Introduction
Intrahepatic cholangiocarcinoma (ICC) is an
intrahepatic malignancy arising from the biliary epithelium in the
intrahepatic bile duct from the segmental and area ducts and their
finer branches to the small bile ducts and ductules (1,2). ICC is
the second most frequent intrahepatic primary liver tumour after
hepatocellular carcinoma (3),
accounting for 5–10% of primary liver cancer cases (4). Of note, the global incidence of ICC has
been steadily increasing over the last 30 years (4). From the early 1970s to 1999, the ICC
incidence in United States and China increased by >150%
(4,5). Due to a lack of clinical symptoms and
appropriate markers for early diagnosis, ICC is usually diagnosed
at an advanced stage (4), mostly
with local invasion, liver parenchymal and lymph node metastases,
leading to a poor outcome following surgical removal, which is
currently the only curative option (6,7). The
increasing incidence of ICC, its poor prognosis and lack of
treatment options necessitate further studies on its risk factors,
early diagnostic markers and prognostic factors.
A number of prognostic factors have previously been
reported for ICC, including liver function, vascular invasion,
tumour-node-metastasis (TNM) classification and lymph node
metastasis (8,9); however, there is little consensus
regarding the appropriate prognostic factors and thresholds
(10,11). Accumulating evidence indicates the
prospective of inflammation-based parameters as prognostic factors
(12). This is supported by the wide
range of associations between inflammation and tumour initiation,
invasion and metastasis (13,14).
Tumour infiltration and infiltrating lymphocytes in the tumour
microenvironment induce the production of a repertoire of cytokines
and inflammatory factors (15); in
turn, interleukin (IL)-6, tumour necrosis factor (TNF) and
neutrophil accumulation due to the systemic inflammation, enhance
tumour growth, invasion and metastasis (16–19).
Targeting IL-6 and TNF to interrupt their signalling cascades has
been demonstrated to reduce angiogenesis, myeloid cell infiltration
and tumour growth (20,21).
Over the past decade, a number of parameters and
scoring systems have been developed based on systemic inflammation,
which may be evaluated by the serum levels of platelets,
neutrophils, lymphocytes, albumin and C-reactive protein (CRP), to
assess the prognosis of malignant solid tumours. These include the
Glasgow Prognostic Score (GPS), which is based on serum CRP and
albumin levels (22–28), neutrophil-to-lymphocyte ratio (NLR)
(29,30), platelet-to-lymphocyte ratio (31,32),
prognostic nutritional index (33,34), and
prognostic index (34,35).
Certain inflammation-based parameters and scoring
systems were previously shown to reliably predict the prognosis of
cholangiocarcinoma. Preoperative NLR is correlated with the overall
survival of ICC patients, and NLR>5 is an independent risk
factor for recurrence (36). GPS is
an independent prognostic factor for extrahepatic
cholangiocarcinoma according to a study on 62 patients (37). The aim of the present study was to
investigate the feasibility of using preoperative GPS as an ICC
prognostic factor.
Patients and methods
Patient selection
The ICC subjects were recruited among patients who
had undergone partial hepatectomy performed by the same group of
surgeons at the Department of Oncological Surgery, Quanzhou First
Hospital, Fujian Medical University (Quanzhou, China) from June,
2005 to September, 2011. All selected patients had complete
long-term follow-up records and their clinical background
information was available for retrospective analysis. Patients with
preoperative metastasis, or those undergoing systemic chemotherapy,
transcatheter arterial chemoembolization, or local ablation
therapy, as well as patients with acute inflammation or rheumatoid
arthritis, were excluded. Blood tests were performed 3 days prior
to surgery and ICC was confirmed by postoperative histopathological
examination.
The present study complied with the standards of the
Helsinki Declaration on human research ethics and was approved by
the Institutional Ethics Board of Fujian Medical University.
Written informed consent from the investigated patients was not
obtained due to the retrospective nature of this study. All data
were analysed anonymously.
Follow-up survey and data
collection
The follow-up surveys were conducted monthly to
quarterly within 2 years after surgery, quarterly to half-yearly
between 2 and 5 years, and half-yearly thereafter. The survey
included comprehensive medical history, measurement of carbohydrate
antigen 19–9 (CA19-9) levels and imaging surveillance by chest
radiography, abdominal Doppler ultrasonography and computed
tomography. Survival was calculated in months from the date of
surgery to death, and disease-free survival as months from the date
of surgery to recurrence. Recurrence was defined as any unequivocal
occurrence of new cancer foci during imaging surveillance or
histopathological analysis. The follow-up was continued for ≤67
months (mean, 24 months), ending on September 1, 2014 for all 72
patients. Following institutional ethics approval, the complete
medical files, including images, clinical pathological materials,
and follow-up records, were archived in a database for
retrospective analysis.
Clinical data, biochemical parameters
and GPS
The size and number of tumours and presence of
vascular invasion were assessed based on postoperative pathological
outcomes. Serum CRP concentration was measured by a nephelometric
immunoassay on a Beckman Coulter immunochemistry system (IMMAGE
800; Beckman Coulter, Inc., Brea, CA, USA). Serum CA19-9 levels
were assessed by electro-chemiluminescent microparticle immunoassay
(Roche Diagnostics, Shanghai, China), and a level > 37 U/ml was
considered to be positive. Biochemical parameters, such as alanine
aminotransferase (ALT), aspartate aminotransferase (AST), total
bilirubin (TB) and albumin, were determined using a Beckman Coulter
LX-20 clinical chemistry analyser (Beckman Coulter, Inc.).
Hepatitis B virus (HBV) was quantified by chemiluminescence using
an Architect i2000SR immunoassay analyser (Abbott Diagnostics, Lake
Forest, IL, USA). The tumours were staged according to the 7th
edition of TNM system (38) issued
by the American Joint Committee on Cancer/International Union
Against Cancer, and graded following the Edmondson system (39).
GPS was allocated as previously described, combining
preoperative serum CRP and albumin levels. Patients with elevated
CRP level (>10 mg/l) and hypoalbuminemia (<35 g/l) were
scored as 2, patients with only one of the two biochemical
abnormalities were scored as 1, and patients with neither of the
two abnormalities were scored as 0 (22,23).
Statistical analysis
All the statistical tests were performed using IBM
SPSS Statistics software v.19.0 (IBM SPSS Inc., Armonk, NY, USA).
The χ2 test, Fisher's exact probability test and
Student's t-test were used for comparison between groups. The
non-parametric Mann-Whitney U test was used when variables in
groups were not homogeneous. Prognosis was evaluated by 3- and
5-year overall and disease-free survival after surgery.
Kaplan-Meier cumulative survivals were calculated and groups with
different GPS scores were compared using the log-rank test. The Cox
proportional hazards model was used for multivariate analysis and a
threshold α=0.05 was used.
