Introduction
Kidney cancer accounts for ~4% of all cancers
worldwide and renal cell carcinoma (RCC) is the most common type of
kidney cancer (1–3). Radical nephrectomy is usually performed
for advanced RCC; however, recurrence with distant metastasis
occurs in >25% of the patients (4) and chemotherapy is employed for these
metastatic RCC (mRCC) patients. While interleukin (IL)-2 and
interferon (IFN)-α have been used for mRCC (5,6),
molecular-targeted drugs, such as multi-kinase inhibitors, have
been recently developed and exhibit great efficacy for mRCC,
resulting in improved survival (7–9). In
particular, a pivotal study that investigated sunitinib treatment
demonstrated a median overall survival of 32 months for mRCC
(10). The current standard therapy
for mRCC is thus the first-line use of these molecular-targeted
drugs.
To predict the prognosis of mRCC patients treated
with IFN-γ, the Memorial Sloan-Kettering Cancer Center (MSKCC)
index, which includes measurements of performance status, serum
lactate dehydrogenase level, serum calcium level, hemoglobin and
time interval from diagnosis to therapy, was established (11). The Heng model was proposed for
predicting the prognosis of mRCC patients who were treated with
anti-angiogenesis inhibitors and the parameters assayed included
neutrophil and platelet counts (12,13). The
appropriateness of the index used is based on the acknowledgement
of the close association between the clinical course of mRCC and
inflammatory status. Increased serum levels of inflammatory
cytokines in RCC patients have been reported (14–16),
whereas other parameters associated with inflammatory conditions
include not only fever, erythrocyte sedimentation rate and
C-reactive protein (CRP) levels (17), but also neutrophil and lymphocyte
counts (18–21).
Inflammatory cytokines, such as IL-1β and IL-6, are
known to induce systemic inflammation, alteration of systemic
metabolism, atrophy of muscle and fat tissue and loss of appetite
and body weight, resulting in cancer cachexia. A strong association
between inflammatory status and cachexia has also been reported in
cancers of the stomach, lung and pancreas (22–26).
One of the inflammation-based prognostic indices,
the modified Glasgow Prognostic Score (mGPS), is a simple scoring
system that is calculated based on serum CRP and albumin levels and
has been widely used as a predictive tool for mRCC (27–29).
Since the current therapy for mRCC is monotherapy with
molecular-targeted agents, determination of the association between
the efficacy of these therapies and inflammatory conditions is
required. However, the prognostic value of mGPS in mRCC patients
treated with molecular-targeted drugs remains unclear. In the
present study, we retrospectively investigated the mGPS and the
therapeutic effects of molecular-targeted drugs in Japanese
patients with advanced RCC in a single institution.
Patients and methods
Patients
A total of 45 RCC patients who were treated at the
Department of Medical Oncology, Clinical Research Institute,
National Hospital Organization Kyushu Medical Center (Fukuoka,
Japan) between October, 2009 and August, 2015 were screened. Of
these patients, 32 with histologically and/or radiographically
confirmed advanced RCC who were treated with a molecular-targeted
drug as first-line therapy were investigated. The eligibility
criteria were as follows: Measurable or evaluable tumor lesions
according to the Response Evaluation Criteria in Solid Tumors
guidelines, version 1.1 (https://ctep.cancer.gov/protocoldevelopment/docs/recist_guideline.pdf),
confirmation of the date of death or progressive disease, and no
evidence of active infection. There was no restriction regarding
Eastern Cooperative Oncology Group (ECOG) performance status (PS)
or previous cytokine therapies. This study was approved by the
Ethics Committee of the National Organization Kyushu Medical Center
and was conducted according to the guidelines for biomedical
research specified in the Declaration of Helsinki. Due to the
retrospective nature of the present study, patient informed consent
was not obtained.
Clinical variables assessed
Information on patient characteristics and clinical
data were retrieved from medical records and retrospectively
reviewed. The items surveyed in this study included age, gender,
PS, primary tumor site, histopathological diagnosis, metastatic and
recurrent sites, tumor status and previous renal surgery.
Information regarding systemic chemotherapy included the
chemotherapy regimen, progression-free survival (PFS), overall
survival (OS), reasons for terminating initial chemotherapy and
subsequent therapies. Information associated with inflammatory
conditions included the results of blood tests (white blood cells,
neutrophils, lymphocytes, hemoglobin, platelets, albumin and CRP)
and the mGPS. All data corresponded to the period within 7 days
prior to chemotherapy initiation.
The mGPS consists of two factors, namely ther serum
levels of CRP (normal range, 0.00–0.30 mg/dl) and albumin (normal
range, 4.0–5.0 g/dl) (30). Patients
with an increment in the CRP level (>1.0 mg/dl) and a decrease
in the albumin level (<3.5 g/dl) were assigned a score of 2,
those with only an increment in the CRP level (>1.0 mg/dl) were
assigned a score of 1, and those with a normal serum CRP level were
assigned a score of 0.
