Introduction
Thymic carcinoma is an exceptionally rare tumor,
which has a very poor prognosis, differing from thymoma. Advanced
thymic carcinoma is usually treated with chemotherapy using
cytotoxic agents, such as anthracycline-based regimens, which are
recommended by the National Comprehensive Cancer Network guidelines
(www.nccn.org/professionals/physician_gls/pdf/rectal.pdf).
However, the efficacy of those regimens has not been
satisfactory.
There have been several recent reports on the
presence of an oncogenic driver mutation in thymic carcinoma, such
as a c-kit mutation (1–3). In
adition, the efficacy of molecular-targeted therapy for thymic
carcinoma has been demonstrated in previous case reports (4,5). In the
present case report, a patient with c-kit mutation-positive
thymic carcinoma was successfully treated with two consecutive
c-Kit inhibitors.
Case presentation
A 35-year-old woman with a negative smoking history
was diagnosed with advanced thymic carcinoma with multiple
pulmonary metastases in April, 2011. The tumor was histologically
diagnosed as squamous cell carcinoma. The patient received
chemotherapy with carboplatin plus paclitaxel in May, 2011 and
achieved a partial response. However, a computed tomography (CT)
scan in March, 2012 revealed a relapse of the thymic carcinoma,
with an increase in the size of the primary lesion and the
pulmonary metastases. The patient then underwent treatment with
c-MET and Akt inhibitors, as part of a clinical drug investigation.
Despite treatment, the primary lesion and pulmonary metastases
re-relapsed in March, 2013 after only a short period of stable
disease. A repeat biopsy of the pulmonary metastases was performed
to identify oncogenic driver mutations, such as those involving the
epidermal growth factor receptor, echinoderm microtubule-associated
