Introduction
Renal calyx carcinoma (RCXC) is a novel concept,
which is defined by Williams et al (1) as carcinoma developing primarily from the
renal calyx. Recent advances in endourologic techniques have
resulted in increased popularity of endoscopic management of upper
tract urothelial carcinoma (UC) (2–4). To the
best of our knowledge, no previous reports have presented treatment
of RCXC patients with nephron-sparing endoscopic surgery. The
present study reported the use of a flexible ureteroscopic strategy
for the resection of RCXC with a thulium laser in an 81-year-old
female presenting with a 1-year history of intermittent painless
gross hematuria.
Case report
An 81-year-old female presented at hospital with
intermittent painless gross hematuria and was treated with oral
antibiotics for 1 week; the gross hematuria subsequently resolved.
At ~1-year later, the patient again presented at the same hospital
with painless gross hematuria. Four days later, the patient came to
the Emergency Department, Xuanwu Hospital (Beijing, China)
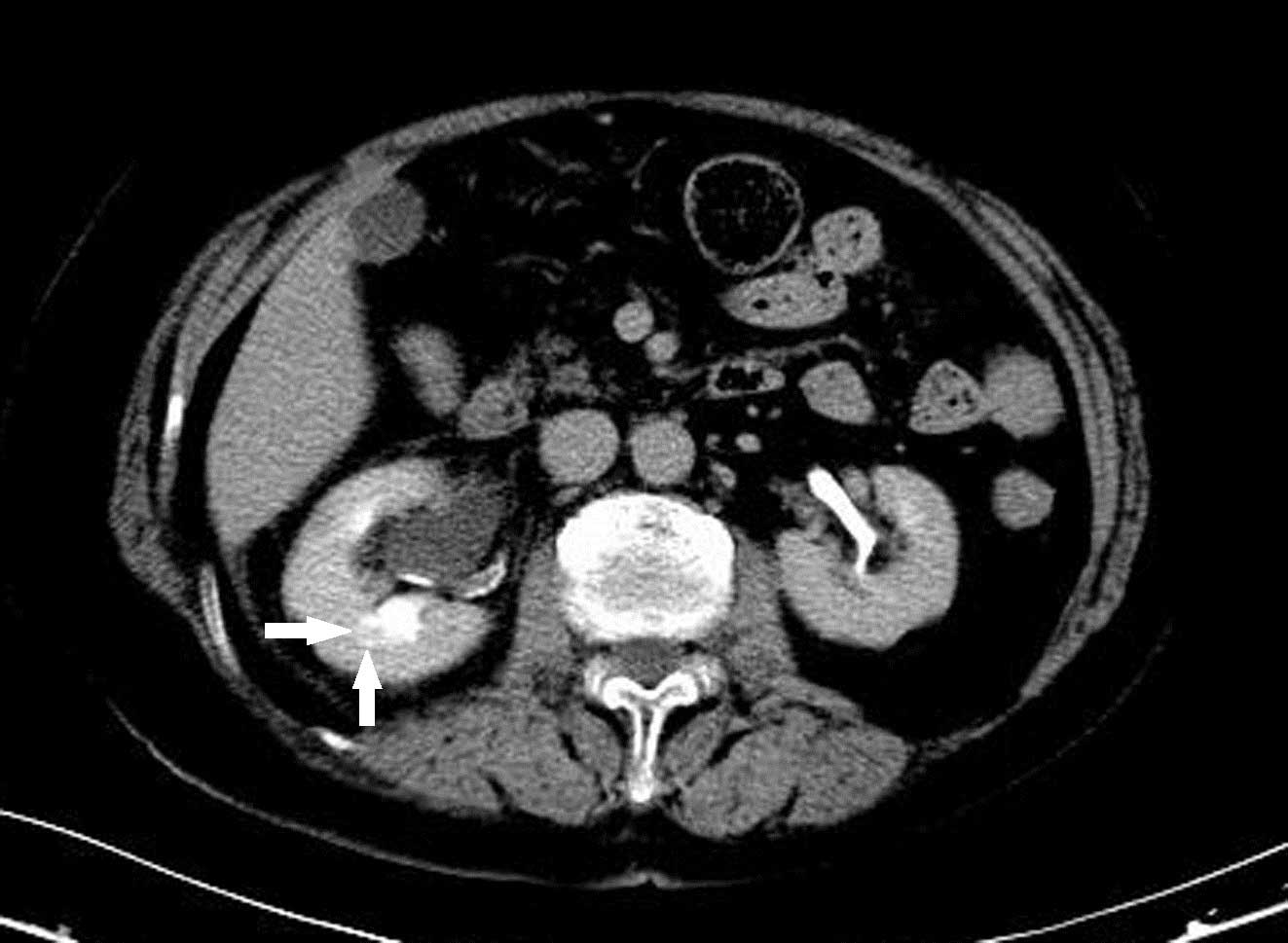