Statistical analysis
PFS was defined as the period from the initiation of
therapy to the day of tumor progression or death from any cause. OS
was defined as the period from initiation of therapy to the day of
death from any cause. The Kaplan-Meier method was used to estimate
PFS and OS, and the log-rank test was used to compare the two
groups according to the mGPS. Correlations between survival and
clinicopathological characteristics were analyzed by using
Wilcoxon's test and Pearson's Chi-square test. P<0.05 was
considered to indicate statistically significant differences. All
the analyses were performed using SPSS software, version 21 (IBM
SPSS, Armonk, NY, USA).
Results
Patient characteristics
The median age of the 32 patients was 66 years
(range, 33–82 years) (Table I); 20
men (62.5%) and 12 women (37.5%) were included. In terms of
histological diagnosis of the renal tumor, clear cell carcinoma was
diagnosed in 21 patients (65.5%); papillary or sarcomatoid cancer
was diagnosed in 5 patients (15.6%), and in 6 patients (18.8%) the
type of the tumor was unknown. A total of 25 patients (78.1%)
underwent surgical resection of RCC; 16 patients (50%) received
prior cytokine therapies, including IFN-α and IL-2; the remaining
16 patients had received no prior treatment. An ECOG PS of 0, 1, 2,
3 and 4 was observed in 15, 13, 2, 1 and 1 patients (46.9, 40.6,
6.3, 3.1 and 3.1%), respectively. Patients with a PS of 3 or 4 were
considered suitable to receive chemotherapy, as their poor PS was
attributed to pain from bone metastasis or bone fracture. When the
MSKCC risk index was calculated, 1 (3.1%) of the patients was
classed as favorable-risk, 23 (71.9%) were intermediate-risk and 8
(25.0%) were poor-risk. When risk was calculated according to the
Heng risk group, 1 (3.1%) of the patients were favorable-risk, 20
(62.5%) were intermediate-risk and 11 (34.4%) were poor-risk.
 | Table I.Patient characteristics (n=32). |
Table I.
Patient characteristics (n=32).
| Characteristics | N (%) |
|---|
| Age, years |
| Mean | 65.4 |
| Median
(range) | 66 (33.0–82.0) |
| Gender |
| Male | 20 (62.5) |
|
Female | 12 (37.5) |
| Histological
type |
| Clear
cell carcinoma | 21 (65.6) |
|
Others | 5 (15.6) |
|
Unknown | 6 (18.8) |
| Resection of the
primary lesion |
|
Present | 25 (78.1) |
|
Absent | 7 (21.9) |
| Previous treatment
(e.g., cytokines) |
|
Present | 16 (50.0) |
|
Absent | 16 (50.0) |
| ECOG performance
status |
| 0 | 15 (46.9) |
| 1 | 13 (40.6) |
| 2 | 2 (6.3) |
| 3 | 1 (3.1) |
| 4 | 1 (3.1) |
| MSKCC risk
group |
|
Favorable | 1 (3.1) |
|
Intermediate | 23 (71.9) |
|
Poor | 8 (25.0) |
| Heng risk
group |
|
Favorable | 1 (3.1) |
|
Intermediate | 20 (62.5) |
|
Poor | 11 (34.4) |
| WBC (/µl) |
|
Mean | 6,403.1 |
| Median
(range) | 6,050
(2,100-11,900) |
| C-reactive protein
(mg/dl) |
|
Mean | 3.26 |
| Median
(range) | 0.36
(0.03–21.03) |
| Albumin (g/dl) |
|
Mean | 3.74 |
| Median
(range) | 3.85
(2.30–4.30) |
| LDH (mg/dl) |
|
Mean | 264.7 |
| Median
(range) | 189.5
(108.0-2,498.0) |
| Corrected calcium
(mg/dl) |
|
Mean | 9.54 |
| Median
(range) | 9.45
(8.30–12.30) |
| Creatinine
(mg/dl) |
|
Mean | 0.94 |
| Median
(range) | 0.91
(0.40–1.40) |
|
Neutrophil/lymphocyte ratio |
|
Mean | 5.02 |
| Median
(range) | 3.12
(0.80–37.80) |
|
Characteristics | N (%) |
| Modified GPS |
| 0 | 21 (65.6) |
| 1 | 3 (9.4) |
| 2 | 8 (25.0) |
| Sequential
therapy |
|
None | 5 (15.6) |
|
Second-line | 19 (59.4) |
| Third-
or further-line | 9 (28.1) |
| Progression-free
survival (days) |
|
Mean | 258 |
| Median
(range) | 212
(13.0–960.0) |
| Overall survival
(days) |
|
Mean | 738 |
| Median
(range) | 487.5
(30.0-2,137.0) |
The mean value of the serum CRP level was 3.26 mg/dl
and its range was 0.03–21.15 mg/dl, indicating wide variation among
patients. A total of 21 patients (65.5%) had an mGPS of 0, 3 (9.4%)
had an mGPS of 1, and 8 (25.0%) had an mGPS of 2. A total of 5
patients (15.6%) did not receive subsequent therapy, 19 (59.4%)
received up to second-line chemotherapy, and 9 (28.1%) received
third- or further-line chemotherapy.
