Introduction
Vaginal cancer is a rare disease, accounting for
only 2% of all gynecological malignancies (1). Squamous cell carcinoma (SCC) is the
most common type of vaginal cancer accounting for 90% of primary
vaginal carcinomas (2). The
incidence of SCC increases with age, with the peak age being 70–79
years. However, 30% of the patients are aged <60 years (3). The diagnosis of primary vaginal
carcinoma should exclude synchronous cervical, vulval or urethral
cancer (4). There is currently no
consensus regarding the treatment of vaginal carcinoma. Surgery and
radiotherapy are mainly used for patients with stage I disease.
Good 5-year survival rates have been reported in patients with
stage II or higher vaginal carcinoma who are treated by
radiotherapy. However, traditional radiotherapy is associated with
several side effects, such as irradiation injury to the bladder and
rectum, vaginal stenosis and dyspareunia, with severe compromise of
the patients' quality of life (5,6).
Treatment individualization has been recommended for early-stage
vaginal cancer. Surgery has achieved satisfactory results for
patients with stage I vaginal carcinoma (7,8). It was
reported that surgery following neoadjuvant chemotherapy achieved a
good therapeutic effect (9–12). However, the effect of chemotherapy on
vaginal SCC has not been extensively evaluated and the majority of
available data are derived from studies with small-sized samples or
case reports, without a universal consensus regarding the
chemotherapy regimens.
Neoadjuvant chemotherapy for cervical cancer is
currently considered to be efficient (13–15). It
has been suggested that, as the vagina and the cervix are lined
with the same type of squamous cell epithelium, the same risk
factors are present in both cervical and vaginal carcinomas
(16). The aim of the present study
was to evaluate the effect of neoadjuvant chemotherapy on patients
with primary vaginal SCC.
Case reports
Case 1
A 56-year-old woman presented in December 2011 with
postmenopausal vaginal bleeding for 2.5 months. The biopsy result
revealed keratinizing SCC. The patient was referred to our hospital
and pelvic examination indicated a 5×5×2-cm solid tumor in the
upper one-third of the posterior wall of the vagina, without
invasion of the paracolpium. The patient was diagnosed with stage I
vaginal carcinoma. The computed tomography showed no lesions in
other parts of the body. The patient was treated with irinotecan
240 mg and cisplatin 100 mg for 6 courses every 3–4 weeks. The
tumor completely regressed after 2 courses of chemotherapy.
Colposcopic biopsy confirmed no residual cancer tissue after 4
courses of chemotherapy. Due to the efficacy of chemotherapy, the
patient and her family declined further surgery. The patient was
followed up for 45 months (last follow-up, April 2016) and she
remained cancer-free with restored sexual function.
Case 2
A 39-year-old woman presented in October 2011 with
vaginal bleeding for 20 days. The pelvic examination identified a
5×4×1-cm solid tumor in the upper one-third of the left wall of the
vagina, invading the paracolpium, but not reaching the pelvic wall.
The biopsy revealed poorly differentiated SCC. The computed
tomography showed no lesions in other parts of the body. The
patient was diagnosed with stage II vaginal carcinoma and was
treated with irinotecan 240 mg and cisplatin 100 mg for 4 courses
every 3–4 weeks. The tumor completely regressed after 2 courses of
chemotherapy. Colposcopic biopsy confirmed the presence of cell
hyperplasia after 3 courses of chemotherapy. Radical resection was
advised, but the patient wished to preserve her fertility. Partial
vaginal resection was performed and no cancer cells were identified
on postoperative pathology. The patient received one more course of
chemotherapy after surgery and was followed up for 48 months (last
follow-up, April 2016), without tumor recurrence.