protein-like 4-anaplastic lymphoma kinase and c-kit genes,
with the aim of identifying other potentially effective
chemotherapies, particularly molecular-targeted therapies.
It was hypothesized that the pulmonary lesions
included a metastatic lesion from the thymic
c-kit-expressing squamous cell carcinoma. This was confirmed
by hematoxylin and eosin staining and immunohistochemistry
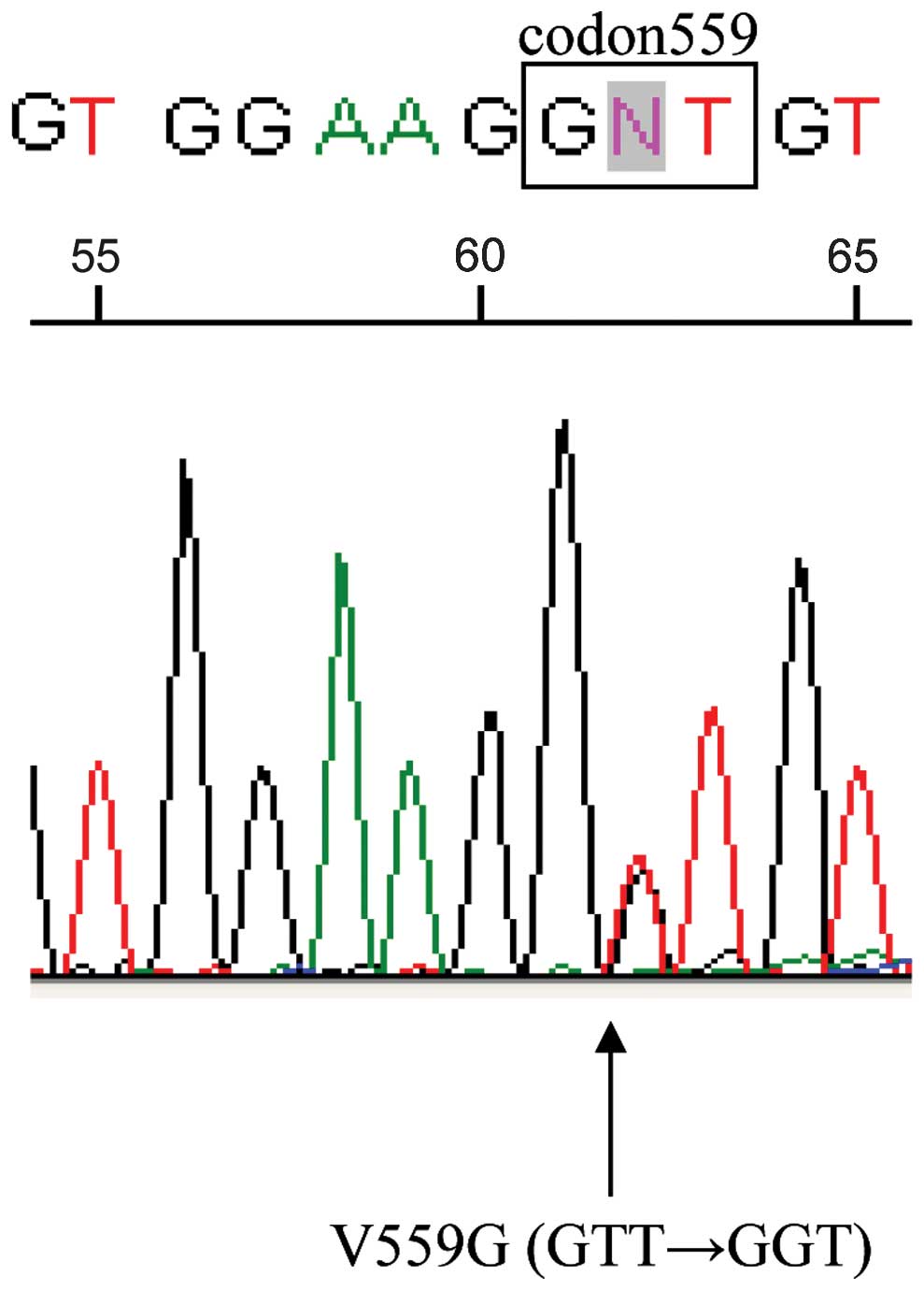
(Fig. 1). Moreover, an active
mutation of c-kit in exon 11 (V559G) was detected in the
pulmonary metastases using the reverse transcription polymerase
chain reaction-invader assay (Fig.
2). No other driver mutations were detected. The patient was
thus treated with imatinib, which is the standard treatment for
gastrointestinal stromal tumors (GISTs).
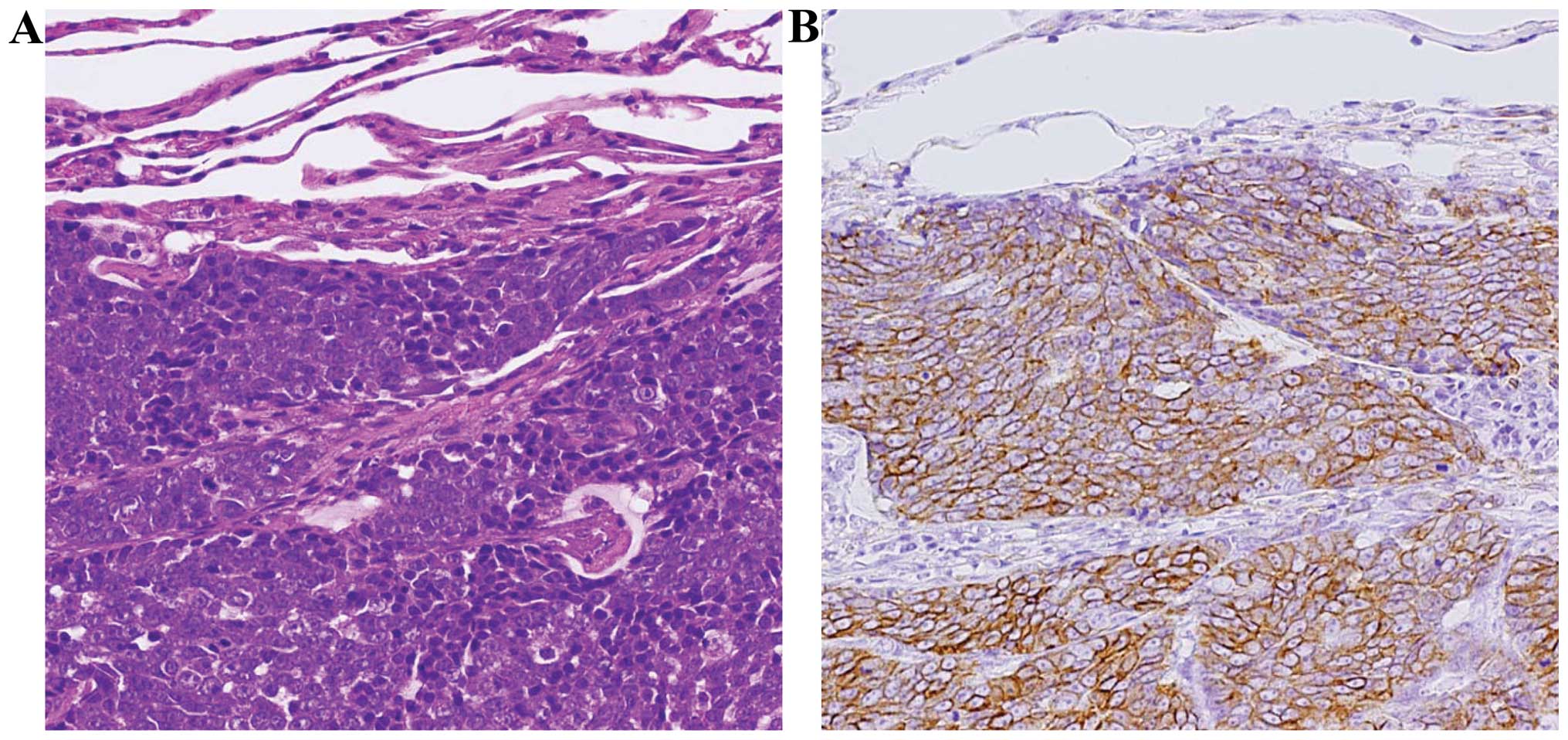 | Figure 1.Histological examination of pulmonary
metastases from the thymic carcinoma. (A) Hematoxylin and eosin
staining (magnification, ×200) and (B) immunohistochemical (IHC)
examination for CD117 (c-Kit; magnification, ×200). The other
results of the IHC examination were as follows (not shown):
CK7+, CK20−, CK903+ (focal),
CD5+ (focal), chromogranin A+,
synaptophysin−, CD56+, CK14/p63+,
TTF-1/NapsinA+ (nuclei), Bcl-2+,
hCG−. CK, cytokeratin; Bcl-2, B-cell lymphoma 2; hCG,
human chorionic gonadotropin; TTF-1, thyroid transcription
factor-1. |
Following treatment with imatinib, which was
initiated in March, 2013, the primary lesion and pulmonary
metastases exhibited a partial response (Fig. 3). Although long-term disease control
was achieved for a period of 21 months, the size of the primary
lesion and pulmonary metastases increased again in November, 2014.
Following failure of imatinib treatment in December, 2014, the
patient was treated with sunitinib, a multiple kinase inhibitor,
which also inhibits c-Kit. A CT scan which was performed following