Efficacy
The median PFS of all patients was 212.0 days [95%
confidence interval (CI): 13.0–960] and the median OS was 487.5
days (95% CI: 30.0–2,137.0).
Correlation analysis of survival and
clinical factors
The correlation between survival and clinical
parameters was then examined (Table
II). A longer PFS and OS were significantly correlated with the
MSKCC risk group, the Heng risk group and PS. Clinical parameters
corresponding to inflammatory status, including
neutrophil/lymphocyte ratio (NLR), serum CRP level, serum albumin
level and mGPS, were also significantly associated with PFS and OS.
The correlation index of the mGPS was the highest (R=0.575,
P=0.001) among all of the parameters examined. Receiving subsequent
therapies was significantly correlated with PFS (R=0.437, P=0.012),
but not with OS (R=0.273, P=0.131).
| Table II.Correlation analysis of survival and
clinical factors. |
Table II.
Correlation analysis of survival and
clinical factors.
| Factors | Progression-free
survival | Overall
survival |
|---|
| Age | 0.247 (0.173) | 0.218 (0.232) |
| Gender | 0.059 (0.747) | 0.063 (0.732) |
| Resection of the
primary lesion | 0.250 (0.168) | 0.323 (0.071) |
| MSKCC risk
group | 0.451
(0.010) | 0.499
(0.004) |
| Heng risk
group | 0.427
(0.015) | 0.556
(0.001) |
| Previous
treatment | 0.152 (0.405) | 0.135 (0.460) |
| ECOG
performance | 0.523
(0.002) | 0.554
(0.001) |
| status |
|
| WBC | 0.264 (0.145) | 0.261 (0.149) |
| NLR | 0.531
(0.002) | 0.533
(0.002) |
| C-reactive
Protein | 0.390
(0.027) | 0.485
(0.005) |
| Albumin | 0.427
(0.015) | 0.613
(<0.0001) |
| mGPS | 0.575
(0.001) | 0.591
(<0.0001) |
| LDH | 0.263 (0.146) | 0.183 (0.315) |
| Corrected
calcium | 0.135 (0.461) | 0.065 (0.722) |
| Creatinine | 0.098 (0.592) | 0.049 (0.788) |
| PFS | – | 0.743
(<0.0001) |
| OS | 0.743
(<0.0001) | – |
| Sequential
therapy | 0.437
(0.012) | 0.273 (0.131) |
Inflammatory conditions and
therapeutic effects
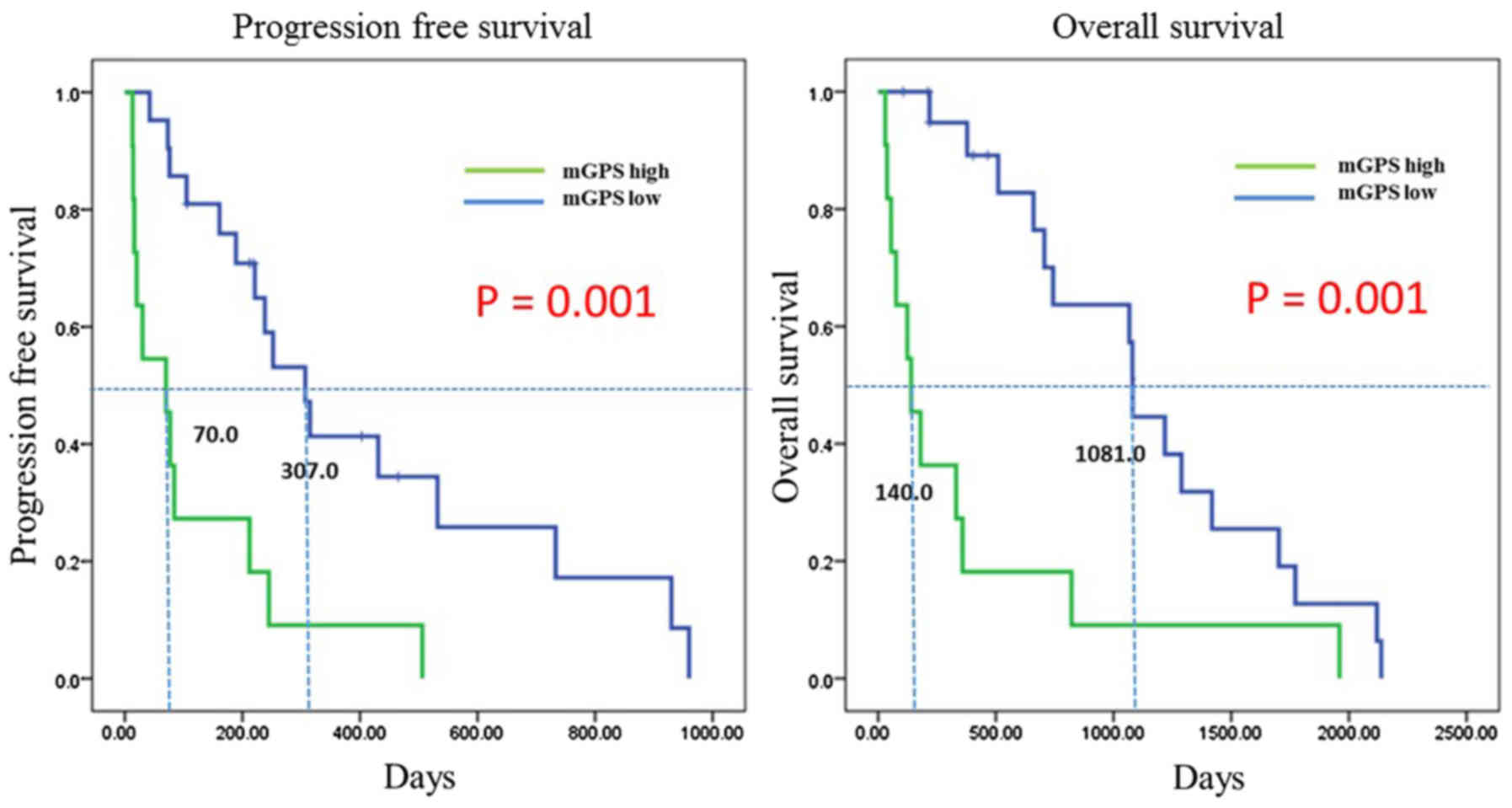
Since a correlation of mGPS with survival was
demonstrated, PFS and OS were further examined with regard to the
mGPS (Fig. 1). The total patients
were categorized into one of two groups: Patients with an mGPS of 0