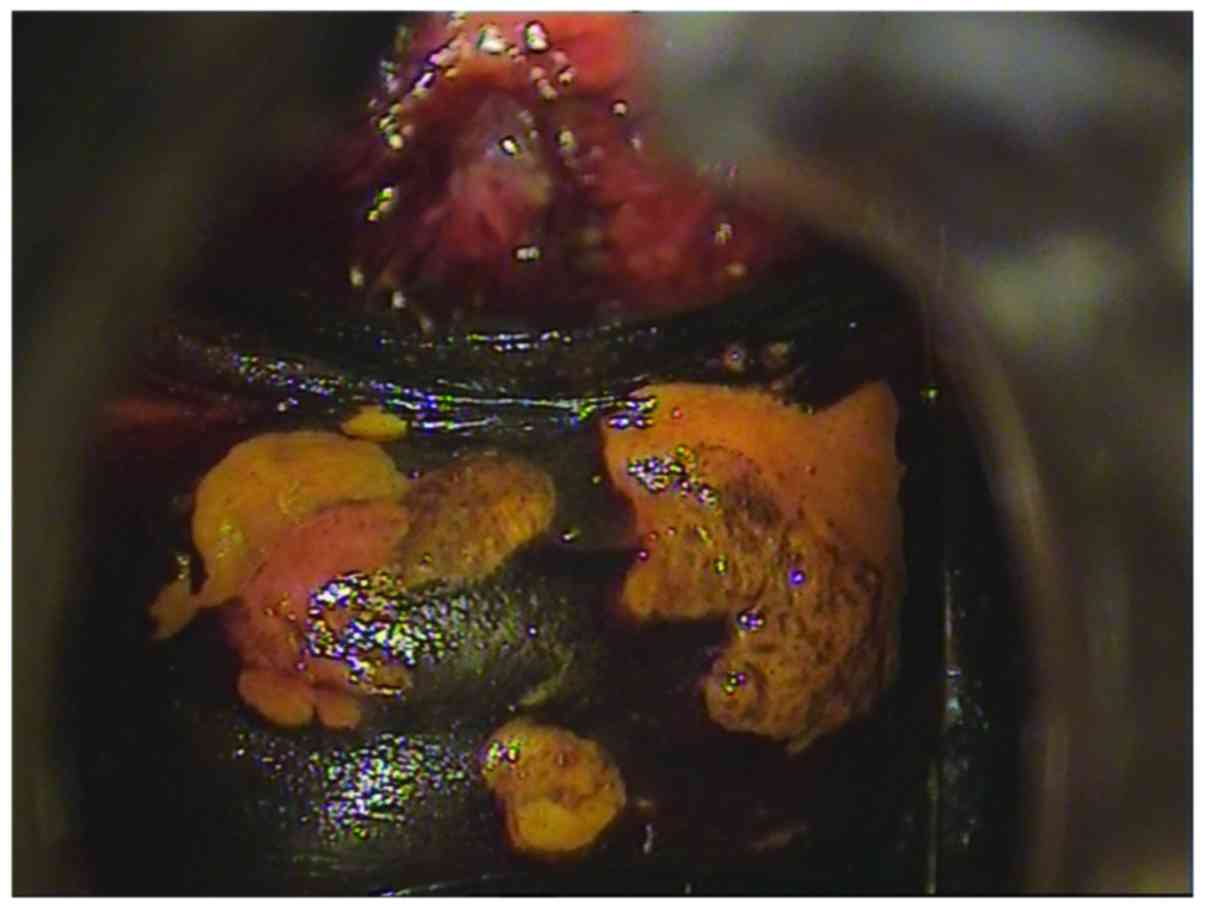
Case 3
A 43-year-old woman presented in November 2015 with
post-coital vaginal bleeding for 7 years and the biopsy revealed
moderately differentiated SCC. The patient was referred to our
hospital and on pelvic examination a 3.5-cm solid tumor was
identified on the middle third of the anterior wall of the vagina
(Fig. 1), without invasion of the
paracolpium. The patient was diagnosed with stage I vaginal
carcinoma. The computed tomography and magnetic resonance imaging
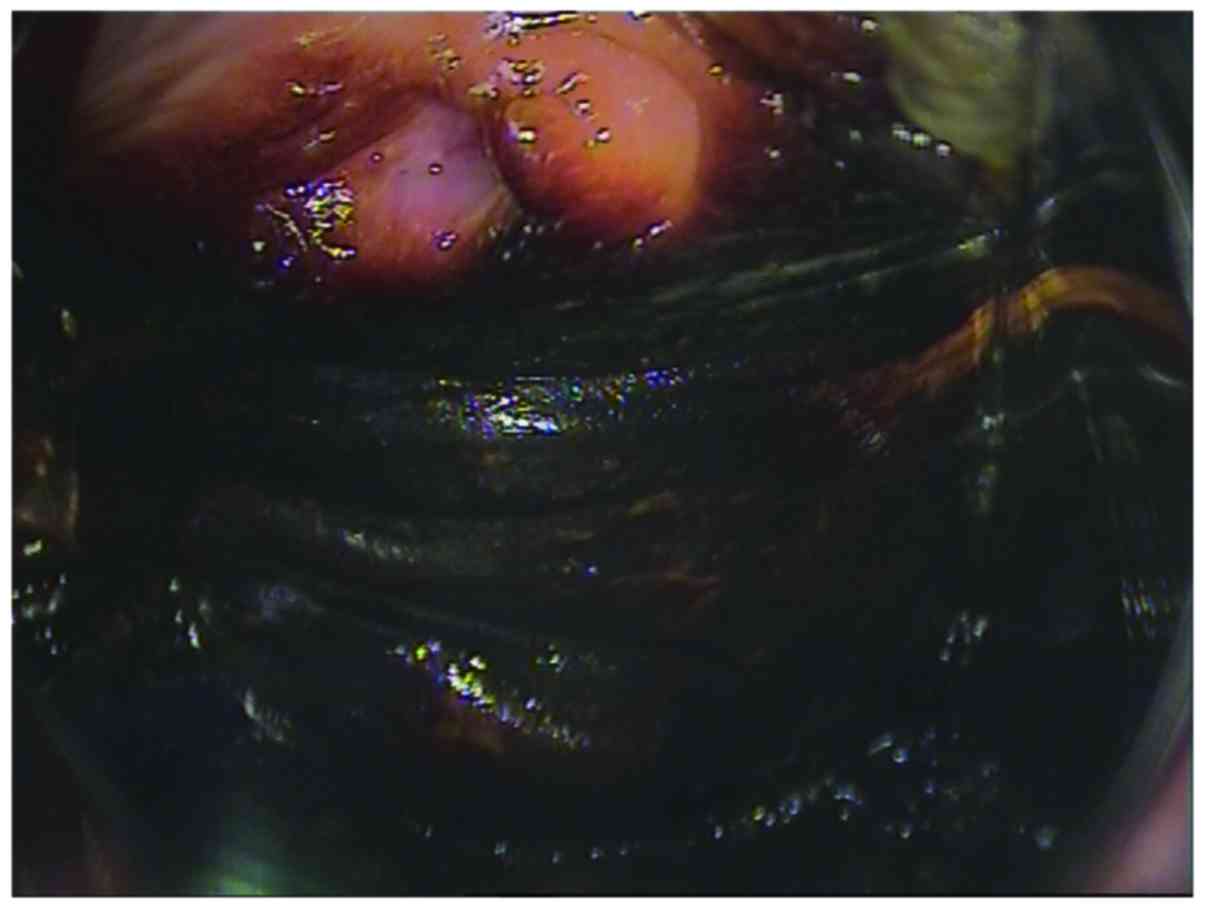
showed no lesions in other parts of the body. The patient was
treated with irinotecan 240 mg and cisplatin 100 mg for 2 courses
every 3 weeks. The tumor completely regressed after 2 courses of
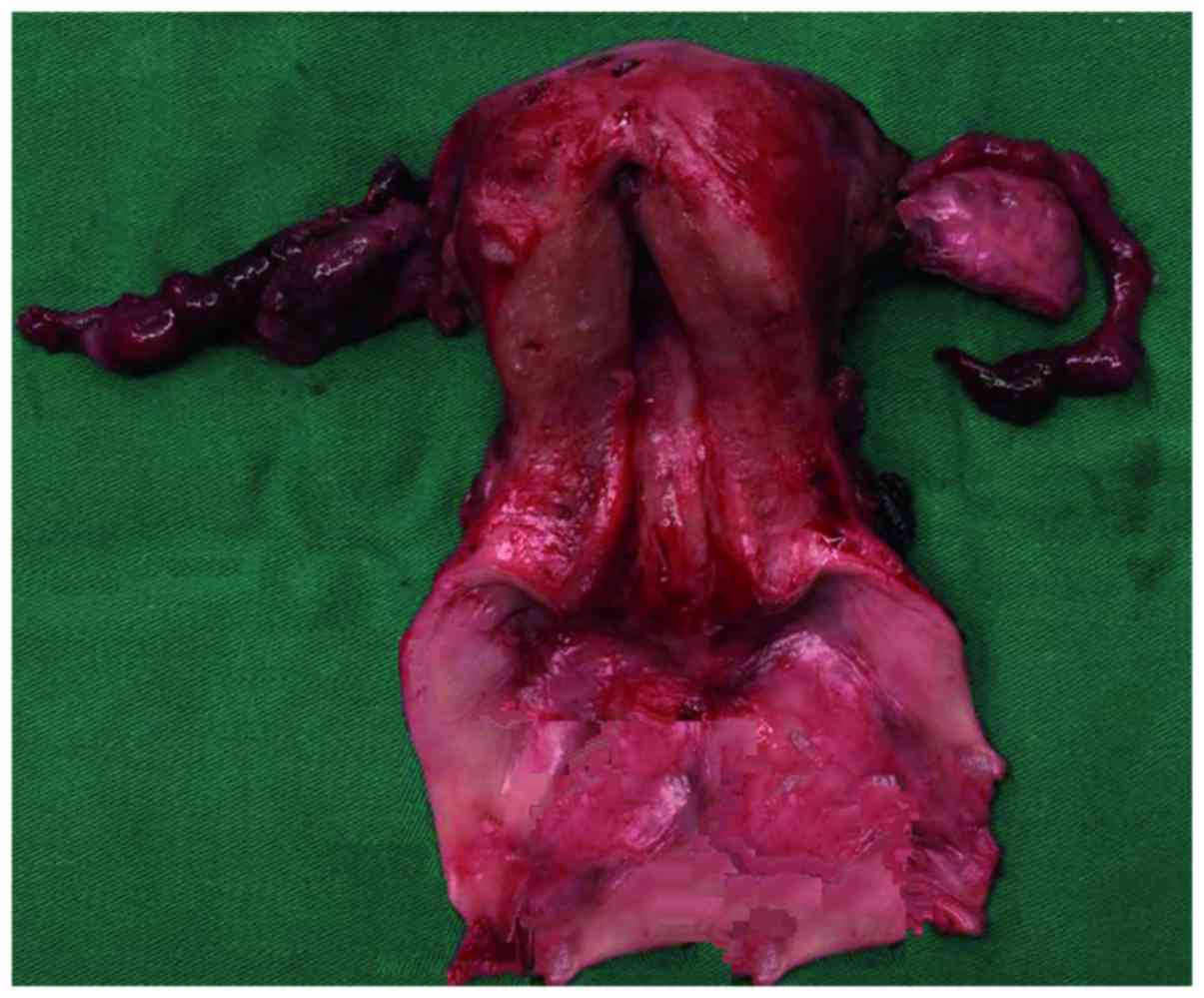
chemotherapy (Fig. 2). The patient