administration of sunitinib revealed a partial response. In June,
2015, the patients disease had been controlled with sunitinib for a
period of 6 months, and the patient continued to receive sunitinib
treatment, with a good performance status. Therefore, long-term
disease control (~27 months), was achieved with imatinib followed
by sunitinib treatment.
Discussion
Several case reports recently demonstrated the
presence of c-kit mutations in thymic carcinoma (1,2), with
long-term disease control achieved with the c-Kit inhibitor
imatinib (4–6). Simillary, there are several reports on
the use of other molecular-targeted therapies for the treatment of
thymic carcinoma, such as sorafenib and sunitinib (7–10).
Molecular-targeted therapy for thymic carcinoma may only appear to
achieve long-term stable disease. However, the correlation between
oncogenic driver mutations and molecular-targeted agents remains
unclear, with the exception of c-kit mutations (11).
Patients with advanced GISTs determined to be
c-kit mutation-positive are generally treated with imatinib
(12). Following failure and
discontinuation of imatinib, GISTs have been treated with sunitinib
as second-line therapy (13). The
efficacy of these c-Kit inhibitors for c-kit
mutation-positive thymic carcinoma is reported to be similar
(5,14). Therefore, GISTs and c-kit
mutation-positive thymic carcinoma may share a similar background
(15) and, thus, we should discuss
the treatment strategies for thymic carcinoma as a GIST.
The efficacy of consecutive molecular-targeted
therapies for thymic carcinoma was demonstrated in this case.
Therefore, thymic carcinoma with an oncogenic driver mutation
should be treated with molecular-targeted agents rather than with
cytotoxic drugs, and it may be suitable to treat a c-kit
mutation-positive thymic carcinoma as a mediastinal GIST.
