Introduction
Angiomyofibroblastoma (AMF) is an uncommon, benign
neoplasm that most commonly involves the vulvovaginal region and
may contain scattered fat cells (1–4).
However, AMFs with a prominent fatty component are extremely rare.
To the best of our knowledge, only 16 cases have been reported in
the English literature to date (5–15), and
such tumors have been referred to as ‘lipomatous variants of AMF’
(2,6,9–11,14,15),
which was first termed by Laskin et al (6), or ‘lipomatous AMF’ (7,12,13). We
herein present another pertinent case to expand our understanding
of lipomatous AMF.
Case report
A 49-year-old woman presented to the Japan
Self-Defense Forces Central Hospital (Tokyo, Japan) with a 4-cm,
left vulvar mass and mild associated tenderness. The tumor had been
slowly increasing in size for 1.3 years. Magnetic resonance imaging
examination revealed a benign lipomatous vulvar tumor, a 7.5-cm
uterine leiomyoma and a 1-cm hepatic hemangioma. No other tumors
were found and the serum laboratory data were normal. The patient
underwent simple hysterectomy for uterine leiomyoma and resection
of the vulvar mass and was discharged 1 month after the surgery
without complications.
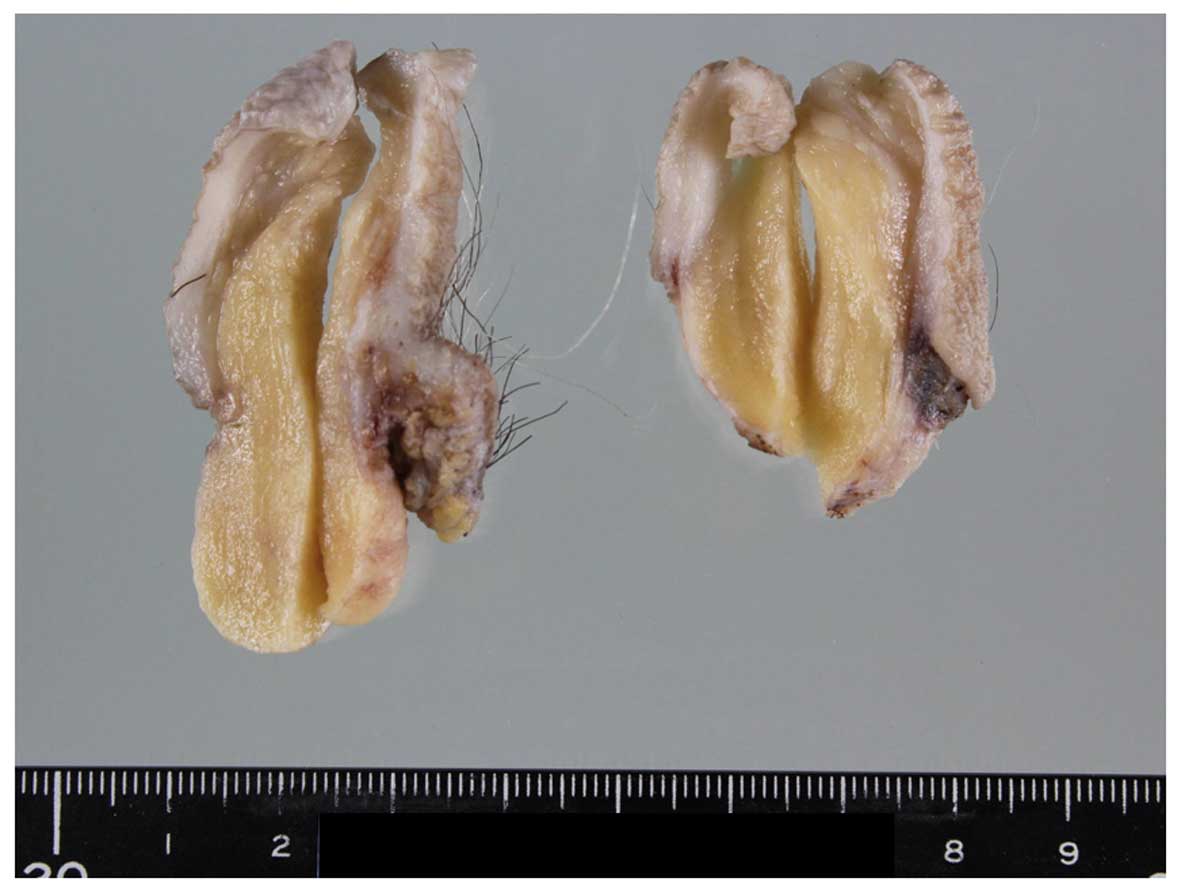
The removed vulvar tumor was a well-demarcated,
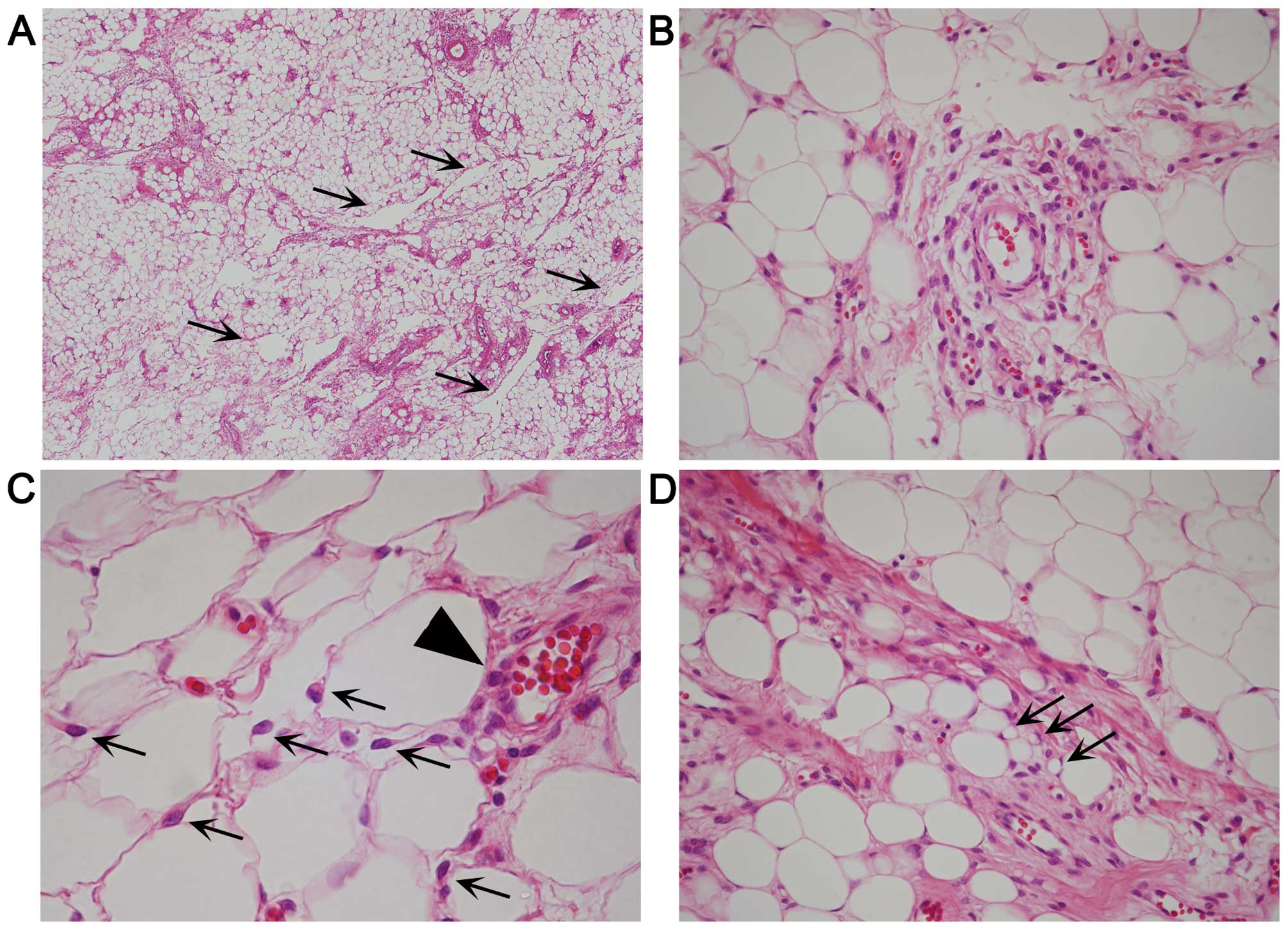
yellowish, solid mass, measuring 5.3×3×2.8 cm (Fig. 1). Histologically, the tumor consisted
of equally distributed abundant fat cells involving ~85% of the
tumor, numerous medium- to small-sized vessels, multifocal fibrous
areas and pseudoangiomatous spaces without cellular lining
(Fig. 2A). No fibrous capsule or
hypocellular myxoid areas were observed. Spindle, rounded, or
epithelioid tumor cells with mildly hyperchromatic ovoid nuclei
proliferated in small nests and/or cords, or singly within the
perivascular fibrous tissue of both fatty and fibrous areas
(Fig. 2B), occasionally adjacent to
the pseudoangiomatous spaces. Similar neoplastic cells were also
singly scattered between fat cells (Fig.
2C), although they were inconspicuous on low-power