Results
Patient characteristics
The median age of the 72 patients was 55 years (mean
± standard deviation, 53.26±11.05 years); 29 of the patients were
male and 43 female (Table I). A
total of 63 and 9 patients were classified as Child-Pugh A and B,
respectively; there were no class C patients. A total of 34 (47.2%)
patients were positive for antibodies against HBV. The overall 1-,
3- and 5-year postoperative survival was 55.56, 29.20 and 8.33%,
respectively, with a median survival of 34 months.
 | Table I.Clinicopathological characteristics
of the patients. |
Table I.
Clinicopathological characteristics
of the patients.
|
Characteristics | No. | Percentage |
|---|
| Gender |
|
|
|
Male | 29 | 40.30 |
|
Female | 43 | 59.70 |
| Age (years) |
|
|
|
Median | 55 |
|
| Mean ±
SD | 53.26±11.05 |
|
| Child-Pugh
class |
|
|
| A | 63 | 87.50 |
| B | 9 | 12.50 |
| CRP (mg/l) |
|
|
|
≤10 | 58 | 80.60 |
|
>10 | 14 | 19.40 |
| Albumin (g/l) |
|
|
|
<35 | 16 | 22.20 |
|
≥35 | 56 | 77.80 |
| HBV status |
|
|
|
Positive | 34 | 47.20 |
|
Negative | 38 | 52.80 |
| Vascular
invasion |
|
|
|
Yes | 40 | 44.40 |
| No | 32 | 55.60 |
| Nο. of tumours |
|
|
| 1 | 55 | 76.40 |
| ≥2 | 17 | 23.60 |
| Tumour size
(cm) |
|
|
| ≤5 | 52 | 72.20 |
|
>5 | 20 | 27.80 |
| AFP (ng/ml) |
|
|
|
<400 | 42 | 58.30 |
|
≥400 | 30 | 41.70 |
| ALT (U/l) |
|
|
|
≤40 | 40 | 55.60 |
|
>40 | 32 | 44.40 |
| AST (U/l) |
|
|
|
≤40 | 39 | 54.20 |
|
>40 | 33 | 45.80 |
| Total bilirubin
(µmol/l) |
|
|
|
≤17.1 | 41 | 56.90 |
|
>17.1 | 31 | 43.10 |
| Ascites |
|
|
|
Negative | 63 | 87.50 |
|
Positive | 9 | 12.50 |
| CA19-9 (U/l) |
|
|
|
<37 | 27 | 37.50 |
|
≥37 | 45 | 62.50 |
| Lymph node
metastases |
|
|
|
Yes | 21 | 29.20 |
| No | 51 | 70.80 |
| TNM
classification |
|
|
| I | 45 | 62.50 |
| II | 24 | 33.33 |
|
III | 3 | 4.20 |
| GPS score |
|
|
| 0 | 49 | 68.10 |
| 1 | 16 | 22.20 |
| 2 | 7 | 9.70 |
A total of 14 (19.4%) patients exhibited elevated
CRP levels (>10 g/l), and 16 (22.2%) patients had
hypoalbuminemia (serum albumin <35 g/l). As a result, 49 (68.1%)
patients were scored a GPS of 0, 16 (22.2%) patients were scored a
GPS of 1 and 7 (9.7%) patients were scored a GPS of 2 (Table II). There was no significant
difference between the GPS groups in terms of age (P=0.191), gender
(P=0.209), ALT (P=0.105), α-fetoprotein (P=0.588), AST (P=0.204),
total bilirubin (P=0.816), HBV positivity (P=0.324), CA-199
(P=0.824), tumour number (P=0.850) and vascular invasion (P=0.234).
However, significant differences were found between different GPS
groups in the preoperative levels of CRP (P<0.001) and albumin
(P<0.001), frequency of ascites accumulation (P=0.035), lymph
node metastasis (P=0.002) and tumour size (P=0.005). A higher GPS
was also correlated with Child-Pugh class (P=0.003) and TNM stage
(P=0.048). Patients with higher GPS score (1 or 2) had higher serum
CRP levels, lower albumin levels, and were more likely classified
as Child-Pugh class B and higher TNM stage, compared with GPS 0
patients; they also more frequently presented with ascites and
lymph node metastasis (Table
II).
| Table II.Association of GPS score with
clinicopathological characteristics in patients undergoing
hepatectomy. |
Table II.
Association of GPS score with
clinicopathological characteristics in patients undergoing
hepatectomy.
|
Characteristics | Overall (n=72) | GPS=0 (n=49) | GPS=1 (n=16) | GPS=2 (n=7) | P-value |
|---|
| Age (years) |
|
|
|
|
|
| Mean ±
SD | 53.26±11.05 | 53.51±11.16 | 49.88±13.00 | 59.29±8.538 | 0.191 |
| Gender |
|
|
|
| 0.209 |
|
Male | 29 | 18 | 6 | 5 |
|
|
Female | 43 | 31 | 10 | 2 |
|
| Child-Pugh
class |
|
|
|
| 0.003 |
