Introduction
Technological improvements in the field of medical
imaging, including mammography, ultrasonography and magnetic
resonance imaging (MRI), have markedly enhanced the accuracy for
breast cancer diagnosis in the early stage (1–3). However,
false-positive and false-negative diagnosis of breast cancer based
on imaging remains (4,5). Therefore, intraoperative frozen section
diagnosis has a vital role in guiding appropriate therapeutic
decision making for breast carcinoma patients and is widely used in
the clinic (6,7). However, due to reasons such as poor
quality of frozen sections, incorrect sampling procedures and
limited experience of pathologists, the average accuracy of
diagnoses based on intraoperative frozen pathology was 92.6–98.0%
(8). Misdiagnosis based on
intraoperative frozen pathology may lead to the selection of an
inappropriate breast surgical procedure, resulting in incomplete
tumor resection or unnecessary removal of the whole breast.
False-negative cases require a second surgery as
soon as possible in order to remove the residual tumor and ensure
tumor-free surgical margins. Prior to the second surgery, the
detailed condition of the postoperative breast must be known in
order to develop an appropriate surgical plan. For this, a precise
breast imaging reexamination is important. Mammography is not
suitable for immediate postoperative imaging as compression of the
breast may lead to wound dehiscence. Ultrasound examination is also
not suitable for postoperative imaging, as the image quality is
usually largely affected by local structural disorders and edema in
the surgical area. MRI is now widely accepted as the most accurate
imaging modality for assessment of breast tumors, as it is capable
of detecting unsuspected multifocal/multicentric or contralateral
breast cancers and is suitable for guiding therapeutic decisions
(9–11). Therefore, MRI was used as the imaging
reexamination method in the present study.
Materials and methods
Patients
Between January 2011 and December 2013, 10 breast
cancer patients diagnosed with non-malignant breast lesions by
preoperative clinical and imaging examinations, as well as by
intraoperative frozen section pathology, but who were finally
confirmed as having malignant breast lesions by paraffin-embedded
tissue histology, were included in the present study. All the
patients were females with an average age of 37.8±12.9 years
(range, 19–57 years). Six of the cases had non-specific invasive
ductal carcinoma, 3 had intraductal carcinoma and 1 had endocrine
carcinoma. Clinical data of the patients are listed in Table I. The present study was approved by
the Ethics Committee of Xi'an Jiaotong University (Xi'an, China)
and all patients gave written informed consent prior to enrolment
in the study.
 | Table I.Clinical information of the 10
patients. |
Table I.
Clinical information of the 10
patients.
| Case no. | Age (years) | Initial pathological
findings | MRI time following
first surgery (days) | Second surgery | Second pathological
findings | Immunohistochemical
findings | Axillary nodes | Clinical stage | Coincidence of MRI
and pathological findings |
|---|
| 1 | 38 | Non-specific invasive
ductal carcinoma | 13 | Modified radical
mastectomy | No tumor residue | ER (+), PR (+), HER2
(−) | 1/23 metastasis | PT1N1M0 | Imaging (−),
pathological findings (−) |
| 2 | 19 | Endocrine
carcinoma | 17 | Breast-conserving
surgery, sentinel lymph node biopsy | Small focal
neuroendocrine carcinoma |
| 3 reactive
hyperplasia | PT1N0M0 | Imaging (−),
pathological findings (+) |
| 3 | 54 | Intraductal
carcinoma | 19 | Modified radical
mastectomy | No tumor residue | ER (−), PR (−), HER2
(−) | 1 reactive
hyperplasia | PT1N0M0 IA | Imaging (−),
pathological findings (−) |
| 4 | 30 | Non-specific invasive
ductal carcinoma | 10 | Modified radical
mastectomy | Tumor residue | ER (−), PR (−), HER2
(−) | 5/7 metastasis | PT1N2M0 | Imaging (+),
pathological findings (+) |
| 5 | 39 | Non-specific invasive
ductal carcinoma | 13 | Modified radical
mastectomy, sentinel lymph node biopsy | Tumor residue | ER (++), PR (+++),
HER2 (−) |
| PT1N0M0 IA | Imaging (+),
pathological findings (+) |
| 6 | 48 | Intraductal
carcinoma | 2 | Breast-conserving
surgery | Tumor residue | ER (++), PR (+), HER2
(+++) | 1 reactive
hyperplasia | PT1N0M0 | Imaging (+),
pathological findings (+) |
| 7 | 24 | Non-specific invasive
ductal carcinoma | 13 | Modified radical
mastectomy | Tumor residue | ER (+), PR (−), HER2
(+) | 3/15 metastasis | PT2N1M0 IIB | Imaging (+),
pathological findings (+) |
| 8 | 57 | Intraductal
carcinoma | 17 | Modified radical
mastectomy, sentinel lymph node biopsy | No tumor residue | ER (++), PR (−), HER2
(−) | 4 reactive
hyperplasia | PT1N0M0 IB | Imaging (−),
pathological findings (−) |
| 9 | 26 | Non-specific invasive
ductal | 28 | Breast-conserving
surgery, sentinel lymph node biopsy | No tumor residue | ER (++), PR (+++),
HER2 (+) | 7 reactive
hyperplasia | PT2N0M0 IIA | Imaging (−),
pathological findings (−) |
| 10 | 43 | Non-specific invasive
ductal carcinoma | 16 | Breast-conserving
surgery, sentinel lymph node biopsy | No tumor residue | ER (−), PR (−), HER2
(−) | 2 reactive
hyperplasia | PT1N0M0 IA | Imaging (−),
pathological findings (−) |
MRI acquisition and analysis
All patients were subjected to MRI examination
between days 2 and 28 after the first surgery with an average time
interval of 15 days.