were assigned to the mGPS low group, whereas those with an mGPS of
1 or 2 were assigned to the mGPS high group. The median PFS of the
mGPS low group was significantly longer compared with that of the
mGPS high group (307.0 vs. 70.0 days, respectively; P=0.001) based
on the Kaplan-Meyer analysis. The median OS of the mGPS low group
was also significantly longer compared with that of the mGPS high
group (1,081.0 vs. 140.0 days, respectively; P=0.001). These data
suggested that molecular-targeted drugs achieved a more favorable
survival in patients of the mGPS low group, who are considered to
be of low inflammatory status.
Therapy and inflammatory
conditions
In order to assess the reasons for the favorable
survival of the mGPS low group, each clinical factor was compared
between the two mGPS patient groups (Table III). While all the mGPS low
patients had an ECOG PS of 0 or 1 (100%), only 63% of the mGPS high
patients had a PS of 0 or 1 (P<0.038). An MSKCC poor risk was
observed in 10% of the mGPS low patients, but in 55% of mGPS high
patients (P<0.018). In terms of histological diagnosis, based on
its molecular mechanisms, clear cell carcinoma is considered to be
more sensitive to molecular-targeted drugs compared with tumors of
other histological types. Clear cell carcinoma was observed in 86%
of the mGPS low and in 45% of the mGPS high patients (P<0.05).
These results suggested that mGPS high patients included a
population with a poor general condition and drug resistance.
Regarding initial therapy, sunitinib was administered in 57% of the
mGPS low patients and in 54% of the mGPS high patients (P=0.065),
suggesting no significant differences between the two groups.
Although 63.6% of the mGPS high patients received initial therapy
alone, only 5% of the mGPS low patients received initial therapy
alone. The percentage of patients who received second-line therapy
in the mGPS low and mGPS high groups was 72 and 36%, respectively,
and the percentage of patients who received third- or further-line
therapy was 33 and 18%, respectively (P=0.003).
| Table III.Therapy and inflammatory status of
the mGPS low and high patient groups. |
Table III.
