Introduction
Lung cancer is the most common cause of
cancer-associated mortality worldwide (1). Multiple primary lung cancer (MPLC) is
rare (2), ranging between 0.2 and 20%
(3), which has ≥2 primary lung
cancers with different pathological types (4). Two manifestations of MPLC exist:
Metachronous or synchronous, and depending on which, their
morphology and histology are similar (5). To distinguish MPLC from metastatic
cancer in the lung or recurrence is difficult, however, it is of
great significance for therapeutic management and prognosis. The
diagnosis of MPLC not only depends on biopsy pathology, but also
often requires molecular biology techniques, including DNA polity,
gene mutations and microsatellite alteration (6–9). The
present study reported a case of primary non-small cell lung cancer
(NSCLC) in the left lobe and synchronous small cell lung cancer
(SCLC) in the right lung lobe. The patient with synchronous MPLC
tolerated two cycles of a chemotherapy regimen that consisted of
etoposide (100 mg/m2 of body-surface area) from one to
three days and nedaplatin (75 mg/m2 of body-surface
area) on day one. The patient exhibited a favorable response,
including loss of the dry cough and a reduction in the two lesions,
observed by chest computed tomography (CT) during follow-up.
Case study
A 66-years-old male was referred to the Department
of Respiratory Disease at Yijishan Hospital of Wannan Medical
College (Wuhu, China) in April 2015 with a dry cough accompanied
with blood in phlegm over the previous 1 month. The previous
medical history of the patient was uneventful, with the exception
of a 40 pack/year history of smoking. Physical examination revealed
a rough respiratory murmur in each lung. Laboratory findings were
within normal limits, with the exception of prostate special
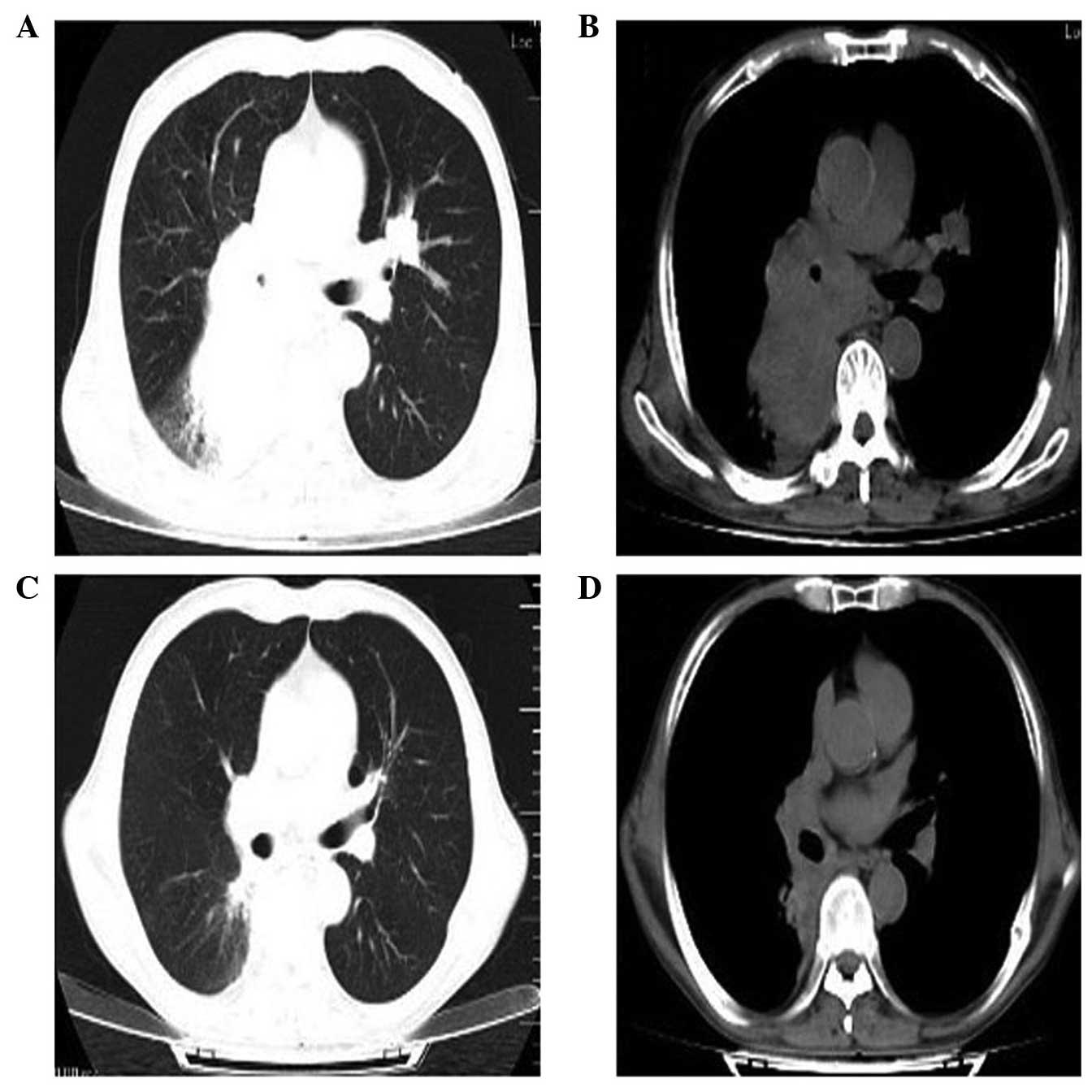
antigen (PSA) at 5.35 ng/ml. Chest CT images obtained in April 2015
revealed an irregular soft-tissue mass with a 9.6 cm maximum
diameter, internal uniformity density in the middle-low right lobe
close to pulmonary hilum, and a nodular high-density shadow with a
2.5 cm maximum diameter that was a lobulated lesion in the left
upper lobe (Fig. 1A and B). The
patient was positive for metastasis to the mediastinal lymph node.
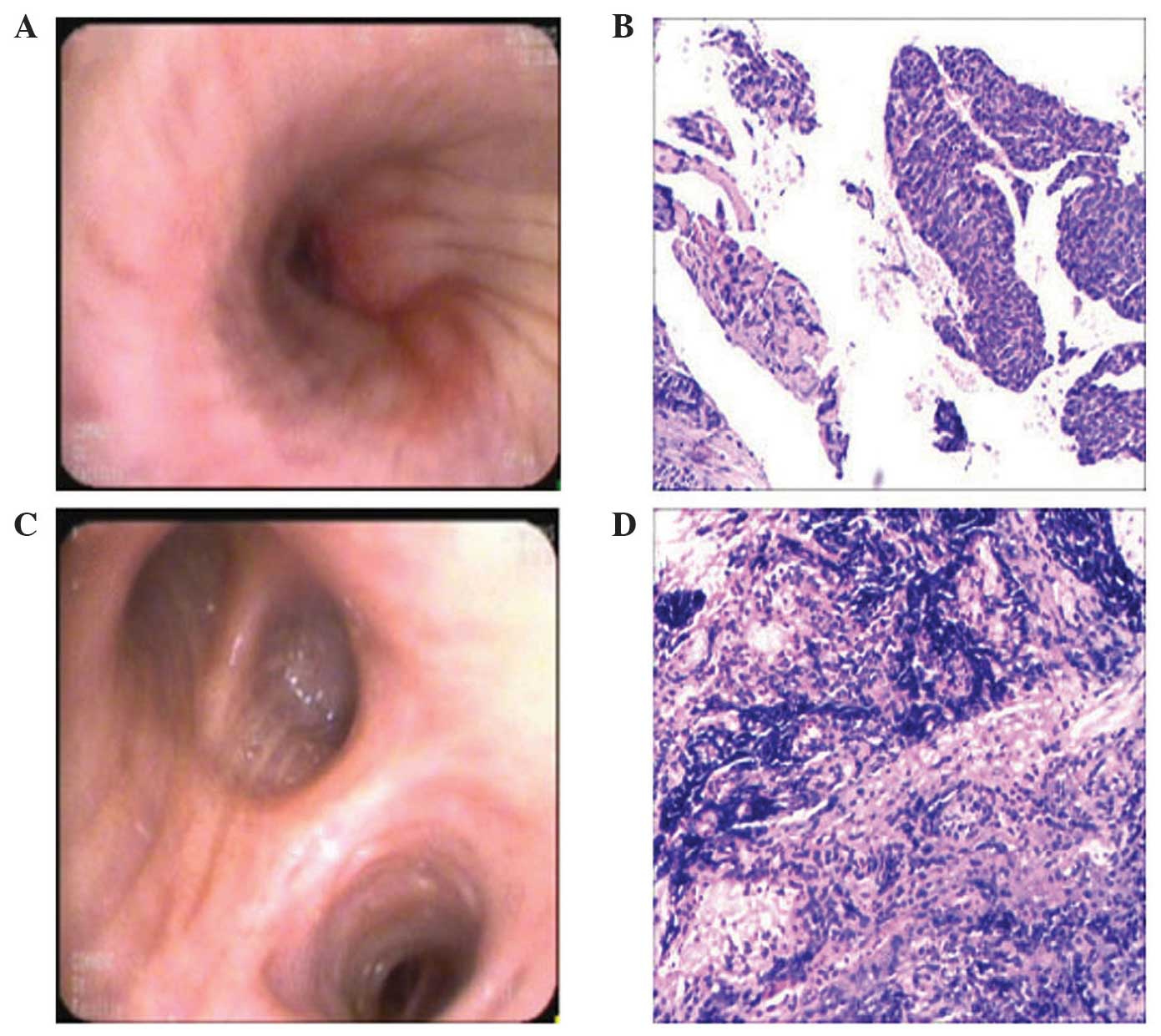
Fiber bronchoscopic biopsy was performed a few days later, which
revealed squamous cell carcinoma in the left lobe and SCLC in the
right lobe (Fig. 2).
Immunohistochemical staining of SCLC revealed a marked positivity
for AE1/AE3, Syn, cluster of differentiation 56, thyroid
transcription factor-1, p63 (few), Ki-67 (80%) and EMA. By
contrast, the SCLC was negative for CgA(−), NapsinA and p40. The
patient refused gene detection of squamous cell carcinoma in the
left lobe due to expense. The patient tolerated two cycles of a
chemotherapy regimen that consisted of etoposide (100
mg/m2 of body-surface area) from 1–3 days and nedaplatin
(75 mg/m2 of body-surface area) on day 1. The patient
exhibited a favorable response, including reduction in the dry
cough, and reduction of the two lesions in the chest CT performed
during follow-up (Fig. 1C and D). A
limitation of the present case report is that only two cycles of
etopiside combined with nedaplatin were administered in May and
June 2015. The treatment with chemotherapy was interrupted due to
the large expenditure.
Discussion
The present study reported an uncommon case of a
66-year-old male patient diagnosed with MPLC. Fiber bronchoscopy
pathological biopsy revealed two completely different pathological
types, which were squamous cell lung carcinoma in the left lobe and
SCLC in the right lobe. The patient tolerated two cycles of a
chemotherapy regimen that consisted of etoposide (100
mg/m2 of body-surface area) from 1–3 days and nedaplatin
(75 mg/m2 of body-surface area) on day 1. The patient
had a favorable response, including loss of the dry cough and
reduction in the two lesions observed by chest CT during the
follow-up.