MRI was performed using a 3.0-T system (GE Signa
HDxt; GE Healthcare, Milwaukee, WI, USA). All patients were
examined in a prone position using a double breast coil. An axial
fat-suppressed T2-weighted short-TI inversion recovery sequence was
performed with the following parameters: Repetition time (TR)/echo
time (TE), 8,800.00 msec/33.88 msec; field of view, 320.00 mm;
matrix size, 512×512; and slice thickness, 4 mm with a 1-mm gap. An
axial T1 sequence was performed with the following parameters:
TR/TE, 580 msec/7.20 msec; field of view, 320.00 mm; matrix size,
512×512; and slice thickness, 4 mm with a 1-mm gap. An axial
echo-planar imaging (EPI)-diffusion-weighted imaging (DWI) sequence
(b=1,000) was performed with the following parameters: TR/TE, 6,000
msec/69.60 msec; field of view, 320.00 mm; matrix size, 256×256;
and slice thickness, 4 mm with a 1-mm gap. An axial Vibrant+C
sequence was performed with the following parameters: TR/TE, 4.29
msec/2.10 msec; field of view, 320.00 mm; matrix size, 512×512; and
slice thickness, 1.4 mm with a 0.7-mm gap. The contrast agent
(Omniscan®; GE Healthcare, Cork, Ireland; 0.1 mmol/kg
body weight) was manually injected at the beginning of the 5th
acquisition, followed by 10 cc saline to flush in all contrast
medium. Two experienced radiologists independently reviewed the
images using ImageJ 1.44p software (National Institutes of Health,
Bethesda, MD, USA).
Results
MRI analysis
The breast MRI features of the 10 patients are
summarized in Table II. All the
cases showed a local mammary architecture distortion in the routine
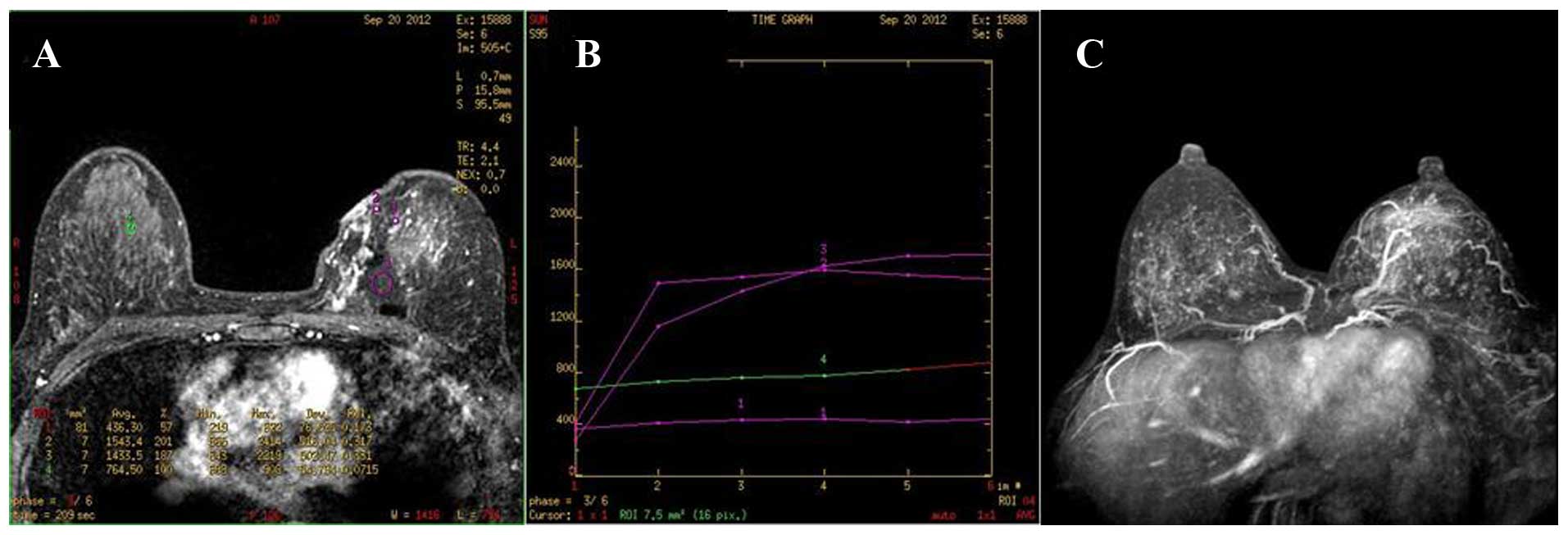
MRI and in the enhancement MRI. The enhancement characteristics of
the 10 cases were as follows: 3 cases showed stippled enhancement,
2 had small nodular enhancement, 1 featured dendritic enhancement
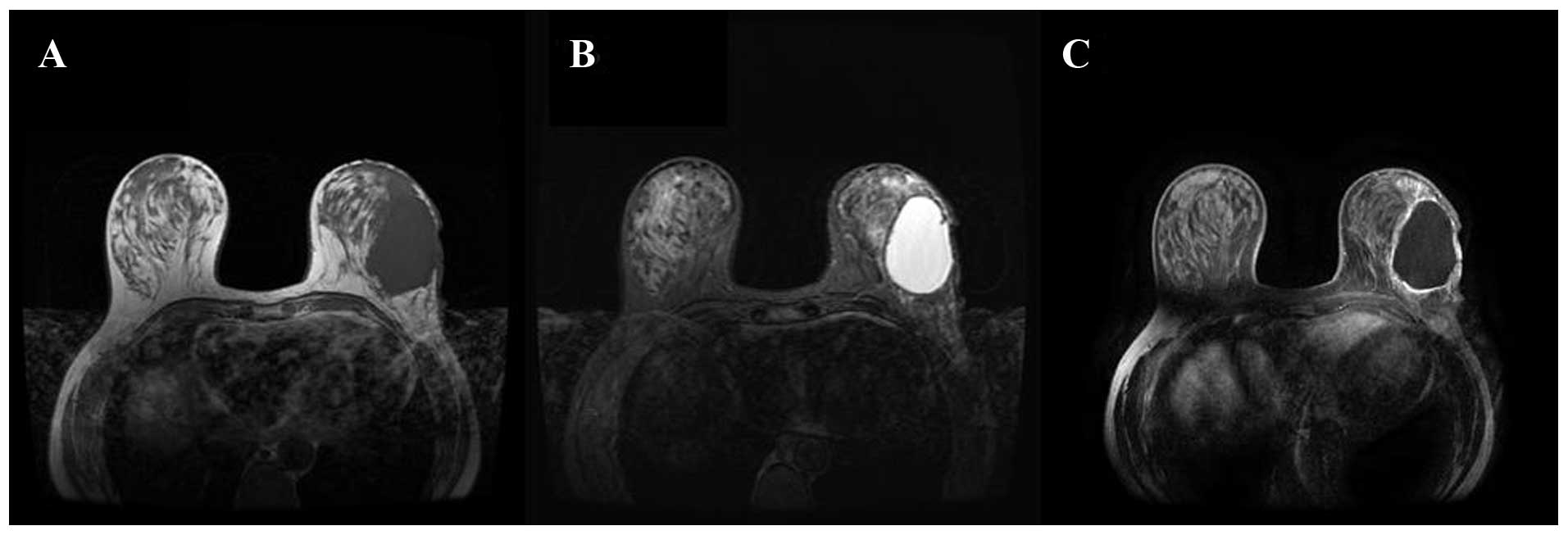
(Fig. 1), 1 showed a ring-shaped
enhancement of the cystic wall (Fig.