| A | 63 | 47 | 12 | 4 |
|
| B | 9 | 2 | 4 | 3 |
|
| CRP (mg/l) | 8.321±16.33 | 2.34±2.52 | 12.07±10.24 | 41.65±34.88 |
<0.001 |
| Albumin (g/l) | 36.99±5.05 | 39.34±3.12 | 32.93±5.31 | 29.90±2.61 |
<0.001 |
| HBV status |
|
|
|
|
|
|
Positive | 34 | 26 | 6 | 2 | 0.324 |
|
Negative | 38 | 23 | 10 | 5 |
|
| Vascular
invasion |
|
|
|
|
0.234 |
|
Yes | 40 | 26 | 8 | 6 |
|
| No | 32 | 23 | 8 | 1 |
|
| Tumour size
(cm) |
|
|
|
| 0.005 |
| Mean ±
SD | 5.82±3.42 | 5.01±3.22 | 7.06±3.37 | 8.71±2.81 |
|
| No. of tumours |
|
|
|
| 0.850 |
| 1 | 55 | 37 | 13 | 5 |
|
| ≥2 | 17 | 12 | 3 | 2 |
|
| AFP (ng/ml) |
|
|
|
|
|
| Mean ±
SD |
4,130.0±10,926.52 |
4,645.83±12,107.70 |
3,088.98±7,596.47 |
253.63±5,536.98 | 0.588 |
| ALT (U/l) |
|
|
|
|
|
| Mean ±
SD | 83.24±166.23 | 60.12±73.20 | 160.81±323.78 | 67.71±39.13 | 0.105 |
| AST (U/l) |
|
|
|
|
|
| Mean ±
SD | 85.26±153.28 | 63.40±74.93 | 140.48±295.08 | 106.67±51.43 | 0.204 |
| Total bilirubin
(µmol/l) |
|
|
|
|
|
| Mean ±
SD | 24.58±26.41 | 23.96±20.62 | 28.89±46.83 | 21.92±15.63 | 0.816 |
| CA 19–9 (U/l) |
|
|
|
| 0.824 |
|
<37 | 27 | 19 | 5 | 3 |
|
|
≥37 | 45 | 30 | 11 | 4 |
|
| Ascites |
|
|
|
| 0.035 |
|
Negative | 63 | 44 | 15 | 4 |
|
|
Positive | 9 | 5 | 1 | 4 |
|
| Lymph node
metastases |
|
|
|
| 0.002 |
|
Yes | 21 | 8 | 9 | 4 |
|
| No | 51 | 41 | 7 | 3 |
|
| TNM
classification |
|
|
|
| 0.048 |
| I | 3 | 3 | 0 | 0 |
| II | 24 | 21 | 3 | 0 |
|
III | 45 | 25 | 13 | 7 |
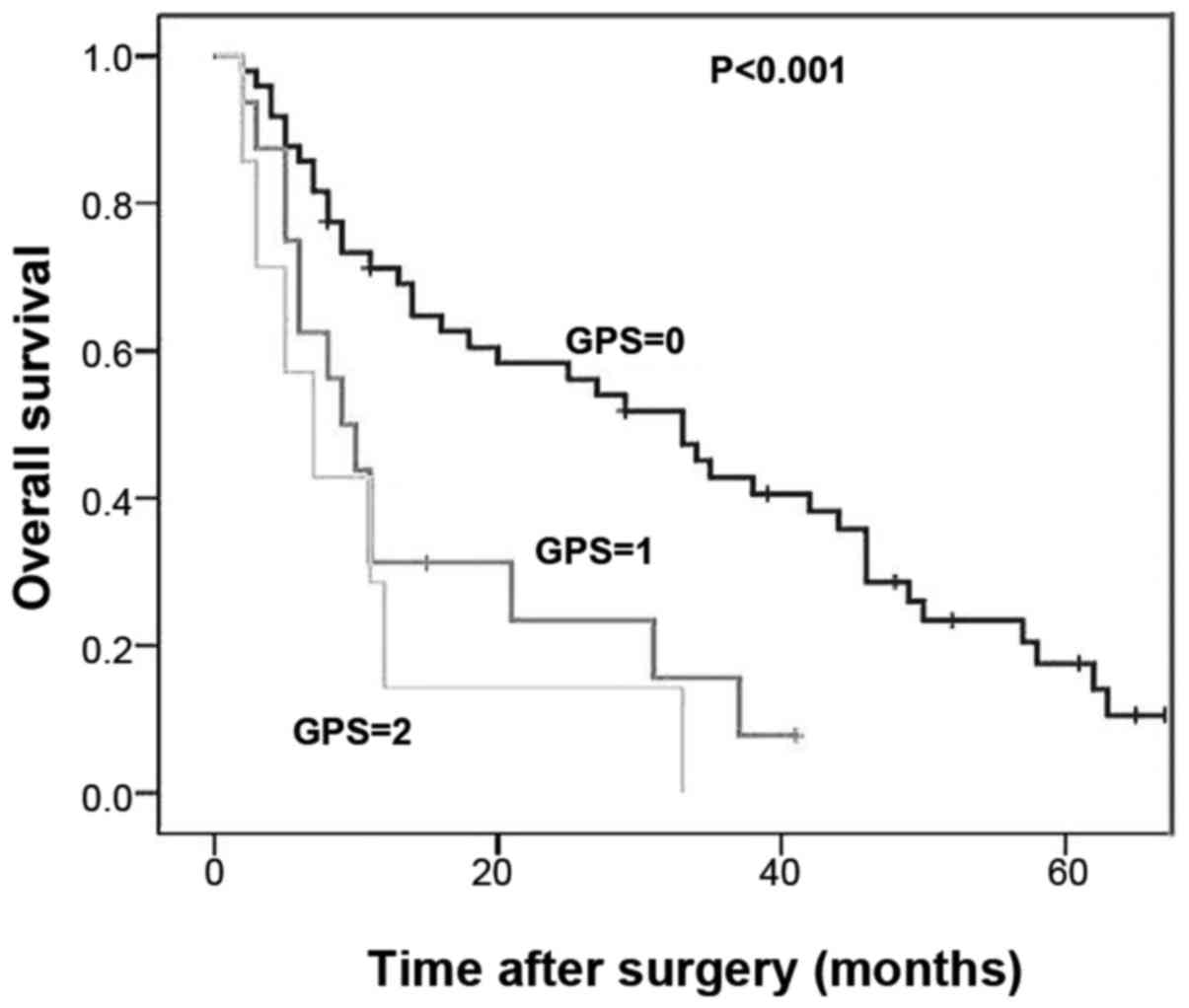
GPS predicts overall survival
The 1- and 3-year overall survival rates of ICC
patients with a GPS score of 0 (GPS-low) were 69.1 and 40.7%,
respectively. The 1- and 3-year overall survival rates of ICC
patients with a GPS score of 1 were 31.3 and 6.3%, respectively;
for patients with a GPS score of 2, these rates decreased to 28.6
and 0%, respectively. Kaplan-Meier analysis with a log-rank test
indicated a significant decrease in the survival rate of patients
with higher GPS scores (1 or 2) compared with the GPS-low group
(Fig. 1, P<0.001). However, there
was no significant difference in survival between patients with a
GPS score of 1 and 2 (P=0.428); thus, these two populations were
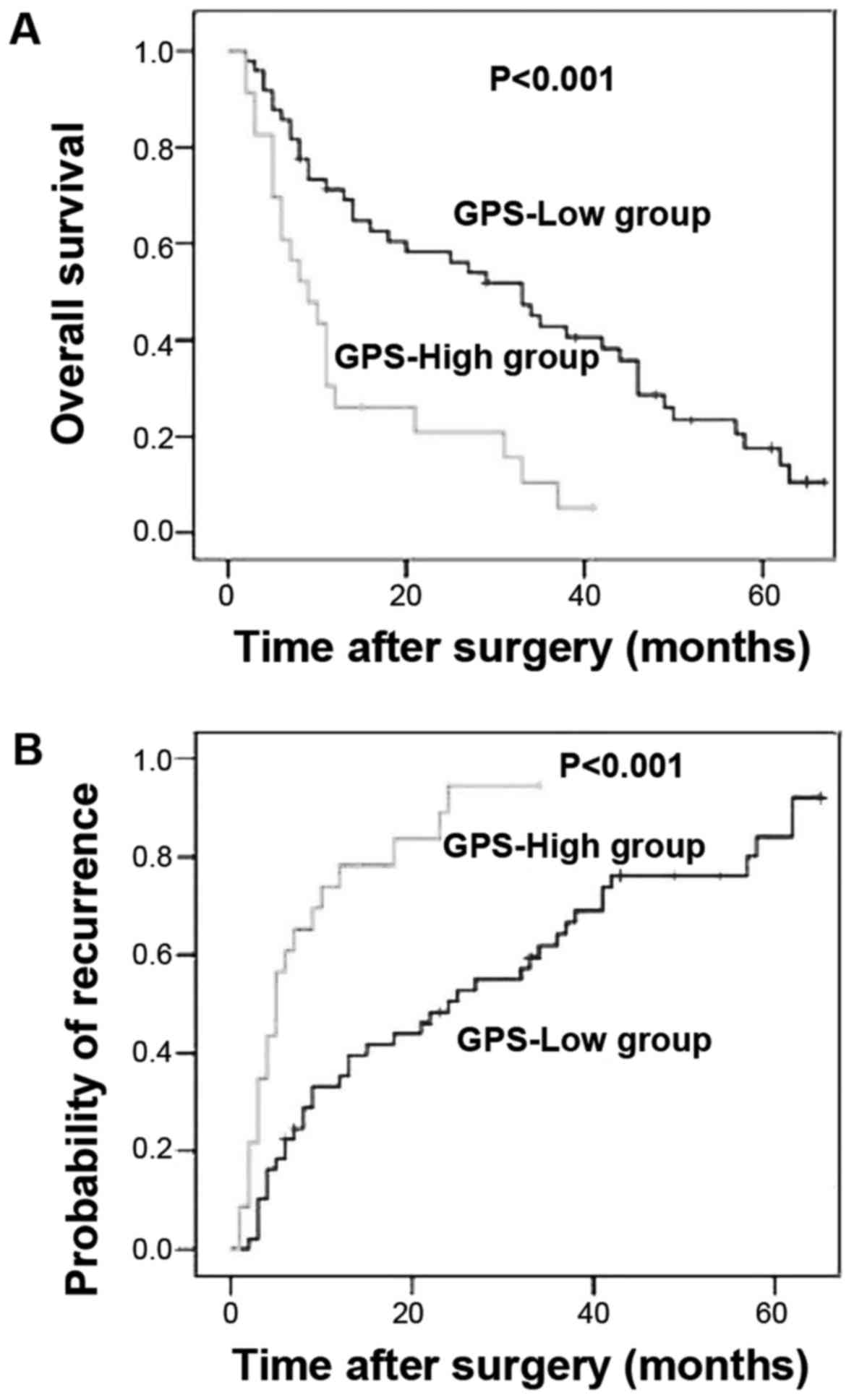
merged into a GPS-high group and compared with the GPS-low
patients. The 1- and 3-year overall survival rates of patients from
the GPS-high group were 30.4 and 10.4%, respectively, which were
significantly lower compared with those of the GPS-low group
(Fig. 2, P<0.001).
On univariate analysis to assess the other
prognostic factors, preoperative CRP (P<0.001), albumin
(P=0.016) and CA19-9 (P=0.038) levels were found to be
significantly associated with the 1- and 3-year overall survival.
Occurrence of lymph node metastasis (P=0.001), HBV positivity
(P=0.009), Child-Pugh class B (P=0.013) and high TNM stage
(P=0.002) also predicted poor survival in ICC patients.
Due to the association of GPS with CRP and albumin
levels, its correlation with patient survival was assessed in a
multivariate analysis using a Cox proportional hazards model. Also
included in the multivariate analysis were 5 variables other than
CRP and albumin, such as CA19-9, occurrence of lymph node
metastasis, positivity for HBV, Child-Pugh class and TNM stage,
which were correlated with patient survival based on the univariate
analysis (Table III). The
multivariate analysis revealed that GPS (HR=2.037, 95% CI:
1.092–3.799, P=0.025), TNM classification (HR=2.000, 95% CI:
1.188–3.367, P=0.009) and HBV positivity (HR=0.559, 95% CI:
0.328–0.953, P=0.032) were independently associated with overall
survival (Table III).