complaining of acute pain in the right waist and back. Urinary
tract ultrasound and contrast-enhanced urinary tract computed
tomography (CT) revealed hydronephrosis of the right upper urinary
tract. No stone was observed on X-ray or CT, however, CT revealed a
small suspicious mass in the lower calyx of the right kidney
(Fig. 1). Furthermore, the patient
underwent cystoscopy, and no evidence of bladder carcinoma or stone
was found. However, the urine ejected from the right ureteral
orifice was noted to have a reddish tint compared with the left
ureteral orifice. Renal function tests revealed a blood creatinine
of 114 µmol/l, right renal glomerular filtration rate (GFR) of 32.6
ml/min and left renal GFR of 21.7 ml/min. No evidence of metastasis
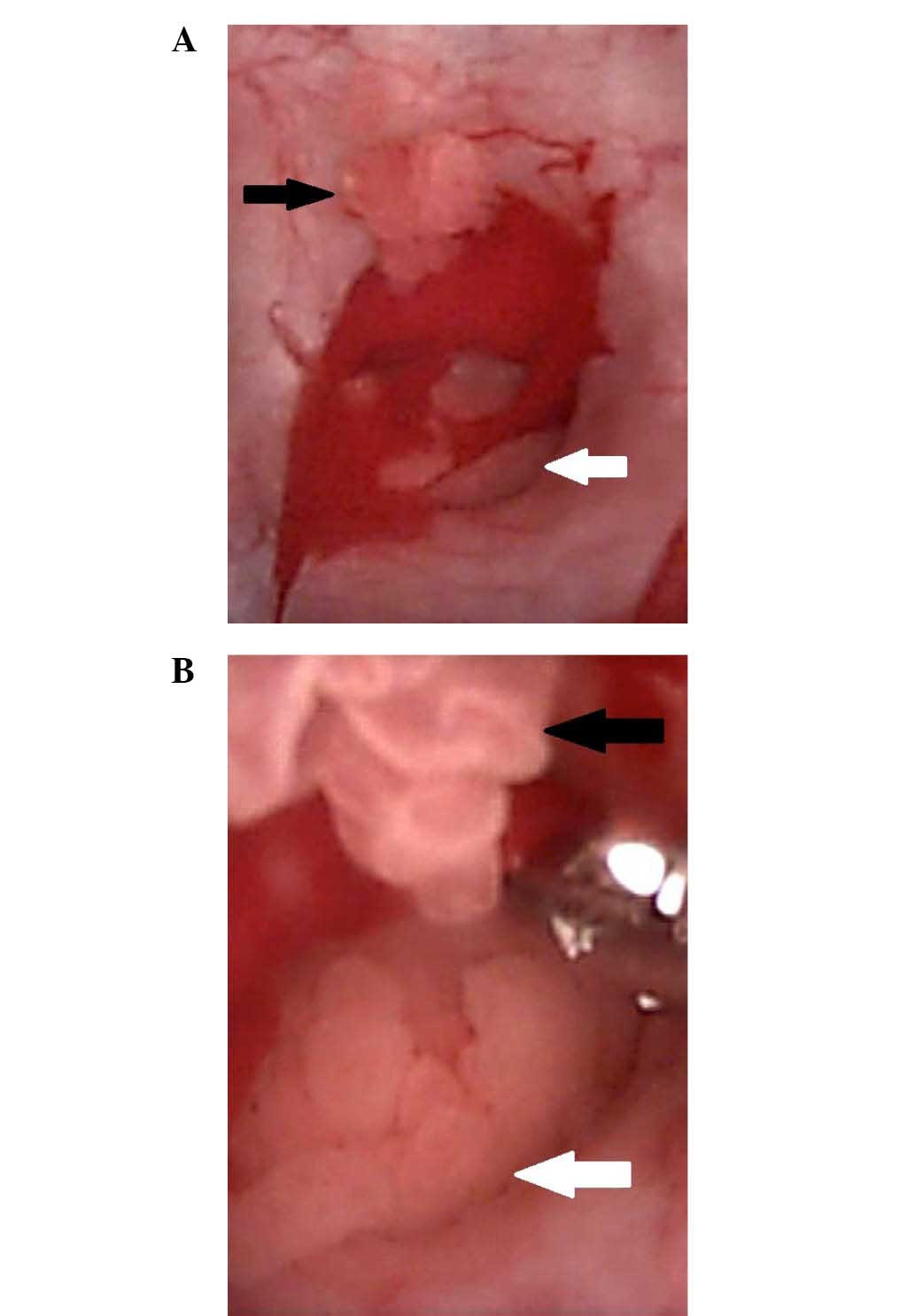
were observed on the bone scan and chest X-ray. At 6 days later,
the patient underwent a flexible ureteroscopic examination
performed under general anesthesia, and a 9 mm tumor with an
epicenter in the lower renal calyx of the right kidney was
detected, along with additional small lesions around the calyx