2) and 3 had no abnormal enhancement. The lesions of 7 cases
had a type-I enhancement curve (progressive enhancement pattern)
and 3 had a type-II enhancement curve (plateau pattern). Regarding
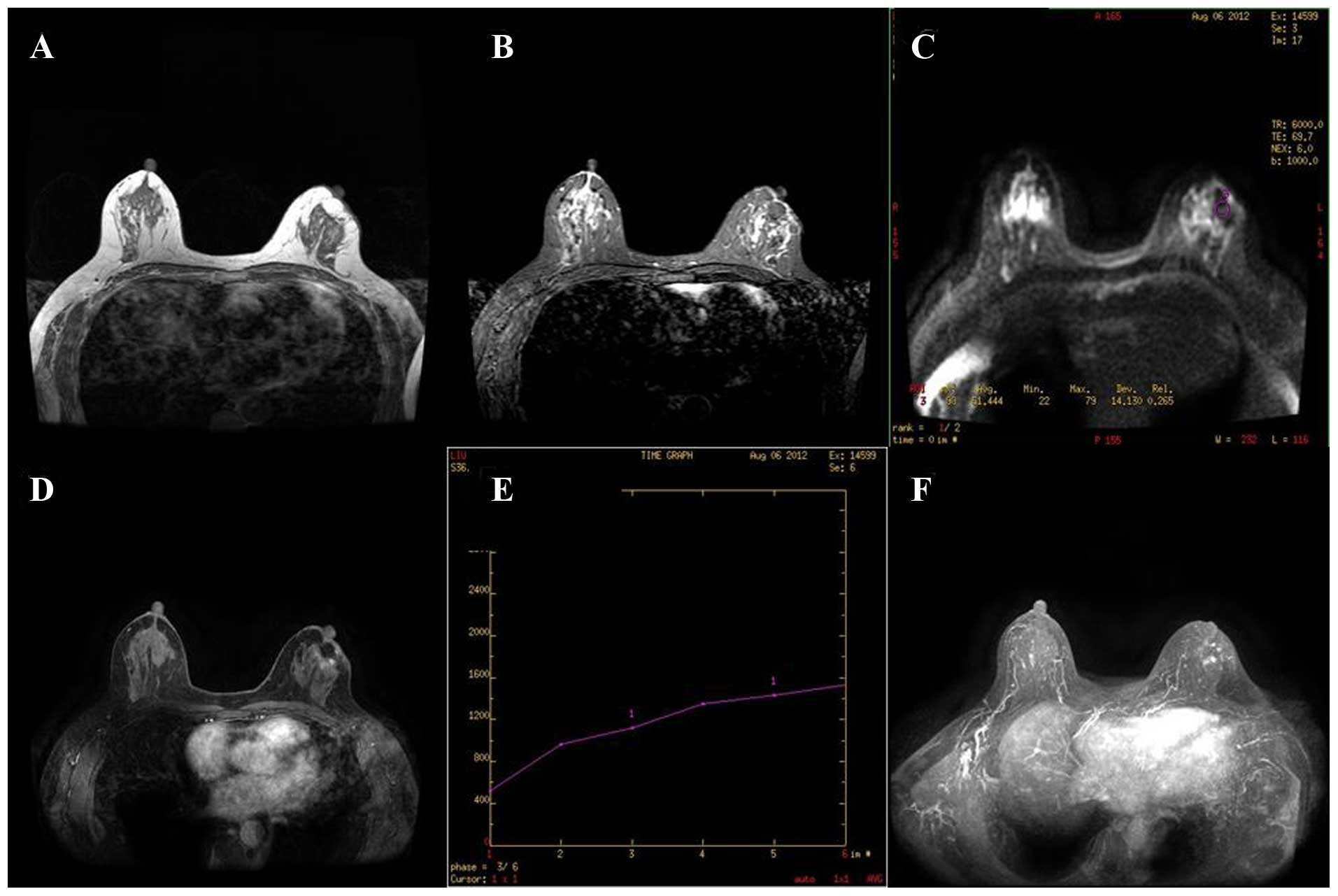
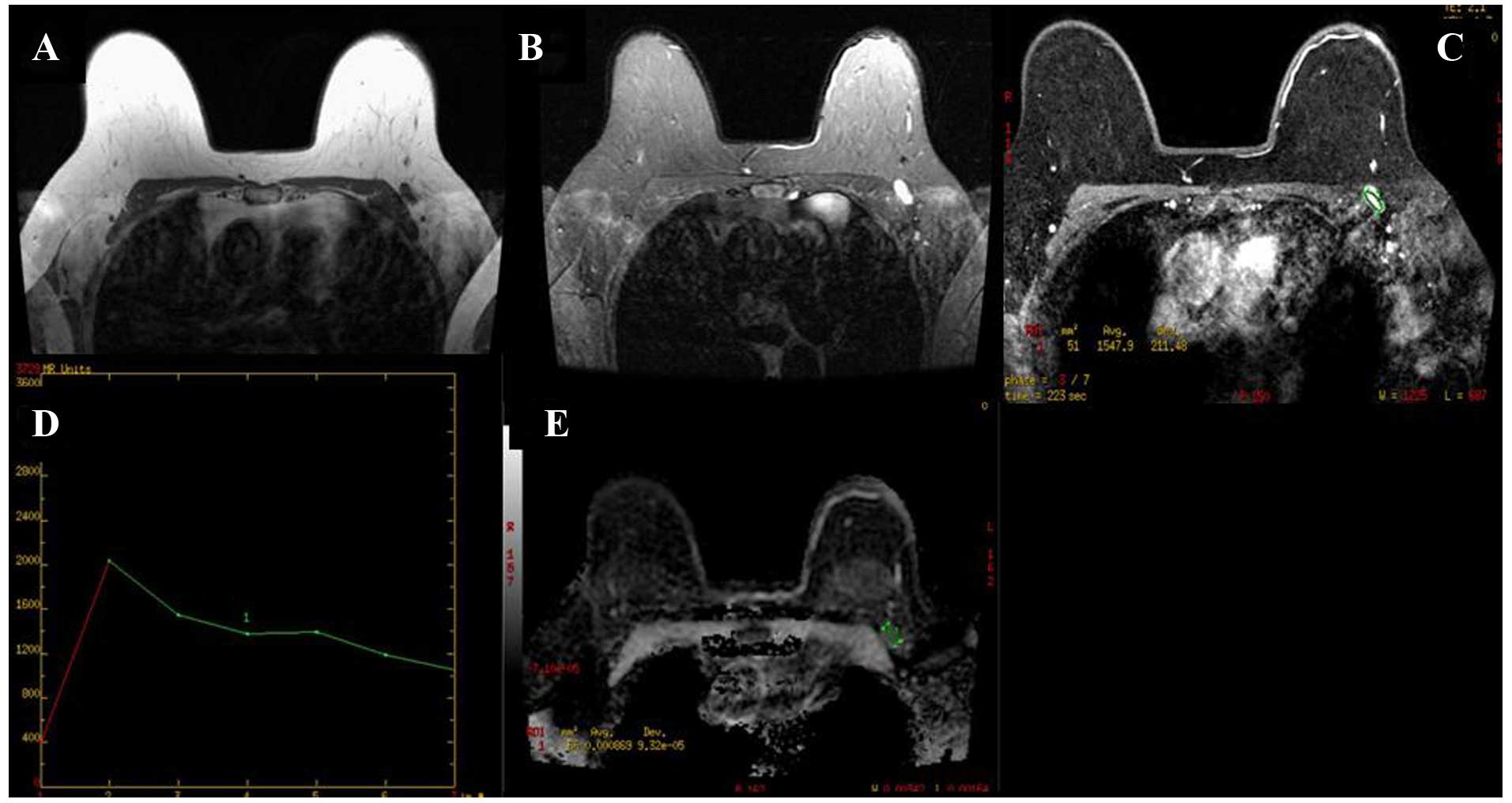
the apparent diffusion coefficients (ADCs) of the 10 patients, 4
were found to be abnormally decreased according to the threshold
value of 1.2±0.25×10−3 mm2/sec (12), with resulting ADCs of
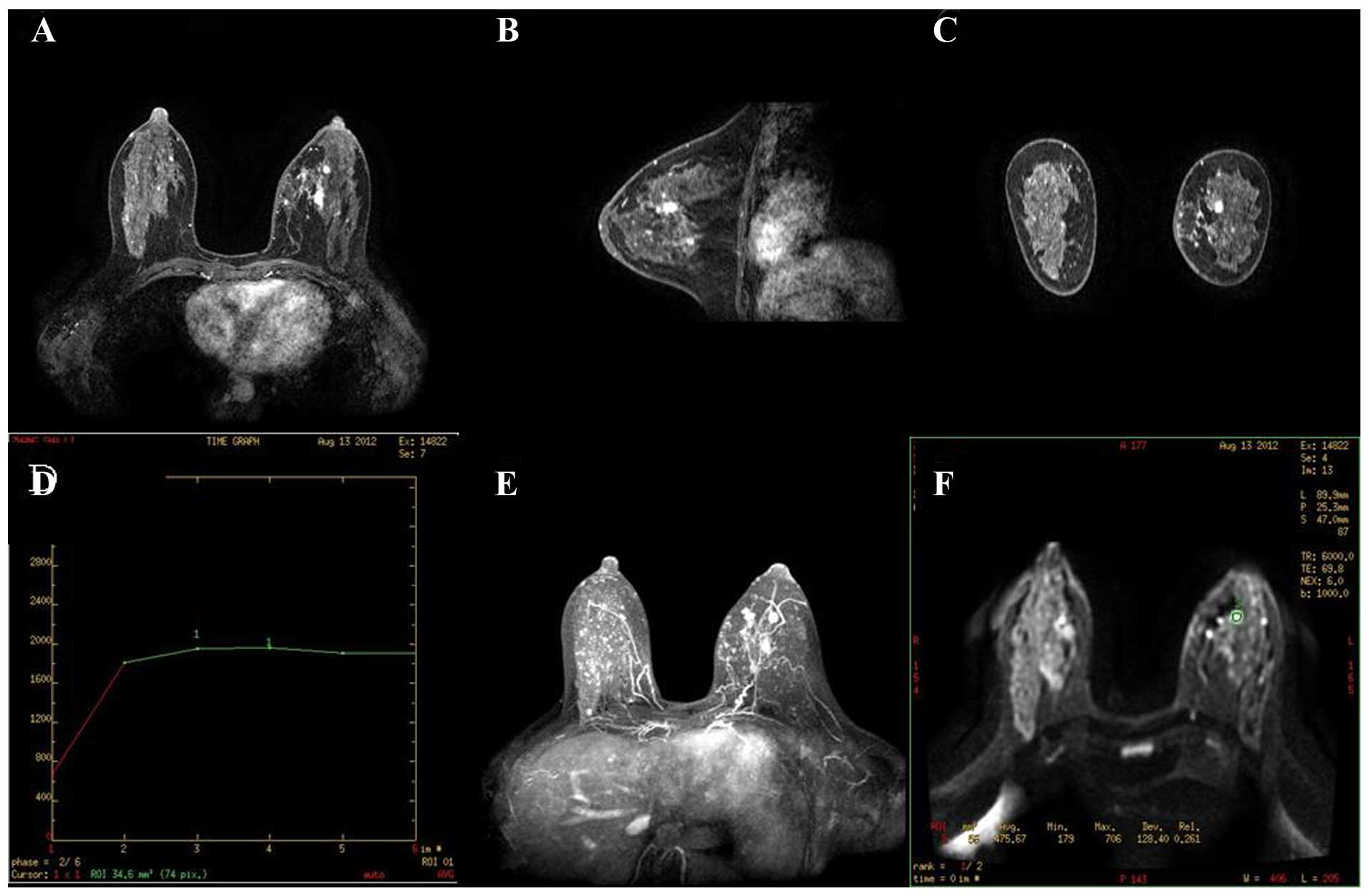
0.77×10−3 mm2/sec (Fig. 3), 0.96×10−3
mm2/sec, 0.88–1.07×10−3 mm2/sec
(Fig. 4) and 1.18×10−3
mm2/sec respectively. Furthermore, 1 swollen axillary
lymph node was found in the armpit of the lesion side with an ADC
of 0.7×10−3 mm2/sec (Fig. 5).
| Table II.Breast MRI features of the
patients. |
Table II.
Breast MRI features of the
patients.
| Imaging method | Imaging feature | Cases (n) |
|---|
| MRI plain scan | Structural
disorder | 10 |
|
| Local skin,
subcutaneous tissue edema | 10 |
|
| Residual cavity | 3 |
| Diffusion-weighted
imaging scan | Decrease in apparent
diffusion coefficient | 4 |
| MRI dynamic
enhancement scan | Stippled
enhancement | 3 |
|
| Nodular
enhancement | 2 |
|
| Dendritic
enhancement | 1 |
