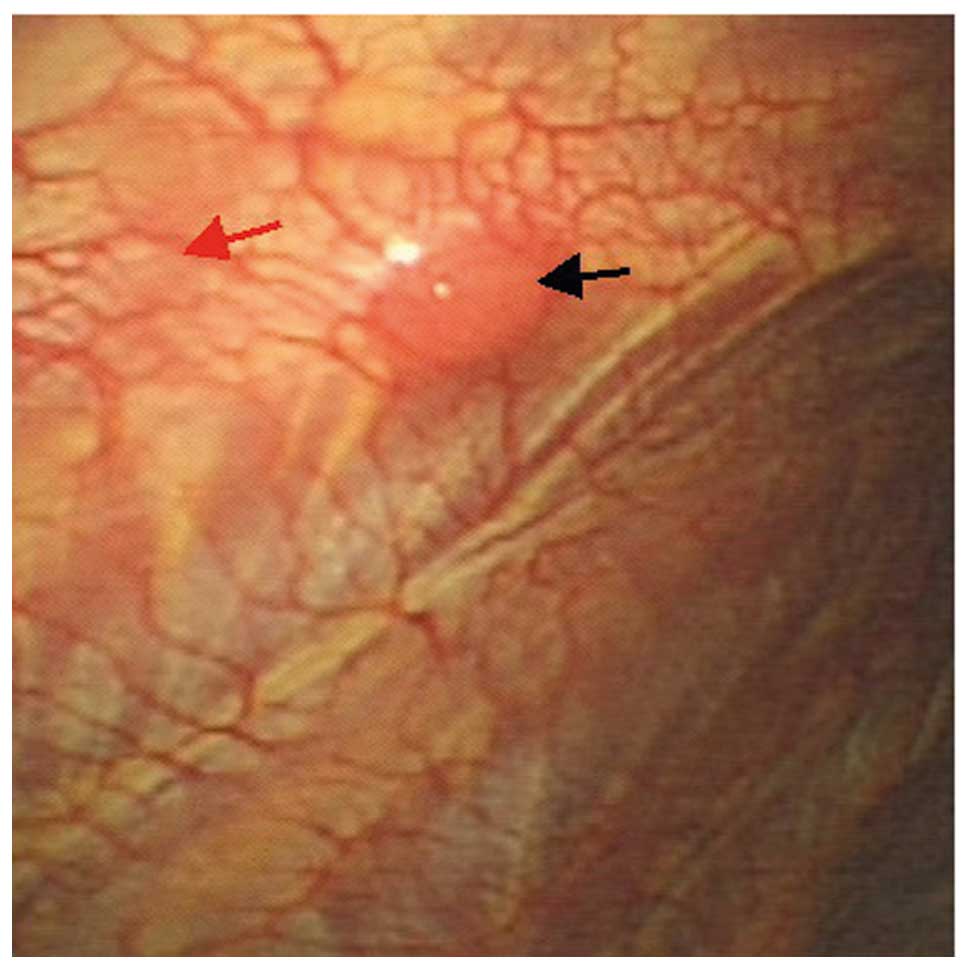
(Fig. 3B). Semi-rigid thoracoscopy
was performed, which revealed a solitary pleural nodule sized
~1×0.8 cm on the parietal pleura (Fig.
4). Histopathological evaluation of the biopsied nodule
revealed sheets of neoplastic plasma cells, which were positive for
CD38 and multiple myeloma oncogene 1 (MUM1), with λ light chain
restriction and a Ki-67 index of 50% (Fig. 5). The patient was diagnosed with
IgA-λ-type MM with pleural involvement, based on the clinical
manifestations, laboratory examinations, radiographic findings and
the results of bone marrow and pleural biopsies. The patient
received chemotherapy with bortezomib, epiadriamycin and
dexamethasone; however, he deteriorated rapidly after one cycle of
chemotherapy and succumbed to the disease 8 weeks after the initial
presentation.
Written informed consent was obtained from the
patient regarding the publication of this case report and any
accompanying images.