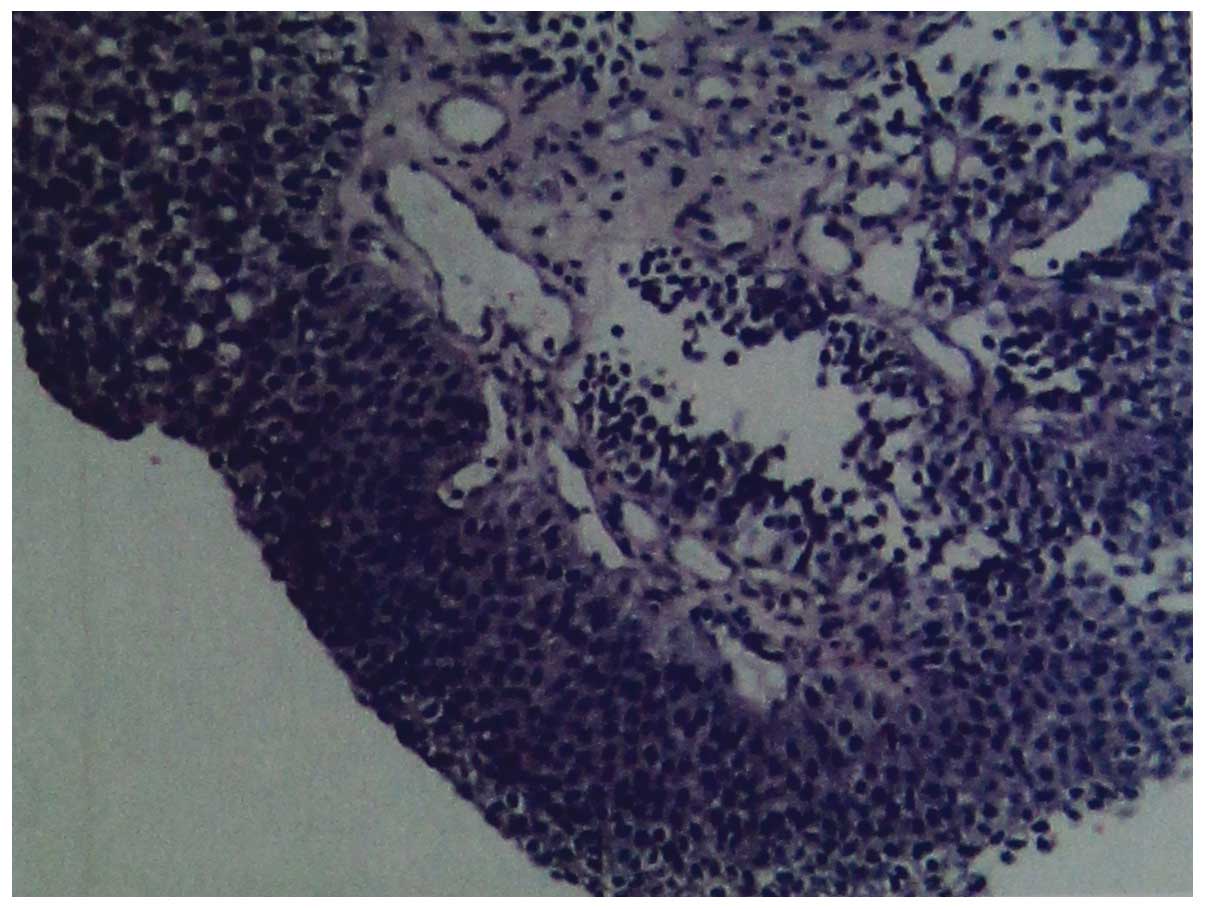
(Fig. 2). Biopsies were obtained and
sent for pathological examination, which revealed low-grade UC
(Fig. 3). Following discussions with
the patient and her family, particularly with regards to other
co-morbidities, including renal insufficiency, coronary heart
disease, hypertension, diabetes and advanced-age, it was decided to
proceed with endoscopic management using thulium laser.
At 4 days after the initial ureteroscopy, the
patient underwent endoscopic resection of the RCXC under general
anesthesia with flexible ureteroscopy in the lithotomy position.
The laser energy setting was set to 9 w, and saline was used for
irrigation. Following entering the pelviureteric junction, the
ureteroscope was carefully guided to the mass in the lower calyx of
the right kidney using pre-operative CT imaging. Subsequently, the
thulium laser was utilized to firstly ablate the margins of the
renal sinus fat. Next, the entire tumor was resected to a depth of
4 mm using laser fulguration. The wound was irrigated with 100 ml
of 0.1 mg/ml epirubicin in saline, followed by irrigation with 500
ml distilled water. The other calyxes were examined using flexible
ureteroscopy to confirm that no tissue was left behind. Finally, a
4.7-Fr double J ureteral stent was placed in the right urinary
tract. The total surgery duration was 66 min. The double J ureteral
stent was removed 1-month later and no recurrence was detected at
the 6-month follow-up.
Discussion
The collecting duct and the urothelium of the upper
urinary tract system share similar embryological origins (5). However, the histopathological features
of UC of the renal pelvis and collecting duct carcinoma (CDC) are
quite different. Williams et al (1) were the first to present the concept of
RCXC in 2013. RCXC can be either CDC or UC of the renal pelvis, and
compared with traditionally defined upper tract urothelial
carcinomas, RCXC has a locally aggressive behavior, which may limit
its spread into the urothelium of the urinary tract (1). However, traditional imaging techniques
and rigid ureteroscopic examinations typically fail to detect such
lesions in the early stage (6).