|
| Ring-like enhancement
of cystic wall | 1 |
|
| No abnormal
enhancement | 3 |
|
| Type I curve | 7 |
|
| Type II curve | 3 |
Based on the morphological features and curves of
the enhancement MRI, as well as the ADC values, the presence of
residual breast cancer was evaluated. The results demonstrated that
tumor residues were present in 4 cases and 1 axillary lymph node
metastasis was detected by MRI and the second pathological
analysis, while in only 1 case, the tumor residue was misdiagnosed
by MRI but confirmed by the second pathological analysis.
All of the patients received corresponding second
surgeries. Among them, 4 underwent breast-conserving surgery and 6
underwent modified radical mastectomy.
Discussion
With the development of cytological techniques for
determining the nature of sono- or mammographically diagnosed
breast abnormalities, percutaneous image-guided core needle biopsy
has become an alternative to surgical biopsy for the histological
assessment of breast lesions (13).
However, intraoperative frozen section pathology is widely used in
numerous countries, including China. In general, frozen section
pathology examination is a requisite during surgery for all
patients with diseases of the breast and surgeons select an
appropriate surgical approach based on the result of the frozen
section diagnosis. Therefore, frozen section pathology is crucial
for the diagnosis of breast abnormalities (14).
In the present study, the pathological
characteristics of the breast lesions in the majority of patients
were typical and a pathological diagnosis was easily made. For
certain patients, however, it was not the case. The average rate of
correct diagnosis based on frozen section pathology is 92.6–98.0%,
and accordingly, the rate of misdiagnosis is 2.0–7.4%. The main
reasons of misdiagnosis are as follows: i) Incorrect sampling; ii)
poor quality of frozen sections (15); iii) a limited time for pathologist to
diagnose; iv) a lack of specific stains and immunohistochemistry;
and v) limited experience of the pathologist (16). Misdiagnosis based on intraoperative
frozen sections of breast tumors is unavoidable and leads to the
selection of an inappropriate surgical plan and causes a
psychological, physical and economic burden for patients (17). Therefore, it is important to establish
an appropriate therapy plan for patients as soon as possible
following identification of the misdiagnosis (18).