Discussion
As a hematopoietic malignancy, MM primarily affects
the bone marrow, but may also involve extramedullary tissue. The
characteristic clinical manifestations of MM, collectively referred
to as ‘CRAB’, include hypercalcemia, renal failure, anemia and bone
lesions. MPE is an uncommon manifestation, occurring in ~6% of
patients with MM (1). Our patient
presented with the typical ‘CRAB’ signs and symptoms in addition to
a pleural myelomatous lesion. The possible etiological factors for
pleural effusion include congestive heart failure secondary to
amyloidosis, chronic renal failure, nephritic syndrome secondary to
renal tubular infiltration with paraprotein and development of
glomerular damage, direct infiltration of pleural fluid from
adjacent tissues, hypoalbuminemia, pulmonary embolism, secondary
neoplasm, lymphatic drainage obstruction by tumor infiltration,
infection and pleural myelomatous involvement (3). It has been reported that 80% of MPE
cases are related to IgA MM (4); our
patient was also IgA type. In the present case, the unilateral
exudative effusion was mainly attributed to a localized pleural
myelomatous lesion. Chemotherapy is the mainstay of therapy for
pleural myeloma, despite the low response rate and short survival
time.
An English literature search for related studies
between 1990 and 2015 was conducted through PubMed, using the
search criteria (‘pleural effusion’ and ‘multiple myeloma’) or
‘myelomatous pleural effusions’, which yielded 152 candidate
articles. Based on the inclusion criteria (pleural myelomatous
involvement confirmed by cytological analysis of pleural effusion
or histopathological evaluation of pleural biopsy specimens), a
total of 22 cases were included in the final review and analysis.
The patient characteristics, including general information,
laboratory test results, diagnostic methods and clinical outcomes,
were retrospectively reviewed and are summarized in Table I. The patient age ranged from 40 to
83 years, with a mean of 60 years and a slight male predominance.
The diagnosis was made by cytological analysis of the pleural
effusion in 15 cases; pleural biopsy specimens were examined in 7
patients, including 3 undergoing video-assisted thoracoscopy
sampling (VATS) and 1 undergoing semi-rigid thoracoscopy (present
case). The diagnostic method for pleural myeloma was not specified
in the remaining case. All patients with pleural involvement had a
short survival (ranging from 4 weeks to 12 months) after
presentation with pleural effusion. The literature review revealed
that MM with pleural involvement most commonly affects older (≥50
years) and elderly patients (≥65 years) and is associated with a
poor prognosis.
 | Table I.Reported cases of pleural myeloma. |
Table I.
Reported cases of pleural myeloma.
| First author
(Refs.) | Year | Age/gender | Ig type | EMI | Osteolysis | Pathology | Thoracoscopy | Survivala (months) |
|---|
| Jiang (5) | 2015 | 78/ND | IgD | No | Yes | CPE | No | ND |
| Suwatanapongched
(6) | 2014 | 76/M | IgG-λ | No | Yes | CPE | No | 1 |
| Zhang (7) | 2014 | 53/M | IgG-κ | No | No | Pleural biopsy | VATS | ND |
| Xu (8) | 2013 | 45/M | Negative | No | Yes | Pleural biopsy | No | 12 |
| Chim (9) | 2013 | 56/M | IgG-λ | No | No | ND | No | 5 |
| Oudart (3) | 2012 | 62/F | IgG-κ | ND | ND | CPE | No | ND |
| Klanova (10) | 2012 | 43/F | IgG-κ | Yesb | Yes | CPE | No | 12 |
| Keklik (11) | 2012 | 52/M | IgG-κ | No | Yes | CPE | No | ND |
| Al-Farsi (12) | 2010 | 56/M | IgG-κ | No | Yes | CPE | No | 6 |
| Huang (13) | 2010 | 67/F | IgA-λ | NG | ND | CPE | No | ND |
| Malhotra (14) | 2010 | 50/M | ND | NG | ND | CPE | No | 2 |
| Ghoshal (15) | 2010 | 61/F | ND | NG | Yes | Pleural biopsy | No | ND |
| Nakazato (16) | 2009 | 74/M | IgG-κ | Yesb | Yes | CPE | No | 8 |
| Neuman (17) | 2009 | 47/M | ND | ND | Yes | CPE | No | ND |
| Chang (18) | 2009 | 83/F | IgD-λ | ND | No | CPE | No | 2 |
| Yokoyama (19) | 2008 | 58/M | IgD | Yesb | NG | Pleural biopsy | No | 3 |
| Kim (20) | 2008 | 76/F | IgA-λ | ND | Yes | CPE | No | 1 |
| Dhingra (21) | 2007 | 40/M | IgG | ND | Yes | CPE | No | ND |
| Inoue (22) | 2005 | 51/F | IgG-λ | Yesb | ND | Pleural biopsy | VATS | 10 |
| Kim (23) | 2000 | 61/F | IgG-λ | ND | ND | Pleural biopsy | No | ND |
| Rodríguez (4) | 1994 | 51/M | IgA-κ | ND | Yes | CPE | No | 11 |
| Makino (24) | 1992 | 73/F | IgG | ND | No | CPE | No | ND |
| Present case | 2015 | 70/M | IgA-λ | ND | Yes | Pleural biopsy | SRTS | 8 |
In the previously reported cases reviewed herein,
pleural myeloma was identified by pleural effusion cytology or/and
histological examination of pleural biopsy specimens, despite the
advantages of thoracoscopy, or open and multiple-site biopsy.