Therapy and inflammatory status of
the mGPS low and high patient groups.
|
| mGPS low | mGPS high |
|
|---|
|
|
|
|
|
|---|
| Variables | n=21 | (%) | n=11 | (%) | P-value |
|---|
| ECOG PS |
|
|
|
| 0.038a |
| 0 | 12 | 57 | 3 | 27 |
| 1 | 9 | 43 | 4 | 36 |
| 2 | 0 | 0 | 2 | 18 |
| 3 | 0 | 0 | 1 | 9 |
| 4 | 0 | 0 | 1 | 9 |
| MSKCC |
|
|
|
| 0.018b |
|
Favorable | 1 | 4 | 0 | 0 |
|
Intermediate | 18 | 86 | 5 | 45 |
|
Poor | 2 | 10 | 6 | 55 |
| Histology |
|
|
|
| 0.018b |
| CC | 18 | 86 | 5 | 45 |
|
pRCC | 0 | 0 | 3 | 27 |
|
Others | 3 | 14 | 3 | 27 |
| Therapeutic
drugs |
|
|
|
| 0.0647b |
|
Sunitinib | 12 | 57 | 6 | 54 |
|
Sorefenib | 3 | 14 | 1 | 5 |
|
Pazopanib | 5 | 24 | 2 | 10 |
|
Temsirolimus | 1 | 5 | 2 | 10 |
| Subsequent
therapyc |
|
|
|
| 0.003b |
|
None | 1 | 5 | 7 | 64 |
|
Second-line | 15 | 72 | 4 | 36 |
| Third
or further-line | 7 | 33 | 2 | 18 |
Discussion
The pathogenesis of RCC has been considered to be
closely associated with inflammation. A variety of indices related
to inflammation have been reported to exhibit a predictive value
for RCC, including serum CRP level, platelet count, NLR (31,32),
platelet to lymphocyte ratio (31,33),
lymphocyte-to-monocyte ratio (31,34), the
prognostic nutritional index (31,35), GPS
(29) and mGPS (27). Cytokines and their receptors, such as
IL-6 and granulocyte-stimulating factor receptor 1 have also been
reported as indices of inflammatory status. Serum CRP and albumin
levels were found to be particularly good indicators of
inflammatory status. A retrospective evaluation of 406 RCC patients
indicated that the CRP/albumin ratio was valuable for the
prediction of OS (31). The
CRP/albumin ratio was also found to be an independent prognostic
factor in hepatocellular (36) and
esophageal carcinoma (37).
The present study investigated the mGPS of 32 RCC
patients prior to the initial chemotherapy, and the mGPS low
patients (score 0) exhibited a favorable prognosis. mGPS is also
calculated using serum CRP and albumin levels. Lamb et al
reported the predictive value of mGPS based on analyses of 169 RCC
patients who received curative resection (27). Previous studies that assessed the
predictive value of mGPS were mostly targeted towards the
curability of RCC patients who had undergone curative resection.
Therefore, there is little information available regarding the
predictive value of the mGPS for metastatic or recurrent RCC
patients who were treated with molecular-targeted agents. The
present findings, indicating a positive correlation between PFS and
OS of these RCC patients and their mGPS, strongly suggest a
predictive value of mGPS for patients with metastatic or recurrent
RCC.
The mechanisms underlying the correlation of
inflammatory status with prognosis of metastatic or recurrent RCC
have been considered to be as follows: First, since
inflammation-associated cytokines may directly induce tumor cell
growth, there may be a higher induction of RCC cell proliferation
in mGPS high patients compared with that in mGPS low patients.
Second, inflammation is often associated with cachexia and
deterioration of the patients' general condition, resulting in
insufficient administration of chemotherapy. In this study,
favorable PFS with first-line chemotherapy in mGPS low patients
suggested that the mGPS may be correlated with efficacy of the
initial molecular-targeted therapy. One possible reason for this
correlation is that the mGPS low patients may have harbored cancer
cells with relatively non-aggressive characteristics (low
proliferation rate, as mentioned above) that were sensitive to
tyrosine kinase inhibitors (TKIs). The cell proliferation of clear
cell carcinoma has been reported to depend on vascular endothelial
growth factor receptor (VEGFR) signaling and is sensitive to TKIs,
which inhibits the effect of VEGFR signaling (7–10).
However, the serum CRP level in patients with clear cell carcinoma
was found to be higher compared with that in patients with
papillary cell carcinoma (38).
Although the mGPS low patient group included a higher percentage of
clear cell carcinoma patients than the mGPS high patient group in
this study, it is not conclusive that the favorable PFS of the mGPS
low patients is attributed to the high percentage of clear cell
carcinoma patients. The present data also demonstrated that the
mGPS low patients tended to exhibit favorable PS and MSKCC.
Parameters such as PS and MSKCC are considered to reflect the
patients' general status; thus, the longer PFS of the mGPS low
patients may also be associated with their better general condition
due to a low inflammatory status.
Additionally, the mGPS low patients exhibited longer
OS compared with the mGPS high patients. This difference may be
associated with the high percentage of patients who were able to
receive subsequent chemotherapies. Overall survival following
termination of the initial chemotherapy in the mGPS low patients
was found to be significantly longer compared with that of the mGPS
high patients (median OS, 1,111 days vs. 180 days, respectively;
P=0.006). Although no examination of the mGPS of each patient group
after termination of the initial chemotherapy was performed, this
finding suggested that subsequent chemotherapy may also be
effective for mGPS low patients with metastatic and recurrent
RCC.