magnification. Binucleated tumor cells were occasionally seen.
Mitotic figures were absent. A small number of vacuolated cells
(Fig. 2D) were present neighboring
to tumor cells, but lipoblasts were not identified. Mast cells were
also present near the tumor cells. Immunohistochemically, the tumor
cells were diffusely positive for vimentin, estrogen receptor (ER)
and CD10, but ER-negative and/or CD10-negative tumor cells were
also identified. The tumor cells were focally and weakly positive
for progesterone receptor (PgR) and B-cell lymphoma 2 (Bcl-2), but
were negative for desmin, cytokeratin, epithelial membrane antigen
(EMA), S-100 protein, human melanoma black 45 (HMB45), C-kit and
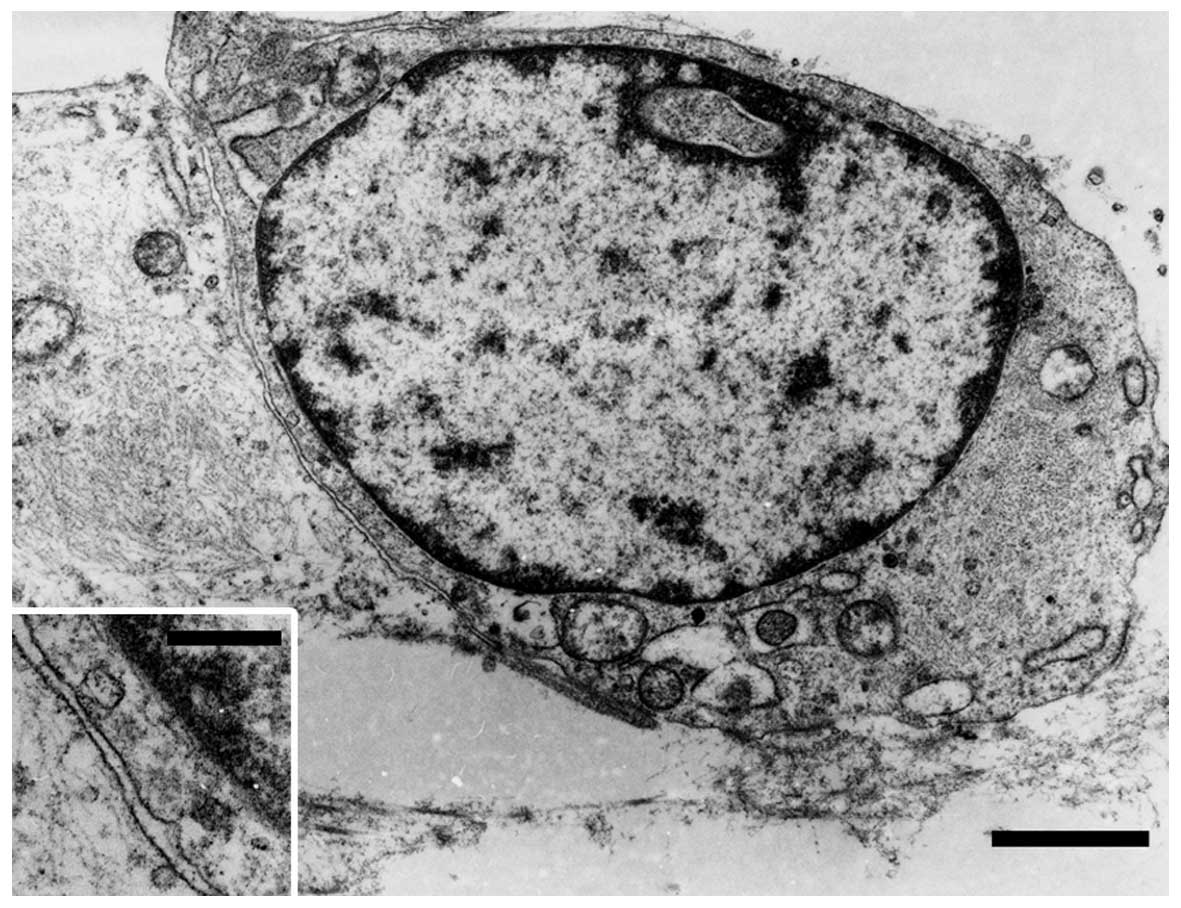
p40. Ultrastructurally, the tumor cells were joined to adjacent
tumor cells without distinct junctional structures. The cytoplasm
of the tumor cells was relatively scarce, but contained rough
endoplasmic reticulum, intermediate filaments, mitochondria,
pinocytotic vesicles (Fig. 3) and
Golgi apparatus. There were no convincing transitional
characteristics between tumor and fat cells.
Discussion
The present tumor was rich in fat cells, and singly
scattered neoplastic cells between the fat cells were difficult to
detect. However, nest- or cord-like growth of rounded and/or
epithelioid tumor cells was identified, mostly in the perivascular
fibrous tissue. Ultrastructurally, the tumor cells displayed
fibroblastic characteristics. These findings are consistent with
those of typical AMF (1–6), and the tumor was diagnosed as
lipomatous AMF. In the present case, pseudoangiomatous
characteristics were observed throughout the tumor, which have not
been mentioned in previous reports of lipomatous AMF (5–15).
However, similar characteristics are known to occur in AMF and
spindle cell lipoma (1,2).
The clinicopathological characteristics of
previously reported cases of lipomatous AMF (5–15) and
the present case are summarized in Table
I. The fatty component ranged from 30 to >90% of the tumor,
apart from 3 cases where the fatty proportion was not mentioned.