However, a localized pleural myelomatous lesion is difficult to
detect on CT or ultrasonography, which hampers image-guided direct
biopsy of the lesion. With the advances in thoracoscopic
techniques, open and multiple-site pleural biopsy may be performed
by VATS or semi-rigid thoracoscopy. These procedures may improve
the diagnostic rate in patients with pleural lesions of unknown
etiology. However, thoracoscopy is rarely considered as a feasible
option for identifying the etiology of pleural effusion in patients
with MM. In selected patients, semi-rigid thoracoscopy may be
superior to VATS in terms of safety and cost-effectiveness. As
semi-rigid thoracoscopy may be successfully performed under local
anesthesia and intravenous sedation, the majority of patients with
mild or moderate cardiopulmonary dysfunction may safely undergo
this procedure, while they would not be eligible for VATS due to
the risks associated with general anesthesia. Our patient underwent
semi-rigid thoracoscopy with biopsy of a small solitary nodule on
the left parietal pleura, which was diagnosed as a myelomatous
lesion. To the best of our knowledge, this was the first report of
a solitary pleural myelomatous lesion diagnosed by pleural biopsy
via semi-rigid thoracoscopy. Semi-rigid thoracoscopy may be
successfully performed by pulmonologists under local anesthesia.
The procedure appears to be safer, more cost-effective and
comfortable for patients compared with VATS.
In summary, we reported a case of solitary pleural
myelomatous nodule diagnosed by semi-rigid thoracoscopy and pleural
histopathology. Although MPE is uncommon, MM should be considered
in patients with pleural effusion of unknown etiology. Semi-rigid
thoracoscopy appears to be a feasible option for diagnosing pleural
myeloma in the era of precision medicine.
Glossary
Abbreviations
Abbreviations:
|
MM
|
multiple myeloma
|
|
MPE
|
myelomatous pleural effusion
|
|
NL
|
normal limit
|
|
CT
|
computed tomography
|
|
VATS
|
video-assisted thoracoscopy
|
References
|
1
|
Kintzer JS Jr, Rosenow EC III and Kyle RA:
Thoracic and pulmonary abnormalities in multiple myeloma. A review
of 958 cases. Arch Intern Med. 138:727–730. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Light RW: The Light criteria: The
beginning and why they are useful 40 years later. Clin Chest Med.
34:21–26. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Oudart JB, Maquart FX, Semouma O, Lauer M,
Arthuis-Demoulin P and Ramont L: Pleural effusion in a patient with
multiple myeloma. Clin Chem. 58:672–674. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rodríguez JN, Pereira A, Martinez JC,
Conde J and Pujol E: Pleural effusion in multiple myeloma. Chest.
105:622–624. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jiang AG, Yang YT, Gao XY and Lu HY:
Bilateral pleural effusion as an initial manifestation of multiple
myeloma: A case report and literature review. Exp Ther Med.
9:1040–1042. 2015.PubMed/NCBI
|
|
6
|
Suwatanapongched T, Pornsuriyasak P,
Kanoksil W, Morasert T and Virayavanich W: A 76-year-old man with
anemia, bone pain, and progressive dyspnea. Diagnosis: Bilateral
myelomatous pleural effusions with extramedullary plasmacytomas.