The molecular-targeted drugs that may be suitable
for mGPS high patients with metastatic or recurrent RCC must be
determined. For this purpose, an understanding of the regulatory
mechanisms of inflammation in RCC patients is required. Mammalian
target of rapamycin (mTOR) inhibitor suppresses cellular growth of
RCC by blocking mTOR-mediated signaling. Cytokine signaling
pathways including IL-6, tumor growth factor-β and insulin-like
growth factor share the common property of mTOR activation
(39,40). Since inhibition of mTOR has been
demonstrated to induce muscle protein wasting in cancer cachexia
(41,42), it may be suggested that an mTOR
inhibitor may be suitable only for mGPS low patients. However,
inflammatory cytokines have been reported to suppress the
production of VEGF from tumor cells and to regulate the tumor
microenvironment (43). Although a
direct correlation between inflammatory status and the efficacy of
anti-angiogenic therapy has not been reported, molecular-targeted
drugs and inflammatory cytokines may exert synergistic effects, and
further investigation is required to determine the appropriate
therapeutic strategy for RCC patients with a high inflammatory
status.
Although the present study was performed in order to
retrospectively investigate a small number of patients, superiority
of PFS and OS of the mGPS low over the mGPS high patient group was
observed. These results are consistent with results from curatively
resected RCC patients, and the potential prognostic value of mGPS
for metastatic or recurrent RCC patients treated with
molecular-targeted agents may be a novel finding.
The present study strongly suggested that
inflammatory status prior to the initial chemotherapy is correlated
with PFS and OS. Since the possible reasons for the favorable
survival of patients with low inflammatory status may include
acceleration of tumor growth by inflammation and insufficient
administration of chemotherapies due to inflammation, the selection
of the appropriate molecular-targeted drugs should be further
investigated. Inflammation-related indices, such as the mGPS,
reflect the interaction between the host immune system and the
tumor. The mGPS may be used not only as a predictive parameter of
RCC, but also as a biomarker to monitor the actual inflammatory
status in cases of future treatments by immune checkpoint
inhibitors.
Acknowledgements
The authors would like to thank the medical staff of
each institution who contributed to the treatment of the
patients.
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Naito S, Tomita Y, Rha SY, Uemura H, Oya
M, Song HZ, Zhong LH and Wahid MI: Kidney Cancer Working Group
report. Jpn J Clin Oncol. 40:(Suppl 1). i51–i56. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
MacLennan S, Imamura M, Lapitan MC, Omar
MI, Lam TB, Hilvano-Cabungcal AM, Royle P, Stewart F, MacLennan G,
MacLennan SJ, et al: Systematic review of oncological outcomes
following surgical management of localised renal cancer. Eur Urol.
61:972–993. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dutcher JP, Fisher RI, Weiss G, Aronson F,
Margolin K, Louie A, Mier J, Caliendo G, Sosman JA, Eckardt JR, et
al: Outpatient subcutaneous interleukin-2 and interferon-alpha for
metastatic renal cell cancer: Five-year follow-up of the cytokine
working group study. Cancer J Sci Am. 3:157–162. 1997.PubMed/NCBI
|
|
6
|
Negrier S, Escudier B, Lasset C, Douillard
JY, Savary J, Chevreau C, Ravaud A, Mercatello A, Peny J, Mousseau
M, et al: Recombinant human interleukin-2, recombinant human
interferon alfa-2a, or both in metastatic renal-cell carcinoma.
Groupe Francais d'Immunotherapie. N Engl J Med. 338:1272–1278.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Motzer RJ, Hutson TE, Cella D, Reeves J,
Hawkins R, Guo J, Nathan P, Staehler M, de Souza P, Merchan JR, et
al: Pazopanib versus sunitinib in metastatic renal-cell carcinoma.