| Table III.Univariate and multivariate analyses
of clinicopathological factors for overall and disease-free
survival. |
Table III.
Univariate and multivariate analyses
of clinicopathological factors for overall and disease-free
survival.
|
| Overall
survival | Disease-free
survival |
|---|
|
|
|
|
|---|
|
| Survival rate
(%) | Univariate | Multivariate | Survival rate
(%) | Univariate | Multivariate |
|---|
|
| |
|
| |
|
|
|---|
| Variables | 1-year | 3-year | P value | HR (95% CI) | 1-year | 3-year | P value | HR (95% CI) |
|---|
| Gender |
|
|
|
|
|
|
|
|
| Male
(n=43) | 57.7 | 35.6 |
0.137 |
| 47.5 | 16.1 |
0.120 |
|
| Female
(n=29) | 55.1 | 23.7 |
|
| 50.6 | 30.1 |
|
|
| Age (years) |
|
|
|
|
|
|
|
|
| <55
(n=36) | 50.0 | 26.8 | 0.293 |
| 38.9 | 18.5 |
0.318 |
|
| ≥55
(n=36) | 60.4 | 36.3 |
|
| 54.8 | 24.7 |
|
|
| Child-Pugh
class |
|
|
|
|
|
|
|
|
| A
(n=63) | 60.1 |
33.7 | 0.013 |
| 52.0 | 28.4 |
0.005 |
|
| B
(n=9) | 22.2 | 0 |
|
| 15.3 | 0 |
|
|
| CRP (mg/l) |
|
|
|
|
|
|
|
|
| ≤10
(n=58) | 65.2 | 36.9 |
<0.001 |
| 57.8 | 32.7 | <0.001 |
|
| >10
(n=14) | 14.3 | 7.1 |
|
| 7.1 | 0 |
|
|
| Albumin (g/l) |
|
|
|
|
|
|
|
|
| <35
(n=16) | 37.5 | 7.8 | 0.016 |
| 25.0 | 0 | 0.007 |
|
| ≥35
(n=56) | 62.3 | 37.3 |
|
| 58.4 | 31.2 |
|
|
| HBV status |
|
|
|
0.032 |
|
|
| 0.006 |
|
Positive (n=34) | 67.6 | 47.2 | 0.009 |
(0.328–0.953) | 61.8 | 31.8 | 0.003 |
(0.232–0.785) |
|
Negative (n=38) | 43.8 | 18.4 |
|
| 31.9 | 10.2 |
|
|
| Vascular
invasion |
|
|
|
|
|
|
|
|
| Yes
(n=40) | 54.3 | 30.6 | 0.879 | | 46.4 | 27.0 | 0.875 |
|
| No
(n=32) | 53.1 | 31.3 |
|
| 50.0 | 21.9 |
|
|
| No. of tumours |
|
|
|
|
|
|
|
|
| 1
(n=55) | 54.2 | 31.5 | 0.838 |
| 42.1 | 25.2 |
0.820 |
|
| ≥2
(n=17) | 52.9 | 29.4 |
|
| 47.1 | 212 |
|
|
| Lymph node
metastasis |
|
|
|
|
|
|
|
|
|
Negative (n=51) | 62.3 | 38.1 |
0.001 |
| 60.3 | 35.6 |
0.002 |
|
|
Positive (n=21) | 38.1 | 14.3 |
|
| 28.6 | 0 |
|
|
| Tumour size
(cm) |
|
|
|
|
|
|
|
|
| ≤5
(n=20) | 69.6 | 44.7 | 0.054 |
| 69.1 | 43.0 | 0.028 |
|
| >5
(n=52) | 49.5 | 29.8 |
|
| 43.8 | 17.7 | |
|
| AFP (ng/ml) |
|
|
|
|
|
|
|
|
| <400
(n=43) | 62.1 | 39.2 | 0.082 |
| 61.0 | 29.4 | 0.076 |
|
| ≥400
(n=29) | 41.4 | 22.6 |
|
| 36.7 | 17.6 |
|
|
| ALT (U/l) |
|
|
|
|
|
|
|
|
| ≤40
(n=40) | 59.7 | 31.9 | 0.622 |
| 54.5 | 19.8 | 0.798 |
|
| >40
(n=32) | 52.9 | 33.1 |
|
| 46.2 | 26.0 |
|
|
| AST (U/l) |
|
|
|
|
|
|
|
|
| ≤40
(n=39) | 66.3 | 41.1 | 0.217 |
| 61.0 | 25.7 | 0.166 |
|
| >40
(n=33) | 45.5 | 22.6 |
|
| 38.8 | 19.8 |
|
|
| Total bilirubin
(µmol/l) |
|
|
|
|
|
|
|
|
| ≤17.1
(n=41) | 58.3 | 41.5 |
0.574 |
| 55.4 | 26.7 | 0.716 |
|
|
>17.1 (n=31) | 54.8 | 21.8 |
|
| 45.2 | 18.1 |
|
|
| CA19-9 (U/l) |
|
|
|
|
|
|
|
|
| <37
(n=27) | 66.0 | 38.8 | 0.038 |
| 62.0 | 32.5 | 0.046 |
|
| ≥37
(n=45) | 46.6 | 24.0 |
|
| 44.1 | 16.0 |
|
|
| Ascites |
|
|
|
|
|
|
|
|
|
Negative (n=63) | 56.9 | 33.6 | 0.676 |
| 50.4 | 24.7 | 0.597 |
|
|
Positive (n=9) | 53.3 | 20.0 |
|
| 40.0 | 15.2 |
|
|
| TNM
classification |
|
|
|
|
|
|
|
|
| I
(n=3) | 100 | 100 | 0.002 | 0.009 (1.188
3.367) | 100 | 100 |
<0.001 | 0.001
(1.565–5.066) |
| II
(n=24) | 70.1 | 48.8 |
|
| 65.2 | 34.5 |
|
|
| III
(n=45) | 44.4 | 20.0 |
|
| 37.8 | 11.1 |
|
|
| GPS |
|
|
|
0.025 |
|
|
| 0.045 |
| 0
(n=49) | 69.1 | 40.7 |
<0.001 |
(1.092–3.799) | 64.7 | 35.7 |
<0.001 |
(1.014–3.822) |
| 1 or 2
(n=23) | 30.4 | 10.4 |
|
| 21.7 | 0 |
|
|
GPS correlates with the recurrence of
ICC
Analysis of the time and frequency of ICC recurrence
following hepatectomy unveiled a significantly higher recurrence
frequency among the GPS-high patients compared with that among the
GPS-low patients. The GPS-low patients had a 35.3 and 64.7% risk of