then received laparoscopic subradical hysterectomy, bilateral
adnexectomy, pelvic lymphadenectomy, complete resection of the
vagina and peritoneal vaginoplasty (Fig.
3). Postoperative pathological examination identified no cancer
cells in the resected tissue. The patient has had a vaginal mould
for 6 months postoperatively, without complications (last
follow-up, April 2017).
All 3 patients tolerated the chemotherapy well.
There were no serious complications, such as bone marrow
suppression or diarrhea, which may affect the course of treatment.
All 3 patients achieved clinical and pathological complete response
confirmed by pathological examination of colposcopic biopsy
specimens or surgically resected tissue. Written informed consent
was obtained from the patients and their families regarding the
publication of their case details.
Discussion
Primary vaginal cancer is a rare gynecological
malignancy and its diagnosis should exclude cervical, vulval or
urethral cancer. The main histopathological types of primary
vaginal carcinoma include SCC, adenocarcinoma, malignant melanoma
and sarcoma. SCC is the most common histotype and accounts for
85–95% of all cases (2,3,16). The
incidence of SCC increases with age, with ~50% patients aged >70
years at diagnosis. The main pathogenic risk factors include human
papillomavirus infection, injury through use of pessaries, previous
gynecological disorders, multiple sexual partners, earlier pelvic
irradiation, and smoking (16–18). The
high-risk prognostic factors include age at onset, tumor size,
clinical stage and pathological type. The 5-year survival rate of
vaginal SCC was reported to be 84% for stage I, 75% for stage II
and 57% for stage III/IV disease (19).