At present, false-negative cases are required to
undergo reexcision or even sentinel lymph node biopsy with the
smallest possible delay in order to ensure complete resection of
the tumor and prevent metastasis to the lymph nodes. Prior to
selection of the second surgical scheme, a comprehensive and
objective assessment of the postoperative breast is required.
However, compared with patients not receiving surgery, breast
imaging is more complex for patients who recently underwent
surgery. Under such conditions, MRI may be the optimal choice among
the three most common types of breast examinations (mammography,
ultrasound and MRI) to assess the condition of the postoperative
breast (19). MRI has certain
advantages: The breast does not require to be compressed in the
process of scanning. Furthermore, the scan sequence of MRI is
diversified and each sequence may be used for the analysis of
lesions from different inspections. Additionally, MRI can help
physicians evaluate the presence of multifocal lesions (20). Finally, MRI can predict axillary lymph
node metastasis (21). Therefore, the
present study retrospectively reviewed the postoperative MRI scans
of these patients.
To date, only a small number of studies have
reported the use of MRI in the short-term follow-up for the
detection of postoperative residual breast cancer. Chae et
al (22) reported that dynamic
contrast-enhanced breast MRI was a useful tool for residual disease
prediction following excisional biopsy for breast cancer. However,
the study subjects were patients who underwent excisional biopsy,
rather than patients misdiagnosed by intraoperative frozen section
pathology. Furthermore, in the present study, MRI findings were
analyzed on the basis of contrast-enhanced and DWI scans, while in
the study by Chae et al (22),
MRI findings were analyzed only on the basis of contrast-enhanced
scans.
Among the 10 subjects of the present study, 4 cases
with tumor residues and 1 case with axillary lymph node metastasis
were diagnosed by MRI and the second pathology. None of the
patients received MRI prior to the surgery due to various reasons.
However, 1 patient with a tumor residue was misdiagnosed by MRI,
following which a correct diagnosis was made based on the
pathological findings.
The images of the 4 patients diagnosed as having
tumor residues by MRI and pathology were analyzed. Three cases
showed nodular enhancement and 1 showed structural disorders with
branch-like enhancement. One case showed type-I time-signal
intensity curves (TIC) and 3 showed type-II TIC. The ADC value for
all 4 cases was <1×10−3 mm2/sec. These
results demonstrated that for breast cancer patients, MRI within 1
month after breast surgery had a high diagnostic capacity in spite
of local structural disorders due to surgery.
In the patient misdiagnosed by MRI, no abnormal
enhancement was found in the MRI and the ADC value was
1.4–2.0×10−3 mm2/sec. In this case, the
information provided by the MRI was inconsistent with the
pathological findings, which may be that the pathological type of
this patient was neuroendocrine carcinoma. The current consensus is
that the majority of cases of neuroendocrine carcinoma are well
differentiated and lack typical and evident malignant signs
observed by imaging, which may conduce to the misdiagnosis based on
MRI (23).
In the present study, based on the results of the
postoperative MRI, surgeons adopted two different surgical modes
for the 10 patients; 4 were subjected to breast-conserving surgery
and 6 accepted modified radical mastectomy. Histological
examination of paraffin-embedded tissues following the second
surgery showed no residual cancer in any of the 10 patients, who
have not presented with any signs of tumor recurrence to date.
In conclusion, the present study suggested that
short-term follow-up MRI is of value for detecting postoperative
residual breast tumors and may guide surgeons in the selection of
the optimal surgical scheme. However, due to the limited number of
cases, further studies on a larger patient cohort are required to
confirm this conclusion.
References
|
1
|
Murray PJ, Wivell G and Denton E: Breast
cancer screening and diagnosis in the 21st century within the UK.
Post Reprod Health. 21:105–111. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pak F, Kanan HR and Alikhassi A: Breast
cancer detection and classification in digital mammography based on
non-subsampled contourlet transform (NSCT) and Super resolution.
Comput Methods Programs Biomed. 122:89–107. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mann RM, Balleyguier C, Baltzer PA, Bick
U, Colin C, Cornford E, Evans A, Fallenberg E, Forrai G, Fuchsjäger
MH, et al: Breast MRI: EUSOBI recommendations for women's
information. Eur Radiol. 25:3669–3678. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chetlen A, Mack J and Chan T: Breast
cancer screening controversies: Who, when, why, and how? Clin
Imaging. 2015.(Epub ahead of print). PubMed/NCBI
|
|
5
|
Giess CS, Yeh ED, Raza S and Birdwell RL:
Background parenchymal enhancement at breast MR imaging: Normal
patterns, diagnostic challenges and potential for false-positive
and false-negative interpretation. Radiographics. 34:234–247. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
El-Bolkainy TM, Shabaan HA, Abodeif WT,
El-Bolkainy MN and El-Tony A: Intra-operative diagnosis of breast
mass-lesions: Comparison of the validity of touch smear preparation
and frozen section techniques. J Egypt Natl Canc Inst. 20:63–69.