Although traditional radical nephroureterectomy with
bladder cuff excisions remains the gold standard surgical treatment
for upper tract urothelial carcinoma (UTUC) (4), this procedure may result in morbidity
and loss of nephron units (3). As
endourologic techniques have developed further, nephron-sparing
procedures (NSPs) have become the first-line management strategy
for selected patients with low grade UTUC and are feasible to
complete resection or fulguration. Management with NSPs consists of
ureteroscopic or percutaneous approaches (4), and the technical feasibility and safety
of the NSPs have been shown in several previous studies (3,7). Potential
candidates for NSPs include those with low risk UTUC who have a
normal contralateral kidney or those patients with serious
comorbidities (i.e. patients with a solitary kidney or renal
insufficiency) (4). In the present
study, the patient's bilateral renal GFR was 54.3 ml/min, which is
indicative of renal insufficiency. In addition, the diameter of the
tumor was ~9 mm and the lesion was located in a renal calyx with
limited involvement of the surrounding renal pelvis urothelium, and
the histopathological findings revealed low-grade urothelial
carcinoma. All of these features were consistent with UTUC that is
low-risk. Following communication with the patient and her family,
a conservative endoscopic surgical approach followed by long-term
endoscopic surveillance was selected.
Previously, several adjuvant topical agents,
including Bacillus Calmette-Guérin (BCG), mitomycin C, epirubicin
and thiotepa, have been used for UTUC perfusion treatment (4,8). Benefits
of the antegrade perfusion with BCG in patients with UTUC following
ablation of early stage tumors has also been demonstrated (8). Nonetheless, certain controversy remains
regarding the safety and efficacy of retrograde instillations,
which may cause pyelovenous influx and ureteric obstruction during
perfusion (4). However, in the
present case, the entire operation was performed using flexible
ureteroscopy, and it was not believed to be worthwhile to make
additional incisions to enable antegrade perfusion. Therefore, the
present study selected retrograde perfusion with epirubicin
immediately following the resections. Following perfusion with
epirubicin, distilled water was used to wash the renal pelvis and
flexible ureteroscopy was used to check that no residual tissue
remained in other renal calyces.
In conclusion, flexible ureteroscopy with thulium
laser is a novel nephron sparing endoscopic treatment for primary
carcinoma of renal calyx. This procedure is feasible for select
patients who are willing to undergo long-term endoscopic
surveillance as follow-up.
References
|
1
|
Williams PA and Mai KT: Primary carcinoma
of renal calyx. Pathol Res Pract. 209:654–661. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rouprêt M, Traxer O, Tligui M, Conort P,
Chartier-Kastler E, Richard F and Cussenot O: Upper urinary tract
transitional cell carcinoma: Recurrence rate after percutaneous
endoscopic resection. Eur Urol. 51:709–713; discussion 714. 2013.
View Article : Google Scholar
|
|
3
|
Yakoubi R, Colin P, Seisen T, Léon P,
Nison L, Bozzini G, Shariat SF and Rouprêt M: Radical
nephroureterectomy versus endoscopic procedures for the treatment
of localised upper tract urothelial carcinoma: A meta-analysis and
a systematic review of current evidence from comparative studies.
Eur J Surg Oncol. 40:1629–1634. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rouprêt M, Babjuk M, Compérat E, Zigeuner
R, Sylvester RJ, Burger M, Cowan NC, Böhle A, Van Rhijn BW,
Kaasinen E, et al: European Association of Urology Guidelines on
Upper Urinary Tract Urothelial Cell Carcinoma: 2015 Update. Eur
Urol. 68:868–879. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bohnenpoll T and Kispert A: Ureter growth
and differentiation. Semin Cell Dev Biol. 36:21–30. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yamany T, van Batavia J, Ahn J, Shapiro E
and Gupta M: Ureterorenoscopy for upper tract urothelial carcinoma:
How often are we missing lesions? Urology. 85:311–315. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hoffman A, Yossepowitch O, Erlich Y,
Holland R and Lifshitz D: Oncologic results of nephron sparing
endoscopic approach for upper tract low grade transitional cell
carcinoma in comparison to nephroureterectomy-a case control study.
BMC Urol. 14:972014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Giannarini G, Kessler TM, Birkhäuser FD,
Thalmann GN and Studer UE: Antegrade perfusion with bacillus
Calmette-Guerin in patients with non-muscle-invasive urothelial
carcinoma of the upper urinary tract: Who may benefit? Eur Urol.
60:955–960. 2011. View Article : Google Scholar : PubMed/NCBI
|