developing recurrent disease after 1 and 3 years, respectively,
whereas ICC recurred in 78.3% of the GPS-high patients after 1 year
and 100% after 3 years, indicating a significantly poorer
progression-free survival (Fig. 2,
P<0.001). Multivariate analysis suggested that GPS (HR=1.969,
95% CI: 1.014–3.822, P=0.045), TNM classification (HR=2.816, 95%
CI: 1.565–5.066, P=0.001) and HBV positivity (HR=0.426, 95% CI:
0.232–0.785, P=0.006) were independent prognostic factors for ICC
recurrence (Table III).
Discussion
An association between inflammation and ICC
progression has been established. The risk factors for ICC
incidence vary with different geographic regions: In Asia, ICC is
mainly due to infection by pathogens including liver flukes and
hepatitis B and C viruses; in Western countries, it may be
attributed to chronic inflammation, primary sclerosing cholangitis,
obesity, hepatolithiasis, bacterial infection and bile
stasis-related chronic cholangitis (40). Chronic inflammation and biliary
irritation are, however, commonly shared among these diseases
(40). These support recent findings
that inflammation-based scores or parameters may be used as
prognostic markers for patients with cholangiocarcinoma (36,37). In
this study, we demonstrated that the inflammation-based prognostic
score, GPS, is associated with the recurrence and overall survival
of ICC patients and may be used as an independent prognostic
marker.
Analysis of clinicopathological data of 72 ICC
patients indicated that GPS classification precisely reflects the
preoperative CRP and albumin levels, Child-Pugh class, tumour size,
TNM classification, and the occurrence of ascites and lymph node
metastasis. Patients with high GPS scores (1 or 2) exhibited a
significantly shorter overall survival compared with those with a
low GPS score (0), although no statistically significant difference
was observed between patients with GPS scores of 1 and 2, which is
likely due to the limited number of patients in these two groups.
Our analysis using the Cox hazards model suggested that GPS, as
well as TNM classification and HBV positivity, is an independent
prognostic factor for the recurrence of ICC and the overall patient
survival.
Although GPS has frequently been associated with the
prognosis of solid tumours, such as lung (22,23),
liver (27,28), kidney (26), ovarian (24), colorectal (25), gastric (41,42) and
pancreatic cancer (43), the
association has yet to be fully elucidated. One component of the
GPS score, CRP, is an acute phase protein synthesized by
hepatocytes in response to inflammation, infection, tissue damage
and cancer, reflecting systemic inflammation (44). Although there is no causal
association between elevated CRP and cancer development, the
cytokines that mediate CRP, such as IL-1, IL-6 and TNF, are key
pro-inflammatory factors in hepatobiliary inflammation and cancer
(45). For example, IL-6 contributes
to the growth of malignant cholangiocytes by affecting the promoter
methylation and expression of several genes, including epidermal
growth factor receptor (46). IL-6
also promotes malignant cholangiocyte growth by activating the
mitogen-activated protein kinase pathway and enhancing the
expression of the anti-apoptotic protein myeloid cell leukemia-1 in
an either autocrine or paracrine manner (47,48).
These are consistent with the significant preoperative increase of
IL-6 in the serum of patients with cholangiocarcinoma and its
apparent decrease after surgery (49,50).
IL-1 family cytokines and TNF also facilitate oncogenesis of
cholangiocarcinoma, as previously described (51–53).