Therefore, the term ‘lipomatous’ AMF may be used when the fat cells
constitute ≥30% of the tumor. The tumor size and the patient age
ranged from 1.8 to 11 cm (mean, 5.6 cm) and from 23 to 69 years
(mean, 46.6 years), respectively. Aggressive behavior has not been
reported. Sarcomatous characteristics have rarely been reported in
AMF (16), but never in lipomatous
AMF. Immunohistochemically, the tumor cells were positive for
vimentin (11/11), ER (12/12), Bcl-2 (9/9), PgR (8/9), CD34 (5/12),
desmin (6/14), CD10 (2/4), CD99 (2/3), muscle-specific actin (1/3),
smooth muscle actin (1/9) and S-100 protein (1/10), and negative
for cytokeratin (0/5), EMA (0/5), C-kit (0/4), HMB45 (0/3), glial
fibrillary acidic protein (0/1), CD68 (0/1) and factor VIII (0/1).
In AMF, the tumor cells are strongly and diffusely positive for
desmin, although such positivity may be reduced or absent in
postmenopausal patients (1).
However, excluding cases without distinct information, no desmin
reactivity was observed in 5 (71%) of 7 patients with lipomatous
AMF aged <50 years (8–12,14),
which was unlike the typical AMF characteristics. In the present
case, the tumor cells were also negative for desmin, and the
cytoplasmic intermediate filaments were considered to be
vimentin.
 | Table I.Clinicopathological characteristics of
lipomatous angiomyofibroblastoma. |
Table I.
Clinicopathological characteristics of
lipomatous angiomyofibroblastoma.
| Authors, year | Age
(years)/gender | Location | Tumor size (cm) | % Fat cells | Immunohistochemical
characteristics | Follow-up | (Refs.) |
|---|
| Nielsen et al,
1996 | NAa/F | NAa | NAa | NA (numerous) | NAa | NA | (5) |
| Laskin et al,
1997 | 39/F | Labium majus | 5.5 | >50 | NA | NED/6 years | (6) |
|
| 42/F | Labium majus | 5 | >50 | CD34+
(weak) | NED/6 years |
| Magro et al,
2014 | 58/F | Vulva | 3.2 | 40 | Vim+, desmin-, SMA+,
CD34-, ER+, PgR+, Bcl-2+,
CD99+ | NA | (7) |
| Hiruki et al,
1993 | 39/F | Vulva | 11 | NA (prominent) | Vim+,
desmin+, MSA−, S-100−, factor
VIII− | NA | (8) |
| Shintaku et
al, 2002 | 45/M | Inguinal region | 3.9 | 30 | Vim+,
desmin−, SMA−, S-100−,
CD34+, ER+, PgR-, CD68-, GFAP-, CK-, EMA- | NA | (9) |
| Cao et al,
2005 | 50/F | Vulva | 1.8 | 70–80 | Vim+,
desmin−, MSA−, S-100+ (rare),
CD34+, ER+, PgR+, CK−,
EMA−, Bcl-2+, CD10−,
C-kit− | NA | (10) |
|
| 23/F | Labium | 7.7 | 30–40 | Vim+,
desmin+, MSA+, S-100−,
CD34−, ER+, PgR+, CK−,
EMA−, Bcl-2+, CD10+,
C-kit− | NA |
|
| Lee et al,
2010 | 46/F | Vulva | 4 | NA (several) | Vim+,
desmin−, ER+, PgR+ | NED/7 months | (11) |
| Vora et al,
2011 | 41/F | Labium majus | 2.9 | 60 | Vim+, desmin-, SMA-,
ER+, PgR+ | NED/6 months | (12) |
| Magro et al,
2014 | 56/F | Vulva | 4.5 | 60 | Vim+,
desmin+, SMA−, S-100−,
CD34−, CK−, EMA−,
Bcl-2+, CD10−, C-kit−,
HMB45−, CD99+ | NED/2 years | (13) |
|
| 69/F | Vagina | 7.5 | 60 | Vim+,
desmin+, SMA−, CD34+,
ER+, PgR+, Bcl-2+,
CD99− | NA |
| Upreti et
al, 2015 | 49/F | Labium majus | 6 | 60 | Vim+,
desmin−, SMA−, S-100−,
CD34−, ER+, PgR+,
CD31−, HMB45− | NED/19 months | (14) |
| Luis et al,
2015 | 57/F | Vulva | 12 | >90 | S-100−,
ER+, Βcl-2+; desmin/SMA/CD34, see
commentsb | NA | (15) |
|
| 35/F | Labium | 6 | >90 | S-100−,
ER+, Βcl-2+; desmin/SMA/CD34, see
commentsb | NA |
|
|
| 47/F | Labium | 2.5 | 50 | S-100−,
ER+, Βcl-2+; desmin/SMA/CD34, see
commentsb | NA |
|
| Present case | 49/F | Vulva | 5.3 | 85 | Vim+,
desmin−, SMA−, S-100−,
CD34−, ER+, PgR+, CK−,
EMA−, Bcl-2+, CD10+,
HMB45−, p40− | NED/1 month |
Differential diagnosis of lipomatous AMF includes
spindle cell lipoma, angiomyolipoma and cellular angiofibroma.