The standard treatment for patients affected by
vaginal cancer is radiotherapy. Hiniker et al (5) investigated 91 cases of patients with
vaginal cancer and reported that the dose of radiation was 70–80
Gy. Platta et al (6)
investigated 63 patients with vaginal cancer who were treated with
radiotherapy. The 5-year survival rate was 73.3% for stage I–II and
34.4% for stage III–IV disease. However, the incidence rate of
serious side effects (grade >3) was 23.1%. It was also reported
that surgery alone is preferable to radiotherapy for stage I
vaginal cancer (7,8). Due to the particular anatomical
location of the vagina, the range of resection without injury to
the surrounding structures is limited. However, the side effects of
radiotherapy, such as vaginal stenosis, paracolpium fibrosis and
radiocystitis, may severely compromise the patient's quality of
life. Surgery is the recommended treatment for young patients with
early-stage vaginal cancer.
There are currently no randomized controlled
clinical trials comparing various treatments due to the low
incidence of vaginal cancer. Treatment is mainly focused on the
management of cervical or vulval cancer and, thus far, a standard
treatment for vaginal cancer has not been established. Currently,
the purpose of treatment is not only prolongation of survival, but
also planning personalized and individualized treatment. New
research in the field of gynecological oncology is aimed at
preserving the patient's physiological functions and quality of
life to the greatest extent possible.
The number of studies on chemotherapy regimens of
primary vaginal SCC is limited. It has been reported that the
treatment result is satisfactory when using neoadjuvant
chemotherapy for early-stage vaginal cancer. A clinical research
was performed by Benedetti et al (11). Of 11 patients enrolled, 27% achieved
complete remission and 64% achieved partial remission after
receiving 3 courses of chemotherapy with paclitaxel and cisplatin
every 21 days. All the patients were treated with radical
hysterectomy and total vaginal resection following chemotherapy.
The average follow-up time was 75 months. One patient succumbed to
the disease and 2 patients relapsed. The authors suggested that
neoadjuvant chemotherapy followed by radical surgery is a feasible
therapeutic strategy, with good short- and long-term results. Lv
et al (12) reported the case
of a patient with stage II vaginal cancer. The tumor size was
significantly reduced after 2 courses of chemotherapy with
bleomycin and cisplatin. The patient received radical hysterectomy,
total vaginal resection and vaginal reconstruction using bilateral
pudendal thigh fasciocutaneous flaps. The patient remained
tumor-free with restored sexual function after 30 months. Thus,
surgery may also be performed following neoadjuvant chemotherapy
for patients with stage II vaginal cancer, but the treatment must
be individualized.
Irinotecan is a topoisomerase I inhibitor,
specifically acting on the S phase of the cell cycle by impeding
DNA synthesis and inhibiting the growth of tumor cells (20). Irinotecan is currently widely applied
in the treatment of colorectal, lung, esophageal, cervical and
ovarian cancer, as well as other tumors, with good therapeutic
outcomes. Tsubamoto et al (13) reported 2 cervical cancer patients who
wished to maintain their fertility; they received radical
trachelectomy after 3 courses of chemotherapy with irinotecan and
cisplatin. Postoperative pathological examination confirmed that
there were no cancer cells in the resected tissues. Yamaguchi et
al (21) treated stage IB2 and
IIB cervical cancer with irinotecan and nedaplatin, with good
therapeutic efficacy. Other studies suggested that the vagina and
the cervix are lined with the same type of squamous cell
epithelium, and several risk factors are shared by cervical and
vaginal carcinoma. Accordingly, the etiology is similar for these
two cancers (16). Thus, irinotecan
combined with platinum for the treatment of advanced cervical
cancer has exhibited confirmed therapeutic efficacy; however, there
is little evidence regarding its efficacy against vaginal
cancer.
A search through Medline identified only two reports
of chemotherapy for vaginal cancer with irinotecan combined with
platinum. Umesaki et al (9)
reported a 48-year-old woman who suffered from stage II vaginal
cancer. Pelvic examination identified a 3-cm solid tumor in the
middle third of the posterior wall of the vagina. The tumor
disappeared after 1 course of chemotherapy with irinotecan and
cisplatin. The patient underwent radical hysterectomy, bilateral
adnexectomy, pelvic lymphadenectomy and resection of the upper
two-thirds of the vagina. Postoperative pathological examination
revealed no cancer cells in the resected tissue. The patient was
followed up for 1 year and there was no tumor recurrence. Mabuchi
et al (10) reported a
36-year-old woman who suffered from stage I vaginal cancer. The
tumor was sized ~3×4 cm and disappeared after 4 courses of
chemotherapy with irinotecan and nedaplatin; however, the vaginal
biopsy pathology was vaginal intraepithelial neoplasia (VAIN)III.