These may partially underlie the mechanism through which GPS score
correlates with the prognosis of ICC patients.
Preoperative serum albumin reflects nutritional
status (54,55); it decreases in response to systemic
inflammation during malignant tumour growth, leading to
hypoalbuminemia and weight loss (56), which may in turn affect the immune
system of the cancer patients (57).
Hypoalbuminemia therefore suggests systemic inflammation and immune
suppression, in association with the initiation and progression of
malignant tumours, and has been reported as an independent
prognostic marker for ICC (58).
These findings explain the correlation of GPS with recurrence and
prognosis of ICC patients observed in this study.
Our data indicated that 47.2% of ICC patients were
positive for hepatitis B surface antigen, and these patients
generally exhibited longer overall and progression-free survival.
Accumulating evidence suggests a correlation of ICC development
with HBV infection (59,60). HBV DNA may be detectable in tumour
tissues from a proportion of the ICC patients (61,62).
Chronic HBV and hepatitis C virus infection represent risk factors
for ICC occurrence based on a meta-analysis of 13 case-control and
3 cohort studies (63). However, ICC
patients carrying HBV had a better prognosis compared with those
without HBV infection (64,65). This is likely due to a lower tendency
for metastasis towards the perihepatic lymph nodes and a higher
rate of encapsulation in ICC patients with HBV (66,67). In
addition, the immunological memory caused by a previous HBV
infection may be quickly activated by the HBV-relevant ICC,
promoting antitumour immunity (68,69).
The prognosis of ICC is currently assessed
postoperatively by the complicated TNM classification, the
Barcelona Clinic Liver Cancer staging system (70), and the Cancer Liver Italian Program
scoring system (71). GPS scoring
represents a simple and easily applicable method, based on
preoperative serum CRP and albumin levels, which may be determined
biochemically. The present study revealed a significant correlation
between the overall and progression-free survival of ICC patients
following resection and their preoperative GPS scores, and supports
GPS as an effective and easily achievable prognostic marker for ICC
patients.
Acknowledgements
We would like to thank all the members of the
Department of Oncological Surgery of the First Affiliated Hospital
of Fujian Medical University for their help and support.
References
|
1
|
Guest RV, Boulter L, Kendall TJ,
Minnis-Lyons SE, Walker R, Wigmore SJ, Sansom OJ and Forbes SJ:
Cell lineage tracing reveals a biliary origin of intrahepatic
cholangiocarcinoma. Cancer Res. 74:1005–1010. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nakanuma Y, Sripa B, Batanasapt V, Leong
ASY, Ponchon T and Ishak KG: Intrahepatic cholangiocarcinoma.
Pathology and Genetics of Tumours of the Digestive SystemWorld
Health Organization of Tumours. Hamilton SR and Aaltonen LA: IARC;
Lyon: pp. 173–180. 2000
|
|
3
|
Farges O, Fuks D, Le Treut YP, et al: AJCC
7th edition of TNM staging accurately discriminates outcomes of
patients with resectable intrahepatic cholangiocarcinoma:by the
AFC-IHCC-2009 study group. Cancer. 117:2170–2177. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zou S, Li J, Zhou H, Frech C, Jiang X, Chu
JS, Zhao X, Li Y, Li Q, Wang H, et al: Mutational landscape of
intrahepatic cholangiocarcinoma. Nat Commun. 5:56962014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wang JD and Quan ZW: The molecular
mechanism of cholangiocarcinoma. J Pract Oncol Chin. 22:96–98.
2007.
|
|
6
|
de Jong MC, Nathan H, Sotiropoulos GC,
Paul A, Alexandrescu S, Marques H, Pulitano C, Barroso E, Clary BM,
Aldrighetti L, et al: Intrahepatic cholangiocarcinoma: An
international multi-institutional analysis of prognostic factors
and lymph node assessment. J Clin Oncol. 29:3140–3145. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
de Groen PC, Gores GJ, LaRusso NF,
Gunderson LL and Nagorney DM: Biliary tract cancers. N Engl J Med.
341:1368–1378. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Li T, Qin LX, Zhou J, Sun HC, Qiu SJ, Ye
QH, Wang L, Tang ZY and Fan J: Staging, prognostic factors and
adjuvant therapy of intrahepatic cholangiocarcinoma after curative
resection. Liver Int. 34:953–960. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Li H, Wu JS, Wang XT, Lv P, Gong LS, Liu
G, Tian BN, Li YY and Jiang B: Factors predicting surgical
resection in patients with intrahepatic cholangiocarcinoma and
cirrhosis. J Invest Surg. 27:219–225. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang Y, Li J, Xia Y, Gong R, Wang K, Yan
Z, Wan X, Liu G, Wu D, Shi L, et al: Prognostic nomogram for
intrahepatic cholangiocarcinoma after partial hepatectomy. J Clin
Oncol. 31:1188–1195. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Paik KY, Jung JC, Heo JS, Choi SH, Choi DW
and Kim YI: What prognostic factors are important for resected
intrahepatic cholangiocarcinoma? J Gastroenterol Hepatol.
23:766–770. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kinoshita A, Onoda H, Imai N, Iwaku A,
Oishi M, Tanaka K, Fushiya N, Koike K, Nishino H, Matsushima M, et
al: The Glasgow Prognostic Score, an inflammation based prognostic
score, predicts survival in patients with hepatocellular carcinoma.
BMC Cancer. 13:522013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Roxburgh CS and McMillan DC: Role of
systemic inflammatory response in predicting survival in patients
with primary operable cancer. Future Oncol. 6:149–163. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Argilés JM, Busquets S, Toledo M and
López-Soriano FJ: The role of cytokines in cancer cachexia. Curr
Opin Support Palliat Care. 3:263–268. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Balkwill F and Mantovani A: Inflammation
and cancer: Back to Virchow? Lancet. 357:539–545. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kusumanto YH, Dam WA, Hospers GA, Meijer C
and Mulder NH: Platelets and granulocytes in particular the
neutrophils from important compartments for circulating vascular
endothelial growth factor. Angiogenesis. 6:283–287. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ulich TR, Del Castillo J and Guo KZ: In
vivo hematologic effects of recombinant interleukin-6 on
hematopoiesis and circulating numbers of RBCs and WBCs. Blood.
73:108–110. 1989.PubMed/NCBI
|
|
18
|
Philip M, Rowley DA and Schreiber H:
Inflammation as a tumor promoter in cancer induction. Semin Cancer
Biol. 14:433–439. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Heikkilä KK, Ebrahim S and Lawlor DA: A
systematic review of the association between circulating
concentrations of C reactive protein and cancer. Epidemiol
Community Health. 61:824–833. 2007. View Article : Google Scholar
|
|
20
|
Kulbe H, Chakravarty P, Leinster DA,
Charles KA, Kwong J, Thompson RG, et al: A dynamic inflammatory
cytokine network in the human ovarian cancer microenvironment.