Proliferating spindle cells and pseudoangiomatous characteristics
in spindle cell lipoma are similar to those of lipomatous AMF.
However, these tumor cells are usually spindle-shaped only, and do
not form nests. ER positivity has not been reported in spindle cell
lipoma. Angiomyolipoma consists of fat cells and epithelioid or
spindle cells, occasionally in a perivascular arrangement (1,2), which
may mimic lipomatous AMF. However, these epithelioid cells mainly
exhibit smooth muscle configuration, do not usually form nests, and
are consistently positive for HMB45 (1,2). In
addition, the occurrence of spindle cell lipoma and angiomyolipoma
in the vulvovaginal region is extremely rare (1,2,17). These characteristics may help
distinguish lipomatous AMF from spindle cell lipoma and
angiomyolipoma. Cellular angiofibroma was previously referred to as
AMF-like tumor in males, and may contain fat cells (1,2,18). Compared with AMF, in cellular
angiofibroma, the proliferating cells are primarily spindled, the
tumor is more highly cellular, and the proliferating vessels and
stroma are more prominently collagenous and/or hyalinized, although
the spindle cells in cellular angiofibroma may be positive for ER,
PgR, CD34 and desmin (1,2,18–20).
The pathogenesis of lipomatous components within AMF
remains controversial. Some investigators have suggested that
lipomatous components may be due to adipocytic metaplasia or fatty
differentiation of tumor cells (6,7). In the
present case, early fatty-like changes in vacuolated cells were
observed near the tumor cells. However, there were no convincing
transitional characteristics between tumor and fat cells. To
elucidate whether fatty differentiation of tumor cells occurs in
AMF, further investigation is required.
Acknowledgements
The authors would like to thank Yoshiko Uchikoshi
for excellent assistance and Daniel Mrozek for editing the
manuscript.