Chest. 145:913–918. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang LL, Li YY, Hu CP and Yang HP:
Myelomatous pleural effusion as an initial sign of multiple
myeloma-a case report and review of literature. J Thorac Dis.
6:E152–E159. 2014.PubMed/NCBI
|
|
8
|
Xu XL, Shen YH, Shen Q and Zhou JY: A case
of bilateral pleural effusion as the first sign of multiple
myeloma. Eur J Med Res. 18:72013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chim CS and Ma ES: Survival of >20
years in a myeloma patient with an unusual combination of t(14;16)
and hyperdiploidy: A case report. Oncol Lett. 6:1663–1664.
2013.PubMed/NCBI
|
|
10
|
Klanova M, Klener P, Trneny M, Straub J
and Spicka I: Intrapleural bortezomib for the therapy of
myelomatous pleural effusion: A case report. Case Reports Immunol.
2012:9784792012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Keklik M, Sivgin S, Pala C, Eroglu C,
Akyol G, Kaynar L, Koker MY, Camlica D, Unal A, Cetin M and Eser B:
Flow cytometry method as a diagnostic tool for pleural fluid
involvement in a patient with multiple myeloma. Mediterr J Hematol
Infect Dis. 4:e20120632012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Al-Farsi K, Al-Haddabi I, Al-Riyami N,
Al-Sukaiti R and Al-Kindi S: Myelomatous Pleural Effusion: Case
report and review of the literature. Sultan Qaboos Univ Med J.
11:259–264. 2011.PubMed/NCBI
|
|
13
|
Huang TC and Chao TY: Myelomatous pleural
effusion. QJM. 103:705–706. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Malhotra KP, Agrawal V and Prasad N:
Myelomatous pleural effusion: A diagnostic challenge. Indian J
Cancer. 47:351–352. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ghoshal AG, Sarkar S, Majumder A and
Chakrabarti S: Unilateral massive pleural effusion: A presentation
of unsuspected multiple myeloma. Indian J Hematol Blood Transfus.
26:62–64. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Nakazato T, Suzuki K, Mihara A, Sanada Y
and Kakimoto T: Refractory plasmablastic type myeloma with multiple
extramedullary plasmacytomas and massive myelomatous effusion:
Remarkable response with a combination of thalidomide and
dexamethasone. Intern Med. 48:1827–1832. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Neuman G and Denekamp Y: Dyspnea and
pleural effusion as presenting clinical manifestations of multiple
myeloma. Isr Med Assoc J. 11:118–119. 2009.PubMed/NCBI
|
|
18
|
Chang H, Chou WC, Lee SY, Huang JY and
Hung YH: Myelomatous pleural effusion in a patient with
plasmablastic myeloma: A case report. Diagn Cytopathol. 37:205–207.
2009. View
Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yokoyama T, Tanaka A, Kato S and Aizawa H:
Multiple myeloma presenting initially with pleural effusion and a
unique paraspinal tumor in the thorax. Intern Med. 47:1917–1920.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kim YJ, Kim SJ, Min K, Kim HY, Kim HJ, Lee
YK and Zang DY: Multiple myeloma with myelomatous pleural effusion:
A case report and review of the literature. Acta Haematol.
120:108–111. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dhingra KK, Singhal N, Nigam S and Jain S:
Unsuspected multiples myeloma presenting as bilateral pleural
effusion-a cytological diagnosis. Cytojournal. 4:172007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Inoue Y, Chua K, McClure RF, Jimenez MC,
Gocke CD, Badros AZ and Takebe N: Multiple myeloma presenting
initially as a solitary pleural effusion later complicated by
malignant plasmacytic ascites. Leuk Res. 29:715–718. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kim YM, Lee KK, Oh HS, Park SK, Won JH,
Hong DS, Park HS, Park JS and Lee DW: Myelomatous effusion with
poor response to chemotherapy. J Korean Med Sci. 15:243–246. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Makino S, Yamahara S, Nagake Y and Kamura
J: Bence-Jones myeloma with pleural effusion: Response to
alpha-interferon and combined chemotherapy. Intern Med. 31:617–621.
1992. View Article : Google Scholar : PubMed/NCBI
|