Cancer Res. 72:66–75. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Coward J, Kulbe H, Chakravarty P, Leader
D, Vassileva V, Leinster DA, Thompson R, Schioppa T, Nemeth J,
Vermeulen J, et al: Interleukin-6 as a therapeutic target in human
ovarian cancer. Clin Cancer Res. 17:6083–6096. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tomita M, Ayabe T, Chosa E and Nakamura K:
Prognostic significance of pre- and postoperative glasgow
prognostic score for patients with non-small cell lung cancer.
Anticancer Res. 34:3137–3140. 2014.PubMed/NCBI
|
|
23
|
Jiang AG, Chen HL and Lu HY: Comparison of
Glasgow prognostic score and prognostic index in patients with
advanced non-small cell lung cancer. J Cancer Res Clin Oncol.
141:563–568. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sharma R, Hook J, Kumar M and Gabra H:
Evaluation of an inflammation-based prognostic score in patients
with advanced ovarian cancer. Eur J Cancer. 44:251–256. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ikeguchi M, Urushibara S, Shimoda R,
Yamamoto M, Maeta Y and Ashida K: Inflammation-based prognostic
scores and nutritional prognostic index in patients with
locally-advanced unresectable colorectal cancer. World J Surg
Oncol. 12:2102014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ramsey S, Lamb GW, Aitchison M, Graham J
and McMillan DC: Evaluation of an inflammation-based prognostic
score in patients with metastatic renal cancer. Cancer.
109:205–212. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Pan QX, Zhang JH, Su ZJ, Wang CR and Ke
SY: The Glasgow Prognostic Score is an independent prognostic
predictor of hepatocellular carcinoma following radical resection.
Oncol Res Treat. 37:192–197. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ishizuka M, Kubota K, Kita J, Shimoda M,
Kato M and Sawada T: Impact of an inflammation-based prognostic
system on patients undergoing surgery for hepatocellular carcinoma:
A retrospective study of 398 Japanese patients. Am J Surg.
203:101–106. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kaneko M, Nozawa H, Sasaki K, Hongo K,
Hiyoshi M, Tada N, Murono K, Nirei T, Kawai K, Sunami E, et al:
Elevated neutrophil to lymphocyte ratio predicts poor prognosis in
advanced colorectal cancer patients receiving oxaliplatin-based
chemotherapy. Oncology. 82:261–268. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Oh BS, Jang JW, Kwon JH, You CR, Chung KW,
Kay CS, Jung HS and Lee S: Prognostic value of C-reactive protein
and neutrophil-to-lymphocyte ratio in patients with hepatocellular
carcinoma. BMC Cancer. 13:782013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kwon HC, Kim SH, Oh SY, Lee S, Lee JH,
Choi HJ, Park KJ, Roh MS, Kim SG, Kim HJ, et al: Clinical
significance of preoperative neutrophil-lymphocyte versus
platelet-lymphocyte ratio in patients with operable colorectal
cancer. Biomarkers. 17:216–222. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Smith RA, Bosonnet L, Raraty M, Sutton R,
Neoptolemos JP, Campbell F and Ghaneh P: Preoperative
platelet-lymphocyte ratio is an independent significant prognostic
marker in resected pancreatic ductal adenocarcinoma. Am J Surg.
197:466–472. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kasymjanova G, MacDonald N, Agulnik JS,
Cohen V, Pepe C, Kreisman H, Sharma R and Small D: The predictive
value of pre-treatment inflammatory markers in advanced
non-small-cell lung cancer. Curr Oncol. 17:52–58. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Proctor MJ, Morrison DS, Talwar D, Balmer
SM, Fletcher CD, O'Reilly DS, Foulis AK, Horgan PG and McMillan DC:
A comparison of inflammation-based prognostic scores in patients
with cancer. A Glasgow Inflammation Outcome Study. Eur J Cancer.
47:2633–2641. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Pinato DJ, North BV and Sharma R: A novel,
externally validated inflammation-based prognostic algorithm in
hepatocellular carcinoma: The prognostic nutritional index (PNI).
Br J Cancer. 106:1439–1445. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Gomez D, Morris-Stiff G, Toogood GJ, Lodge
JP and Prasad KR: Impact of systemic inflammation on outcome
following resection for intrahepatic cholangiocarcinoma. J Surg
Oncol. 97:513–518. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Oshiro Y, Sasaki R, Fukunaga K, Kondo T,
Oda T, Takahashi H and Ohkohchi N: Inflammation-based prognostic
score is a useful predictor of postoperative outcome in patients
with extrahepatic cholangiocarcinoma. J Hepatobiliary Pancreat Sci.
20:389–395. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Hiraoka A, Kawamura T, Aibiki T, Okudaira
T, Toshimori A, Yamago H, Nakahara H, Suga Y, Azemoto N, Miyata H,
et al: Prognosis and therapy for ruptured hepatocellular carcinoma:
Problems with staging and treatment strategy. Eur J Radiol.
84:366–371. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Edmondson HA and Steiner PE: Primary
carcinoma of the liver: A study of 100 cases among 48,900
necropsies. Cancer. 7:462–503. 1954. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Leyva-Illades D, McMillin M, Quinn M and
Demorrow S: Cholangiocarcinoma pathogenesis: Role of the tumor
microenvironment. Transl Gastrointest Cancer. 1:71–80.
2012.PubMed/NCBI
|
|
41
|
Dutta S, Crumley AB, Fullarton GM, Horgan
PG and McMillan DC: Comparison of the prognostic value of tumour
and patient related factors in patients undergoing potentially
curative resection of gastric cancer. Am J Surg. 204:294–299. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Wang DS, Ren C, Qiu MZ, Luo HY, Wang ZQ,
Zhang DS, Wang FH, Li YH and Xu RH: Comparison of the prognostic
value of various preoperative inflammation-based factors in
patients with stage III gastric cancer. Tumour Biol. 33:749–756.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Glen P, Jamieson NB, McMillan DC, Carter
R, Imrie CW and McKay CJ: Evaluation of an inflammation-based
prognostic score in patients with inoperable pancreatic cancer.
Pancreatology. 6:450–453. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Allin KH and Nordestgaard BG: Elevated
C-reactive protein in the diagnosis, prognosis, and cause of
cancer. Crit Rev Clin Lab Sci. 48:155–170. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Johnson C, Han Y, Hughart N, McCarra J,
Alpini G and Meng F: Interleukin-6 and its receptor, key players in
hepatobiliary inflammation and cancer. Transl Gastrointest Cancer.