To the best of our knowledge, MPLC is a special type
of primary lung carcinoma occurring in one or both lung lobes,
which may be ≥2 different pathological types (4). Two manifestations in MPLC exist:
Metachronous or synchronous, and depending on which, their
morphology and histology are similar (5). The mechanism of the MPLC remains to be
fully understood, and only a few studies have addressed that it may
be associated with field cancerization (10,11). Chang
et al (12) reported the links
between MPLC, and the epidermal growth factor receptor (EGFR) and
p53 genes. Somatic alterations in EGFR were demonstrated, which can
not only greatly improve the clonality assessment, but also affect
the management of patients with MPLC. In addition, it is of
significance to distinguish MPLC from metastatic carcinoma in the
lung for the management and prognosis. The incidence of MPLC is
attributed to the development of higher-resolution chest imaging
techniques, positron emission computed tomography-CT, fiber
bronchoscopy biopsy and percutaneous lung biopsy by CT fluoroscopy.
The initial diagnostic criteria were established in 1975 by Martin
and Melamed (4), and were updated by
the American College of Chest Physicians (ACCP) (13). Different pathological categories is of
great importance for the identification of MPLC (14). However, following the Martin-Melamed
and ACCP criteria only distinguish certain MPLC types from
metastases. Girard et al (7)
confirmed that 3/7 patents with paired adenocarcinoma exhibited
multiple primary lung tumors by means of EGFR/KRAS mutation
testing. When it comes to similar pathological types, MPLC can be
confirmed by means of DNA polity, gene mutations and microsatellite
alteration (6–9,15,16). No standard guidelines exist for the
management of MPLC. However, the current case demonstrated a few
important principles. SCLC generally exhibits a higher growth
fraction, a more rapid doubling time and earlier development of
widespread metastases when compared with NSCLC (17). SCLC is highly sensitive to initial
chemotherapy, particularly in the most common regimen (etoposide
plus cisplatin), which can provide symptomatic improvement and
prolonged survival (18,19). However, Veronesi et al
(20) indicated that outcomes
following surgery in patients with early SCLC were comparable to
those in patients with NSCLC. The patient with an enlarged
mediastinal lymph node exhibited squamous carcinoma combined with
SCLC, therefore, that chemotherapy with etoposide and nedaplatin
was performed. Therefore, if an MPLC patient is confirmed with
synchronous SCLC and NSCLC, the appropriate chemotherapy regimen
must be selected as quickly as possible.
In conclusion, the present study reported a case of
MPLC with simultaneous SCLC and NSCLC. The management of patients
with MPLC requires highly individualized treatment plans that are
dissimilar to standard practices in the setting of a single tumor.
Consideration must be given to the chemotherapy regimen that
improve symptoms and prolongs survival.
Acknowledgements
The authors would like to thank Renguang Pei
(Department of Interventional Therapy, Yijishan Hospital of Wannan
Medical College, Wuhu, China) for providing assistance with writing
and organization of this manuscript.
References
|
1
|
Jemal A, Siegel R, Ward E, Murray T, Xu J,
Smigal C and Thun MJ: Cancer statistics, 2006. CA Cancer J Clin.
56:106–130. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Detterbeck FC, Postmus PE and Tanoue LT:
The stage classification of lung cancer: Diagnosis and management
of lung cancer, 3rd ed: American college of chest physicians
evidence-based clinical practice guidelines. Chest. 143(5 Suppl):
e191S–e210S. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Rea F, Zuin A, Callegaro D, Bortolotti L,
Guanella G and Sartori F: Surgical results for multiple primary
lung cancers. Eur J Cardiothorac Surg. 20:489–495. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Martini N and Melamed MR: Multiple primary
lung cancers. J Thorac Cardiovasc Surg. 70:606–612. 1975.PubMed/NCBI
|
|
5
|
Riquet M, Cazes A, Pfeuty K, Ngabou UD,
Foucault C, Dujon A and Banu E: Multiple lung cancers prognosis:
What about histology. Ann Thorac Surg. 86:921–926. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Arai J, Tsuchiya T, Oikawa M, Mochinaga K,
Hayashi T, Yoshiura K, Tsukamoto K, Yamasaki N, Matsumoto K,
Miyazaki T and Nagayasu T: Clinical and molecular analysis of
synchronous double lung cancers. Lung Cancer. 77:281–287. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Girard N, Ostrovnaya I, Lau C, Park B,
Ladanyi M, Finley D, Deshpande C, Rusch V, Orlow I, Travis WD, et
al: Genomic and mutational profiling to assess clonal relationships
between multiple non-small cell lung cancers. Clin Cancer Res.