2008.PubMed/NCBI
|
|
7
|
Niu Y, Fu XL, Yu Y, Wang PP and Cao XC:
Intra-operative frozen section diagnosis of breast lesions: A
retrospective analysis of 13,243 Chinese patients. Chin Med J
(Engl). 120:630–615. 2007.PubMed/NCBI
|
|
8
|
Wen MC, Chen JT and Ho WL: Frozen-section
diagnosis in surgical pathology: A quality assurance study.
Kaohsiung J Med Sci. 13:534–539. 1997.PubMed/NCBI
|
|
9
|
Law Y, Cheung PS, Lau S and Lo GG: Impact
of magnetic resonance imaging on preoperative planning for breast
cancer surgery. Hong Kong Med J. 19:294–299. 2013.PubMed/NCBI
|
|
10
|
Houssami N, Turner R and Morrow M:
Preoperative magnetic resonance imaging in breast cancer:
Meta-analysis of surgical outcomes. Ann Surg. 257:249–255. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Vilar VS, Goldman SM, Ricci MD, et al:
Analysis by MRI of residual tumor after radiofrequency ablation for
early stage breast cancer. AJR Am J Roentgenol. 198:W285–W291.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yili Z, Xiaoyan H, Hongwen D, Yun Z, Xin
C, Peng W and Youmin G: The value of diffusion-weighted imaging in
assessing the ADC changes of tissues adjacent to breast carcinoma.
BMC Cancer. 9:182009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Brunner AH, Sagmeister T, Kremer J, Riss P
and Brustmann H: The accuracy of frozen section analysis in
ultrasound- guided core needle biopsy of breast lesions. BMC
Cancer. 9:3412009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bellolio JE, Guzmán GP, Orellana CJ, Roa
SJC, Villaseca HM, Araya OJC, Tapia EO and Ineda NV: Diagnostic
value of frozen section biopsy during surgery for breast lesions or
neoplasms. Rev Med Chil. 137:1173–1178. 2009.(In Spanish).
PubMed/NCBI
|
|
15
|
Geramizadeh B, Larijani TR, Owji SM,
Attaran SY, Torabinejad S, Aslani FS, Monabati A, Kumar PV and
Tabei SZ: Accuracy of intra-operative frozen section consultation
in south of Iran during four years. Indian J Pathol Microbiol.
53:414–417. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Brun JL, Cortez A, Rouzier R, Callard P,
Bazot M, Uzan S and Daraï E: Factors influencing the use and
accuracy of frozen section diagnosis of epithelial ovarian tumors.
Am J Obstet Gynecol. 199:244.e1–e7. 2008. View Article : Google Scholar
|
|
17
|
Kim JH, Kim TJ, Park YG, Lee SH, Lee CW,
Song MJ, Lee KH, Hur SY, Bae SN and Park JS: Clinical analysis of
intra-operative frozen section proven borderline tumors of the
ovary. Gynecol Oncol. 20:176–180. 2009. View Article : Google Scholar
|
|
18
|
Slama J, Dundr P, Dusek L and Cibula D:
High false negative rate of frozen section examination of sentinel
lymph nodes in patients with cervical cancer. Gynecol Oncol.
129:384–388. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Saunders C and Taylor D: Expanding the
indications for MRI in the diagnosis and treatment of breast
cancer: What is best practice? J Med Radiat Sci. 62:47–53. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Almotairi M, Oudjhane K and Chavhan GB:
Pediatric multifocal liver lesions evaluated by MRI. Indian J
Radiol Imaging. 25:296–302. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kuijs VJ, Moossdorff M, Schipper RJ,
Beets-Tan RG, Heuts EM, Keymeulen KB, Smidt ML and Lobbes MB: The
role of MRI in axillary lymph node imaging in breast cancer
patients: A systematic review. Insights Imaging. 6:203–215. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chae EY, Cha JH, Kim HH, et al: Evaluation
of residual disease using breast MRI after excisional biopsy for
breast cancer. AJR Am J Roentgenol. 200:1167–1173. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rovera F, Masciocchi P, Coglitore A, La
Rosa S, Dionigi G, Marelli M, Boni L and Dionigi R: Neuroendocrine
carcinomas of the breast. Int J Surg. 6(Suppl 1): S113–S115. 2008.
View Article : Google Scholar : PubMed/NCBI
|