1:58–70. 2012.PubMed/NCBI
|
|
46
|
Wehbe H, Henson R, Meng F, Mize-Berge J
and Patel T: Interleukin-6 contributes to growth in
cholangiocarcinoma cells by aberrant promoter methylation and gene
expression. Cancer Res. 66:10517–10524. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Park J, Tadlock L, Gores GJ and Patel T:
Inhibition of interleukin 6-mediated mitogen-activated protein
kinase activation attenuates growth of a cholangiocarcinoma cell
line. Hepatology. 30:1128–1133. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Meng F, Yamagiwa Y, Ueno Y and Patel T:
Over-expression of interleukin-6 enhances cell survival and
transformed cell growth in human malignant cholangiocytes. J
Hepatol. 44:1055–1065. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Heimbach JK, Gores GJ, Haddock MG, Alberts
SR, Nyberg SL, Ishitani MB and Rosen CB: Liver transplantation for
unresectable perihilar cholangiocarcinoma. Semin Liver Dis.
24:201–207. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Jarnagin WR, Fong Y, DeMatteo RP, Gonen M,
Burke EC, BS J Bodniewicz, BA M Youssef, Klimstra D and Blumgart
LH: Staging, resectability, and outcome in 225 patients with hilar
cholangiocarcinoma. Ann Surg. 234:507–517, discussion 517–519.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Yamada D, Rizvi S, Razumilava N, Bronk SF,
Davila JI, Champion MD, Borad MJ, Bezerra JA, Chen X and Gores GJ:
IL-33 facilitates oncogene-induced cholangiocarcinoma in mice by an
interleukin-6-sensitive mechanism. Hepatology. 61:1627–1642. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Jaiswal M, LaRusso NF, Burgart LJ and
Gores GJ: Inflammatory cytokines induce DNA damage and inhibit DNA
repair in cholangiocarcinoma cells by a nitric oxide-dependent
mechanism. Cancer Res. 60:184–190. 2000.PubMed/NCBI
|
|
53
|
Maemura K, Natsugoe S and Takao S:
Molecular mechanism of cholangiocarcinoma carcinogenesis. J
Hepatobiliary Pancreat Sci. 21:754–760. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Gupta D and Lis CG: Pretreatment serum
albumin as a predictor of cancer survival: A systematic review of
the epidemiological literature. Nutr J. 9:692010. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Lien YC, Hsieh CC, Wu YC, Hsu HS, Hsu WH,
Wang LS, Huang MH and Huang BS: Preoperative serum albumin level is
a prognostic indicator for adenocarcinoma of the gastric cardia. J
Gastrointest Surg. 8:1041–1048. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
McMillan DC, Watson WSO, O'Gorman P,
Preston T, Scott HR and McArdle CS: Albumin concentrations are
primarily determined by the body cell mass and the systemic
inflammatory response in cancer patients with weight loss. Nutr
Cancer. 39:210–213. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Ohki S, Shibata M, Gonda K, Machida T,
Shimura T, Nakamura I, Ohtake T, Koyama Y, Suzuki S, Ohto H, et al:
Circulating myeloid-derived suppressor cells are increased and
correlate to immune suppression, inflammation and hypoproteinemia
in patients with cancer. Oncol Rep. 28:453–458. 2012.PubMed/NCBI
|
|
58
|
Nakeeb A, Pitt HA, Sohn TA, Coleman J,
Abrams RA, Piantadosi S, Hruban RH, Lillemoe KD, Yeo CJ and Cameron
JL: Cholangiocarcinoma. A spectrum of intrahepatic, perihilar, and
distal tumors. Ann Surg. 224:463–473, discussion 473–475. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Tanaka M, Tanaka H, Tsukuma H, Ioka A,
Oshima A and Nakahara T: Risk factors for intrahepatic
cholangiocarcinoma: A possible role of hepatitis B virus. J Viral
Hepat. 17:742–748. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Donato F, Gelatti U, Tagger A, Favret M,
Ribero ML, Callea F, Martelli C, Savio A, Trevisi P and Nardi G:
Intrahepatic cholangiocarcinoma and hepatitis C and B virus
infection, alcohol intake, and hepatolithiasis: A case-control
study in Italy. Cancer Causes Control. 12:959–964. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Wu Y, Wang T, Ye S, Zhao R, Bai X, Wu Y,
Abe K and Jin X: Detection of hepatitis B virus DNA in
paraffin-embedded intrahepatic and extrahepatic cholangiocarcinoma
tissue in the northern Chinese population. Hum Pathol. 43:56–61.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Perumal V, Wang J, Thuluvath P, Choti M
and Torbenson M: Hepatitis C and hepatitis B nucleic acids are
present in intrahepatic cholangiocarcinomas from the United States.
Hum Pathol. 37:1211–1216. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Zhou Y, Zhao Y, Li B, Huang J, Wu L, Xu D,
Yang J and He J: Hepatitis viruses infection and risk of
intrahepatic cholangiocarcinoma: Evidence from a meta-analysis. BMC
Cancer. 12:2892012. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Zhou HB, Wang H, Li YQ, Li SX, Wang H,
Zhou DX, Tu QQ, Wang Q, Zou SS, Wu MC, et al: Hepatitis B virus
infection: A favorable prognostic factor for intrahepatic
cholangiocarcinoma after resection. World J Gastroenterol.
17:1292–1303. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Zhang L, Cai JQ, Zhao JJ, Bi XY, Tan XG,
Yan T, Li C and Zhao P: Impact of hepatitis B virus infection on
outcome following resection for intrahepatic cholangiocarcinoma. J
Surg Oncol. 101:233–238. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Peng NF, Li LQ, Qin X, Guo Y, Peng T, Xiao
KY, Chen XG, Yang YF, Su ZX, Chen B, et al: Evaluation of risk
factors and clinicopathologic features for intrahepatic
cholangiocarcinoma in Southern China: A possible role of hepatitis
B virus. Ann Surg Oncol. 18:1258–1266. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Zhou H, Wang H, Zhou D, Wang H, Wang Q,
Zou S, Tu Q, Wu M and Hu H: Hepatitis B virus-associated
intrahepatic cholangiocarcinoma and hepatocellular carcinoma may
hold common disease process for carcinogenesis. Eur J Cancer.
46:1056–1061. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Llovet JM, Brú C and Bruix J: Prognosis of
hepatocellular carcinoma: The BCLC staging classification. Semin
Liver Dis. 19:329–338. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Ding FX, Wang F, Lu YM, Li K, Wang KH, He
XW and Sun SH: Multiepitope peptide-loaded virus-like particles as
a vaccine against hepatitis B virus-related hepatocellular
carcinoma. Hepatology. 49:1492–1502. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Ward SM, Phalora P, Bradshaw D,
Leyendeckers H and Klenerman P: Direct ex vivo evaluation of
long-lived protective antiviral memory B cell responses against
hepatitis B virus. J Infect Dis. 198:813–817. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
No authors listed: A new prognostic system
for hepatocellular carcinoma: a retrospective study of 435
patients: the Cancer of the Liver Italian Program (CLIP)
investigators. Hepatology. 28:751–755. 1998. View Article : Google Scholar : PubMed/NCBI
|