15:5184–5190. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Girard N, Deshpande C, Azzoli CG, Rusch
VW, Travis WD, Ladanyi M and Pao W: Use of epidermal growth factor
receptor/Kirsten rat sarcoma 2 viral oncogene homolog mutation
testing to define clonal relationships among multiple lung
adenocarcinomas: Comparison with clinical guidelines. Chest.
137:46–52. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shen C, Xu H, Liu L, Zhou Y, Chen D, Du H,
Han Z and Che G: ‘Unique trend’ and ‘contradictory trend’ in
discrimination of primary synchronous lung cancer and metastatic
lung cancer. BMC Cancer. 13:4672013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pasic A, Vonk-Noordegraaf A, Risse EK,
Postmus PE and Sutedja TG: Multiple suspicious lesions detected by
autofluorescence bronchoscopy predict malignant development in the
bronchial mucosa in high risk patients. Lung Cancer. 41:295–301.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Braakhuis BJ, Tabor MP, Kummer JA, Leemans
CR and Brakenhoff RH: A genetic explanation of Slaughter's concept
of field cancerization: Evidence and clinical implications. Cancer
Res. 63:1727–1730. 2003.PubMed/NCBI
|
|
12
|
Chang YL, Wu CT, Lin SC, Hsiao CF, Jou YS
and Lee YC: Clonality and prognostic implications of p53 and
epidermal growth factor receptor somatic aberrations in multiple
primary lung cancers. Clin Cancer Res. 13:52–58. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kozower BD, Larner JM, Detterbeck FC and
Jones DR: Special treatment issues in non-small cell lung cancer:
Diagnosis and management of lung cancer, 3rd ed: American college
of chest physicians evidence-based clinical practice guidelines.
Chest. 143(5 Suppl): e369S–e399S. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shen C, Wang X, Tian L, Zhou Y, Chen D, Du
H, Wang W, Liu L and Che G: ‘Different trend’ in multiple primary
lung cancer and intrapulmonary metastasis. Eur J Med Res.
20:172015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ono K, Sugio K, Uramoto H, Baba T, Ichiki
Y, Takenoyama M, Hanagiri T, Oyama T and Yasumoto K: Discrimination
of multiple primary lung cancers from intrapulmonary metastasis
based on the expression of four cancer-related proteins. Cancer.
115:3489–3500. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chen D, Mei L, Zhou Y, Shen C, Xu H, Niu Z
and Che G: A novel differential diagnostic model for multiple
primary lung cancer: Differentially-expressed gene analysis of
multiple primary lung cancer and intrapulmonary metastasis. Oncol
Lett. 9:1081–1088. 2015.PubMed/NCBI
|
|
17
|
Kalemkerian GP, Akerley W, Bogner P,
Borghaei H, Chow LQ, Downey RJ, Gandhi L, Ganti AK, Govindan R,
Grecula JC, et al: Small cell lung cancer. J Natl Compr Canc Netw.
11:78–98. 2013.PubMed/NCBI
|
|
18
|
Hann CL and Rudin CM: Management of
small-cell lung cancer: Incremental changes but hope for the
future. Oncology (Williston Park). 22:1486–1492. 2008.PubMed/NCBI
|
|
19
|
Jackman DM and Johnson BE: Small-cell lung
cancer. Lancet. 366:1385–1396. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Veronesi G, Bottoni E, Finocchiaro G and
Alloisio M: When is surgery indicated for small-cell lung cancer.
Lung Cancer. 90:582–589. 2015. View Article : Google Scholar : PubMed/NCBI
|