The patient received partial resection of the vagina and the
results of the postoperative pathological examination were also
VAINIII. Thus, 2 more courses of chemotherapy were administered.
The patient was followed up for 14 menstrual cycles and there was
no tumor recurrence. These two reports confirmed the efficacy of
irinotecan combined with platinum in the treatment of early-stage
vaginal cancer.
In the present study, 3 relatively young patients
developed early-stage vaginal cancer. Case 1 was extremely
responsive to irinotecan and cisplatin and the tumor completely
regressed after 2 courses of chemotherapy. Colposcopic biopsy
confirmed absence of residual cancer tissue after 4 courses of
chemotherapy. The patient was followed up for 45 months after a
total of 6 courses of chemotherapy. No tumor recurrence was found,
and the patient's sexual function was restored to normal. Case 2
had stage II vaginal cancer, with a wide range of lesions. There
was residual tumor tissue after 3 courses of chemotherapy, but the
patient wished to preserve her fertility. The patient was treated
with partial vaginal resection, but refused continued treatment
after 4 courses of chemotherapy due to amenorrhea; she was followed
up for 48 months and there was no tumor recurrence. Case 3 was a
43-year-old patient whose tumor completely regressed after 2
courses of chemotherapy. The patient received laparoscopic
subradical hysterectomy, bilateral adnexectomy, pelvic
lymphadenectomy, complete resection of the vagina and peritoneal
vaginoplasty. The patient has had a vaginal mould for 6 months
postoperatively, without any complications. The 3 patients
discussed herein were treated with either chemotherapy or
chemotherapy combined with surgery and the curative effect was
satisfactory. The lesion size decreased following chemotherapy and
the scope and difficulty of the surgery were reduced. Furthermore,
the goal of treatment was attained without damaging the bladder,
rectum or vagina by radiation. The first 2 patients had no tumor
recurrence after long-term follow-up. The treatment outcome and
quality of life were satisfactory.
Although there are a few studies available regarding
the clinical efficacy of chemotherapy for the treatment of vaginal
cancer, the majority included small-sized samples or case reports.
Due to the lack of large-sized, multi-centre, randomized controlled
trials, no unanimously accepted chemotherapy regimen has been
developed to date. The incidence of vaginal cancer is low, mostly
affecting elderly patients. However, for young early-stage patients
who wish to preserve fertility and sexual function, radiotherapy
may affect their quality of life. Thus, treatment should be
individualized for such patients; chemotherapy alone or combined
with surgery appears to be a feasible option. However, further
research is required to determine the standards of chemotherapy
regimens, courses and operative methods.
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hacker NF, Eifel PJ and Van der Velden J:
Cancer of the vagina. Int J Gynaecol Obstet. 131 Suppl 2:S84–S87.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Creasman WT, Phillps JL and Menck HR: The
national cancer data base report on cancer of the vagina. Cancer.
83:1033–1040. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Beller U, Benedet JL, Creasman WT, Nqan
HY, Quinn MA, Maisonneuve P, Pecorelli S, Odicino F and Heintz AP:
Carcinoma of the vagina. FIGO 26th annual report on the results of
treatment in gynecological cancer. Int J Gynaecol Obstet. 95 Suppl
1:S29–S42. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hiniker SM, Roux A, Murphy JD, Harris JP,
Tran PT, Kapp DS and Kidd EA: Primary squamous cell carcinoma of
the vagina: Prognostic factors, treatment patterns, and outcomes.