N Engl J Med. 369:722–731. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Motzer RJ, Hutson TE, Tomczak P,
Michaelson MD, Bukowski RM, Rixe O, Oudard S, Negrier S, Szczylik
C, Kim ST, et al: Sunitinib versus interferon alfa in metastatic
renal-cell carcinoma. N Engl J Med. 356:115–124. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sternberg CN, Davis ID, Mardiak J,
Szczylik C, Lee E, Wagstaff J, Barrios CH, Salman P, Gladkov OA,
Kavina A, et al: Pazopanib in locally advanced or metastatic renal
cell carcinoma: Results of a randomized phase III trial. J Clin
Oncol. 28:1061–1068. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Motzer RJ, Barrios CH, Kim TM, Falcon S,
Cosgriff T, Harker WG, Srimuninnimit V, Pittman K, Sabbatini R, Rha
SY, et al: Phase II randomized trial comparing sequential
first-line everolimus and second-line sunitinib versus first-line
sunitinib and second-line everolimus in patients with metastatic
renal cell carcinoma. J Clin Oncol. 32:2765–2772. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Motzer RJ, Bacik J, Murphy BA, Russo P and
Mazumdar M: Interferon-alfa as a comparative treatment for clinical
trials of new therapies against advanced renal cell carcinoma. J
Clin Oncol. 20:289–296. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Heng DY, Xie W, Regan MM, Harshman LC,
Bjarnason GA, Vaishampayan UN, Mackenzie M, Wood L, Donskov F, Tan
MH, et al: External validation and comparison with other models of
the international metastatic renal-cell carcinoma database
consortium prognostic model: A population-based study. Lancet
Oncol. 14:141–148. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Heng DY, Xie W, Regan MM, Warren MA,
Golshayan AR, Sahi C, Eigl BJ, Ruether JD, Cheng T, North S, et al:
Prognostic factors for overall survival in patients with metastatic
renal cell carcinoma treated with vascular endothelial growth
factor-targeted agents: Results from a large, multicenter study. J
Clin Oncol. 27:5794–5799. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bromwich EJ, McArdle PA, Canna K, McMillan
DC, McNicol AM, Brown M and Aitchison M: The relationship between
T-lymphocyte infiltration, stage, tumour grade and survival in
patients undergoing curative surgery for renal cell cancer. Br J
Cancer. 89:1906–1908. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Crumley AB, McMillan DC, McKernan M,
McDonald AC and Stuart RC: Evaluation of an inflammation-based
prognostic score in patients with inoperable gastro-oesophageal
cancer. Br J Cancer. 94:637–641. 2006.PubMed/NCBI
|
|
16
|
Forrest LM, McMillan DC, McArdle CS,
Angerson WJ and Dunlop DJ: Evaluation of cumulative prognostic
scores based on the systemic inflammatory response in patients with
inoperable non-small-cell lung cancer. Br J Cancer. 89:1028–1030.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Fujikawa K, Matsui Y, Oka H, Fukuzawa S
and Takeuchi H: Serum C-reactive protein level and the impact of
cytoreductive surgery in patients with metastatic renal cell
carcinoma. J Urol. 162:1934–1937. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bazzi WM, Tin AL, Sjoberg DD, Bernstein M
and Russo P: The prognostic utility of preoperative
neutrophil-to-lymphocyte ratio in localized clear cell renal cell
carcinoma. Can J Urol. 23:8151–8154. 2016.PubMed/NCBI
|
|
19
|
Hu K, Lou L, Ye J and Zhang S: Prognostic
role of the neutrophil-lymphocyte ratio in renal cell carcinoma: A
meta-analysis. BMJ Open. 5:e0064042015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Templeton AJ, Knox JJ, Lin X, Simantov R,
Xie W, Lawrence N, Broom R, Fay AP, Rini B, Donskov F, et al:
Change in neutrophil-to-lymphocyte ratio in response to targeted
therapy for metastatic renal cell carcinoma as a prognosticator and
biomarker of efficacy. Eur Urol. 70:358–364. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhang GM, Zhu Y, Gu WJ, Zhang HL, Shi GH
and Ye DW: Pretreatment neutrophil-to-lymphocyte ratio predicts
prognosis in patients with metastatic renal cell carcinoma
receiving targeted therapy. Int J Clin Oncol. 21:373–378. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Argiles JM, Busquets S, Stemmler B and
López-Soriano FJ: Cancer cachexia: Understanding the molecular
basis. Nat Rev Cancer. 14:754–762. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
McMillan DC, Scott HR, Watson WS, Preston
T, Milroy R and McArdle CS: Longitudinal study of body cell mass
depletion and the inflammatory response in cancer patients. Nutr
Cancer. 31:101–105. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
O'Gorman P, McMillan DC and McArdle CS:
Prognostic factors in advanced gastrointestinal cancer patients
with weight loss. Nutr Cancer. 37:36–40. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Scott HR, McMillan DC, Crilly A, McArdle
CS and Milroy R: The relationship between weight loss and
interleukin 6 in non-small-cell lung cancer. Br J Cancer.
73:1560–1562. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Scott HR, McMillan DC, Forrest LM, Brown
DJ, McArdle CS and Milroy R: The systemic inflammatory response,
weight loss, performance status and survival in patients with
inoperable non-small cell lung cancer. Br J Cancer. 87:264–267.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lamb GW, Aitchison M, Ramsey S, Housley SL
and McMillan DC: Clinical utility of the Glasgow Prognostic Score
in patients undergoing curative nephrectomy for renal clear cell
cancer: Basis of new prognostic scoring systems. Br J Cancer.