References
|
1
|
Yoh K, Nishiwaki Y, Ishii G, Goto K,
Kubota K, Ohmatsu H, Niho S, Nagai K and Saijo N: Mutational status
of EGFR and KIT in thymoma and thymic carcinoma. Lung Cancer.
62:316–320. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Petrini I, Zucali PA, Lee HS, Pineda MA,
Meltzer PS, Walter-Rodriguez B, Roncalli M, Santoro A, Wang Y and
Giaccone G: Expression and mutational status of c-kit in thymic
epithelial tumors. J Thorac Oncol. 5:1447–1453. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Aisner SC, Dahlberg S, Hameed MR, Ettinger
DS, Schiller JH, Johnson DH, Aisner J and Loehrer PJ: Epidermal
growth factor receptor, C-kit and Her2/neu immunostaining in
advanced or recurrent thymic epithelial neoplasms staged according
to the 2004 World Health Organization in patients treated with
octreotide and prednisone: An Eastern Cooperative Oncology Group
study. J Thorac Oncol. 5:885–892. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ströbel P, Hartmann M, Jakob A, Mikesch K,
Brink I, Dirnhofer S and Marx A: Thymic carcinoma with
overexpression of mutated KIT and the response to imatinib. N Engl
J Med. 350:2625–2626. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Buti S, Donini M, Sergio P, Garagnani L,
Schirosi L, Passalacqua R and Rossi G: Impressive response with
imatinib in a heavily pretreated patient with metastatic c-KIT
mutated thymic carcinoma. J Clin Oncol. 29:e803–e805. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hamada S, Masago K, Mio T, Hirota S and
Mishima M: Good clinical response to imatinib mesylate in atypical
thymic carcinoid with KIT overexpression. J Clin Oncol. 29:e9–e10.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Disel U, Oztuzcu S, Beşen AA, Karadeniz C,
Köse F, Sümbül AT, Sezer A, Nursal GN, Abalı H and Ozyılkan O:
Promising efficacy of sorafenib in a relapsed thymic carcinoma with
C-KIT exon 11 deletion mutation. Lung Cancer. 71:109–112. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Li XF, Chen Q, Huang WX and Ye YB:
Response to sorafenib in cisplatin-resistant thymic carcinoma: A
case report. Med Oncol. 26:157–160. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Thomas A, Rajan A, Berman A, Tomita Y,
Brzezniak C, Lee MJ, Lee S, Ling A, Spittler AJ, Carter CA, et al:
Sunitinib in patients with chemotherapy-refractory thymoma and
thymic carcinoma: An open-label phase 2 trial. Lancet Oncol.
16:177–186. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Neuhaus T and Luyken J: Long lasting
efficacy of sorafenib in a heavily pretreated patient with thymic
carcinoma. Target Oncol. 7:247–251. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pagano M, Sierra NM, Panebianco M, Rossi
G, Gnoni R, Bisagni G and Boni C: Sorafenib efficacy in thymic
carcinomas seems not to require c-KIT or PDGFR-alpha mutations.
Anticancer Res. 34:5105–5110. 2014.PubMed/NCBI
|
|
12
|
Demetri GD, von Mehren M, Blanke CD, Van
den Abbeele AD, Eisenberg B, Roberts PJ, Heinrich MC, Tuveson DA,
Singer S, Janicek M, et al: Efficacy and safety of imatinib
mesylate in advanced gastrointestinal stromal tumors. N Engl J Med.
347:472–480. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Demetri GD, van Oosterom AT, Garrett CR,
Blackstein ME, Shah MH, Verweij J, McArthur G, Judson IR, Heinrich
MC, Morgan JA, et al: Efficacy and safety of sunitinib in patients
with advanced gastrointestinal stromal tumour after failure of
imatinib: A randomised controlled trial. Lancet. 368:1329–1338.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lim SH, Lee JY, Sun JM, Kim KM, Ahn JS,
Ahn MJ and Park K: A new KIT gene mutation in thymic cancer and a
promising response to imatinib. J Thorac Oncol. 8:e91–e92. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rossi V, Donini M, Sergio P, Passalacqua
R, Rossi G and Buti S: When a thymic carcinoma ‘becomes’ a GIST.
Lung Cancer. 80:106–108. 2013. View Article : Google Scholar : PubMed/NCBI
|