Gynecol Oncol. 131:380–385. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Platta CS, Anderson B, Geye H, Das R,
Straub M and Bradley K: Adjuvant and definitive radiation therapy
for primary carcinoma of the vagina using brachytherapy and
external beam radiation therapy. J contemp Brachytherapy. 5:76–82.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tjalma WA, Monaghan JM, de Barros Lopes A,
Naik R, Nordin AJ and Weyler JJ: The role of surgery in invasive
squamous carcinoma of the vagina. Gynecol Oncol. 81:360–365. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sinha B, Stehman F, Schilder J, Clark L
and Cardense H: Indiana University experience in the management of
vaginal cancer. Int J Gynecol Cancer. 19:686–693. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Umesaki N, Kawamura N, Tsujimura A,
Ichimura T, Tanaka T and Oqita S: Stage II vaginal cancer
responding to chemotherapy with irinotecan and cisplatin: A case
report. Oncol Rep. 6:123–125. 1999.PubMed/NCBI
|
|
10
|
Mabuchi Y, Yahata T, Kobayashi A, Tanizaki
Y, Minami S and Ino K: Vaginal carcinoma in a young woman who
underwent fertility-sparing treatment involving chemotherapy and
conservative surgery. J Obstet Gynaecol Res. 41:989–992. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Panici P Benedetti, Bellati F, Plotti F,
Di Donato V, Antonilli M, Perniola G, Manci N, Muzii L and Angioli
R: Neoadjuvant chemotherapy followed by radical surgery in patients
affected by vaginal carcinoma. Gynecol Oncol. 111:307–311. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lv L, Sun Y, Liu H, Lou J and Peng Z:
Neoadjuvant chemotherapy followed by radical surgery and
reconstruction of the vagina in a patient with stage II primary
vaginal squamous carcinoma. J Obstet Gynaecol Res. 36:1245–1248.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tsubamoto H, Kanazawa R, Inoue K, Ito Y,
Komori S, Maeda H and Hirota S: Fertility-sparing management for
bulky cervical cancer using neoadjuvant transuterine arterial
chemotherapy followed by vaginal trachelectomy. Int J Gynecol
Cancer. 22:1057–1062. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pareja R, Rendón GJ, Vasquez M, Echeverri
L, Sanz-Lomana CM and Ramirez PT: Immediate radical trachelectomy
versus neoadjuvant chemotherapy followed by conservative surgery
for patients with stage IB1 cervical cancer with tumors 2 cm or
larger: A literature review and analysis of oncological and
obstetrical outcomes. Gynecol Oncol. 137:574–580. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Robova H, Halaska MJ, Pluta M, Skapa P,
Matecha J, Lisy J and Rob L: Oncological and pregnancy outcomes
after high-dose density neoadjuvant chemotherapy and
fertility-sparing surgery in cervical cancer. Gynecol Oncol.
135:213–216. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hellman K, Silfverswärd C, Nilsson B,
Hellström AC, Frankendal B and Pettersson F: Primary carcinoma of
the vagina: Factors influencing the age at diagnosis. The
rediumhemmet series 1956–96. Int J Gynecol cancer. 14:491–501.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Daling JR, Madeleine MM, Schwartz SM,
Shera KA, Carter JJ, McKnight B, Porter PL, Galloway DA, McDougall
JK and Tamimi H: A population based study of squamous cell vaginal
cancer: HPV and cofactors. Gynecol Oncol. 84:263–270. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Larsson GL, Helenius G, Andersson S, Sorbe
B and Karisson MG: Prognostic impact of human papilloma virus (HPV)
genotyping and HPV-16 subtyping in vaginal carcinoma. Gynecol
Oncol. 129:406–411. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Blecharz P, Reinfuss M, Jakubowicz J,
Piotr S, Wysocki W, Karolewski K and Urbański K: Prognostic factors
in patients with primary invasive vaginal carcinoma. Ginekol Pol.
83:904–909. 2012.PubMed/NCBI
|
|
20
|
Ramesh M, Ahlawat P and Srinivas NR:
Irinotecan and its active metabolite, SN-38: Review of
bioanalytieal methods and recent update from clinical pharmacology
perspectives. Biomed Chromatogr. 24:104–123. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yamaguchi S, Nishimura R, Yaegashi N,
Kiguchi K, Sugiyama T, Kita T, Kubushiro K, Kokawa K, Hiura M,
Mizutani K, et al: Phase II study of neoadjuvant chemotherapy with
irinotecan hydrochloride and nedaplatin followed by radical
hysterectomy for bulky stage Ib2 to IIb, cervical squamous cell
carcinoma: Japanese Gynecologic Oncology Group study (JGOG 1065).
Oncol Rep. 28:487–493. 2012.PubMed/NCBI
|