106:279–283. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Proctor MJ, Morrison DS, Talwar D, Balmer
SM, O'Reilly DS, Foulis AK, Horgan PG and McMillan DC: An
inflammation-based prognostic score (mGPS) predicts cancer survival
independent of tumour site: A Glasgow inflammation outcome study.
Br J Cancer. 104:726–734. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ramsey S, Lamb GW, Aitchison M, Graham J
and McMillan DC: Evaluation of an inflammation-based prognostic
score in patients with metastatic renal cancer. Cancer.
109:205–212. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
McMillan DC, Crozier JE, Canna K, Angerson
WJ and McArdle CS: Evaluation of an inflammation-based prognostic
score (GPS) in patients undergoing resection for colon and rectal
cancer. Int J Colorectal Dis. 22:881–886. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Chen Z, Shao Y, Fan M, Zhuang Q, Wang K,
Cao W, Xu X and He X: Prognostic significance of preoperative
C-reactive protein: Albumin ratio in patients with clear cell renal
cell carcinoma. Int J Clin Exp Pathol. 8:14893–14900.
2015.PubMed/NCBI
|
|
32
|
Pichler M, Hutterer GC, Stoeckigt C,
Chromecki TF, Stojakovic T, Golbeck S, Eberhard K, Gerger A,
Mannweiler S, Pummer K and Zigeuner R: Validation of the
pre-treatment neutrophil-lymphocyte ratio as a prognostic factor in
a large European cohort of renal cell carcinoma patients. Br J
Cancer. 108:901–907. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Gunduz S, Mutlu H, Tural D, Yıldız Ö,
Uysal M, Coskun HS and Bozcuk H: Platelet to lymphocyte ratio as a
new prognostic for patients with metastatic renal cell cancer. Asia
Pac J Clin Oncol. 11:288–292. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Chang Y, An H, Xu L, Zhu Y, Yang Y, Lin Z
and Xu J: Systemic inflammation score predicts postoperative
prognosis of patients with clear-cell renal cell carcinoma. Br J
Cancer. 113:626–633. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Jeon HG, Choi DK, Sung HH, Jeong BC, Seo
SI, Jeon SS, Choi HY and Lee HM: Preoperative prognostic
nutritional index is a significant predictor of survival in renal
cell carcinoma patients undergoing nephrectomy. Ann Surg Oncol.
23:321–327. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Kinoshita A, Onoda H, Imai N, Iwaku A,
Oishi M, Tanaka K, Fushiya N, Koike K, Nishino H and Matsushima M:
The C-reactive protein/albumin ratio, a novel inflammation-based
prognostic score, predicts outcomes in patients with hepatocellular
carcinoma. Ann Surg Oncol. 22:803–810. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wei XL, Wang FH, Zhang DS, Qiu MZ, Ren C,
Jin Y, Zhou YX, Wang DS, He MM, Bai L, et al: A novel
inflammation-based prognostic score in esophageal squamous cell
carcinoma: The C-reactive protein/albumin ratio. BMC Cancer.
15:3502015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Jabs WJ, Busse M, Krüger S, Jocham D,
Steinhoff J and Doehn C: Expression of C-reactive protein by renal
cell carcinomas and unaffected surrounding renal tissue. Kidney
Int. 68:2103–2110. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Robert F, Mills JR, Agenor A, Wang D,
DiMarco S, Cencic R, Tremblay ML, Gallouzi IE, Hekimi S, Wing SS
and Pelletier J: Targeting protein synthesis in a Myc/mTOR-driven
model of anorexia-cachexia syndrome delays its onset and prolongs
survival. Cancer Res. 72:747–756. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Yoshida T, Tabony AM, Galvez S, Mitch WE,
Higashi Y, Sukhanov S and Delafontaine P: Molecular mechanisms and
signaling pathways of angiotensin II-induced muscle wasting:
Potential therapeutic targets for cardiac cachexia. Int J Biochem
Cell Biol. 45:2322–2332. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Gordon BS, Kelleher AR and Kimball SR:
Regulation of muscle protein synthesis and the effects of catabolic
states. Int J Biochem Cell Biol. 45:2147–2157. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Manne ND, Lima M, Enos RT, Wehner P,
Carson JA and Blough E: Altered cardiac muscle mTOR regulation
during the progression of cancer cachexia in the ApcMin/+ mouse.
Int J Oncol. 42:2134–2140. 2013.PubMed/NCBI
|
|
43
|
Nagineni CN, William A, Cherukuri A,
Samuel W, Hooks JJ and Detrick B: Inflammatory cytokines regulate
secretion of VEGF and chemokines by human conjunctival fibroblasts:
Role in dysfunctional tear syndrome. Cytokine. 78:16–19. 2016.
View Article : Google Scholar : PubMed/NCBI
|