Glossary
Abbreviations
Abbreviations:
|
AMF
|
angiomyofibroblastoma
|
|
ER
|
estrogen receptor
|
|
PgR
|
progesterone receptor
|
|
EMA
|
epithelial membrane antigen
|
References
|
1
|
Fletcher CDM, Bridge JA, Hogendoorn PCW
and Mertens F: WHO classification of tumours of soft tissue and
bone. 4th. International Agency for Research on Cancer; Lyon:
2013
|
|
2
|
Goldblum JR, Folpe AL and Weiss SW:
Enzinger and Weiss's soft tissue tumors. 6th. Elsevier/Saunders;
Philadelphia, PA: 2014
|
|
3
|
Fletcher CDM, Tsang WYW, Fisher C, Lee KC
and Chan JKC: Angiomyofibroblastoma of the vulva. A benign neoplasm
distinct from aggressive angiomyxoma. Am J Surg Pathol. 16:373–382.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hisaoka M, Kouho H, Aoki T, Daimaru Y and
Hashimoto H: Angiomyofibroblastoma of the vulva: A
clinicopathologic study of seven cases. Pathol Int. 45:487–492.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nielsen GP, Rosenberg AE, Young RH,
Dickersin GR, Clement PB and Scully RE: Angiomyofibroblastoma of
the vulva and vagina. Mod Pathol. 9:284–291. 1996.PubMed/NCBI
|
|
6
|
Laskin WB, Fetsch JF and Tavassoli FA:
Angiomyofibroblastoma of the female genital tract: Analysis of 17
cases including a lipomatous variant. Hum Pathol. 28:1046–1055.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Magro G, Righi A, Caltabiano R, Casorzo L
and Michal M: Vulvovaginal angiomyofibroblastomas: Morphologic,
immunohistochemical, and fluorescence in situ hybridization
analysis for deletion of 13q14 region. Hum Pathol. 45:1647–1655.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hiruki T, Thomas MJ and Clement PB: Vulvar
angiomyofibroblastoma. Am J Surg Pathol. 17:423–424. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shintaku M, Naitou M and Nakashima Y:
Angiomyofibroblastoma-like tumor (lipomatous variant) of the
inguinal region of a male patient. Pathol Int. 52:619–622. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cao D, Srodon M, Montgomery EA and Kurman
RJ: Lipomatous variant of angiomyofibroblastoma: Report of two
cases and review of the literature. Int J Gynecol Pathol.
24:196–200. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lee SJ, Chung YJ, Lee SH, Choi YJ, Kim N,
Son HJ and Yoon JH: Lipomatous variant of angiomyofibroblastoma on
the vulva: A case report. Korean J Obstet Gynecol. 53:851–855.
2010. View Article : Google Scholar
|
|
12
|
Vora S, Gaba ND and Stamatakos MD:
Lipomatous angiomyofibroblastoma: A case report of a unique vulvar
mass. J Reprod Med. 56:347–350. 2011.PubMed/NCBI
|
|
13
|
Magro G, Salvatorelli L, Angelico G,
Vecchio GM and Caltabiano R: Lipomatous angiomyofibroblastoma of
the vulva: Diagnostic and histogenetic considerations. Pathologica.
106:322–326. 2014.PubMed/NCBI
|
|
14
|
Upreti S, Morine A, Ng D and Bigby SM:
Lipomatous variant of angiomyofibroblastoma: A case report and
review of the literature. J Cutan Pathol. 42:222–226. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Luis PP, Quiñonez E, Nogales FF and
McCluggage WG: Lipomatous variant of angiomyofibroblastoma
involving the vulva: Report of 3 cases of an extremely rare
neoplasm with discussion of the differential diagnosis. Int J
Gynecol Pathol. 34:204–207. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Nielsen GP, Young RH, Dickersin GR and
Rosenberg AE: Angiomyofibroblastoma of the vulva with sarcomatous
transformation (“angiomyofibrosarcoma”). Am J Surg Pathol.
21:1104–1108. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Reis-Filho JS, Milanezi F, Soares MF,
Fillus-Neto J and Schmitt FC: Intradermal spindle cell/pleomorphic
lipoma of the vulva: Case report and review of the literature. J
Cutan Pathol. 29:59–62. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Laskin WB, Fetsch JF and Mostofi FK:
Angiomyofibroblastomalike tumor of the male genital tract: Analysis
of 11 cases with comparison to female angiomyofibroblastoma and
spindle cell lipoma. Am J Surg Pathol. 22:6–16. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Iwasa Y and Fletcher CDM: Cellular
angiofibroma: Clinicopathologic and immunohistochemical analysis of
51 cases. Am J Surg Pathol. 28:1426–1435. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Flucke U, van Krieken JH and Mentzel T:
Cellular angiofibroma: Analysis of 25 cases emphasizing its
relationship to spindle cell lipoma and mammary-type
myofibroblastoma. Mod Pathol. 24:82–89. 2011. View Article : Google Scholar : PubMed/NCBI
|